
Complete Metabolic Response in FDG-PET-CT Scan before Discontinuation of Immune Checkpoint Inhibitors Correlates with Long Progression-Free Survival

 ,
,  ,
, 

Abstract
Simple Summary
Abstract
1. Introduction
2. Material and Methods
3. Results
3.1. Patient Baseline Characteristics
3.2. Tumor Response at Time of Treatment Discontinuation
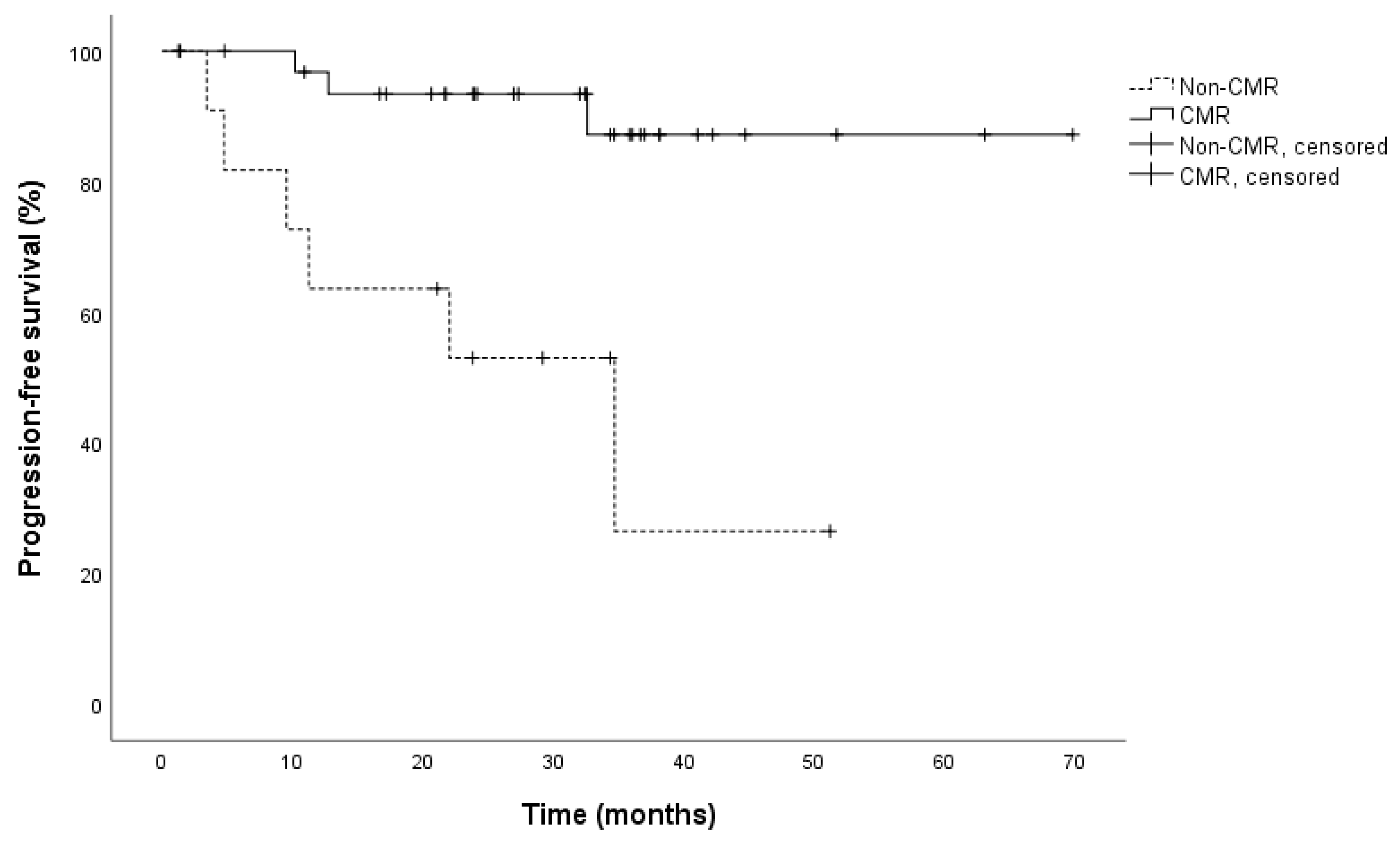
3.3. Patient Survival
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-Year Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef]
- Motzer, R.J.; Escudier, B.; McDermott, D.F.; George, S.; Hammers, H.J.; Srinivas, S.; Tykodi, S.S.; Sosman, J.A.; Procopio, G.; Plimack, E.R.; et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N. Engl. J. Med. 2015, 373, 1803–1813. [Google Scholar] [CrossRef]
- Horn, L.; Spigel, D.R.; Vokes, E.E.; Holgado, E.; Ready, N.; Steins, M.; Poddubskaya, E.; Borghaei, H.; Felip, E.; Paz-Ares, L.; et al. Nivolumab Versus Docetaxel in Previously Treated Patients With Advanced Non–Small-Cell Lung Cancer: Two-Year Outcomes From Two Randomized, Open-Label, Phase III Trials (CheckMate 017 and CheckMate 057). J. Clin. Oncol. 2017, 35, 3924–3933. [Google Scholar] [CrossRef]
- Naidoo, J.; Page, D.B.; Li, B.T.; Connell, L.C.; Schindler, K.; La Couture, M.E.; Postow, M.A.; Wolchok, J.D. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann. Oncol. 2015, 26, 2375–2391. [Google Scholar] [CrossRef] [PubMed]
- Wolchok, J.D.; Kluger, H.; Callahan, M.K.; Postow, M.A.; Rizvi, N.A.; Lesokhin, A.M.; Segal, N.H.; Ariyan, C.E.; Gordon, R.-A.; Reed, K.; et al. Nivolumab plus Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2013, 369, 122–133. [Google Scholar] [CrossRef] [PubMed]
- Nardin, C.; Dalle, S.; Leccia, M.T.; Mortier, L.; Dalac-Rat, S.; Dutriaux, C.; Legoupil, D.; Montaudie, H.; Dereure, O.; De Quatrebarbes, J.; et al. Long-term immune-related adverse events under PD-1 inhibitors: A multicenter prospective cohort study (MELBASE). J. Clin. Oncol. 2020, 38, 10057. [Google Scholar] [CrossRef]
- Long, G.V.; Schachter, J.; Ribas, A.; Arance, A.M.; Grob, J.-J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.M.; Lotem, M.; et al. 4-year survival and outcomes after cessation of pembrolizumab (pembro) after 2-years in patients (pts) with ipilimumab (ipi)-naive advanced melanoma in KEYNOTE-006. J. Clin. Oncol. 2018, 36, 9503. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Hamid, O.; Daud, A.; Wolchok, J.D.; Joshua, A.M.; Hwu, W.-J.; Weber, J.S.; Gangadhar, T.C.; Joseph, R.W.; et al. Durable complete response after discontinuation of pembrolizumab in patients With Metastatic Melanoma. J. Clin. Oncol. 2018, 36, 1668–1674. [Google Scholar] [CrossRef] [PubMed]
