
Uni-, Bi- or Trifocal Hepatocellular Carcinoma in Western Patients: Recurrence and Survival after Percutaneous Thermal Ablation


 , ,
, ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Design and Ethics
2.2. Patients and Tumor Data
2.3. Percutaneous Thermal Ablation
2.4. Follow-Up and Outcomes
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Follow-Up and Events
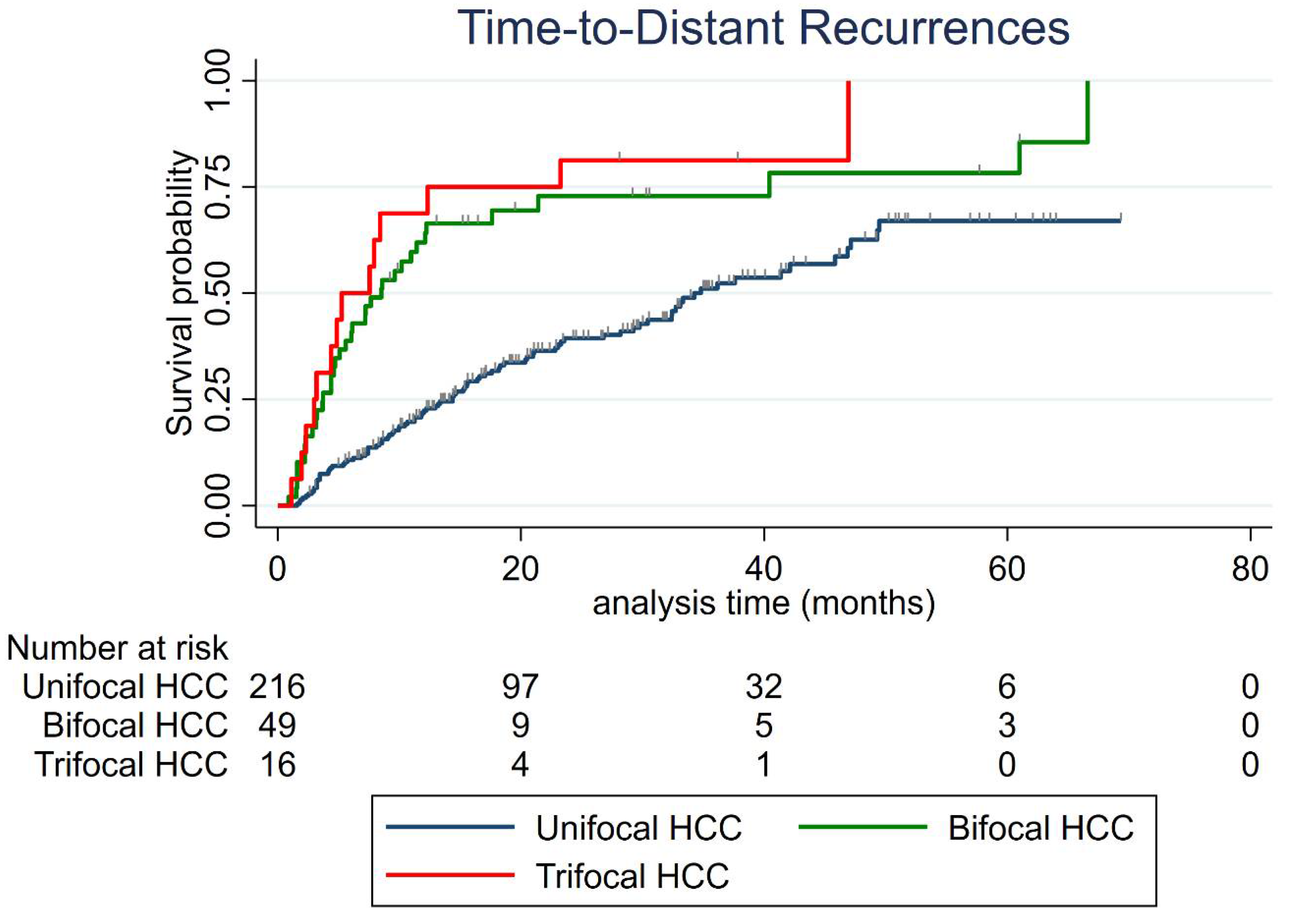
3.3. Distant Recurrence
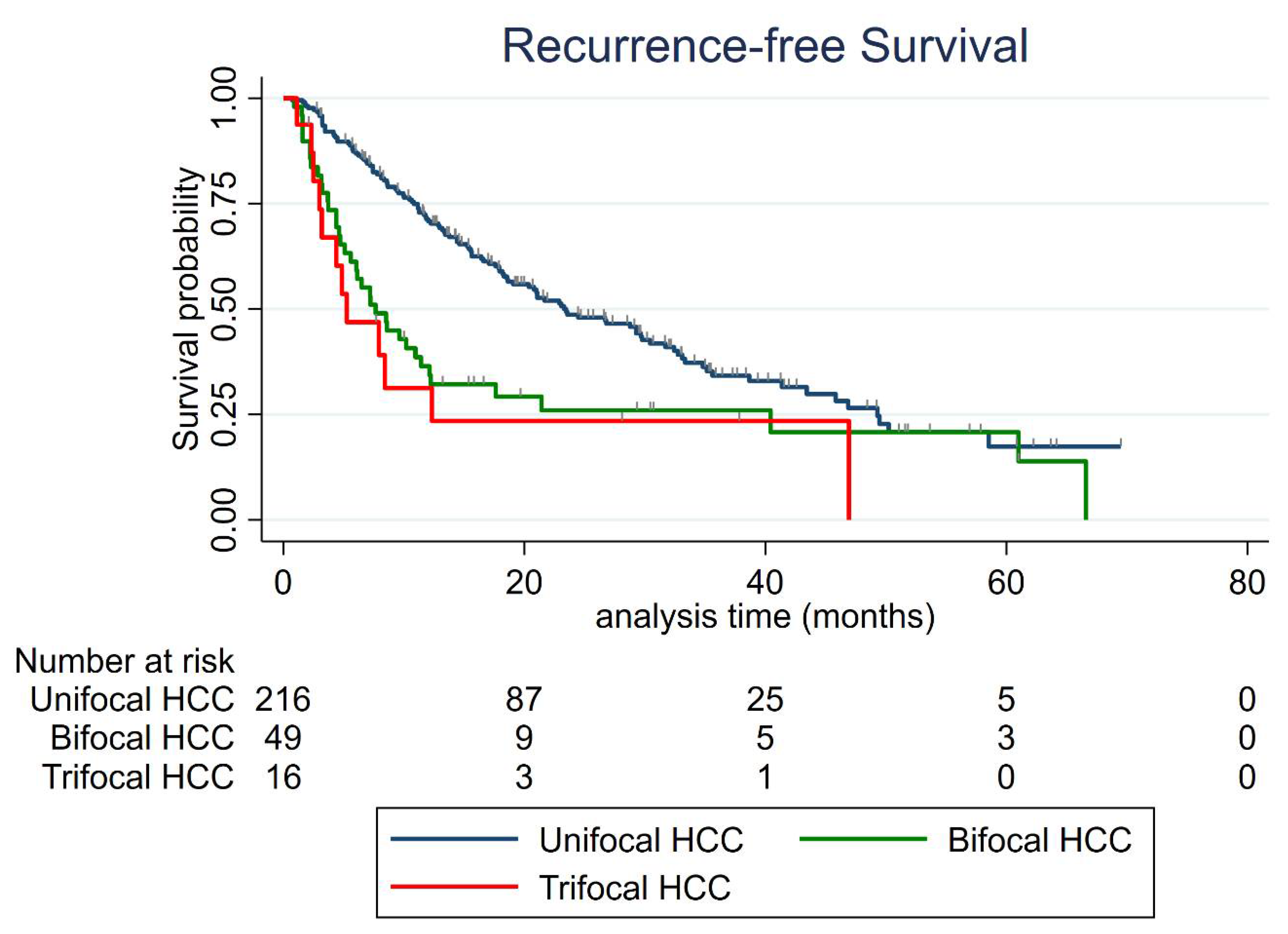
3.4. Recurrence-Free Survival (RFS)
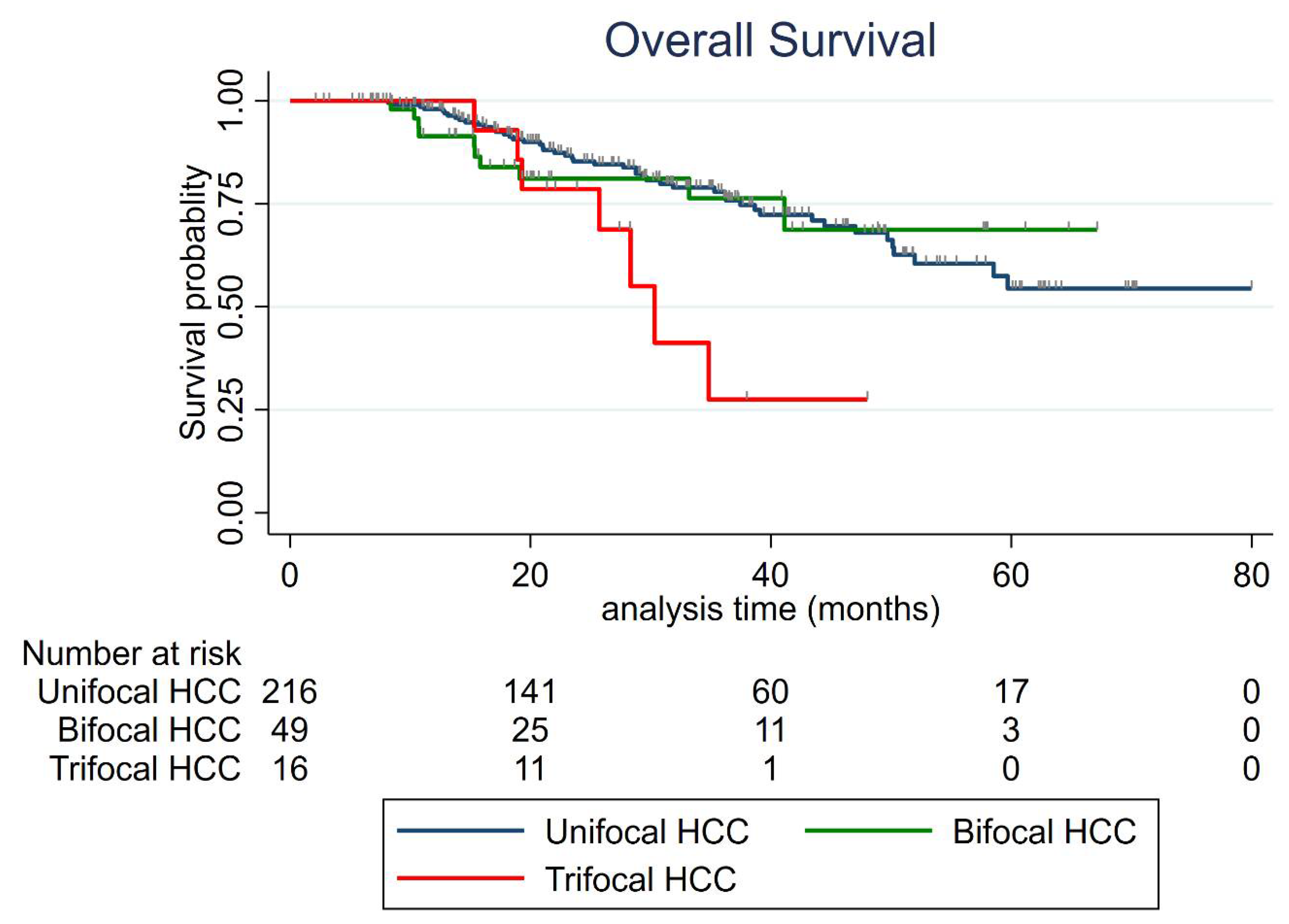
3.5. Overall Survival (OS)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PTA | Percutaneous Thermal Ablation |
| HCC | Hepatocellular Carcinoma |
| BCLC | Barcelona Clinic Liver Cancer |
| US | Ultrasonography |
| RFS | Recurrence-Free Survival |
| AFP | Alpha-Fetoprotein |
| OS | Overall Survival |
| MELD | Model for End-Stage Liver Disease |
| NAFLD | Non-Alcoholic Fatty Liver Disease |
| ECOG | Eastern Cooperative Oncology Group |
| AASLD | American Association for the Study of Liver Disease |
| EASL | European Association for the Study of the Liver |
| BMI | Body Mass Index |
| ALBI | Albumin–Bilirubin |
| MRI | Magnetic Resonance Imaging |
| ASA | American Society of Anesthesiologists |
| CT | Computed Tomography |
| SIR | Society of Interventional Radiology |
| LTP | Local tumor progression |
| SD | Standard Deviation |
| IQR | Interquartile Range |
| AIC | Akaike Information Criterion |
| TACE | Transarterial Chemoembolization |
| OR | Odds Ratio |
| CI | Confidence Interval |
| HR | Hazard Ratio |
| NASH | Non-Alcoholic Steatohepatitis |
References
- Galle, P.R.; Forner, A.; Llovet, J.M.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.-L.; Schirmacher, P.; Vilgrain, V. EASL Clinical Practice Guidelines: Management of Hepatocellular Carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global Cancer Statistics 2018: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular Carcinoma. Lancet 2018, 391, 1301–1314. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD Guidelines for the Treatment of Hepatocellular Carcinoma: Heimbach et al. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef]
- Shiina, S.; Tateishi, R.; Arano, T.; Uchino, K.; Enooku, K.; Nakagawa, H.; Asaoka, Y.; Sato, T.; Masuzaki, R.; Kondo, Y.; et al. Radiofrequency Ablation for Hepatocellular Carcinoma: 10-Year Outcome and Prognostic Factors. Am. J. Gastroenterol. 2012, 107, 569–577. [Google Scholar] [CrossRef] [PubMed]
- N’Kontchou, G.; Mahamoudi, A.; Aout, M.; Ganne-Carrié, N.; Grando, V.; Coderc, E.; Vicaut, E.; Trinchet, J.C.; Sellier, N.; Beaugrand, M.; et al. Radiofrequency Ablation of Hepatocellular Carcinoma: Long-Term Results and Prognostic Factors in 235 Western Patients with Cirrhosis. Hepatology 2009, 50, 1475–1483. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Cioni, D.; Crocetti, L.; Franchini, C.; Pina, C.D.; Lera, J.; Bartolozzi, C. Early-Stage Hepatocellular Carcinoma in Patients with Cirrhosis: Long-Term Results of Percutaneous Image-Guided Radiofrequency Ablation. Radiology 2005, 234, 961–967. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Lee, J.M.; Lee, J.Y.; Kim, S.H.; Yoon, J.H.; Kim, Y.J.; Han, J.K.; Choi, B.I. Radiofrequency Ablation of Hepatocellular Carcinoma as First-Line Treatment: Long-Term Results and Prognostic Factors in 162 Patients with Cirrhosis. Vasc. Interv. Radiol. 2014, 270, 10. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Ravetta, V.; Rosa, L.; Ghittoni, G.; Viera, F.T.; Garbagnati, F.; Silini, E.M.; Dionigi, P.; Calliada, F.; Quaretti, P.; et al. Repeated Radiofrequency Ablation for Management of Patients with Cirrhosis with Small Hepatocellular Carcinomas: A Long-Term Cohort Study. Hepatol. Baltim. Md. 2011, 53, 136–147. [Google Scholar] [CrossRef]
