
Spontaneous Non-Sustained Ventricular Tachycardia and Premature Ventricular Contractions and Their Prognostic Relevance in Patients with Cancer in Routine Care

 ,
, 
 , ,
, , 

Abstract
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Population
2.2. 24-h Electrocardiograms
2.3. Statistical Analyses
3. Results
3.1. Study Population
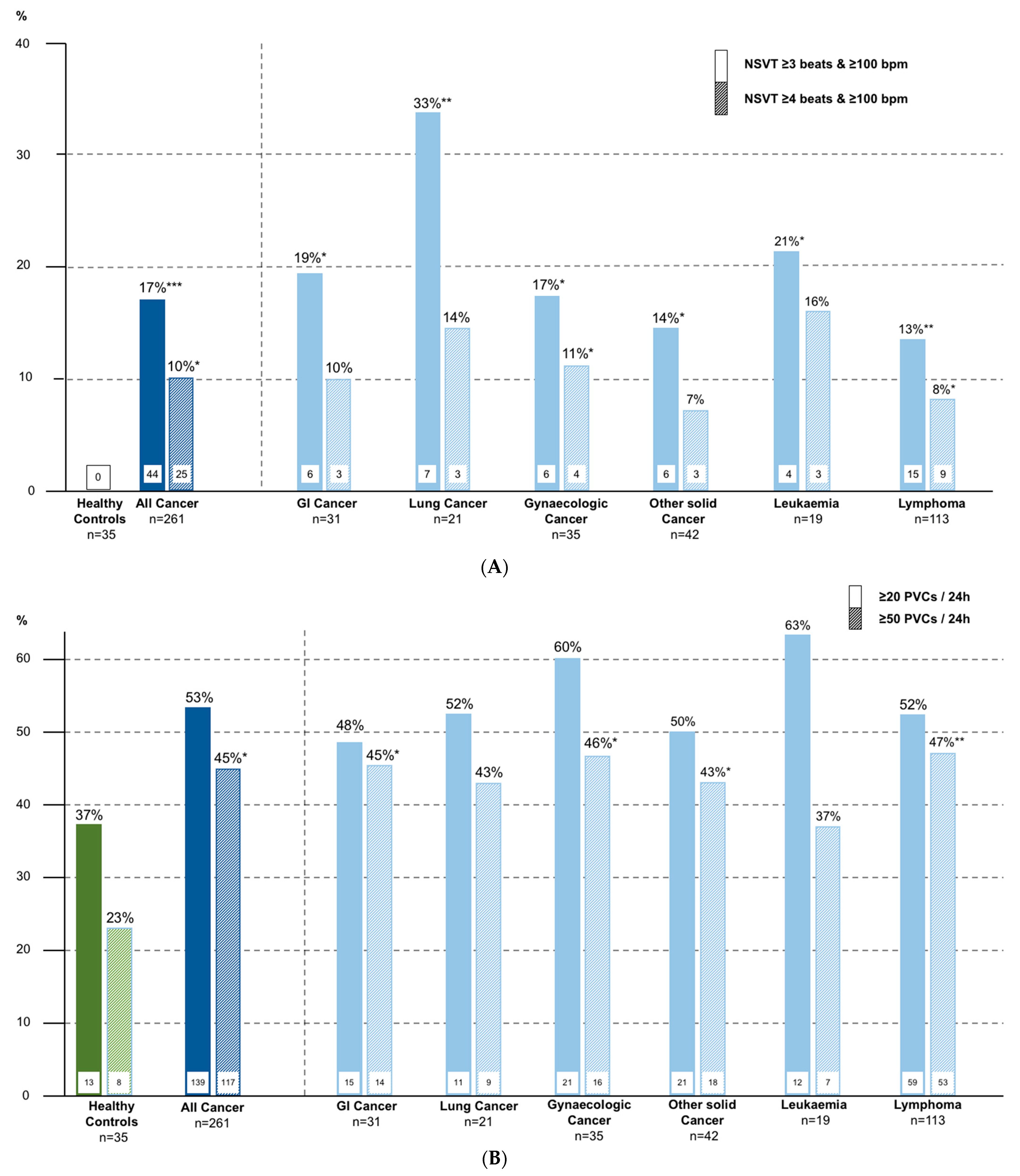
3.2. 24-h Electrocardiograms
3.3. Comparing Patients with and without Ventricular Arrhythmias
3.4. Comparing Patients with and without Death during Follow-Up
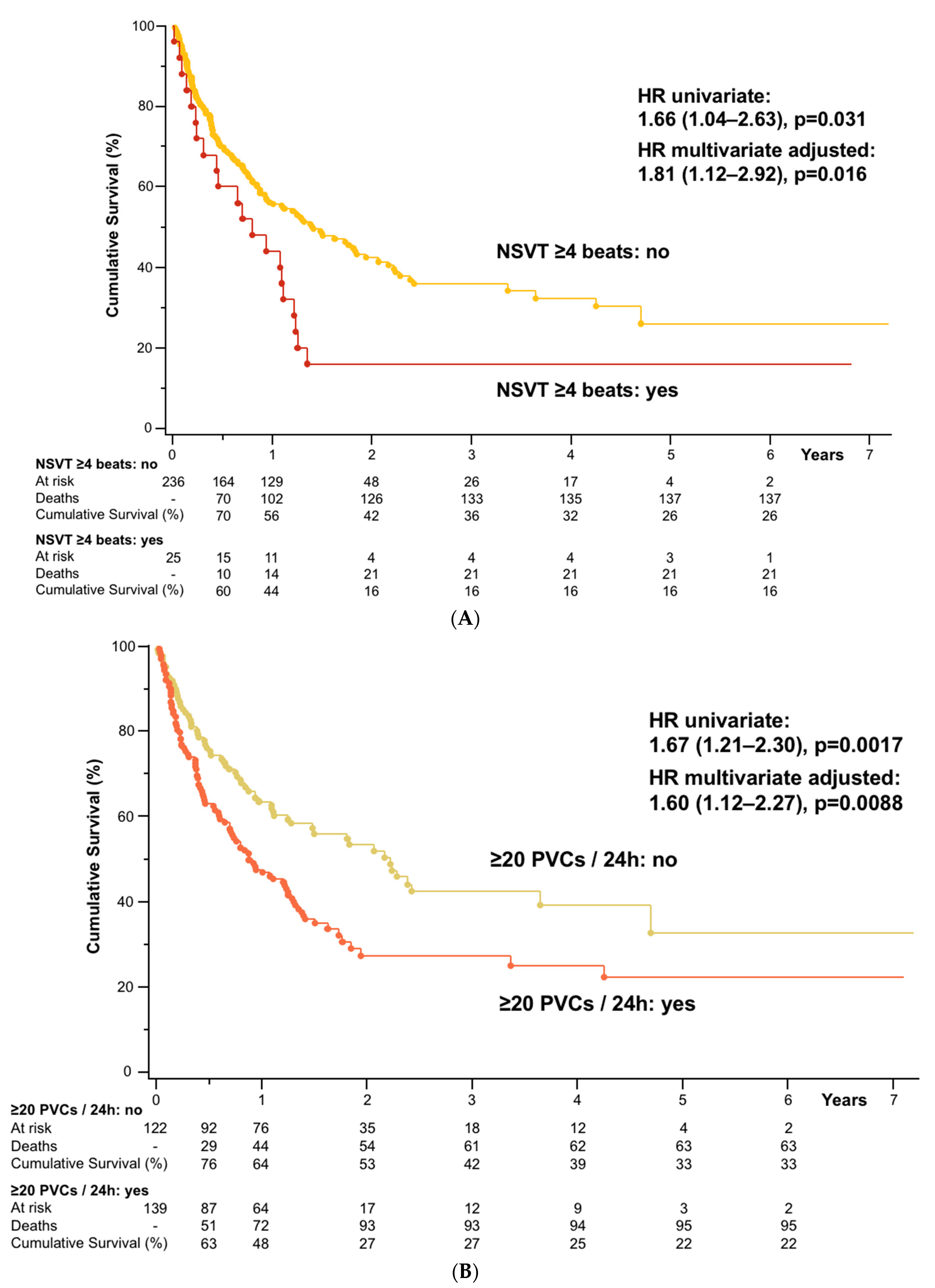
3.5. Survival Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Inagaki, J.; Rodriguez, V.; Bodey, G.P. Proceedings: Cause of death in cancer patients. Cancer 1974, 33, 568–573. [Google Scholar] [CrossRef]
- Brown, B.W.; Brauner, C.; Minnotte, M.C. Noncancer deaths in white adult cancer patients. J. Natl. Cancer Inst. 1993, 85, 979–987. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodruguez Munoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Sandri, M.T.; Colombo, A.; Colombo, N.; Boeri, M.; Lamantia, G.; Civelli, M.; Peccatori, F.; Martinelli, G.; Fiorentini, C.; et al. Prognostic value of troponin I in cardiac risk stratification of cancer patients undergoing high-dose chemotherapy. Circulation 2004, 109, 2749–2754. [Google Scholar] [CrossRef] [PubMed]
- Anker, M.S.; Ebner, N.; Hildebrandt, B.; Springer, J.; Sinn, M.; Riess, H.; Anker, S.D.; Landmesser, U.; Haverkamp, W.; von Haehling, S. Resting heart rate is an independent predictor of death in patients with colorectal, pancreatic, and non-small cell lung cancer: Results of a prospective cardiovascular long-term study. Eur. J. Heart Fail. 2016, 18, 1524–1534. [Google Scholar] [CrossRef] [PubMed]
- Saltzman, H.E. Arrhythmias and heart failure. Cardiol. Clin. 2014, 32, 125–133. [Google Scholar] [CrossRef]
- Oken, M.M.; Creech, R.H.; Tormey, D.C.; Horton, J.; Davis, T.E.; McFadden, E.T.; Carbone, P.P. Toxicity and response criteria of the Eastern Cooperative Oncology Group. Am. J. Clin. Oncol. 1982, 5, 649–655. [Google Scholar] [CrossRef]