- Sachpekidis, C.; Kopp-Schneider, A.; Pan, L.; Papamichail, D.; Haberkorn, U.; Hassel, J.C.; Dimitrakopoulou-Strauss, A. Interim [18F]FDG PET/CT can predict response to anti-PD-1 treatment in metastatic melanoma. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 1932–1943. [Google Scholar] [CrossRef] [PubMed]
- Dimitrakopoulou-Strauss, A. Monitoring of patients with metastatic melanoma treated with immune checkpoint inhibitors using PET–CT. Cancer Immunol. Immunother. 2019, 68, 813–822. [Google Scholar] [CrossRef]
- Young, H.; Baum, R.; Cremerius, U.; Herholz, K.; Hoekstra, O.; Lammertsma, A.; Pruim, J.; Price, P. Measurement of clinical and subclinical tumour response using [18F]-fluorodeoxyglucose and positron emission tomography: Review and 1999 EORTC recommendations. Eur. J. Cancer 1999, 35, 1773–1782. [Google Scholar] [CrossRef]
- Anwar, H.; Sachpekidis, C.; Winkler, J.; Kopp-Schneider, A.; Haberkorn, U.; Hassel, J.C.; Dimitrakopoulou-Strauss, A. Absolute number of new lesions on 18F-FDG PET/CT is more predictive of clinical response than SUV changes in metastatic melanoma patients receiving ipilimumab. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Volckmar, A.-L.; Endris, V.; Gaida, M.M.; Leichsenring, J.; Stögbauer, F.; Allgäuer, M.; Von Winterfeld, M.; Penzel, R.; Kirchner, M.; Brandt, R.; et al. Next generation sequencing of the cellular and liquid fraction of pancreatic cyst fluid supports discrimination of IPMN from pseudocysts and reveals cases with multiple mutated driver clones: First findings from the prospective ZYSTEUS biomarker study. Genes Chromosom. Cancer 2018, 58, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Jesinghaus, M.; Pfarr, N.; Endris, V.; Kloor, M.; Volckmar, A.-L.; Brandt, R.; Herpel, E.; Muckenhuber, A.; Lasitschka, F.; Schirmacher, P.; et al. Genotyping of colorectal cancer for cancer precision medicine: Results from the IPH Center for Molecular Pathology. Genes Chromosom. Cancer 2016, 55, 505–521. [Google Scholar] [CrossRef] [PubMed]
- Ladwa, R.; Atkinson, V. The cessation of anti-PD-1 antibodies of complete responders in metastatic melanoma. Melanoma Res. 2017, 27, 168–170. [Google Scholar] [CrossRef]