- Kim, Y.; Lim, H.K.; Rhim, H.; Lee, M.W.; Choi, D.; Lee, W.J.; Paik, S.W.; Koh, K.C.; Lee, J.H.; Choi, M.S.; et al. Ten-Year Outcomes of Percutaneous Radiofrequency Ablation as First-Line Therapy of Early Hepatocellular Carcinoma: Analysis of Prognostic Factors. J. Hepatol. 2013, 58, 89–97. [Google Scholar] [CrossRef]
- Doyle, A.; Gorgen, A.; Muaddi, H.; Aravinthan, A.D.; Issachar, A.; Mironov, O.; Zhang, W.; Kachura, J.; Beecroft, R.; Cleary, S.P.; et al. Outcomes of Radiofrequency Ablation as First-Line Therapy for Hepatocellular Carcinoma Less than 3 Cm in Potentially Transplantable Patients. J. Hepatol. 2019, 70, 866–873. [Google Scholar] [CrossRef]
- Hermida, M.; Cassinotto, C.; Piron, L.; Aho-Glélé, S.; Guillot, C.; Schembri, V.; Allimant, C.; Jaber, S.; Pageaux, G.-P.; Assenat, E.; et al. Multimodal Percutaneous Thermal Ablation of Small Hepatocellular Carcinoma: Predictive Factors of Recurrence and Survival in Western Patients. Cancers 2020, 12, 313. [Google Scholar] [CrossRef]
- Guiu, B.; Petit, J.-M.; Loffroy, R.; Ben Salem, D.; Aho, S.; Masson, D.; Hillon, P.; Krause, D.; Cercueil, J.-P. Quantification of Liver Fat Content: Comparison of Triple-Echo Chemical Shift Gradient-Echo Imaging and in Vivo Proton MR Spectroscopy. Radiology 2009, 250, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Cardella, J.F.; Kundu, S.; Miller, D.L.; Millward, S.F.; Sacks, D. Society of Interventional Radiology Clinical Practice Guidelines. J. Vasc. Interv. Radiol. 2009, 20, S189–S191. [Google Scholar] [CrossRef] [PubMed]
- Feng, K.; Yan, J.; Li, X.; Xia, F.; Ma, K.; Wang, S.; Bie, P.; Dong, J. A Randomized Controlled Trial of Radiofrequency Ablation and Surgical Resection in the Treatment of Small Hepatocellular Carcinoma. J. Hepatol. 2012, 57, 794–802. [Google Scholar] [CrossRef] [PubMed]
- Takuma, Y.; Shota, I.; Miyatake, H.; Uematsu, S.; Okamoto, R.; Araki, Y.; Takabatake, H.; Morimoto, Y.; Yamamoto, H. Nomograms to Predict the Disease-Free Survival and Overall Survival after Radiofrequency Ablation for Hepatocellular Carcinoma. Intern. Med. 2018, 57, 457–468. [Google Scholar] [CrossRef] [PubMed]
- Wu, K.-T.; Wang, C.-C.; Lu, L.-G.; Zhang, W.-D.; Zhang, F.-J.; Shi, F.; Li, C.-X. Hepatocellular Carcinoma: Clinical Study of Long-Term Survival and Choice of Treatment Modalities. World J. Gastroenterol. 2013, 19, 3649–3657. [Google Scholar] [CrossRef]
- Zhang, W.; Jiang, L.; Yan, L.; Yang, J.; Li, B.; Wen, T.; Zeng, Y.; Wang, W.; Xu, M. Radiofrequency Ablation for HCC Patients with Multifocal Tumours Meeting the Milan Criteria: A Single-Centre Experience. Dig. Liver Dis. 2016, 48, 1485–1491. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Zhang, X.-Y.; Lu, X.; Zhai, B. Laparoscopic Microwave Ablation of Hepatocellular Carcinoma at Liver Surface: Technique Effectiveness and Long-Term Outcomes. Technol. Cancer Res. Treat. 2019, 18. [Google Scholar] [CrossRef]