- De Medina, E.O.R.; Bernard, R.; Coumel, P.; Damato, A.N.; Fisch, C.; Krikler, D.; Mazur, N.A.; Meijler, F.L.; Mogensen, L.; Moret, P.; et al. Definition of terms related to cardiac rhythm. WHO/ISFC Task Force. Eur. J. Cardiol. 1978, 8, 127–144. [Google Scholar]
- Pedersen, C.T.; Kay, G.N.; Kalman, J.; Borggrefe, M.; Della-Bella, P.; Dickfeld, T.; Dorian, P.; Huikuri, H.; Kim, Y.-H.; Knight, B.; et al. EHRA/HRS/APHRS expert consensus on ventricular arrhythmias. Europace 2014, 16, 1257–1283. [Google Scholar] [CrossRef]
- Mehta, C.R.; Senchaudhuri, P.J.C.S.C. Conditional versus unconditional exact tests for comparing two binomials. Cytel Softw. Corp. 2003, 675, 1–5. [Google Scholar]
- Barnard, G.J.N. A new test for 2×2 tables. Nature 1945, 156, 177. [Google Scholar] [CrossRef]
- Martín Andrés, A.; Quevedo, M.J.S.; Mato, A.S. Fisher’s Mid-P-value arrangement in 2 × 2 Comparative trials. Comput. Stat. Data Anal. 1998, 29, 107–115. [Google Scholar] [CrossRef]
- Savitz, D.A.; Olshan, A.F. Describing data requires no adjustment for multiple comparisons: A reply from Savitz and Olshan. Am. J. Epidemiol. 1998, 147, 813–814. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Thompson, J.R. Invited Commentary: Re: ‘Multiple Comparisons and Related Issues in the Interpretation of Epidemiologic Data”. Am. J. Epidemiol. 1998, 147, 801–806. [Google Scholar] [CrossRef] [PubMed]
- Anker, M.S.; von Haehling, S.; Coats, A.J.S.; Riess, H.; Eucker, J.; Porthun, J.; Butler, J.; Karakas, M.; Haverkamp, W.; Landmesser, U.; et al. Ventricular tachycardia, premature ventricular contractions, and mortality in unselected patients with lung, colon, or pancreatic cancer: A prospective study. Eur. J. Heart Fail. 2021, 23, 145–153. [Google Scholar] [CrossRef]