- Jansen, Y.; Rozeman, E.; Mason, R.; Goldinger, S.; Foppen, M.G.; Hoejberg, L.; Schmidt, H.; van Thienen, J.; Haanen, J.; Tiainen, L.; et al. Discontinuation of anti-PD-1 antibody therapy in the absence of disease progression or treatment limiting toxicity: Clinical outcomes in advanced melanoma. Ann. Oncol. 2019, 30, 1154–1161. [Google Scholar] [CrossRef]
- Tan, A.C.; Emmett, L.; Lo, S.; Liu, V.; Kapoor, R.; Carlino, M.S.; Guminski, A.D.; Long, G.V.; Menzies, A.M. FDG-PET response and outcome from anti-PD-1 therapy in metastatic melanoma. Ann. Oncol. 2018, 29, 2115–2120. [Google Scholar] [CrossRef]
- Robert, C.; Ribas, A.; Schachter, J.; Arance, A.; Grob, J.-J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.M.; Lotem, M.; et al. Pembrolizumab versus ipilimumab in advanced melanoma (KEYNOTE-006): Post-hoc 5-year results from an open-label, multicentre, randomised, controlled, phase 3 study. Lancet Oncol. 2019, 20, 1239–1251. [Google Scholar] [CrossRef]
- Warner, A.B.; Palmer, J.S.; Shoushtari, A.N.; Goldman, D.A.; Panageas, K.S.; Hayes, S.A.; Bajwa, R.; Momtaz, P.; Callahan, M.K.; Wolchok, J.D.; et al. Long-Term Outcomes and Responses to Retreatment in Patients with Melanoma Treated with PD-1 Blockade. J. Clin. Oncol. 2020, 38, 1655–1663. [Google Scholar] [CrossRef]
- Hassel, J.C. 5-year results for pembrolizumab treatment of advanced melanoma. Lancet Oncol. 2019, 20, 1187–1189. [Google Scholar] [CrossRef]
- Huynh, K.; Hoon, D.S. Liquid biopsies for assessing metastatic melanoma progression. Crit. Rev. Oncog. 2016, 21, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Gray, E.S.; Rizos, H.; Reid, A.L.; Boyd, S.C.; Pereira, M.R.; Lo, J.; Tembe, V.; Freeman, J.; Lee, J.H.; Scolyer, R.A.; et al. Circulating tumor DNA to monitor treatment response and detect acquired resistance in patients with metastatic melanoma. Oncotarget 2015, 6, 42008–42018. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Long, G.; Larkin, J.; Wolchok, J.; Hassel, J.; Schadendorf, D.; Hodi, F.; Lebbé, C.; Grob, J.-J.; Grossmann, K.; et al. 1082MO 5-year characterization of complete responses in patients with advanced melanoma who received nivolumab plus ipilimumab (NIVO+IPI) or NIVO alone. Ann. Oncol. 2020, 31, S734–S735. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Characteristics | CMR Group | Non-CMR Group | All Patients | p-Value |
|---|---|---|---|---|
| (n = 32) | (n = 13) | (n = 45) | ||
| Age (years) | 0.94 | |||
| Median | 66 | 62 | 64 | |
| Range | 34–84 | 47–96 | 34–96 | |