- Chen, H.-Y.; Lu, S.-N.; Hung, C.-H.; Wang, J.-H.; Chen, C.-H.; Yen, Y.-H.; Kuo, Y.-H.; Kee, K.-M. Predicting Outcomes for Recurrent Hepatocellular Carcinoma within Milan Criteria after Complete Radiofrequency Ablation. PLoS ONE 2020, 15, e0242113. [Google Scholar] [CrossRef]
- Yan, K.; Chen, M.H.; Yang, W.; Wang, Y.B.; Gao, W.; Hao, C.Y.; Xing, B.C.; Huang, X.F. Radiofrequency Ablation of Hepatocellular Carcinoma: Long-Term Outcome and Prognostic Factors. Eur. J. Radiol. 2008, 67, 336–347. [Google Scholar] [CrossRef]
- Brar, G.; Greten, T.F.; Graubard, B.I.; McNeel, T.S.; Petrick, J.L.; McGlynn, K.A.; Altekruse, S.F. Hepatocellular Carcinoma Survival by Etiology: A SEER-Medicare Database Analysis. Hepatol. Commun. 2020, 4, 1541–1551. [Google Scholar] [CrossRef]
- Asaoka, Y.; Tateishi, R.; Nakagomi, R.; Kondo, M.; Fujiwara, N.; Minami, T.; Sato, M.; Uchino, K.; Enooku, K.; Nakagawa, H.; et al. Frequency of and Predictive Factors for Vascular Invasion after Radiofrequency Ablation for Hepatocellular Carcinoma. PLoS ONE 2014, 9, e111662. [Google Scholar] [CrossRef]
- Kim, P.N.; Choi, D.; Rhim, H.; Rha, S.E.; Hong, H.P.; Lee, J.; Choi, J.-I.; Kim, J.W.; Seo, J.W.; Lee, E.J.; et al. Planning Ultrasound for Percutaneous Radiofrequency Ablation to Treat Small (≤3 cm) Hepatocellular Carcinomas Detected on Computed Tomography or Magnetic Resonance Imaging: A Multicenter Prospective Study to Assess Factors Affecting Ultrasound Visibility. J. Vasc. Interv. Radiol. 2012, 23, 627–634. [Google Scholar] [CrossRef]
- Llovet, J.M.; De Baere, T.; Kulik, L.; Haber, P.K.; Greten, T.F.; Meyer, T.; Lencioni, R. Locoregional Therapies in the Era of Molecular and Immune Treatments for Hepatocellular Carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 293–313. [Google Scholar] [CrossRef] [PubMed]
- Majumdar, A.; Roccarina, D.; Thorburn, D.; Davidson, B.R.; Tsochatzis, E.; Gurusamy, K.S. Management of People with Early- or Very Early-Stage Hepatocellular Carcinoma: An Attempted Network Meta-Analysis. Cochrane Database Syst. Rev. 2017, 3, CD011650. [Google Scholar] [CrossRef]
- Centonze, L.; Di Sandro, S.; Lauterio, A.; De Carlis, R.; Frassoni, S.; Rampoldi, A.; Tuscano, B.; Bagnardi, V.; Vanzulli, A.; De Carlis, L. Surgical Resection vs. Percutaneous Ablation for Single Hepatocellular Carcinoma: Exploring the Impact of Li-RADS Classification on Oncological Outcomes. Cancers 2021, 13, 1671. [Google Scholar] [CrossRef]
- Sempokuya, T.; Wong, L.L. Ten-Year Survival and Recurrence of Hepatocellular Cancer. Hepatoma Res. 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Imamura, H.; Matsuyama, Y.; Tanaka, E.; Ohkubo, T.; Hasegawa, K.; Miyagawa, S.; Sugawara, Y.; Minagawa, M.; Takayama, T.; Kawasaki, S.; et al. Risk Factors Contributing to Early and Late Phase Intrahepatic Recurrence of Hepatocellular Carcinoma after Hepatectomy. J. Hepatol. 2003, 38, 200–207. [Google Scholar] [CrossRef]
- Tabrizian, P.; Jibara, G.; Shrager, B.; Schwartz, M.; Roayaie, S. Recurrence of Hepatocellular Cancer after Resection: Patterns, Treatments, and Prognosis. Ann. Surg. 2015, 261, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Fong, Y.; Fortner, J.; Sun, R.L.; Brennan, M.F.; Blumgart, L.H. Clinical Score for Predicting Recurrence After Hepatic Resection for Metastatic Colorectal Cancer: Analysis of 1001 Consecutive Cases. Ann. Surg. 1999, 230, 309. [Google Scholar] [CrossRef]