- Hingorani, P.; Karnad, D.R.; Rohekar, P.; Kerkar, V.; Lokhandwala, Y.Y.; Kothari, S. Arrhythmias Seen in Baseline 24-Hour Holter ECG Recordings in Healthy Normal Volunteers During Phase 1 Clinical Trials. J. Clin. Pharmacol. 2016, 56, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Priori, S.G.; Blomström-Lundqvist, C.; Mazzanti, A.; Blom, N.; Borggrefe, M.; Camm, J.; Elliott, P.M.; Fitzsimons, D.; Hatala, R.; Hindricks, G.; et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 2015, 36, 2793–2867. [Google Scholar]
- Mullis, A.H.; Ayoub, K.; Shah, J.; Butt, M.; Suffredini, J.; Czarapata, M.; Delisle, B.; Ogunbayo, G.O.; Darrat, Y.; Elayi, C.S. Fluctuations in premature ventricular contraction burden can affect medical assessment and management. Heart Rhythm 2019, 16, 1570–1574. [Google Scholar] [CrossRef]
- Zaorsky, N.G.; Churilla, T.M.; Egleston, B.L.; Fisher, S.G.; Ridge, J.A.; Horwitz, E.M.; Meyer, J.E. Causes of death among cancer patients. Ann. Oncol. 2017, 28, 400–407. [Google Scholar] [CrossRef]
- Anker, M.S.; Hülsmann, M.; Cleland, J.G. What do patients with heart failure die from? A single assassin or a conspiracy? Eur. J. Heart Fail. 2019. [Google Scholar] [CrossRef]
- Cramer, L.; Hildebrandt, B.; Kung, T.; Wichmann, K.; Springer, J.; Doehner, W.; Sandek, A.; Valentova, M.; Stojakovic, T.; Scharnagl, H.; et al. Cardiovascular function and predictors of exercise capacity in patients with colorectal cancer. J. Am. Coll. Cardiol. 2014, 64, 1310–1319. [Google Scholar] [CrossRef]
- Anker, M.S.; Sanz, A.P.; Zamorano, J.L.; Mehra, M.R.; Butler, J.; Riess, H.; Coats, A.J.S.; Anker, S.D. Advanced cancer is also a heart failure syndrome: A hypothesis. J. Cachexia Sarcopenia Muscle 2021. [Google Scholar] [CrossRef] [PubMed]
- Anker, M.S.; Sanz, A.P.; Zamorano, J.L.; Mehra, M.R.; Butler, J.; Riess, H.; Coats, A.J.S.; Anker, S.D. Advanced cancer is also a heart failure syndrome: A hypothesis. Eur. J. Heart Fail. 2021, 23, 140–144. [Google Scholar] [CrossRef] [PubMed]
- Shibata, H. Cancer and electrolytes imbalance. Gan Kagaku Ryoho 2010, 37, 1006–1010. [Google Scholar]
