
Serum Markers of Refractoriness and Enteropathy-Associated T-Cell Lymphoma in Coeliac Disease

 , ,
, ,  , , ,
, , ,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Features
2.3. Serum Markers
2.4. Statistical Analysis
3. Results
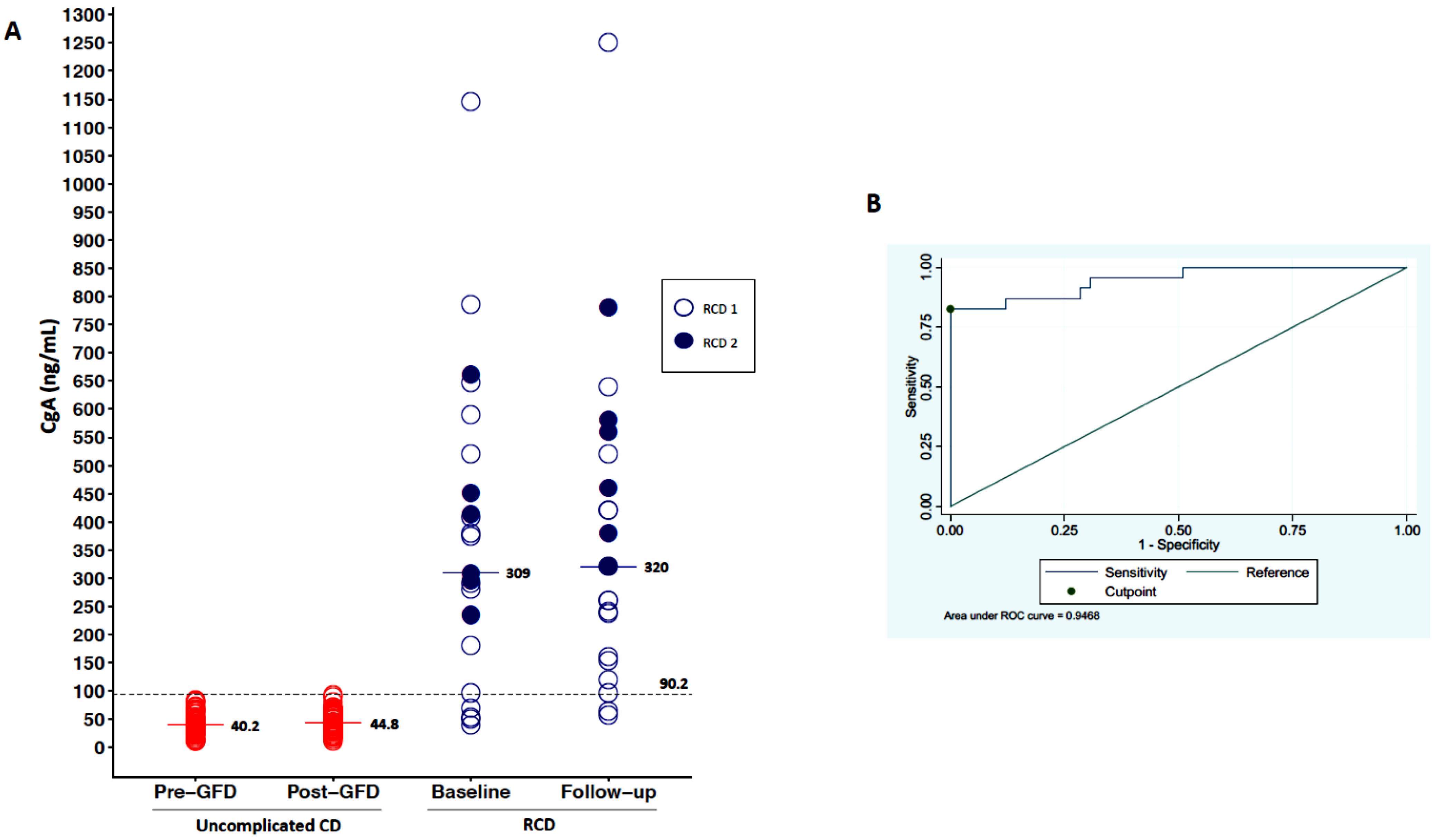
3.1. Serum Levels of CgA
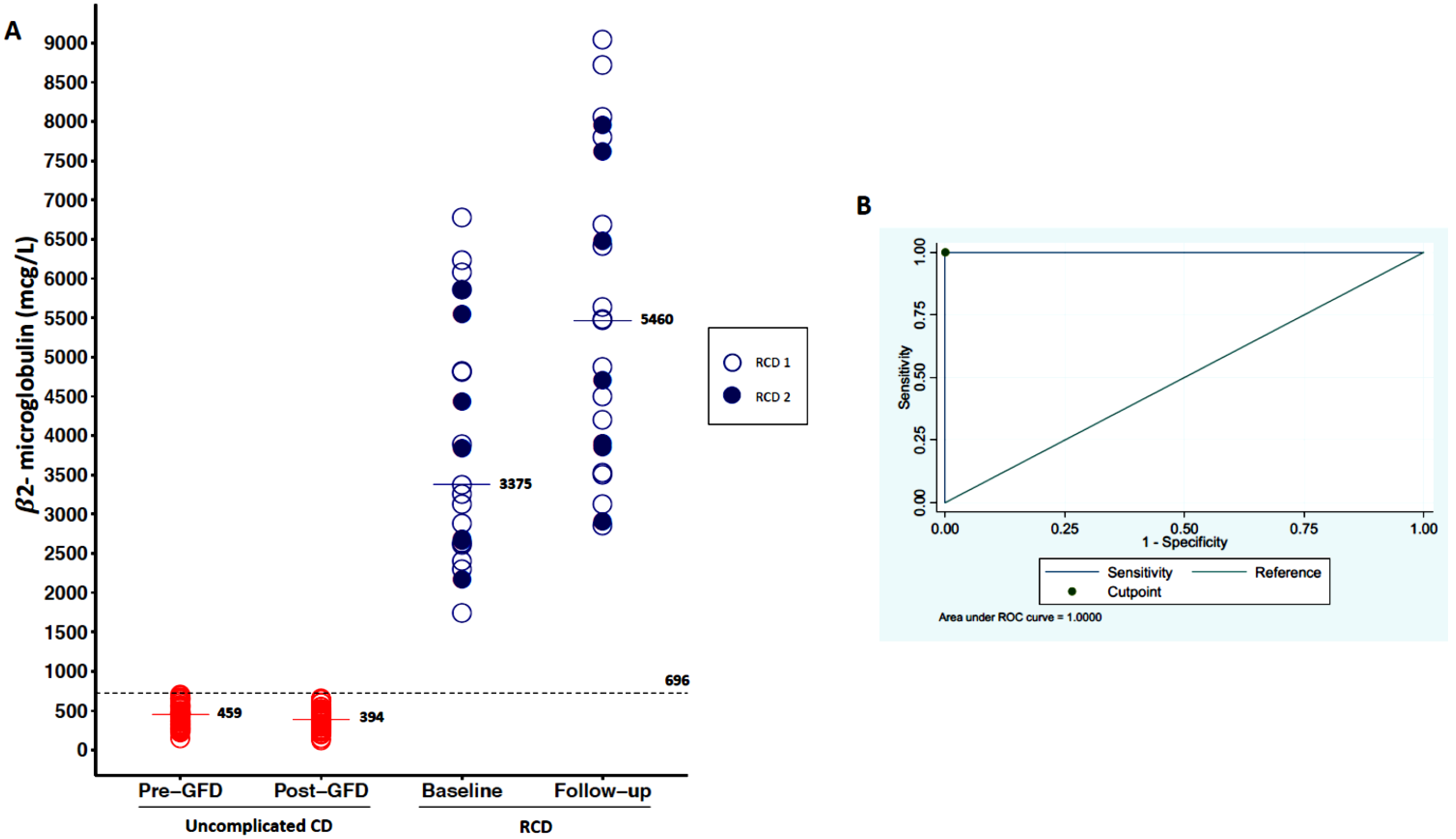
3.2. Serum Levels of β2-Microglobuline
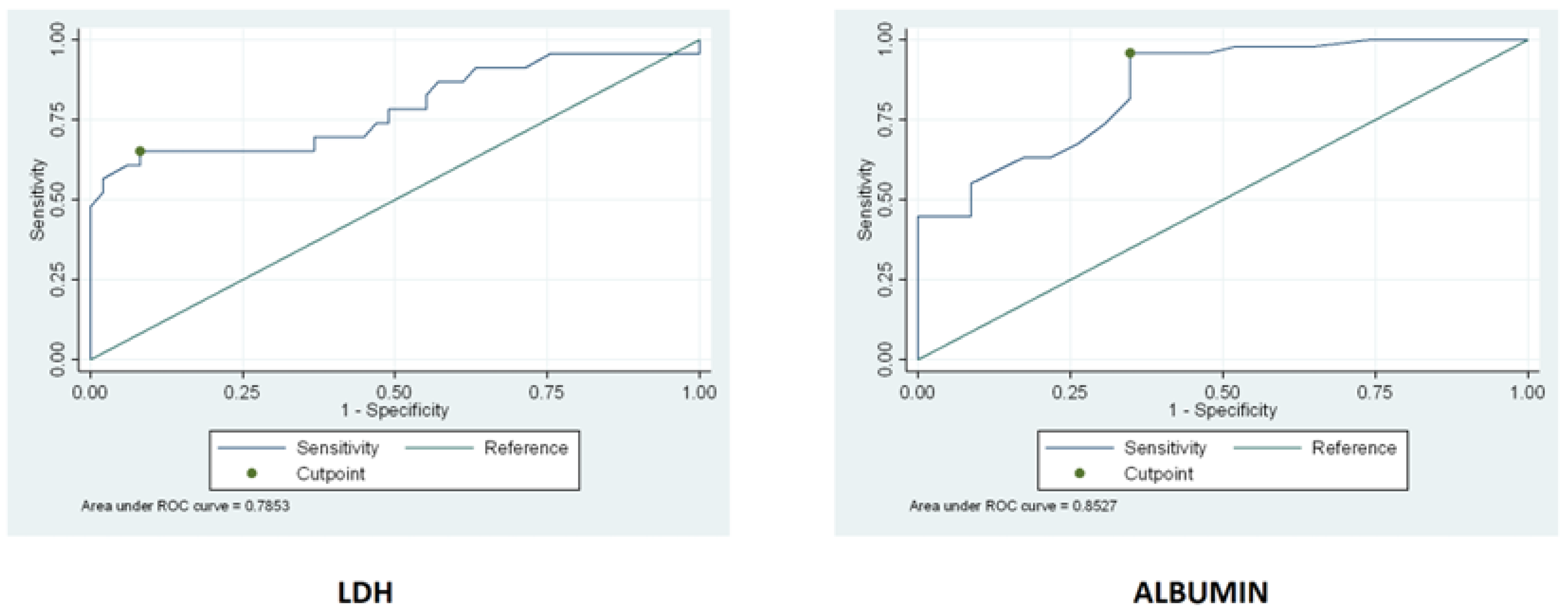
3.3. Serum Levels of LDH and Albumin
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lenti, M.V.; Corazza, G.R. Measuring too much or too little in adult coeliac disease. J. Clin. Pathol. 2019, 72, 341–342. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Corazza, G.R. Coeliac disease. Lancet 2009, 373, 1480–1493. [Google Scholar] [CrossRef]
- Green, P.H.; Cellier, C. Celiac disease. N. Engl. J. Med. 2007, 357, 1731–1743. [Google Scholar] [CrossRef]
- Mulder, C.; Cellier, C. Coeliac disease: Changing views. Best Pract. Res. Clin. Gatroenterol. 2005, 19, 313–321. [Google Scholar] [CrossRef]
- Green, P.H.; Jabri, B. Coeliac disease. Lancet 2003, 362, 383–391. [Google Scholar] [CrossRef]
- Schuppan, D.; Junker, J.; Barisani, D. Celiac disease: From pathogenesis to novel therapies. Gastroenterology 2009, 137, 1912–1933. [Google Scholar] [CrossRef] [PubMed]
- Leonard, M.M.; Sapone, A.; Catassi, C.; Fasano, A. Celiac disease and nonceliac gluten sensitivity: A review. JAMA 2017, 318, 647–656. [Google Scholar] [CrossRef]
- Caio, G.; Ciccocioppo, R.; Zoli, G.; De Giorgio, R.; Volta, U. Therapeutic options for coeliac disease: What else beyond gluten-free diet? Dig. Liver Dis. 2019, 52, 130–137. [Google Scholar] [CrossRef] [PubMed]