- Petrowsky, H.; Gonen, M.; Jarnagin, W.; Lorenz, M.; DeMatteo, R.; Heinrich, S.; Encke, A.; Blumgart, L.; Fong, Y. Second Liver Resections Are Safe and Effective Treatment for Recurrent Hepatic Metastases from Colorectal Cancer. Ann Surg 2002, 235, 9. [Google Scholar] [CrossRef]
- Aufhauser, D.D.; Sadot, E.; Murken, D.R.; Eddinger, K.; Hoteit, M.; Abt, P.L.; Goldberg, D.S.; DeMatteo, R.P.; Levine, M.H. Incidence of Occult Intrahepatic Metastasis in Hepatocellular Carcinoma Treated With Transplantation Corresponds to Early Recurrence Rates After Partial Hepatectomy. Ann. Surg. 2018, 267, 922–928. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular Carcinoma. Nat. Rev. Dis. Primer 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Villanueva, A.; Marrero, J.A.; Schwartz, M.; Meyer, T.; Galle, P.R.; Lencioni, R.; Greten, T.F.; Kudo, M.; Mandrekar, S.J.; et al. Trial Design and Endpoints in Hepatocellular Carcinoma: AASLD Consensus Conference. Hepatol. Baltim. Md 2021, 73 (Suppl. 1), 158–191. [Google Scholar] [CrossRef]
- Bolondi, L.; Burroughs, A.; Dufour, J.-F.; Galle, P.R.; Mazzaferro, V.; Piscaglia, F.; Raoul, J.L.; Sangro, B. Heterogeneity of Patients with Intermediate (BCLC B) Hepatocellular Carcinoma: Proposal for a Subclassification to Facilitate Treatment Decisions. Semin. Liver Dis. 2012, 32, 348–359. [Google Scholar] [CrossRef] [PubMed]
- Golfieri, R.; Bargellini, I.; Spreafico, C.; Trevisani, F. Patients with Barcelona Clinic Liver Cancer Stages B and C Hepatocellular Carcinoma: Time for a Subclassification. Liver Cancer 2019, 8, 78–91. [Google Scholar] [CrossRef]
- Takayasu, K.; Arii, S.; Kudo, M.; Ichida, T.; Matsui, O.; Izumi, N.; Matsuyama, Y.; Sakamoto, M.; Nakashima, O.; Ku, Y.; et al. Superselective Transarterial Chemoembolization for Hepatocellular Carcinoma. Validation of Treatment Algorithm Proposed by Japanese Guidelines. J. Hepatol. 2012, 56, 886–892. [Google Scholar] [CrossRef] [PubMed]
- Maeda, N.; Osuga, K.; Mikami, K.; Higashihara, H.; Onishi, H.; Nakaya, Y.; Tatsumi, M.; Hori, M.; Kim, T.; Tomoda, K.; et al. Angiographic Evaluation of Hepatic Arterial Damage after Transarterial Chemoembolization for Hepatocellular Carcinoma. Radiat. Med. 2008, 26, 206–212. [Google Scholar] [CrossRef] [PubMed]
- Suh, C.H.; Shin, J.H.; Yoon, H.M.; Yoon, H.-K.; Ko, G.-Y.; Gwon, D.-I.; Kim, J.-H.; Sung, K.-B. Angiographic Evaluation of Hepatic Arterial Injury after Cisplatin and Gelfoam–Based Transcatheter Arterial Chemoembolization for Hepatocellular Carcinoma in a 205 Patient Cohort during a 6-Year Follow-Up. Br. J. Radiol. 2014, 87, 20140054. [Google Scholar] [CrossRef] [PubMed]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus Bevacizumab in Unresectable Hepatocellular Carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef] [PubMed]
- Hiroishi, K.; Eguchi, J.; Baba, T.; Shimazaki, T.; Ishii, S.; Hiraide, A.; Sakaki, M.; Doi, H.; Uozumi, S.; Omori, R.; et al. Strong CD8(+) T-Cell Responses against Tumor-Associated Antigens Prolong the Recurrence-Free Interval after Tumor Treatment in Patients with Hepatocellular Carcinoma. J. Gastroenterol. 2010, 45, 451–458. [Google Scholar] [CrossRef]