- Karlstaedt, A.; Zhang, X.; Vitrac, H.; Harmancey, R.; Vasquez, H.; Wang, J.H.; Goodell, M.A.; Taegtmeyer, H. Oncometabolite d-2-hydroxyglutarate impairs α-ketoglutarate dehydrogenase and contractile function in rodent heart. Proc. Natl. Acad. Sci. USA 2016, 113, 10436–10441. [Google Scholar] [CrossRef] [PubMed]
- Tian, M.; Nishijima, Y.; Asp, M.L.; Stout, M.B.; Reiser, P.J.; Belury, M.A. Cardiac alterations in cancer-induced cachexia in mice. Int. J. Oncol. 2010, 37, 347–353. [Google Scholar]
- Mühlfeld, C.; Das, S.K.; Heinzel, F.R.; Schmidt, A.; Post, H.; Schauer, S.; Papadakis, T.; Kummer, W.; Hoefler, G. Cancer induces cardiomyocyte remodeling and hypoinnervation in the left ventricle of the mouse heart. PLoS ONE 2011, 6, e20424. [Google Scholar]
- Barkhudaryan, A.; Scherbakov, N.; Springer, J.; Doehner, W. Cardiac muscle wasting in individuals with cancer cachexia. ESC Heart Fail. 2017, 4, 458–467. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Healthy Controls (n = 35) | Cancer Patients (n = 261) | p-Value | Cancer Deaths (n = 158) | Cancer Survivors (n = 103) | p-Value |
|---|---|---|---|---|---|---|
| Clinical characteristics | ||||||
| Age (years) | 68 ± 6 (IQR 62–73) | 68 ± 12 (IQR 61–76) | 0.86 | 69 ± 10 (IQR 62–75) | 65 ± 17 (IQR 58–76) | 0.016 |
| Female sex, n (%) | 19 (54) | 132 (51) | 0.68 | 76 (48) | 56 (54) | 0.32 |
| BMI (kg/m2) | 26 ± 4 | 24 ± 5 | 0.28 | 25 ± 5 | 26 ± 5 | 0.049 |
| Cancer stage ≥III, n (%) | – | 188 (72) | – | 123 (78) | 65 (63) | 0.0095 |
| Cancer type: solid, n (%) | – | 129 (49) | – | 93 (59) | 36 (35) | 0.0002 |
| ECOG performance status ≥2, n (%) | – | 111 (43) | – | 75 (47) | 36 (35) | 0.046 |
| Prior potentially cardiotoxic anti-cancer drugs, n (%) | – | 162 (62) | – | 104 (66) | 58 (56) | 0.12 |
| Left ventricular ejection fraction (%) | 64 ± 7 | 65 ± 7 (n = 181) | 0.81 | 64 ± 8 (n = 100) | 65 ± 7 (n = 81) | 0.27 |
| Laboratory parameters | ||||||
| Haemoglobin (g/dL) | 14.2 ± 1.3 | 10.8 ± 2.0 | <0.0001 | 10.6 ± 1.9 | 11.1 ± 2.1 | 0.040 |
| Leucocytes (/nL) | 6.6 (5.5–7.6) | 6.5 (4.3-9.6) | 0.99 | 6.9 (4.4–9.9) | 6.1 (4.3–9.2) | 0.40 |