- Corazza, G.R.; Lenti, M.V. Does biopsy still have a role for adult coeliac disease? Lancet Gastroenterol. Hepatol. 2017, 2, 773–774. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Biagi, F.; Gobbi, P.G.; Corazza, G.R. How I treat enteropathy-associated T-cell lymphoma. Blood 2012, 119, 2458–2468. [Google Scholar] [CrossRef]
- Rubio-Tapia, A.; Murray, J.A. Classification and management of refractory coeliac disease. Gut 2010, 59, 547–557. [Google Scholar] [CrossRef]
- Cellier, C.; Bouma, G.; van Gils, T.; Khater, S.; Malamut, G.; Crespo, L.; Collin, P.; Green, P.H.R.; Crowe, S.E.; Tsuji, W.; et al. Safety and efficacy of AMG 714 in patients with type 2 refractory coeliac disease: A phase 2a, randomised, double-blind, placebo-controlled, parallel-group study. Lancet Gastroenterol. Hepatol. 2019, 4, 960–970. [Google Scholar] [CrossRef]
- Nasr, I.; Nasr, I.; Campling, H.; Ciclitira, P.J. Approach to patients with refractory coeliac disease. F1000Research 2016, 5, 2544. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Corazza, G.R. Defining gluten refractory enteropathy. Eur. J. Gastroenterol. Hepatol. 2001, 13, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Miceli, E.; Poggi, N.; Missanelli, A.; Bianchi, P.; Moratti, R.; Corazza, G.R. Is serum citrulline measurement clinically useful in coeliac disease? Intern. Emerg. Med. 2008, 3, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Biagi, F.; Bianchi, P.I.; Marchese, A.; Trotta, L.; Vattiato, C.; Balduzzi, D.; Brusco, G.; Andrealli, A.; Cisarò, F.; Astegiano, M.; et