- Duffy, A.G.; Ulahannan, S.V.; Makorova-Rusher, O.; Rahma, O.; Wedemeyer, H.; Pratt, D.; Davis, J.L.; Hughes, M.S.; Heller, T.; ElGindi, M.; et al. Tremelimumab in Combination with Ablation in Patients with Advanced Hepatocellular Carcinoma. J. Hepatol. 2017, 66, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Zerbini, A.; Pilli, M.; Penna, A.; Pelosi, G.; Schianchi, C.; Molinari, A.; Schivazappa, S.; Zibera, C.; Fagnoni, F.F.; Ferrari, C.; et al. Radiofrequency Thermal Ablation of Hepatocellular Carcinoma Liver Nodules Can Activate and Enhance Tumor-Specific T-Cell Responses. Cancer Res. 2006, 66, 1139–1146. [Google Scholar] [CrossRef] [PubMed]
- Mizukoshi, E.; Yamashita, T.; Arai, K.; Sunagozaka, H.; Ueda, T.; Arihara, F.; Kagaya, T.; Yamashita, T.; Fushimi, K.; Kaneko, S. Enhancement of Tumor-Associated Antigen-Specific T Cell Responses by Radiofrequency Ablation of Hepatocellular Carcinoma. Hepatol. Baltim. Md. 2013, 57, 1448–1457. [Google Scholar] [CrossRef] [PubMed]
- Hermida, M.; Preel, A.; Assenat, E.; Piron, L.; Cassinotto, C.; Ursic-Bedoya, J.; Guillot, C.; Herrero, A.; Panaro, F.; Pageaux, G.; et al. Small Steatotic HCC: A Radiological Variant Associated With Improved Outcome After Ablation. Hepatol. Commun. 2021, 5, 689–700. [Google Scholar] [CrossRef]
- Nault, J.-C.; Martin, Y.; Caruso, S.; Hirsch, T.Z.; Bayard, Q.; Calderaro, J.; Charpy, C.; Copie-Bergman, C.; Ziol, M.; Bioulac-Sage, P.; et al. Clinical Impact of Genomic Diversity From Early to Advanced Hepatocellular Carcinoma. Hepatol. Baltim. Md. 2020, 71, 164–182. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Global | Unifocal | Bifocal | Trifocal | p-Value |
| Patients | 281 | 216 | 49 | 16 | |
| Age (median (IQR) years) | 65 (59–72) | 66 (60–73) | 63 (57–69) | 58.5 (52.5–65.5) | 0.082 |
| Sex (n, %) | |||||
| Male | 225 (80.07) | 170 (78.70) | 42 (85.71) | 13 (81.25) | 0.568 |
| Female | 56 (19.93) | 46 (21.30) | 7 (14.29) | 3 (18.75) | |
| ASA score (n, %) | 0.253 | ||||
| 1–2 | 146 (51.96) | 110 (50.92) | 30 (61.22) | 6 (37.50) | |
| 3–4 | 135 (48.04) | 106 (49.08) | 19 (38.78) | 10 (62.50) | |
| Diabetes (n, %) | 0.534 | ||||
| No | 170 (60.50) | 124 (57.41) | 33 (67.35) | 13 (81.25) | |
| Yes | 111 (39.50) | 92 (42.59) | 16 (32.65) | 3 (18.75) | |
| Metformin treatment (n, %) | 52 (18.51) | 43 (19.91) | 7 (14.29) | 2 (12.50) | 0.627 |
| Statin treatment (n, %) | 49 (17.44) | 40 (18.52) | 8 (16.33) | 1 (6.25) | 0.648 |
| BMI (median (IQR) kg/m2) | 27 (24–30) | 27 (24–30) | 27 (24–31) | 27 (24–29.5) | 0.399 |
| Prior treatment for HCC (n, %) | 0.264 | ||||
| Naïve patient | 138 (49.11) | 106 (49.07) | 27 (55.10) | 5 (31.25) | |
| Yes | 143 (50.89) | 110 (50.93) | 22 (44.90) | 11 (68.75) | |
| PTA (in medical history) | 58 (20.64) | 49 (22.69) | 6 (12.24) | 3 (18.75) | |
| Liver disease | |||||
| Cirrhosis (n, %) | 1.000 | ||||
| No | 23 (8.19) | 18 (8.33) | 4 (8.16) | 1 (6.25) | |
| Yes | 258 (91.81) | 198 (91.67) | 45 (91.84) | 15 (93.75) | |
| Causes for hepatopathy (n, %) | 0.23 | ||||
| Alcohol | 115 (40.9) | 83 (38.4) | 25 (51) | 7 (43.8) | |
| Viral hepatitis or mixed | 113 (40.2) | 88 (40.7) | 19 (38.8) | 6 (37.5) | |
| NASH | 41 (14.6) | 36 (16.7) | 2 (4.1) | 3 (18.7) | |
| Hemochromatosis and others | 12 (4.3) | 9 (4.2) | 3 (6.1) | 0 (0) | |
| Steatosis (n, %) | 0.430 | ||||
