
Differential Prognosis and Response of Denovo vs. Secondary Muscle-Invasive Bladder Cancer: An Updated Systematic Review and Meta-Analysis

 ,
, 
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Inclusion and Exclusion Criteria
2.2.1. Inclusion Criteria: Studies
- Conducted in patients diagnosed with bladder cancer.
- That assessed the prognostic differences between patients with primMIBC and
- Those with secMIBC who have undergone RC with or without NAC.
- With no less than 10 patients in each group.
- That directly reported the hazard ratio (HR) with 95% confidence interval (CI) or in which the reported data allow for calculation of the HR were included in the analysis.
2.2.2. Exclusion Criteria
2.3. Data Extraction
2.4. Methodological Quality Assessment
2.5. Statistical Analysis
3. Results
3.1. Study Characteristics
3.2. Patients’ Characteristics
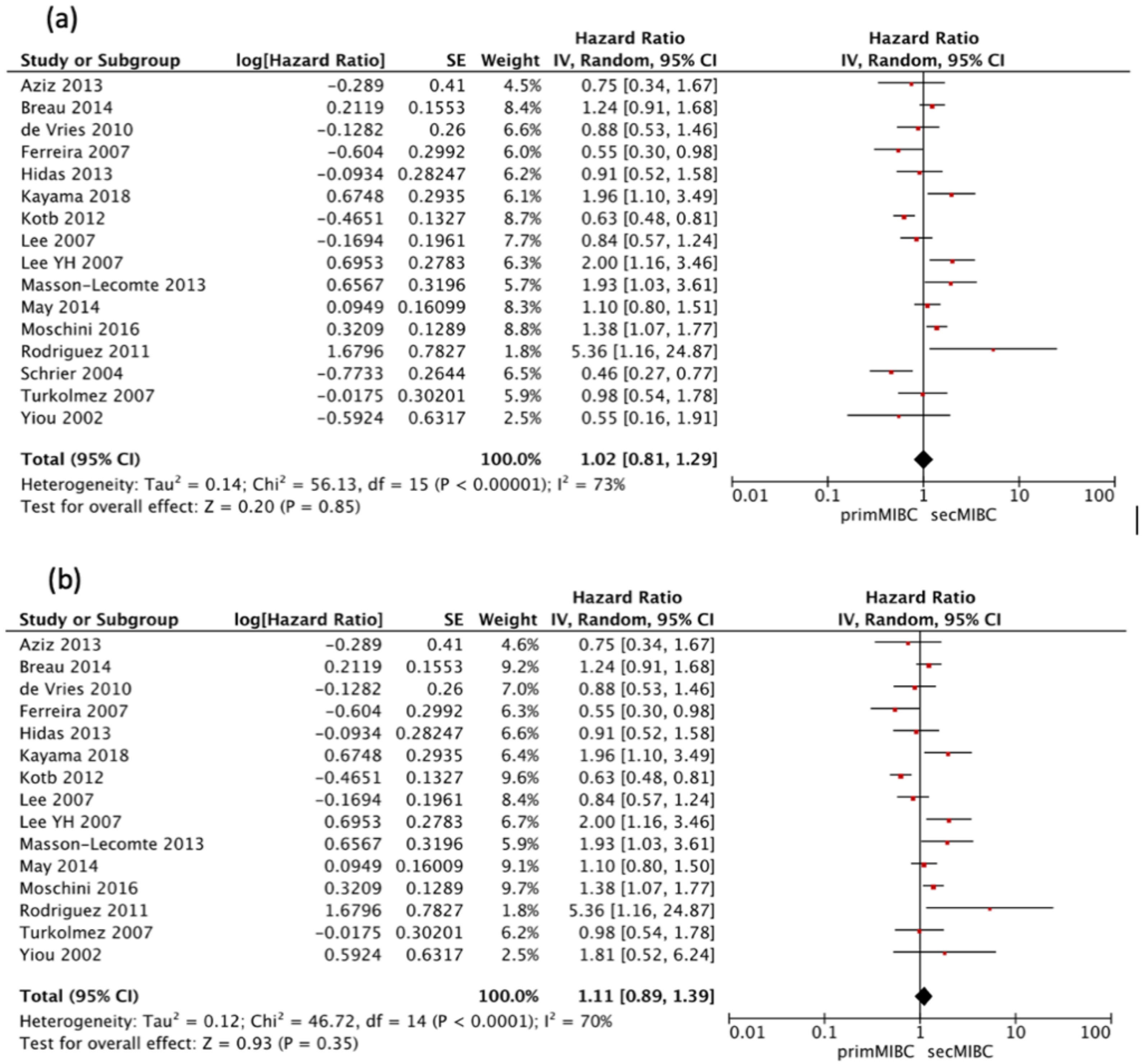
3.3. Overall Survival
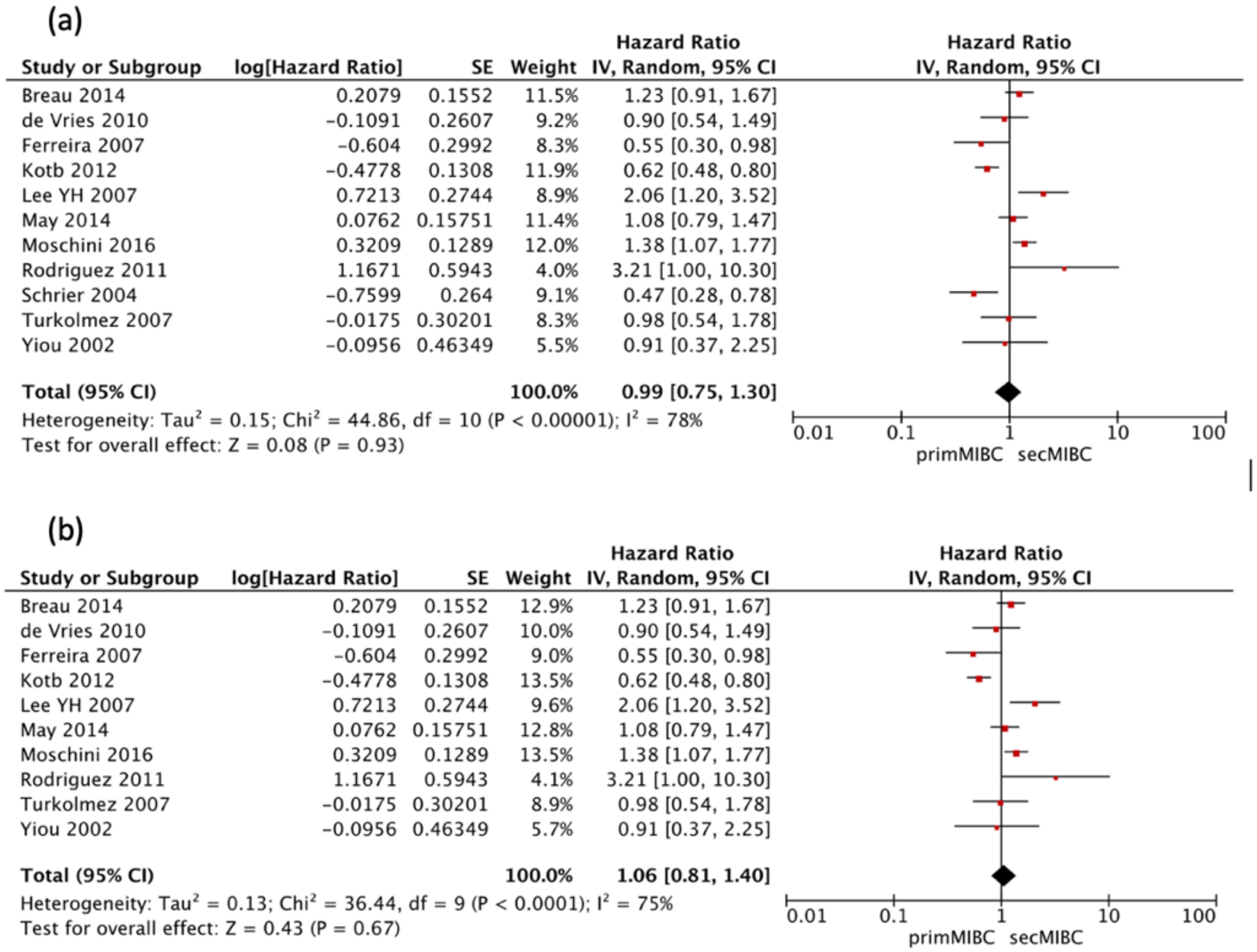
3.4. Cancer-Specific Survival
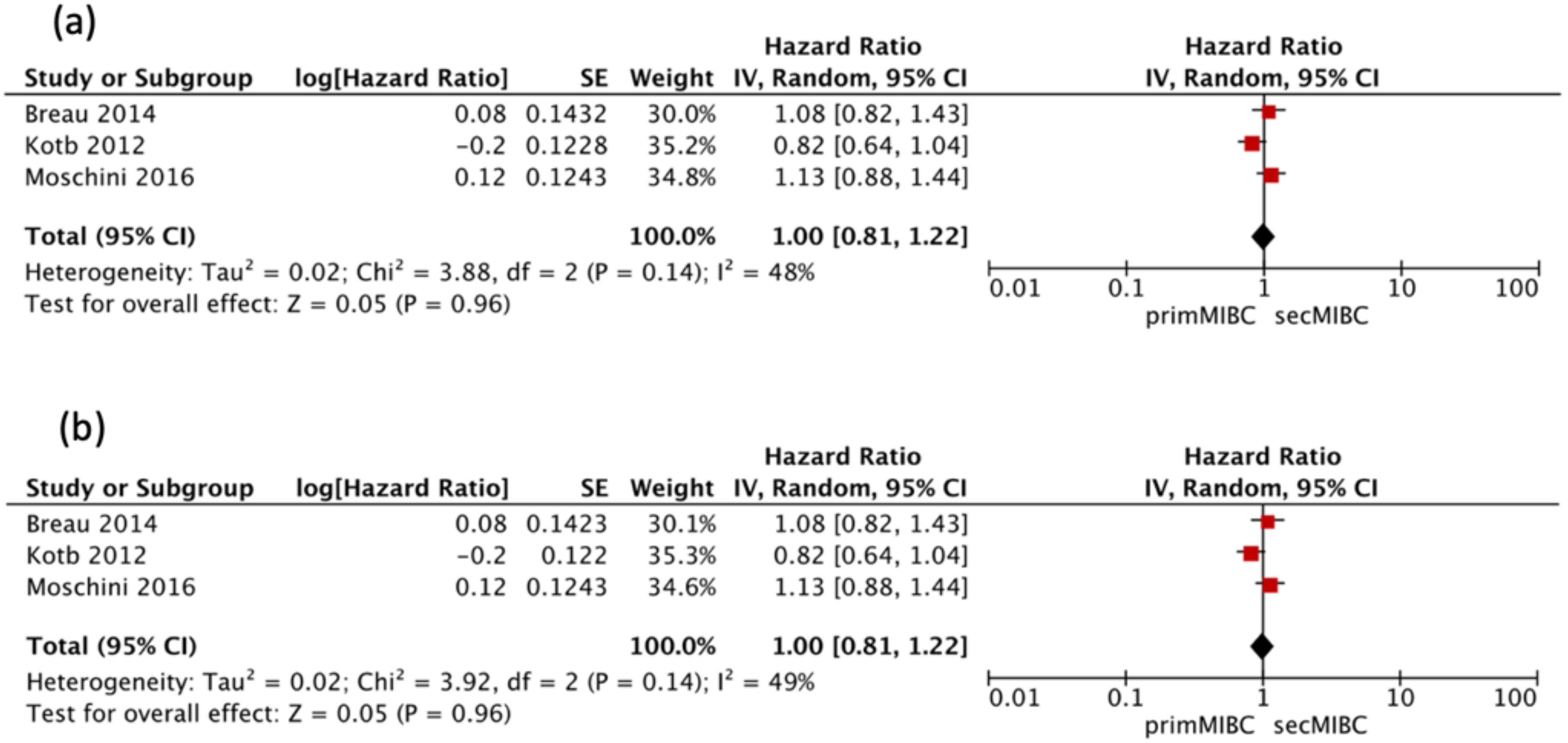
3.5. Progression Free Survival
3.6. Quality Assessment
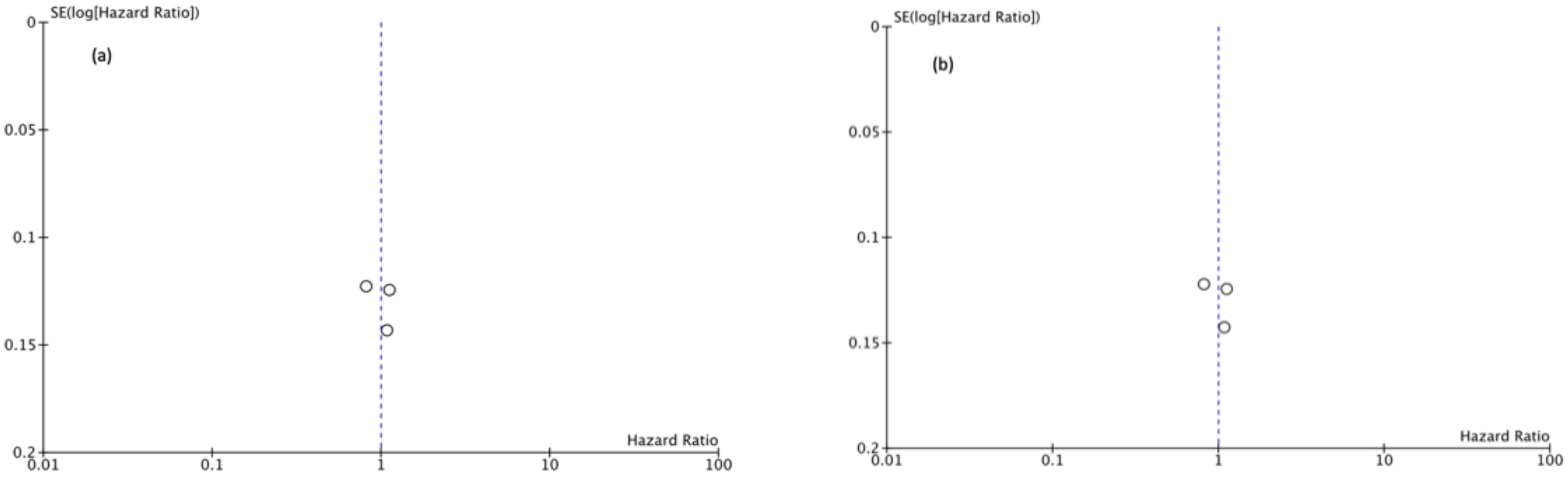
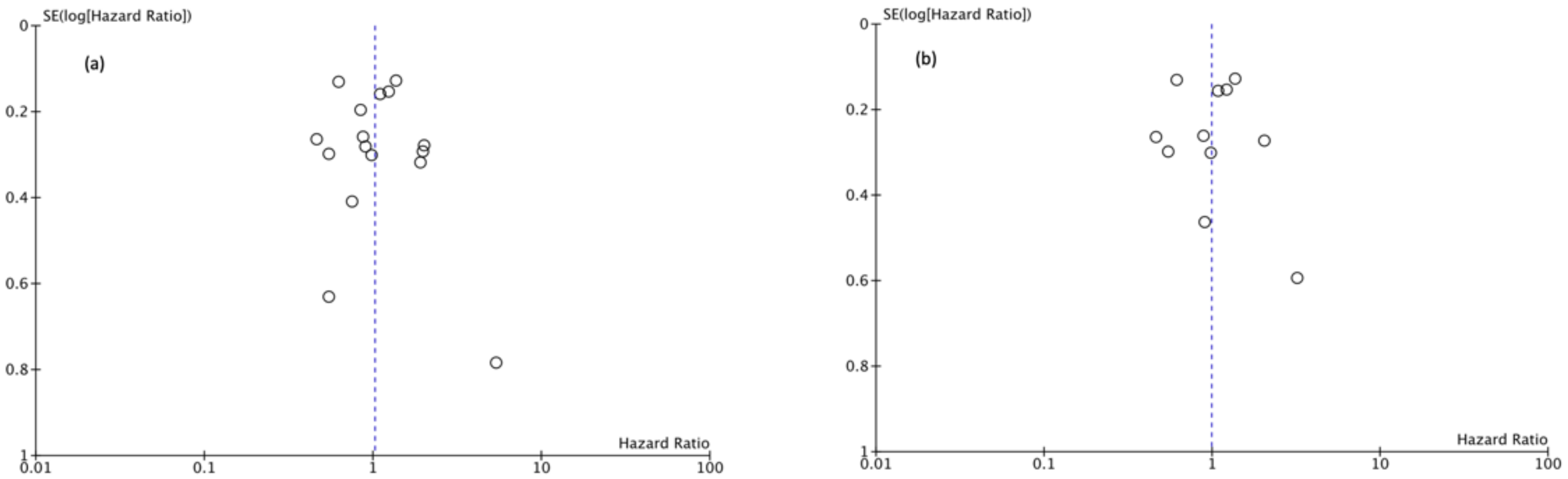
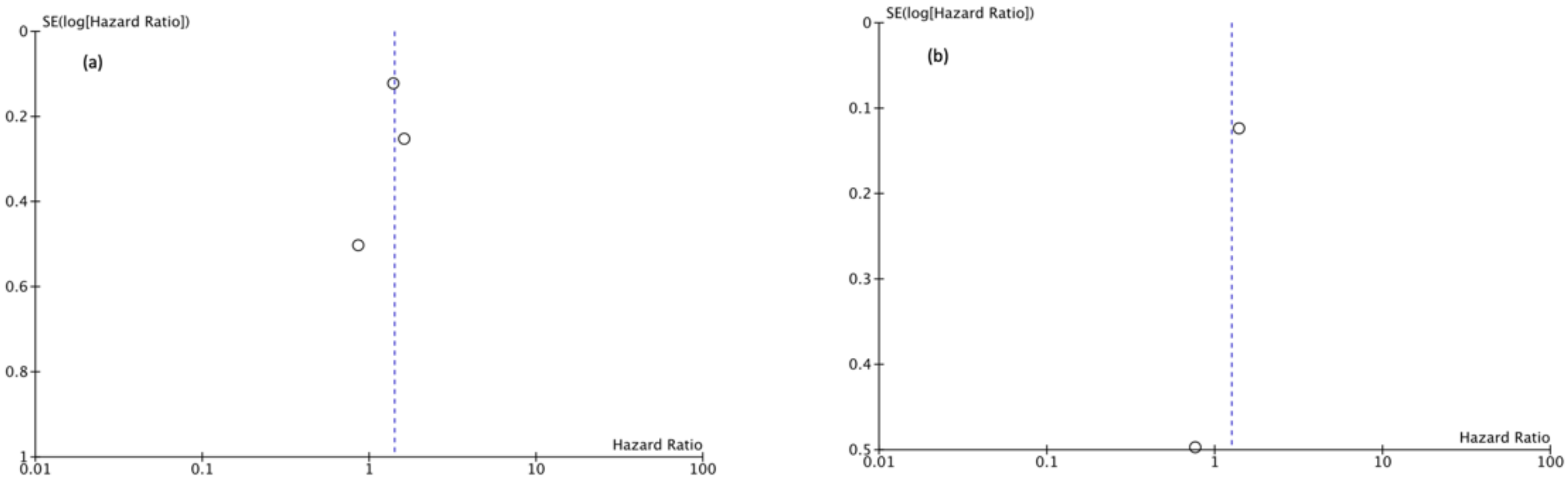
3.7. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cumberbatch, M.G.K.; Jubber, I.; Black, P.C.; Esperto, F.; Figueroa, J.D.; Kamat, A.M.; Kiemeney, L.; Lotan, Y.; Pang, K.; Silverman, D.T.; et al. Epidemiology of Bladder Cancer: A Systematic Review and Contemporary Update of Risk Factors in 2018. Eur. Urol. 2018, 74, 784–795. [Google Scholar] [CrossRef] [PubMed]
- Compérat, E.; Larré, S.; Rouprêt, M.; Neuzillet, Y.; Pignot, G.; Quintens, H.; Houede, N.; Roy, C.; Durand, X.; Varinot, J.; et al. Clinicopathological characteristics of urothelial bladder cancer in patients less than 40 years old. Virchows Arch. 2015, 466, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Babjuk, M.; Burger, M.; Compérat, E.M.; Gontero, P.; Mostafid, A.H.; Palou, J.; van Rhijn, B.W.; Rouprêt, M.; Shariat, S.F.; Sylvester, R.; et al. European Association of Urology Guidelines on Non-muscle-invasive Bladder Cancer (TaT1 and Carcinoma In Situ)-2019 Update. Eur. Urol. 2019, 76, 639–657. [Google Scholar] [CrossRef]
- Breau, R.H.; Karnes, R.J.; Farmer, S.A.; Thapa, P.; Cagiannos, I.; Morash, C.; Frank, I. Progression to detrusor muscle invasion during urothelial carcinoma surveillance is associated with poor prognosis. BJU Int. 2013, 113, 900–906. [Google Scholar] [CrossRef]
