Isolation and Enumeration of CTC in Colorectal Cancer Patients: Introduction of a Novel Cell Imaging Approach and Comparison to Cellular and Molecular Detection Techniques

 ,
,  and
and
Simple Summary
Abstract

1. Introduction
2. Results
2.1. Patients and Demographics
2.2. Spiking Experiments and Validation of Cytological and RT-qPCR Detection Techniques
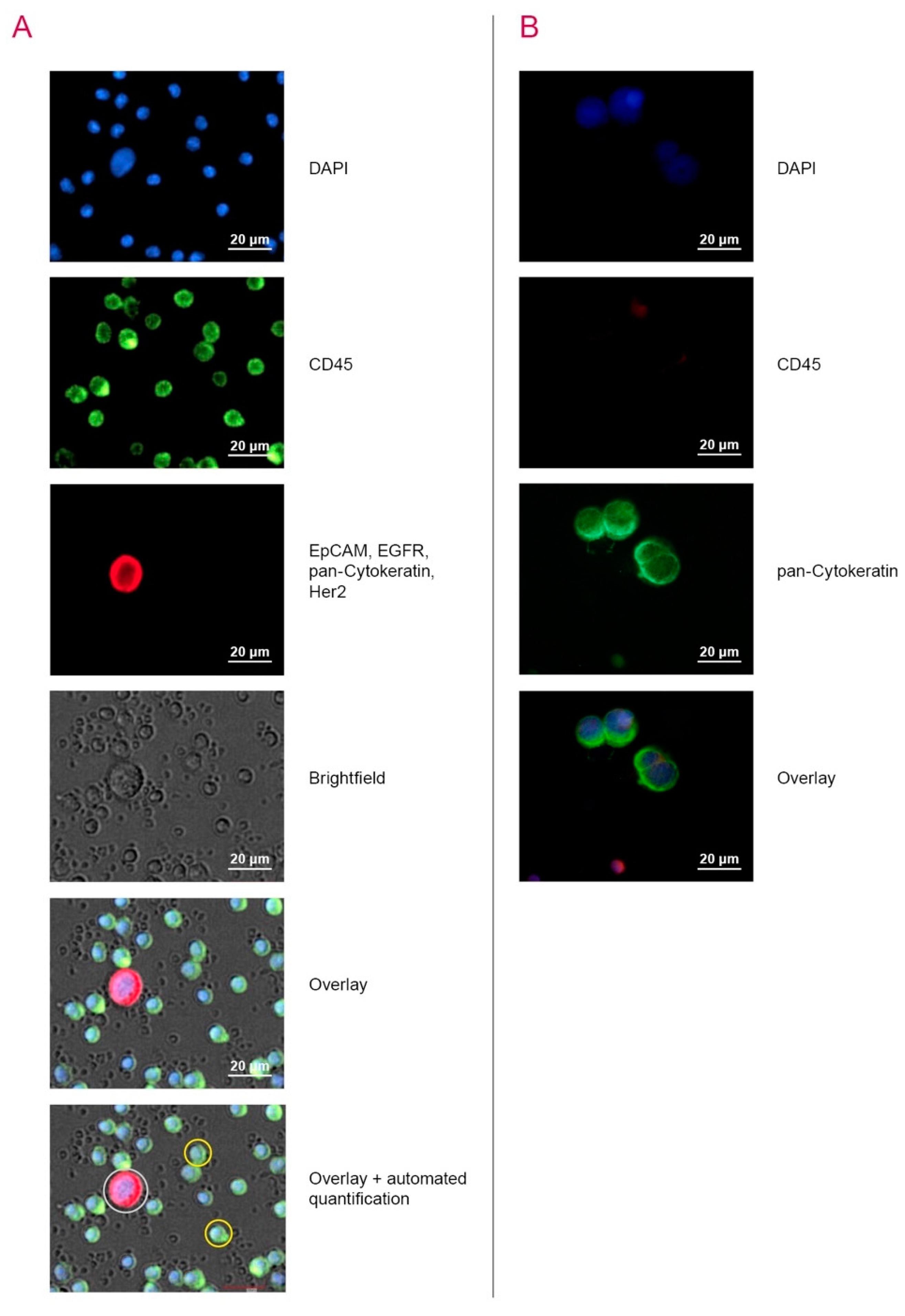
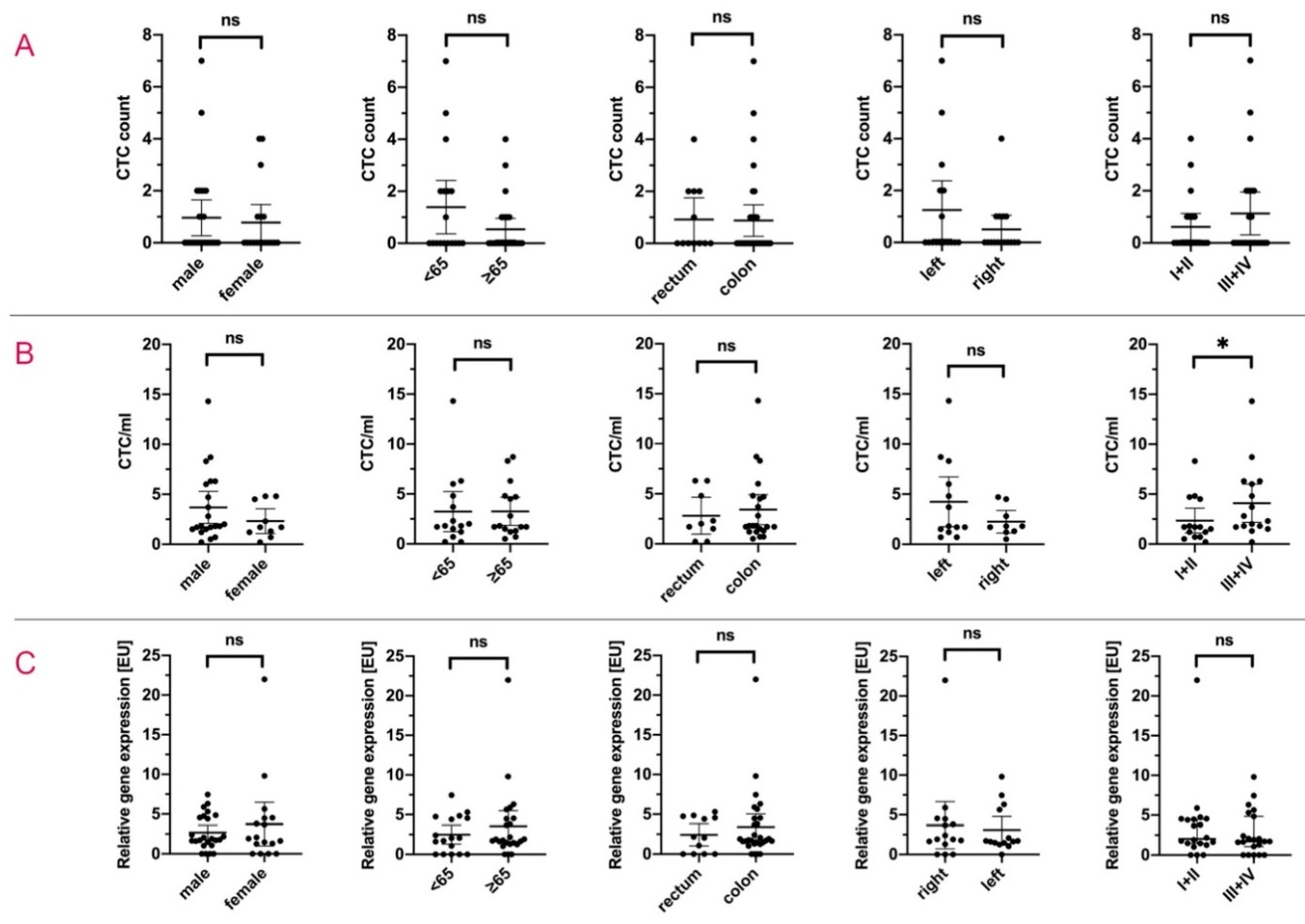
2.3. Detection of CTC by Automated Microscopy with the Cell Imager NYONE®
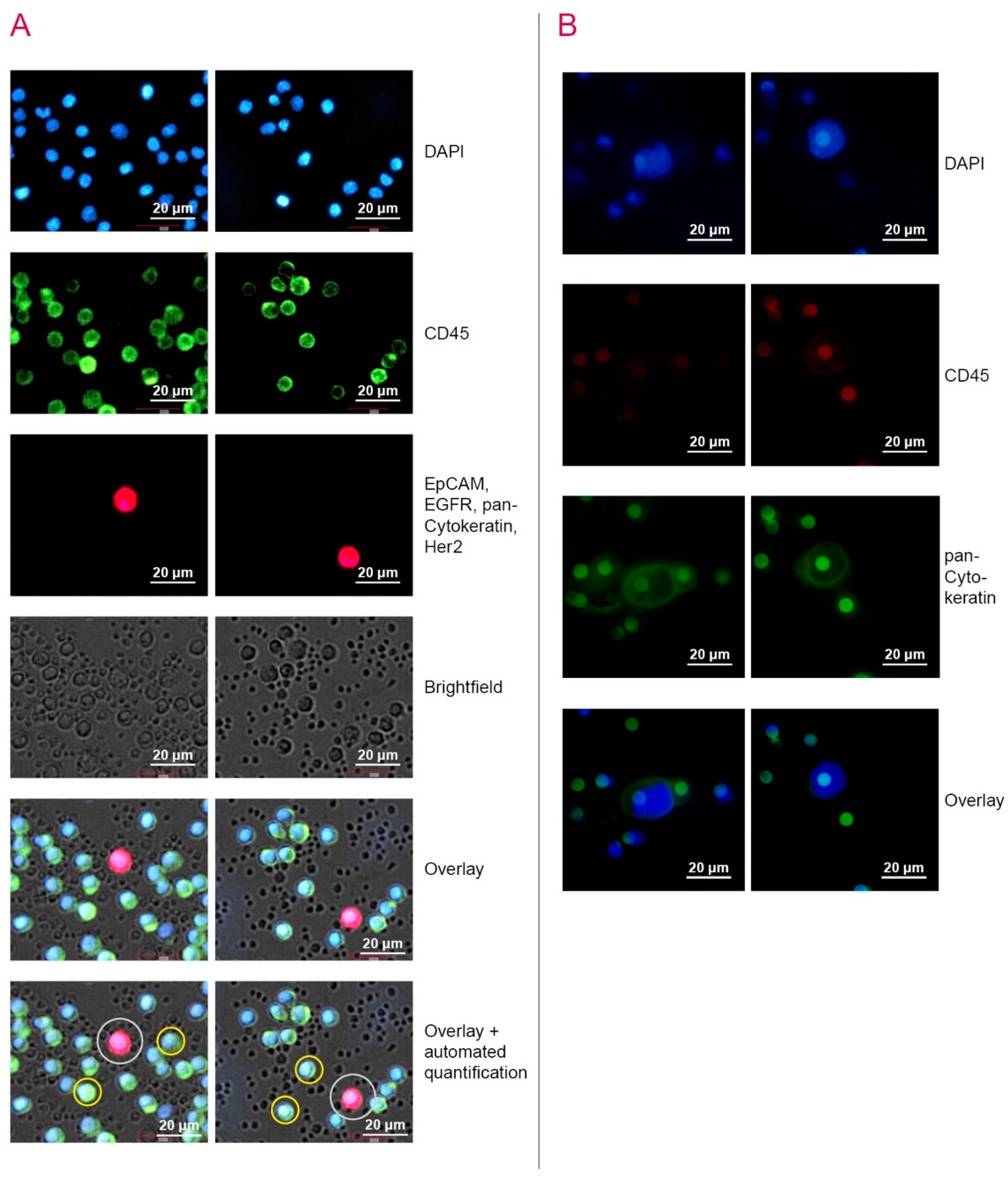