al. A score that verifies adherence to a gluten-free diet: A cross-sectional, multicentre validation in real clinical life. Br. J. Nutr. 2012, 108, 1884–1888. [Google Scholar] [CrossRef] [PubMed]
- Ludvigsson, J.F.; Bai, J.C.; Biagi, F.; Card, T.R.; Ciacci, C.; Ciclitira, P.J.; Green, P.H.; Hadjivassiliou, M.; Holdoway, A.; van Heel, D.A.; et al. BSG Coeliac Disease Guidelines Development Group; British Society of Gastroenterology. Diagnosis and management of adult coeliac disease: Guidelines from the British Society of Gastroenterology. Gut 2014, 63, 1210–1228. [Google Scholar] [CrossRef] [PubMed]
- Di Sabatino, A.; Giuffrida, P.; Vanoli, A.; Luinetti, O.; Manca, R.; Biancheri, P.; Gaetano, B.; Costanza, A.; Alessandra, P.; Chiara, S.; et al. Increase in neuroendocrine cells in the duodenal mucosa of patient with refractory coeliac disease. Am. J. Gastroenterol. 2014, 109, 258–269. [Google Scholar] [CrossRef]
- Bonamico, M.; Culasso, F.; Pitzalis, G.; Mariani, P.; Morellini, M.; Procopio, A.; Triglione, P.; Signoretti, A.; Ballati, G. Beta-2 microglobuline levels in celiac disease. J. Pediatric Gastroenterol. Nutr. 1990, 11, 330–336. [Google Scholar] [CrossRef]
- Krauss, N.; Schuppan, D. Monitoring non-responsive patients who have celiac disease. Gastrointest Endosc. Clin. N. Am. 2006, 16, 317–327. [Google Scholar] [CrossRef]