- Sylvester, R.J.; van der Meijden, A.P.; Oosterlinck, W.; Witjes, J.A.; Bouffioux, C.; Denis, L.; Newling, D.W.; Kurth, K. Predicting Recurrence and Progression in Individual Patients with Stage Ta T1 Bladder Cancer Using EORTC Risk Tables: A Combined Analysis of 2596 Patients from Seven EORTC Trials. Eur. Urol. 2006, 49, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Schrier, B.P.; Hollander, M.P.; van Rhijn, B.W.; Kiemeney, L.A.; Witjes, J.A. Prognosis of Muscle-Invasive Bladder Cancer: Difference between Primary and Progressive Tumours and Implications for Therapy. Eur. Urol. 2004, 45, 292–296. [Google Scholar] [CrossRef]
- Moschini, M.; Sharma, V.; Dell’Oglio, P.; Cucchiara, V.; Gandaglia, G.; Cantiello, F.; Zattoni, F.; Pellucchi, F.; Briganti, A.; Damiano, R.; et al. Comparing long-term outcomes of primary and progressive carcinoma invading bladder muscle after radical cystectomy. BJU Int. 2015, 117, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.H.; Cho, K.S.; Hong, S.J. The Difference in the Prognosis and Characteristics between the Progressive and Primary Muscle-invasive Bladder Cancer Treated with Radical Cystectomy. Korean J. Urol. 2007, 48, 1109–1115. [Google Scholar] [CrossRef]
- Kotb, A.F.; Kovac, E.; Kassouf, W.; Chin, J.; Fradet, Y.; Izawa, J.; Estey, E.; Fairey, A.; Rendon, R.; Cagiannos, I.; et al. Radical cystectomy for clinically muscle invasive bladder cancer: Does prior non-invasive disease affect clinical outcomes? World J. Urol. 2012, 30, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Hidas, G.; Pode, D.; Shapiro, A.; Katz, R.; Appelbaum, L.; Pizov, G.; Zorn, K.C.; Landau, E.H.; Duvdevani, M.; Gofrit, O.N. The natural history of secondary muscle-invasive bladder cancer. BMC Urol. 2013, 13, 23. [Google Scholar] [CrossRef]
- Kayama, E.; Kikuchi, E.; Fukumoto, K.; Shirotake, S.; Miyazaki, Y.; Hakozaki, K.; Kaneko, G.; Yoshimine, S.; Tanaka, N.; Takahiro, M.; et al. History of Non–Muscle-Invasive Bladder Cancer May Have a Worse Prognostic Impact in cT2-4aN0M0 Bladder Cancer Patients Treated With Radical Cystectomy. Clin. Genitourin. Cancer 2018, 16, e969–e976. [Google Scholar] [CrossRef] [PubMed]