| Platelets (/nL) | 227 ± 46 | 225 ± 166 | 0.97 | 231 ± 195 | 217 ± 108 | 0.48 |
| Sodium (mmol/L) | 141 ± 2 | 139 ± 4 | 0.0002 | 138 ± 4 | 140 ± 3 | 0.0027 |
| Potassium (mmol/L) | 4.2 ± 0.4 | 3.9 ± 0.5 | 0.0004 | 3.9 ± 0.5 | 3.9 ± 0.5 | 0.91 |
| Creatinine (mg/dL) | 0.87 ± 0.19 | 1.00 ± 0.59 | 0.22 | 1.03 ± 0.68 | 0.94 ± 0.40 | 0.23 |
| GOT (U/L) | 26 (22–28) | 26 (19-37) (n = 171) | 0.75 | 27 (19–39) (n = 101) | 25 (19–34) (n = 70) | 0.34 |
| Secondary diagnoses | ||||||
| Arterial hypertension, n (%) | 7 (20) | 132 (51) | 0.0007 | 79 (50) | 53 (51) | 0.82 |
| Coronary artery disease, (%) | 0 | 34 (13) | 0.0040 | 22 (14) | 12 (12) | 0.59 |
| Atrial fibrillation, n (%) | 0 | 14 (5) | 0.08 | 8 (5) | 6 (6) | 0.79 |
| Previous myocardial infarction, n (%) | 0 | 20 (8) | 0.033 | 13 (8) | 7 (7) | 0.67 |
| Diabetes mellitus type 2, n (%) | 0 | 50 (19) | 0.0003 | 31 (20) | 19 (18) | 0.81 |
| Chronic kidney disease, n (%) | 0 | 41 (16) | 0.0014 | 28 (18) | 13 (13) | 0.27 |
| Previous stroke, n (%) | 0 | 27 (10) | 0.011 | 17 (11) | 10 (10) | 0.79 |
| Current use of antibiotics, n (%) | 0 | 45 (17) | 0.0007 | 33 (21) | 12 (12) | 0.054 |
| 24 h-ECG | ||||||
| Average 24 h heart rate (bpm) | 70 ± 9 | 78 ± 14 | 0.0007 | 79 ± 16 | 77 ± 11 | 0.41 |
| No. of premature atrial contractions/24 h | 82 (27–302) | 195 (27–1167) | 0.22 | 227 (32–1226) | 146 (24–761) | 0.20 |
| No. of premature ventricular contractions/24 h | 9 (1–43) | 26 (2–360) | 0.06 | 54 (4–467) | 12 (1–280) | 0.013 |
| ≥20 Premature ventricular contractions/24 h, n (%) | 13 (37) | 139 (53) | 0.07 | 95 (60) | 44 (43) | 0.0059 |
| ≥50 Premature ventricular contractions/24 h, n (%) | 8 (23) | 117 (45) | 0.013 | 80 (51) | 37 (36) | 0.020 |
| NSVT with ≥3 beats & ≥100 bpm, n (%) | 0 | 44 (17) | 0.0008 | 31 (20) | 13 (13) | 0.14 |
| NSVT with ≥4 beats & ≥100 bpm, n (%) | 0 | 25 (10) | 0.016 | 21 (13) | 4 (4) | 0.0066 |
| Variable | Univariate Model | |||||||
| HR | 95% CI | χ2 | p-Value | |||||