- Di Sabatino, A.; Biagi, F.; Lenzi, M.; Frulloni, L.; Lenti, M.V.; Giuffrida, P.; Corazza, G.R. Clinical usefulness of serum antibodies as biomarkers of gastrointestinal and liver diseases. Dig. Liver Dis. 2017, 49, 947–956. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, F.A.; Wibell, L.; Evrin, P.E. Beta-2 microglobuline in clinical medicine. Scand. J. Clin. Lab. Invest. Suppl. 1980, 154, 27–37. [Google Scholar] [PubMed]
- Lenti, M.V.; Rugge, M.; Lahner, E.; Miceli, E.; Toh, B.-H.; Genta, R.M.; De Block, C.; Hershko, C.; Di Sabatino, A. Autoimmune gastritis. Nat. Rev. Dis. Primers 2020, 6, 56. [Google Scholar] [CrossRef]
- Miceli, E.; Padula, D.; Lenti, M.V.; Gallia, A.; Albertini, R.; Di Stefano, M.; Klersy, C.; Corazza, G.R. A laboratory score in the diagnosis of autoimmune atrophic gastritis: A prospective study. J. Clin. Gastroenterol. 2015, 49, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Lahner, E.; Zagari, R.M.; Zullo, A.; Di Sabatino, A.; Meggio, A.; Cesaro, P.; Lenti, M.V.; Annibale, B.; Corazza, G.R. Chronic atrophic gastritis: Natural history, diagnosis and therapeutic management. A position paper by Italian Society of Hospital Gastroenterologists and Digestive Endoscopists (AIGO), the Italian Society of Digestive Endoscopy (SIED), the Italian Society of Gastroenterologists (SIGE), and the Italian Society of Internal Medicine (SIMI). Dig. Liver Dis. 2019, 51, 1621–1632. [Google Scholar] [PubMed]
- El-Salhy, M.; Gilja, O.H.; Gundersen, D.; Hatlebakk, J.G.; Hausken, T. Duodenal chromogranin a cell density as a biomarker for the diagnosis of irritable bowel syndrome. Gastroenterol. Res. Pract. 2014, 2014, 462856. [Google Scholar] [CrossRef]