- Türkölmez, K.; Tokgöz, H.; Reşorlu, B.; Köse, K.; Bedük, Y. Muscle-Invasive Bladder Cancer: Predictive Factors and Prognostic Difference Between Primary and Progressive Tumors. Urology 2007, 70, 477–481. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, U.; Matheus, W.E.; Pedro, R.N.; D’Ancona, C.A.L.; Reis, L.O.; Stopiglia, R.M.; Denardi, F.; Netto, J.N.R.; Zequi, S.D.C.; Da Fonseca, F.P.; et al. Primary Invasive versus Progressive Invasive Transitional Cell Bladder Cancer: Multicentric Study of Overall Survival Rate. Urol. Int. 2007, 79, 200–203. [Google Scholar] [CrossRef]
- Aziz, A.; Gierth, M.; Fritsche, H.; May, M.; Otto, W.; Denzinger, S.; Wieland, W.; Merseburger, A.; Riedmiller, H.; Kocot, A.; et al. Oncological Outcome of Primary versus Secondary Muscle-Invasive Bladder Cancer Is Comparable after Radical Cystectomy. Urol. Int. 2013, 91, 97–102. [Google Scholar] [CrossRef] [PubMed]
- De Vries, R.; Nieuwenhuijzen, J.; Vincent, A.; Van Tinteren, H.; Horenblas, S. Survival after cystectomy for invasive bladder cancer. Eur. J. Surg. Oncol. (EJSO) 2010, 36, 292–297. [Google Scholar] [CrossRef]
- Yiou, R.; Patard, J.-J.; Benhard, H.; Abbou, C.-C.; Chopin, D. Outcome of radical cystectomy for bladder cancer according to the disease type at presentation. BJU Int. 2002, 89, 374–378. [Google Scholar] [CrossRef]
- May, M.; Helke, C.; Nitzke, T.; Vogler, H.; Hoschke, B. Survival Rates after Radical Cystectomy according to Tumor Stage of Bladder Carcinoma at First Presentation. Urol. Int. 2004, 72, 103–111. [Google Scholar] [CrossRef]
- Lee, C.T.; Dunn, R.L.; Ingold, C.; Montie, J.E.; Wood, D.P. Early-Stage Bladder Cancer Surveillance Does Not Improve Survival If High-Risk Patients Are Permitted to Progress to Muscle Invasion. Urology 2007, 69, 1068–1072. [Google Scholar] [CrossRef]
- Jäger, W.; Thomas, C.; Haag, S.; Hampel, C.; Salzer, A.; Thüroff, J.W.; Wiesner, C. Early vs delayed radical cystectomy for ‘high-risk’ carcinoma not invading bladder muscle: Delay of cystectomy reduces cancer-specific survival. BJU Int. 2011, 108, E284–E288. [Google Scholar] [CrossRef]
- Pietzak, E.J.; Zabor, E.C.; Bagrodia, A.; Armenia, J.; Hu, W.; Zehir, A.; Funt, S.; Audenet, F.; Barron, D.; Maamouri, N.; et al. Genomic Differences Between “Primary” and “Secondary” Muscle-invasive Bladder Cancer as a Basis for Disparate Outcomes to Cisplatin-based Neoadjuvant Chemotherapy. Eur. Urol. 2019, 75, 231–239. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred Reporting Items for Systematic Reviews and Meta Analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 6. [Google Scholar] [CrossRef] [PubMed]