| Absent | 176 (64.23) | 138 (65.71) | 30 (62.50) | 8 (50.00) | |
| Present | 98 (35.77) | 72 (34.29) | 18 (37.50) | 8 (50.00) | |
| MR quantification (median (IQR) %) | 3 (2–6) | 3 (2–6) | 3 (2–6) | 5 (3–10) | 0.547 |
| Child-Pugh class | 0.511 | ||||
| A5 | 235 (83.6) | 183 (84.7) | 39 (79.6) | 13 (81.2) | |
| A6 | 39 (13.9) | 27 (12.5) | 9 (18.4) | 3 (18.8) | |
| B7 | 7 (2.5) | 7 (3.2) | 0 (0.0) | 0 (0.0) | |
| MELD score (median (IQR)) | 8 (7–10) | 8 (7–10) | 10 (7–13) | 8.5 (8–10) | 0.144 |
| MELD score > 9 | 95 (33.81) | 68 (31.48) | 20 (40.82) | 7 (43.75) | 0.300 |
| Laboratory data (median (IQR)) | |||||
| AFP (ng/mL) | 5.2 (7.7) | 4.7 (6.3) | 7.6 (20.8) | 7.7 (12.4) | 0.094 |
| Total bilirubin (µmol/l) | 11 (10.2) | 11 (9.6) | 12 (9) | 12 (13.1) | 0.368 |
| Albumin (g/l) | 41 (6) | 41 (6) | 40 (6) | 41.5 (6.5) | 0.707 |
| Prothrombin activity (%) | 85 (23) | 86 (22) | 78 (23) | 84 (23.5) | 0.102 |
| Platelet count (×10/mm3) | 124 (91) | 132 (96) | 100.5 (116.5) | 100.5 (116.5) | 0.231 |
| Platelet count ≤ 90000/ mm3 (n, %) | 96 (34.16) | 66 (30.56) | 22 (44.90) | 8 (50.00) | 0.063 |
| Neutrophiles (×10/mm3) | 3.28 (1.63) | 3.32 (1.59) | 3.16 (1.85) | 3.65 (2.51) | 0.813 |
| Lymphocytes (×10/mm3) | 1.42 (0.91) | 1.41 (0.92) | 1.42 (0.95) | 1.65 (1.19) | 0.879 |
| Monocytes (×10/mm3) | 0.51 (0.27) | 0.52 (0.28) | 0.49 (0.22) | 0.56 (0.24) | 0.812 |
| Creatinine (µmol/L) | 75 (28) | 76.5 (29) | 71 (18.40) | 66.5 (26) | 0.057 |
| ALBI score | 0.839 | ||||
| 1 | 179 (66.54) | 139 (67.48) | 30 (63.83) | 10 (62.50) | |
| 2 | 90 (33.46) | 67 (32.52) | 17 (36.17) | 6 (37.50) | |
| HCC | |||||
| Size of the largest nodule (median (IQR) mm) | 16 (13–20) | 15 (12–20) | 17 (13–20) | 17 (16–21) | 0.099 |
| Tumor size < 20 mm (n, %) | 197 (70.11) | 154 (71.30) | 32 (65.31) | 11 (68.75) | 0.696 |
| At least one biospy-proven nodule (n, %) | 55 (19.6) | 42 (19.4) | 10 (20.4) | 3 (18.8) | 0.96 |
| Subcaspular location (n, %) | 105 (37.4) | 77 (35.7) | 23 (46.9) | 5 (31.3) | 0.31 |
| Dome location (n, %) | 70 (24.9) | 60 (27.8) | 7 (14.3) | 3 (18.8) | 0.11 |
| Peri-vascular tumor (n, %) | 64 (22.8) | 58 (26.8) | 5 (10.2) | 1 (6.3) | 0.01 |
| Steatotic HCC (n, %) | 57 (22.27) | 51 (25.63) | 4 (9.30) | 2 (14.29) | 0.046 |
| PTA | |||||
| PTA modality (n, %) | 0.857 | ||||
| Radiofrequency | 122 (43.42) | 92 (42.59) | 23 (46.94) | 7 (43.75) | |
| Microwave | 159 (56.58) | 124 (57.41) | 26 (53.06) | 9 (56.25) | |
| Imaging guidance (n, %) | 0.369 | ||||
| Ultrasonography guidance | 147 (52.31) | 119 (55.09) | 21 (42.86) | 7 (43.75) | |
| CT guidance | 130 (46.26) | 93 (43.06) | 28 (57.14) | 9 (56.25) |
| Cumulative Distant Recurrence Rate Per Year | Unifocal | Bifocal | Trifocal |
|---|---|---|---|
| 6-month | 10.7% (95% CI: 7.3–15.7) | 38.8% (95% CI: 26.8–53.8) | 50% (95% CI: 29–75.5) |
| 1-year | 21.8% (95% CI: 16.8–28.1%) | 61.9% (95% CI: 48.5–75.4%) | 68.8% (95% CI: 46.4–88.6%) |
| 2-year | 39.4% (95% CI: 32.6–47.1%) | 72.9% (95% CI: 58.9–85.2%) | 81.3% (95% CI: 59.8–95.4%) |
| 3-year | 51.1% (95% CI: 43–59.7%) | 72.9% (95% CI: 58.9–85.2%) | 81.3% (95% CI: 59.8–95.4%) |
| Characteristics of the 1st Distant Recurrence | Unifocal | Bifocal | Trifocal | p Value |
|---|---|---|---|---|
| Tumor number recurrence ≤ 3 | 64/93 (68.8%) | 29/37 (78.4%) | 9/14 (64.3%) | 0.5 |