| Significant and Clinically Relevant Variables | ||||||||
| NSVT ≥4 beats & ≥100 bpm (yes vs. no) | 1.66 | 1.04–2.63 | 4.6 | 0.033 | ||||
| ≥20 Premature ventricular contractions/24 h (yes vs. no) | 1.67 | 1.21–2.30 | 9.9 | 0.0017 | ||||
| Age (per 1 year) | 1.01 | 1.001–1.03 | 4.3 | 0.039 | ||||
| BMI (per 1 kg/m2) | 0.95 | 0.91–0.98 | 8.1 | 0.0043 | ||||
| Cancer stage (≥III vs. I/II) | 1.66 | 1.14–2.42 | 7.0 | 0.0082 | ||||
| Cancer type (solid vs. haematologic) | 2.09 | 1.52–2.87 | 20.3 | <0.0001 | ||||
| ECOG performance status (≥2 vs. 0/1) | 1.58 | 1.15–2.17 | 8.2 | 0.0043 | ||||
| Haemoglobin (per 1 g/dL) | 0.91 | 0.84–0.99 | 5.3 | 0.021 | ||||
| Sodium (per 1 mmol/L) | 0.94 | 0.90–0.98 | 10.4 | 0.0013 | ||||
| Opioids (yes vs. no) | 1.67 | 1.13–2.47 | 6.7 | 0.0097 | ||||
| Antidepressants (yes vs. no) | 1.85 | 1.14–2.99 | 6.2 | 0.013 | ||||
| Prior potentially cardiotoxic anti-cancer drugs (yes vs. no) | 1.41 | 1.02–1.96 | 4.2 | 0.039 | ||||
| Sex (female vs. male) | 0.80 | 0.59–1.10 | 1.9 | 0.17 | ||||
| Potassium (per 1 mmol/L) | 1.07 | 0.78–1.48 | 0.2 | 0.66 | ||||
| Current use of antibiotics (yes vs. no) | 1.29 | 0.88–1.90 | 1.7 | 0.19 | ||||
| Coronary artery disease (yes vs. no) | 0.99 | 0.63–1.56 | 0.001 | 0.98 | ||||
| Variable | Multivariate Model 1 | Multivariate Model 2 | ||||||
| HR | 95% CI | χ2 | p-Value | HR | 95% CI | χ2 | p-Value | |
| Multivariate Survival Analyses in Cancer Patients with NSVT ≥4 beats & ≥100 bpm | ||||||||
| NSVT ≥4 beats & ≥100 bpm (yes vs. no) | 1.82 | 1.13–2.94 | 6.0 | 0.015 | 1.76 | 1.09–2.84 | 5.3 | 0.022 |
| Age (per 1 year) | 1.02 | 1.01–1.04 | 8.4 | 0.0038 | 1.02 | 1.01–1.04 | 8.2 | 0.0041 |
| Sodium (per 1 mmol/L) | 0.96 | 0.92–1.002 | 3.5 | 0.061 | 0.96 | 0.92–1.003 | 3.4 | 0.07 |
| Haemoglobin (per 1 g/dL) | 0.92 | 0.84–1.0003 | 3.8 | 0.051 | 0.92 | 0.84–1.004 | 3.5 | 0.06 |
| BMI (per 1 kg/m2) | 0.96 | 0.93–0.996 | 4.7 | 0.031 | 0.96 | 0.92–0.998 | 4.2 | 0.041 |
| Opioids (yes vs. no) | 1.33 | 0.88–2.03 | 1.8 | 0.18 | 1.33 | 0.87–2.04 | 1.7 | 0.19 |