- Parmar, M.K.; Torri, V.; Stewart, L. Extracting summary statistics to perform meta-analyses of the published literature for sur-vival endpoints. Stat. Med. 1998, 17, 2815–2834. [Google Scholar] [CrossRef]
- Masson-Lecomte, A.; Vordos, D.; Yiou, R.; Allory, Y.; Abbou, C.; De La Taille, A.; Salomon, L. 1621 Oncological Outcome of Radical Cystectomy for Bcg Failure Compared to Primary Invasive Disease. J. Urol. 2013, 189, e735. [Google Scholar] [CrossRef]
- Faba, O.R.; Palou, J.; Rosales, A.; Breda, A.; Algaba, F.; Urdaneta, G.; Villavicencio, H. Clinical Predictive Factors of Poor Outcome in Patients with Stage pT0 Disease at Radical Cystectomy. J. Urol. 2011, 186, 442–447. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, H.; Sun, G.; Zhang, X.; Zhao, J.; Liu, J.; Shen, P.; Shi, M.; Zeng, H. Comparison of the prognosis of primary and progressive muscle-invasive bladder cancer after radical cystectomy: A systematic review and meta-analysis. Int. J. Surg. 2018, 52, 214–220. [Google Scholar] [CrossRef] [PubMed]
- Ge, P.; Wang, L.; Lü, M.; Mao, L.; Li, W.; Wen, R.; Lin, J.; Wang, J.; Chen, J. Oncological Outcome of Primary and Secondary Muscle-Invasive Bladder Cancer: A Systematic Review and Meta-analysis. Sci. Rep. 2018, 8, 7543. [Google Scholar] [CrossRef] [PubMed]
- Fahmy, N.M.; Mahmud, S.; Aprikian, A.G. Delay in the Surgical Treatment of Bladder Cancer and Survival: Systematic Review of the Literature. Eur. Urol. 2006, 50, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- May, M.; Nitzke, T.; Helke, C.; Vogler, H.; Hoschke, B. Significance of the time period between diagnosis of muscle invasion and radical cystectomy with regard to the prognosis of transitional cell carcinoma of the urothelium in the bladder. Scand. J. Urol. Nephrol. 2004, 38, 231–235. [Google Scholar] [CrossRef]
- Lee, C.T.; Madii, R.; Daignault, S.; Dunn, R.L.; Zhang, Y.; Montie, J.E.; Wood, D.P. Cystectomy Delay More Than 3 Months from Initial Bladder Cancer Diagnosis Results in Decreased Disease Specific and Overall Survival. J. Urol. 2006, 175, 1262–1267. [Google Scholar] [CrossRef]