| Portal vein invasion or extra-hepatic metastasis | 13/93 (14%) | 5/37 (13.5%) | 2/14 (14.3%) | 0.82 |
| Size of the largest nodule (mm) | 14 (11–18) | 14 (12–19) | 13 (10–16) | 0.59 |
| Alpha-foetoprotein (ng/mL) | 4.7 (3–10.3) | 7.7 (4–31.9) | 6.3 (4–13.1) | 0.49 |
| Non-Curative treatment * | 42.4% | 36.2% | 38.5% | 0.71 |
| Univariate Analysis | Multivariate Analysis | Bootstrapping (200 Replications) | ||||
|---|---|---|---|---|---|---|
| Variables | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value |
| Patients | ||||||
| Age | 1.0 (0.99–1.02) | 0.65 | ||||
| Sex female vs. male | 0.82 (0.58–1.17) | 0.28 | ||||
| Body Mass Index | 0.99 (0.96–1.02) | 0.36 | ||||
| ASA (>2 vs. ≤2) | 0.92 (0.68–1.23) | 0.56 | ||||
| Diabetes | 0.90 (0.67–1.22) | 0.52 | ||||
| Metformin treatment | 0.79 (0.51–1.22) | 0.29 | ||||
| Statin treatment | 1.05 (0.71–1.56) | 0.79 | ||||
| Treatment-naïve patient | 0.48 (0.36–0.66) | <0.001 | 0.46 (0.32–0.65) | <0.001 | 0.46 (0.31–0.67) | <0.001 |
| Cirrhosis | 1.23 (0.67–2.28) | 0.50 | ||||
| Child-Pugh (B vs. A) | 1.63 (0.79–3.36) | 0.19 | ||||
| Cause of liver disease(vs. alcohol) | ||||||
| Viral hepatitis or mixed | 0.82 (0.56–1.18) | 0.28 | ||||
| Hemochromatosis and others | 0.82 (0.38–1.76) | 0.61 | ||||
| NASH | 0.52 (0.32–0.84) | 0.007 | 0.67 (0.37–1.22) | 0.190 | 0.67 (0.34–1.32) | 0.245 |
| Steatosis | 1.09 (0.80–1.49) | 0.59 | ||||
| Laboratory Data | ||||||
| AFP ≥ 100 vs. <100 ng/mL | 3.27 (1.63–6.55) | 0.001 | 3.31 (1.87–5.87) | <0.001 | 3.31 (1.70–6.45) | <0.001 |
| AFP (per unit) | 1.0 (1.0–1.0) | <0.001 | ||||
| Prothrombin time | 1.0 (0.98–1.01) | 0.56 | ||||
| Platelet count | 1.0 (1.0–1.0) | 0.81 | ||||
| Albumin | 0.97 (0.94–1.00) | 0.057 | ||||
| Bilirubin | 1.02 (1.0–1.03) | 0.11 | ||||
| Creatinine | 1.0 (1.0–1.0) | 0.97 | ||||
| MELD (>9 vs. ≤9) | 1.17 (0.86–1.59) | 0.33 | ||||
| ALBI score 2 vs. 1 | 1.33 (0.97–1.82) | 0.07 | ||||
| HCC | ||||||
| Bifocal HCC (vs. unifocal) | 1.98 (1.27–3.06) | 0.002 | 2.46 (1.60–3.77) | <0.001 | 2.46 (1.53–3.96) | <0.001 |
| Trifocal HCC (vs. unifocal) | 2.50 (1.19–5.23) | 0.015 | 2.70 (1.16–6.29) | 0.021 | 2.70 (1.02–7.08) | 0.044 |
| Tumor size < 2 vs. ≥2 cm | 0.99 (0.73–1.35) | 0.968 | ||||
| Steatotic HCC | 0.59 (0.39–0.88) | 0.011 | 0.81 (0.52–1.26) | 0.35 | 0.81 (0.51–1.28) | 0.364 |
| PTA | ||||||
| PTA modality: MWA vs. RF | 1.1 (0.81–1.48) | 0.54 | ||||
| PTA imaging guidance: US vs. CT | 0.96 (0.71–1.30) | 0.81 | ||||
| Harrell’s C statistic: 0.69 AIC: 1256.97 | ||||||
| Overall Survival Rate Per Year | Unifocal | Bifocal | Trifocal |
|---|---|---|---|
| 1-year | 98% (95%CI: 94.8–99.2%) | 91.4% (95%CI: 78.7–96.7%) | 100% (95 CI: not evaluable) |
| 2-year | 85.3% (95%CI: 78.9–89.9%) | 81.1% (95%CI: 65.6–90.1%) | 78.6% (95%CI: 47.3–92.5%) |
| 3-year | 77.9% (95%CI: 70.3–83.9%) | 76.3% (95%CI: 58.1–87.5%) | 27.5% (95%CI: 4.4–58.6%) |
| Variables | Univariate Analysis | Multivariate Analysis | Bootstrapping (200 Replications) | |||
|---|---|---|---|---|---|---|
| Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | Hazard Ratio (95% CI) | p Value | |
| Patients | ||||||
| Age | 1.01 (0.99–1.04) | 0.25 | ||||
| Sex female vs. male | 0.67 (0.35–1.29) | 0.23 | ||||
| Body Mass Index | 1.02 (0.97–1.07) | 0.48 | ||||
| ASA (>2 vs. ≤2) | 1.79 (1.10–2.95) | 0.020 | 1.14 (0.76–2.78) | 0.25 | 1.46 (0.67–3.18) | 0.34 |