- El-Salhy, M.; Lomholt-Beck, B.; Hausken, T. Chromogranin A as a possible tool in the diagnosis of irritable bowel syndrome. Scand J. Gastroenterol. 2010, 45, 1435–1439. [Google Scholar] [CrossRef]
- Sciola, V.; Massironi, S.; Conte, D.; Caprioli, F.; Ferrero, S.; Ciafardini, C.; Peracchi, M.; Bardella, M.T.; Piodi, L. Plasma chromogranin A in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2009, 15, 867–871. [Google Scholar] [CrossRef]
- Perfetti, V.; Brunetti, L.; Biagi, F.; Ciccocioppo, R.; Bianchi, P.I.; Corazza, G.R. TCRβ clonality improves diagnostic yield of TCRγ clonality in refractory celiac disease. J. Clin. Gastroenterol. 2012, 46, 675–679. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Biomarker | Type | Baseline | Follow-Up | p-Value 3 | Change |
|---|---|---|---|---|---|
| CgA (ng/mL) | Uncomplicat-ed CD RCD | 40 (26–55) 309 (180–520) | 45 (32–60) 320 (160–520) | 0.001 0.119 | 4 (−0.6–7) 63 (13–112) |
| p-value 1 | <0.001 | <0.001 | / | <0.001 | |
| RCD 1 RCD 2 | 332 (83–555) 309 (235–450) | 250 (137–420) 460 (320–580) | 0.632 0.016 | 41 (−140–72) 118 (85–147) | |
| p-value 2 | 0.285 | 0.196 | / | 0.005 | |
| β2-microglobuline (mcg/L) | Uncomplicat-ed CD RCD | 459 (322–552) 3375 (2626–5542) | 394 (302–470) 5460 (3850–7620) | <0.001 <0.001 | −24 (−75–−2) 1620 (1020–2054) |
| p-value 1 | <0.001 | <0.001 | / | <0.001 | |
| RCD 1 RCD 2 | 3321 (2613–5340) 3840 (2655–5542) | 5740 (3862–7240) 4700 (3850–7620) | <0.001 0.015 | 1685 (1068–2172) 1211 (860–2054) | |
| p-value 2 | 0.487 | 0.456 | / | 0.431 | |
| LDH (mUI/mL) | Uncomplicat-ed CD RCD | 167 (146–192) 220 (168–317) | NA NA | / / | NA NA |
| p-value 1 | <0.001 | / | |||