- Gore, J.L.; Lai, J.; Setodji, C.M.; Litwin, M.S.; Saigal, C.S.; Project, T.U.D.I.A. Mortality increases when radical cystectomy is delayed more than 12 weeks. Cancer 2009, 115, 988–996. [Google Scholar] [CrossRef] [PubMed]
- May, M.; Burger, M.; Brookman-May, S.; Stief, C.G.; Fritsche, H.-M.; Roigas, J.; Zacharias, M.; Bader, M.; Mandel, P.; Gilfrich, C.; et al. EORTC Progression Score Identifies Patients at High Risk of Cancer-Specific Mortality After Radical Cystectomy for Secondary Muscle-Invasive Bladder Cancer. Clin. Genitourin. Cancer 2014, 12, 278–286. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.P.; Lieskovsky, G.; Cote, R.; Groshen, S.; Feng, A.-C.; Boyd, S.; Skinner, E.; Bochner, B.; Thangathurai, D.; Mikhail, M.; et al. Radical Cystectomy in the Treatment of Invasive Bladder Cancer: Long-Term Results in 1054 Patients. J. Clin. Oncol. 2001, 19, 666–675. [Google Scholar] [CrossRef] [PubMed]
- Birkmeyer, J.D.; Siewers, A.E.; Finlayson, E.V.; Stukel, T.A.; Lucas, F.L.; Batista, I.; Welch, H.G.; Wennberg, D.E. Hospital Volume and Surgical Mortality in the United States. N. Engl. J. Med. 2002, 346, 1128–1137. [Google Scholar] [CrossRef]
- Winters, B.R.; Wright, J.L.; Holt, S.K.; Dash, A.; Gore, J.L.; Schade, G.R. Health Related Quality of Life Following Radical Cystectomy: Comparative Analysis from the Medicare Health Outcomes Survey. J. Urol. 2018, 199, 669–675. [Google Scholar] [CrossRef] [PubMed]
- Catto, J.W.; Downing, A.; Mason, S.; Wright, P.; Absolom, K.; Bottomley, S.; Hounsome, L.; Hussain, S.; Varughese, M.; Raw, C.; et al. Quality of Life After Bladder Cancer: A Cross-sectional Survey of Patient-reported Outcomes. Eur. Urol. 2021, 79, 621–632. [Google Scholar] [CrossRef] [PubMed]
- Naselli, A.; Hurle, R.; Paparella, S.; Buffi, N.M.; Lughezzani, G.; Lista, G.; Casale, P.; Saita, A.; Lazzeri, M.; Guazzoni, G. Role of Restaging Transurethral Resection for T1 Non–muscle invasive Bladder Cancer: A Systematic Review and Meta-analysis. Eur. Urol. Focus 2018, 4, 558–567. [Google Scholar] [CrossRef]
- Cumberbatch, M.G.; Foerster, B.; Catto, J.W.; Kamat, A.M.; Kassouf, W.; Jubber, I.; Shariat, S.F.; Sylvester, R.J.; Gontero, P. Repeat Transurethral Resection in Non–muscle-invasive Bladder Cancer: A Systematic Review. Eur. Urol. 2018, 73, 925–933. [Google Scholar] [CrossRef]