| Diabetes | 1.53 (0.94–2.48) | 0.09 | ||||
| Metformin treatment | 1.0 (0.49–2.0) | 1.0 | ||||
| Statin treatment | 1.44 (0.83–2.49) | 0.190 | ||||
| Treatment-naïve patient | 0.59 (0.36–0.98) | 0.041 | 0.42 (0.22–0.79) | 0.007 | 0.42 (0.2–0.85) | 0.017 |
| Local recurrence | 1.12 (0.65–1.93) | 0.67 | ||||
| Distant recurrence | 1.50 (0.90–2.52) | 0.12 | ||||
| Non-Transplantable Recurrence | 4.78 (2.66–8.58) | <0.001 | ||||
| Cirrhosis | 1.0 (0.46–2.1) | 0.99 | ||||
| Child-Pugh (B vs. A) | 2.24 (0.47–10.62) | 0.31 | ||||
| Cause of liver disease(vs. alcohol) | ||||||
| Viral hepatitis or mixed | 0.85 (0.47–1.53) | 0.59 | ||||
| Hemochromatosis and others | 0.24 (0.03–1.7) | 0.15 | ||||
| NASH | 0.71 (0.33–1.52) | 0.38 | ||||
| Steatosis | 1.08 (0.65–1.8) | 0.76 | ||||
| AFP ≥ 100 vs. <100 ng/mL | 4.36 (2.12–8.96) | <0.001 | 3.03 (1.33–6.91) | 0.008 | 3.03 (1.1–8.37) | 0.032 |
| AFP (per unit) | 1.002 (1.001–1.003) | <0.001 | ||||
| Prothrombin time | 0.97 (0.96–0.99) | <0.001 | ||||
| Albumin | 0.93 (0.88–0.98) | 0.006 | ||||
| Bilirubin | 1.04 (1.00–1.07) | 0.026 | ||||
| Creatinine | 1.01 (1.00–1.01) | 0.001 | ||||
| MELD (>9 vs. ≤9) | 2.28 (1.40–3.73) | 0.001 | 2.84 (1.54–5.26) | 0.001 | 2.84 (1.46–5.53) | 0.002 |
| ALBI score 2 vs. 1 | 1.48 (0.88–2.46) | 0.14 | ||||
| HCC | ||||||
| Bifocal HCC (vs. unifocal) | 1.1 (0.53–2.25) | 0.80 | 1.60 (0.69–3.72) | 0.27 | 1.60 (0.66–3.92) | 0.30 |
| Trifocal HCC (vs. unifocal) | 2.75 (1.34–5.63) | 0.006 | 3.30 (1.36–8.02) | 0.008 | 3.31 (1.15–9.49) | 0.026 |
| Tumor size <2 cm (vs. ≥2 cm) | 1.07 (0.64–1.79) | 0.790 | ||||
| Steatotic HCC | 0.18 (0.056–0.56) | 0.003 | 0.12 (0.01–0.89) | 0.038 | 0.12 (3.2 ^−18–4.3^15) | 0.912 |
| PTA | ||||||
| PTA modality: MWA vs. RF | 1.34 (0.82–2.2) | 0.24 | ||||
| PTA imaging guidance US vs. CT | 0.75 (0.48–1.24) | 0.26 | ||||
| Harrell’s C statistic: 0.79 AIC: 356.36 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Preel, A.; Hermida, M.; Allimant, C.; Assenat, E.; Guillot, C.; Gozzo, C.; Aho-Glele, S.; Pageaux, G.-P.; Cassinotto, C.; Guiu, B. Uni-, Bi- or Trifocal Hepatocellular Carcinoma in Western Patients: Recurrence and Survival after Percutaneous Thermal Ablation. Cancers 2021, 13, 2700. https://doi.org/10.3390/cancers13112700
Preel A, Hermida M, Allimant C, Assenat E, Guillot C, Gozzo C, Aho-Glele S, Pageaux G-P, Cassinotto C, Guiu B. Uni-, Bi- or Trifocal Hepatocellular Carcinoma in Western Patients: Recurrence and Survival after Percutaneous Thermal Ablation. Cancers. 2021; 13(11):2700. https://doi.org/10.3390/cancers13112700
Chicago/Turabian StylePreel, Ancelin, Margaux Hermida, Carole Allimant, Eric Assenat, Chloé Guillot, Cecilia Gozzo, Serge Aho-Glele, Georges-Philippe Pageaux, Christophe Cassinotto, and Boris Guiu. 2021. "Uni-, Bi- or Trifocal Hepatocellular Carcinoma in Western Patients: Recurrence and Survival after Percutaneous Thermal Ablation" Cancers 13, no. 11: 2700. https://doi.org/10.3390/cancers13112700
APA StylePreel, A., Hermida, M., Allimant, C., Assenat, E., Guillot, C., Gozzo, C., Aho-Glele, S., Pageaux, G.-P., Cassinotto, C., & Guiu, B. (2021). Uni-, Bi- or Trifocal Hepatocellular Carcinoma in Western Patients: Recurrence and Survival after Percutaneous Thermal Ablation. Cancers, 13(11), 2700. https://doi.org/10.3390/cancers13112700