| Sex | 0.734 | |||
| Female | 13 (40%) | 6 (46%) | 19 (42%) | |
| Male | 19 (60%) | 7 (54%) | 26 (58%) | |
| BRAF mutation | 17 (53%) | 1 (8%) | 18 (40%) | 0.004 |
| BRAF V600E | 13 (41%) | 1 (8%) | 14 (31%) | |
| BRAF V600K | 3 (9%) | – | 3 (7%) | |
| BRAF K601E | 1 (3%) | – | 1 (2%) | |
| Wild type | 15 (47%) | 11 (84%) | 26 (58%) | |
| Missing | – | 1 (8%) | 1 (2%) | |
| NRAS mutation | 0.484 | |||
| p.Q61(R/K/L) | 5 (15%) | 3 (24%) | 8 (18%) | |
| Wild type | 27 (85%) | 9 (68%) | 36 (80%) | |
| Missing | – | 1 (8%) | 1 (2%) | |
| S100 at start of treatment | 0.019 | |||
| Elevated | 14 (44%) | 1 (8%) | 15 (33%) | |
| Normal | 14 (44%) | 10 (77%) | 24 (53%) | |
| Missing | 4 (12%) | 2 (15%) | 6 (14%) | |
| S100 at time of FDG-PET-CT scan | 0.292 | |||
| Elevated | 2 (6%) | – | 2 (4%) | |
| Normal | 24 (75%) | 8 (62%) | 32 (71%) | |
| Missing | 6 (19%) | 5 (38%) | 11 (25%) | |
| LDH at start of treatment | 0.752 | |||
| Elevated | 6 (19%) | 2 (15%) | 8 (18%) | |
| Normal | 26 (81%) | 11 (85%) | 37 (82%) | |
| Missing | – | – | – | |
| LDH at time of FDG-PET-CT scan | 0.024 | |||
| Elevated | – | 2 (16%) | 2 (4%) | |
| Normal | 31 (97%) | 10 (76%) | 41 (92%) | |
| Missing | 1 (3%) | 1 (8%) | 2 (4%) | |
| Therapy | 0.502 | |||
| PD-1 antibody | 23 (72%) | 8 (61%) | 31 (69%) | |
| Ipilimumab | 3 (9%) | 1 (8%) | 4 (9%) | |
| Ipilimumab + nivolumab | 6 (19%) | 4 (31%) | 10 (22%) | |
| Prior systemic therapy | 15 (47%) | 5 (38%) | 20 (44%) | 0.607 |
| ICI | 12 (38%) | 5 (38%) | 17 (38%) | |
| Targeted therapy | 5 (16%) | – | 5 (11%) | |
| Chemotherapy | 3 (9%) | 1 (8%) | 4 (9%) | |
| Study treatment | 3 (9%) | – | 3 (7%) | |
| Duration of treatment (months) | 0.468 | |||
| Median | 22 | 16 | 21 | |
| Range | 1–42 | 1–34 | 1–42 | |
| Follow-up (months) | 0.764 | |||
| Median | 34 | 33 | 34 | |
| Range | 5–70 | 1–57 | 1–70 | |
| Reason for discontinuation | ||||
| Wish of patient | 22 (69%) | 5 (38%) | 27 (60%) | |
| irAEs | 9 (28%) | 7 (54%) | 16 (36%) | |
| Secondary malignancies | 1 (3%) | 1 (8%) | 2 (4%) | |
| Disease progression | 3/32 (9%) | 6/13 (46%) | 9/45 (20%) | 0.007 |
| Characteristic | All Patients | Patients with Preceding CT/MRI Imaging | |
|---|---|---|---|
| n = 45 | n = 17 | ||
| FDG-PET-CT Response | FDG-PET-CT Response | CT/MRI Response | |
| CMR | 32/45 (71%) | CMR 15/17 (88%) | CR 10/17 (59%) |
| Non-CMR | 13/45 (29%) * | Non-CMR 2/17 (12%) * | PR 6/17 (35%) |
| SD 1/17 (6%) | |||