- Shin, K.; Lee, J.; Guo, N.; Kim, J.; Lim, A.; Qu, L.; Mysorekar, I.U.; Beachy, P.A. Hedgehog/Wnt feedback supports regenerative proliferation of epithelial stem cells in bladder. Nat. Cell Biol. 2011, 472, 110–114. [Google Scholar] [CrossRef]
- Brandt, W.D.; Matsui, W.; Rosenberg, J.E.; He, X.; Ling, S.; Schaeffer, E.M.; Berman, D.M. Urothelial carcinoma: Stem cells on the edge. Cancer Metastasis Rev. 2009, 28, 291–304. [Google Scholar] [CrossRef]
- Soltanian, S.; Matin, M.M. Cancer stem cells and cancer therapy. Tumor Biol. 2011, 32, 425–440. [Google Scholar] [CrossRef]
- Yang, Z.-J.; Wechsler-Reya, R.J. Hit ’em where they live: Targeting the cancer stem cell niche. Cancer Cell 2007, 11, 3–5. [Google Scholar] [CrossRef] [PubMed]
- Alison, M.R.; Lim, S.M.L.; Nicholson, L.J. Cancer stem cells: Problems for therapy? J. Pathol. 2010, 223, 148–162. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.K.-L.; Mertz, D.; Loeb, M. Newcastle-Ottawa Scale: Comparing reviewers’ to authors’ assessments. BMC Med. Res. Methodol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Study Design | No. of Patients | Prim | Sec | Duration | Mean FU (Months) | Start of Follow-Up | Surveillance Time Prim (Months) | Treatment of Sec |
|---|---|---|---|---|---|---|---|---|---|---|
| Yiou [16] | France | Retrospective | 55 | 43 | 12 | 1987–1997 | prim: 49, sec: 55.3 | RC | 57 | TURBT BCG |
| Schrier [6] | Netherlands | Retrospective | 163 | 89 | 74 | 1986–2000 | NA | MIBC | NA | TURBT BCG |
| Ferreira [13] | Brazil | Retrospective | 242 | 185 | 57 | 1993-2005 | prim: 98, sec: 96 | RC | 37.4 | TURBT BCG |
| Lee YH [8] | Korea | Retrospective | 223 | 173 | 50 | 1986–2004 | 45 | RC | 15 | TURBT BCG |
| Turkolmez [12] | Turkey | Retrospective | 154 | 109 | 45 | 1990–2005 | prim: 77.8, sec: 90.3 | RC | 41.7 | TURBT BCG |
| Lee [18] | USA | Retrospective | 239 | 169 | 70 | 1990–2003 | prim: 40, sec: 33 (median) | RC | 48 | TURBT BCG |
| de Vries [15] | Netherlands | Retrospective | 188 | 134 | 54 | 1987–2005 | 40.8 | RC | NA | TURBT |
| Rodriguez [24] | Spain | Retrospective | 141 | 72 | 69 | 1978–2002 | 42.5 | RC | NA | TURBT |
| Kotb [9] | Canada | Retrospective | 1150 | 785 | 365 | NA | NA | RC | NA | NA |
| Masson-Lecomte [23] | France | Retrospective | 179 | 155 | 24 | 2001–2011 | NA | RC | 36 | TURBT BCG |
| Hidas [10] | Israel | Retrospective | 144 | 104 | 40 | 1998–2008 | prim: 40.1, sec: 52.6 | Initial TURB+RC | 44 | TURBT BCG |