| Antidepressants (yes vs. no) | 1.50 | 0.91–2.47 | 2.6 | 0.11 | 1.60 | 0.97–2.64 | 3.4 | 0.07 |
| Cancer stage (≥III vs. I/II) | 1.50 | 1.01–2.21 | 4.1 | 0.043 | 1.52 | 1.03–2.24 | 4.4 | 0.037 |
| Cancer type (solid vs. haematologic) | 2.46 | 1.75–3.46 | 26.9 | <0.0001 | 2.54 | 1.80–3.59 | 27.7 | <0.0001 |
| ECOG performance status (≥2 vs. 0/1) | 1.23 | 0.87–1.73 | 1.4 | 0.24 | 1.40 | 0.97–2.01 | 3.3 | 0.07 |
| Prior potentially cardiotoxic anti-cancer drugs (yes vs. no) | 1.68 | 1.18–2.40 | 8.2 | 0.0041 | 1.70 | 1.19–2.43 | 8.4 | 0.0037 |
| Sex (female vs. male) | 0.68 | 0.48–0.95 | 5.1 | 0.024 | ||||
| Potassium (per 1 mmol/L) | 1.15 | 0.83–1.59 | 0.7 | 0.40 | ||||
| Current use of antibiotics (yes vs. no) | 1.33 | 0.88–1.99 | 1.8 | 0.18 | ||||
| Coronary artery disease (yes vs. no) | 1.02 | 0.62–1.67 | 0.004 | 0.95 | ||||
| Multivariate Survival Analyses in Cancer Patients with ≥20 Premature Ventricular Contractions | ||||||||
| ≥20 Premature ventricular contractions/24 h (yes vs. no) | 1.71 | 1.22–2.40 | 9.7 | 0.0019 | 1.63 | 1.15–2.31 | 7.4 | 0.0064 |
| Age (per 1 year) | 1.01 | 0.9991–1.03 | 3.4 | 0.07 | 1.02 | 0.99995–1.03 | 3.8 | 0.05 |
| Sodium (per 1 mmol/L) | 0.97 | 0.92–1.008 | 2.6 | 0.11 | 0.96 | 0.92–1.008 | 2.6 | 0.11 |
| Haemoglobin (per 1 g/dL) | 0.91 | 0.83–0.989 | 4.9 | 0.027 | 0.91 | 0.83–0.991 | 4.7 | 0.031 |
| BMI (per 1 kg/m2) | 0.96 | 0.92–0.993 | 5.3 | 0.021 | 0.96 | 0.92–0.996 | 4.6 | 0.032 |
| Opioids (yes vs. no) | 1.21 | 0.80–1.84 | 0.84 | 0.36 | 1.22 | 0.79–1.86 | 0.8 | 0.37 |
| Antidepressants (yes vs. no) | 1.60 | 0.97–2.64 | 3.5 | 0.06 | 1.67 | 1.01–2.75 | 4.1 | 0.044 |
| Cancer stage (≥III vs. I/II) | 1.64 | 1.11–2.42 | 6.1 | 0.014 | 1.63 | 1.10–2.41 | 6.0 | 0.014 |
| Cancer type (solid vs. haematologic) | 2.44 | 1.74–3.43 | 26.5 | <0.0001 | 2.49 | 1.77–3.52 | 27.0 | <0.0001 |
| ECOG performance status (≥2 vs. 0/1) | 1.30 | 0.92–1.84 | 2.3 | 0.13 | 1.47 | 1.02–2.11 | 4.4 | 0.037 |