| RCD 1 RCD 2 | 218 (163–312) 289 (179–395) | NA NA | / / | NA NA | |
| p-value 2 | 0.131 | / | |||
| Albumin (g/dL) | Uncomlicate-d CD RCD | 4.3 (3.8–5.2) 3.2 (2.8–4.0) | NA NA | / / | NA NA |
| p-value 1 | <0.001 | / | |||
| RCD 1 RCD 2 | 3.2 (2.8–4.0) 3.1 (2.4–3.8) | NA NA | / / | NA NA | |
| p-value 2 | 0.360 | / |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenti, M.V.; Aronico, N.; Giuffrida, P.; Antoci, V.; Santacroce, G.; Vanoli, A.; Klersy, C.; Corazza, G.R.; Di Sabatino, A. Serum Markers of Refractoriness and Enteropathy-Associated T-Cell Lymphoma in Coeliac Disease. Cancers 2021, 13, 2289. https://doi.org/10.3390/cancers13102289
Lenti MV, Aronico N, Giuffrida P, Antoci V, Santacroce G, Vanoli A, Klersy C, Corazza GR, Di Sabatino A. Serum Markers of Refractoriness and Enteropathy-Associated T-Cell Lymphoma in Coeliac Disease. Cancers. 2021; 13(10):2289. https://doi.org/10.3390/cancers13102289
Chicago/Turabian StyleLenti, Marco Vincenzo, Nicola Aronico, Paolo Giuffrida, Valentina Antoci, Giovanni Santacroce, Alessandro Vanoli, Catherine Klersy, Gino Roberto Corazza, and Antonio Di Sabatino. 2021. "Serum Markers of Refractoriness and Enteropathy-Associated T-Cell Lymphoma in Coeliac Disease" Cancers 13, no. 10: 2289. https://doi.org/10.3390/cancers13102289
APA StyleLenti, M. V., Aronico, N., Giuffrida, P., Antoci, V., Santacroce, G., Vanoli, A., Klersy, C., Corazza, G. R., & Di Sabatino, A. (2021). Serum Markers of Refractoriness and Enteropathy-Associated T-Cell Lymphoma in Coeliac Disease. Cancers, 13(10), 2289. https://doi.org/10.3390/cancers13102289