| Aziz [14] | Germany | Retrospective | 150 | 125 | 25 | 2004–2010 | 46 (median) | RC | 17.71 | TURBT BCG |
| May [17] | Germany | Retrospective | 521 | 399 | 122 | 1992–2007 | 65 | RC | 21.72 | TURBT BCG |
| Breau [4] | Canada | Retrospective | 671 | 481 | 190 | 1980–1998 | NA | RC | 21.6 | TURBT BCG |
| Moschini [7] | Italy | Retrospective | 768 | 475 | 293 | 2000–2012 | 109 | RC | NA | TURBT BCG |
| Kayama [11] | Japan | Retrospective | 282 | 231 | 51 | 2004-2015 | 25–161 | RC | NA | NA |
| Study | Mean Age (Years) | Gender (Male) n (%) | Tumor Stage at RC n (%) | HG n (%) | CIS n (%) | LVI n (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prim | Sec | Prim | Sec | T3/4 | N+ | Prim | Sec | Prim | Sec | Prim | Sec | |||
| Prim | Sec | Prim | Sec | |||||||||||
| Breau [4] | 67.9 | 67.6 | 366 (76) | 146 (77) | 194 (40) | 96 (51) | 100 (21) | 38 (20) | NA | NA | NA | 85 (45) | NA | NA |
| Schrier [6] | 63.3 | 68.5 | 65 (73) | 60 (81) | NA | NA | 27 (30) | 21 (28) | NA | NA | NA | NA | NA | NA |
| Moschini [7] | 68 | 67 | 319 (82) | 250 (85) | 292 (61) | 195 (67) | NA | NA | 400 (84) | 263 (90) | 96 (20) | 53 (18) | 112 (24) | 91 (31) |
| Lee YH [8] | 62 | 154 (89) | 46 (92) | 76 (44) | 26 (52) | 26 (15) | 14 (28) | 155 (90) | 40 (80) | 35 (20) | 10 (20) | 38 (22) | 12 (24) | |
| Kotb [9] | NA | 623 (80) | 291 (80) | 451 (58) | 131 (36) | NA | NA | 697 (91) | 338 (97) | NA | NA | 254 (46) | 78 (32) | |
| Hidas [10] | 72.7 | 69.3 | 79 (76) | 33 (83) | 30 (47) | 14 (62) | 13 (20) | 2 (9) | ||||||
| Kayama [11] | 71 (31–91) (median) | 188 (81) | 40 (78) | 82 (36) | 22 (43) | 0 (0) | 0 (0) | 117 (77) | 36 (71) | 20 (9) | 8 (16) | 83 (36) | 18 (35) | |
| Turkolmez [12] | 59.8 | 60.3 | 94 (86) | 40 (89) | 48 (44) | 20 (44) | NA | NA | NA | NA | NA | NA | NA | NA |
| Ferreira [13] | 65.3 | 63.7 | 145 (78) | 47 (83) | 80 (43) | 28 (49) | 57 (21) | 16 (28) | NA | NA | NA | NA | NA | NA |
| Aziz [14] | 69 | 71 | 97 (78) | 24(96) | 76 (61) | 17 (68) | 50 (40) | 9 (36) | 114 (91) | 25 (100) | 61 (49) | 11 (44) | 72 (58) | 13 (52) |
| de Vries [15] | 61 | 103 (77) | 41 (76) | 42 (31) | 13 (24) | 60 (45) | 25 (46) | NA | NA | NA | NA | NA | NA | |
| Yiou [16] | 62 | 66 | NA | NA | 25 (58) | 3 (25) | 13 (30) | 21 (6) | 29 (67) | 6 (50) | NA | NA | NA | NA |
| May [17] | 64.1 | 68.7 | 388/133 | 138 (56) | 52 (57) | 88 (36) | 28 (30) | 178 (72) | 62 (68) | NA | NA | NA | NA | |