| Prior potentially cardiotoxic anti-cancer drugs (yes vs. no) | 1.53 | 1.07–2.17 | 5.5 | 0.019 | 1.54 | 1.08–2.20 | 5.6 | 0.018 |
| Sex (female vs. male) | 0.69 | 0.49–0.97 | 4.6 | 0.03 | ||||
| Potassium (per 1 mmol/L) | 1.14 | 0.83–1.57 | 0.6 | 0.42 | ||||
| Current use of antibiotics (yes vs. no) | 1.24 | 0.82–1.86 | 1.0 | 0.31 | ||||
| Coronary artery disease (yes vs. no) | 0.91 | 0.55–1.50 | 0.1 | 0.71 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albrecht, A.; Porthun, J.; Eucker, J.; Coats, A.J.S.; von Haehling, S.; Pezzutto, A.; Karakas, M.; Riess, H.; Keller, U.; Landmesser, U.; et al. Spontaneous Non-Sustained Ventricular Tachycardia and Premature Ventricular Contractions and Their Prognostic Relevance in Patients with Cancer in Routine Care. Cancers 2021, 13, 2303. https://doi.org/10.3390/cancers13102303
Albrecht A, Porthun J, Eucker J, Coats AJS, von Haehling S, Pezzutto A, Karakas M, Riess H, Keller U, Landmesser U, et al. Spontaneous Non-Sustained Ventricular Tachycardia and Premature Ventricular Contractions and Their Prognostic Relevance in Patients with Cancer in Routine Care. Cancers. 2021; 13(10):2303. https://doi.org/10.3390/cancers13102303
Chicago/Turabian StyleAlbrecht, Annemarie, Jan Porthun, Jan Eucker, Andrew J.S. Coats, Stephan von Haehling, Antonio Pezzutto, Mahir Karakas, Hanno Riess, Ulrich Keller, Ulf Landmesser, and et al. 2021. "Spontaneous Non-Sustained Ventricular Tachycardia and Premature Ventricular Contractions and Their Prognostic Relevance in Patients with Cancer in Routine Care" Cancers 13, no. 10: 2303. https://doi.org/10.3390/cancers13102303
APA StyleAlbrecht, A., Porthun, J., Eucker, J., Coats, A. J. S., von Haehling, S., Pezzutto, A., Karakas, M., Riess, H., Keller, U., Landmesser, U., Haverkamp, W., Anker, S. D., & Anker, M. S. (2021). Spontaneous Non-Sustained Ventricular Tachycardia and Premature Ventricular Contractions and Their Prognostic Relevance in Patients with Cancer in Routine Care. Cancers, 13(10), 2303. https://doi.org/10.3390/cancers13102303