| Patient Characteristic | Univariable Cox Regression Analysis | |
|---|---|---|
| HR (95% CI) | p-Value | |
| Age (years) | 1.2 (0.3–4.6) | 0.746 |
| Sex (male compared with female) | 0.8 (0.2–3.1) | 0.720 |
| BRAF (mutation compared with wild type) | 2.6 (0.5–12.7) | 0.230 |
| NRAS (mutation compared with wild type) | 31.4 (0.1–26,703.8) | 0.316 |
| S100 baseline (normal compared with elevated) | 1.1 (0.3–4.4) | 0.889 |
| S100 time of PET-CT (normal compared with elevated) | 21.2 (0.0–27,689,946,664.3) | 0.775 |
| LDH baseline (normal compared with elevated) | 0.7 (0.2–3.6) | 0.706 |
| LDH time of PET-CT (normal compared with elevated) | 20.9 (0.0–12,520,603,321.5) | 0.768 |
| Therapy (anti-PD-1 compared with ipi ± nivo) | 0.9 (0.2–3.9) | 0.974 |
| Prior systemic therapy (yes compared with no) | 1.4 (0.3–5.6) | 0.651 |
| Metabolic response (CMR compared to non-CMR) | 7.9 (1.9–31.7) | 0.004 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schank, T.E.; Forschner, A.; Sachse, M.M.; Dimitrakopoulou-Strauss, A.; Sachpekidis, C.; Stenzinger, A.; Volckmar, A.-L.; Enk, A.; Hassel, J.C. Complete Metabolic Response in FDG-PET-CT Scan before Discontinuation of Immune Checkpoint Inhibitors Correlates with Long Progression-Free Survival. Cancers 2021, 13, 2616. https://doi.org/10.3390/cancers13112616
Schank TE, Forschner A, Sachse MM, Dimitrakopoulou-Strauss A, Sachpekidis C, Stenzinger A, Volckmar A-L, Enk A, Hassel JC. Complete Metabolic Response in FDG-PET-CT Scan before Discontinuation of Immune Checkpoint Inhibitors Correlates with Long Progression-Free Survival. Cancers. 2021; 13(11):2616. https://doi.org/10.3390/cancers13112616
Chicago/Turabian StyleSchank, Timo E., Andrea Forschner, Michael Max Sachse, Antonia Dimitrakopoulou-Strauss, Christos Sachpekidis, Albrecht Stenzinger, Anna-Lena Volckmar, Alexander Enk, and Jessica C. Hassel. 2021. "Complete Metabolic Response in FDG-PET-CT Scan before Discontinuation of Immune Checkpoint Inhibitors Correlates with Long Progression-Free Survival" Cancers 13, no. 11: 2616. https://doi.org/10.3390/cancers13112616
APA StyleSchank, T. E., Forschner, A., Sachse, M. M., Dimitrakopoulou-Strauss, A., Sachpekidis, C., Stenzinger, A., Volckmar, A.-L., Enk, A., & Hassel, J. C. (2021). Complete Metabolic Response in FDG-PET-CT Scan before Discontinuation of Immune Checkpoint Inhibitors Correlates with Long Progression-Free Survival. Cancers, 13(11), 2616. https://doi.org/10.3390/cancers13112616