| Lee [18] | 65 | 69 | 127 (75) | 55 (79) | 93 (55) | 41 (61) | 46 (28) | 15 (22) | 161 (96) | 65 (93) | NA | NA | NA | NA |
| Masson-Lecomte [23] | 66.8 | 68 | 166/25 | NA | NA | 46 (30) | 11 (42) | NA | NA | NA | NA | NA | NA | |
| Rodriguez [24] | 63 (median) | 116/25 | NA | NA | NA | NA | NA | NA | NA | NA | NA | NA | ||
| First Author | Year | Selection | Comparability | Outcome | Total Score |
|---|---|---|---|---|---|
| Breau [4] | 2014 | 4 | 2 | 3 | 9 |
| Schrier [6] | 2004 | 4 | 1 | 3 | 8 |
| Moschini [7] | 2016 | 4 | 2 | 3 | 9 |
| Lee YH [8] | 2007 | 4 | 1 | 3 | 8 |
| Kotb [9] | 2012 | 4 | 0 | 3 | 7 |
| Hidas [10] | 2013 | 4 | 2 | 3 | 8 |
| Kayama [11] | 2018 | 3 | 1 | 3 | 7 |
| Turkolmez [12] | 2007 | 3 | 1 | 3 | 7 |
| Ferreira [13] | 2007 | 4 | 1 | 3 | 8 |
| Aziz [14] | 2013 | 3 | 1 | 3 | 7 |
| de Vries [15] | 2010 | 4 | 1 | 3 | 8 |
| Yiou [16] | 2002 | 2 | 2 | 3 | 7 |
| May [17] | 2014 | 4 | 2 | 3 | 9 |
| Lee [18] | 2007 | 4 | 2 | 3 | 9 |
| Masson-Lecomte [23] | 2013 | 3 | 1 | 3 | 7 |
| Rodriguez [24] | 2011 | 3 | 1 | 3 | 7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pones, M.; D’Andrea, D.; Mori, K.; Abufraj, M.; Moschini, M.; Comperat, E.; Shariat, S.F. Differential Prognosis and Response of Denovo vs. Secondary Muscle-Invasive Bladder Cancer: An Updated Systematic Review and Meta-Analysis. Cancers 2021, 13, 2496. https://doi.org/10.3390/cancers13102496
Pones M, D’Andrea D, Mori K, Abufraj M, Moschini M, Comperat E, Shariat SF. Differential Prognosis and Response of Denovo vs. Secondary Muscle-Invasive Bladder Cancer: An Updated Systematic Review and Meta-Analysis. Cancers. 2021; 13(10):2496. https://doi.org/10.3390/cancers13102496
Chicago/Turabian StylePones, Mario, David D’Andrea, Keiichiro Mori, Mohammad Abufraj, Marco Moschini, Eva Comperat, and Shahrokh F. Shariat. 2021. "Differential Prognosis and Response of Denovo vs. Secondary Muscle-Invasive Bladder Cancer: An Updated Systematic Review and Meta-Analysis" Cancers 13, no. 10: 2496. https://doi.org/10.3390/cancers13102496
APA StylePones, M., D’Andrea, D., Mori, K., Abufraj, M., Moschini, M., Comperat, E., & Shariat, S. F. (2021). Differential Prognosis and Response of Denovo vs. Secondary Muscle-Invasive Bladder Cancer: An Updated Systematic Review and Meta-Analysis. Cancers, 13(10), 2496. https://doi.org/10.3390/cancers13102496