2.4. Capture and Detection of CTC by ScreenCell® Cyto IS Device
2.5. Relative Quantification of the CTC Load by CK20 RT-qPCR
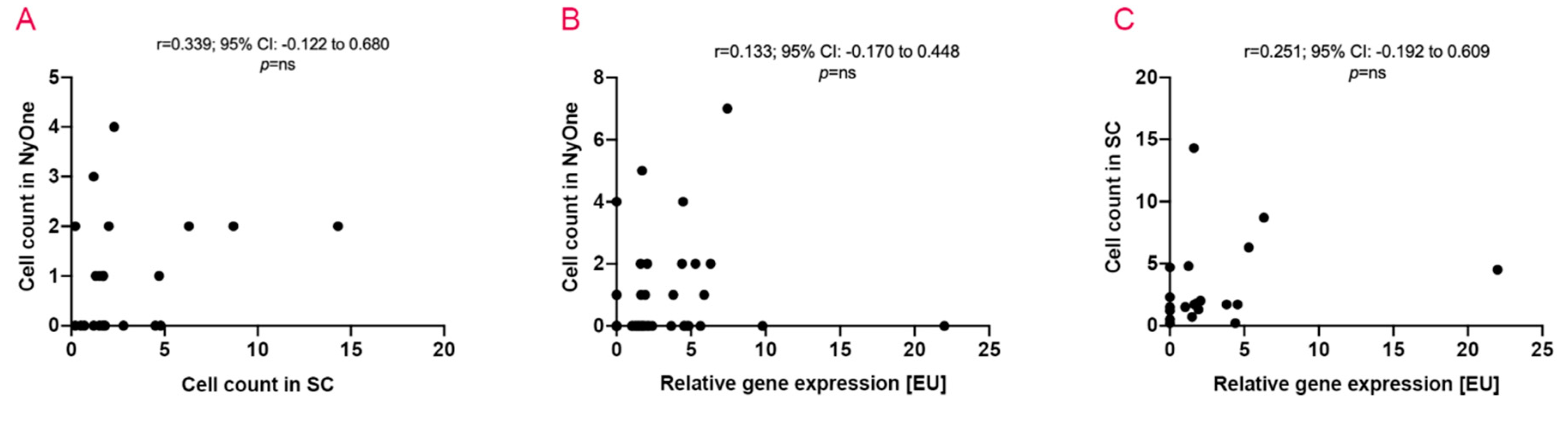
2.6. The Coherence of Applied Detection Methods
3. Discussion
4. Materials and Methods
4.1. Patient/Proband Recruitment and Sample Preparation
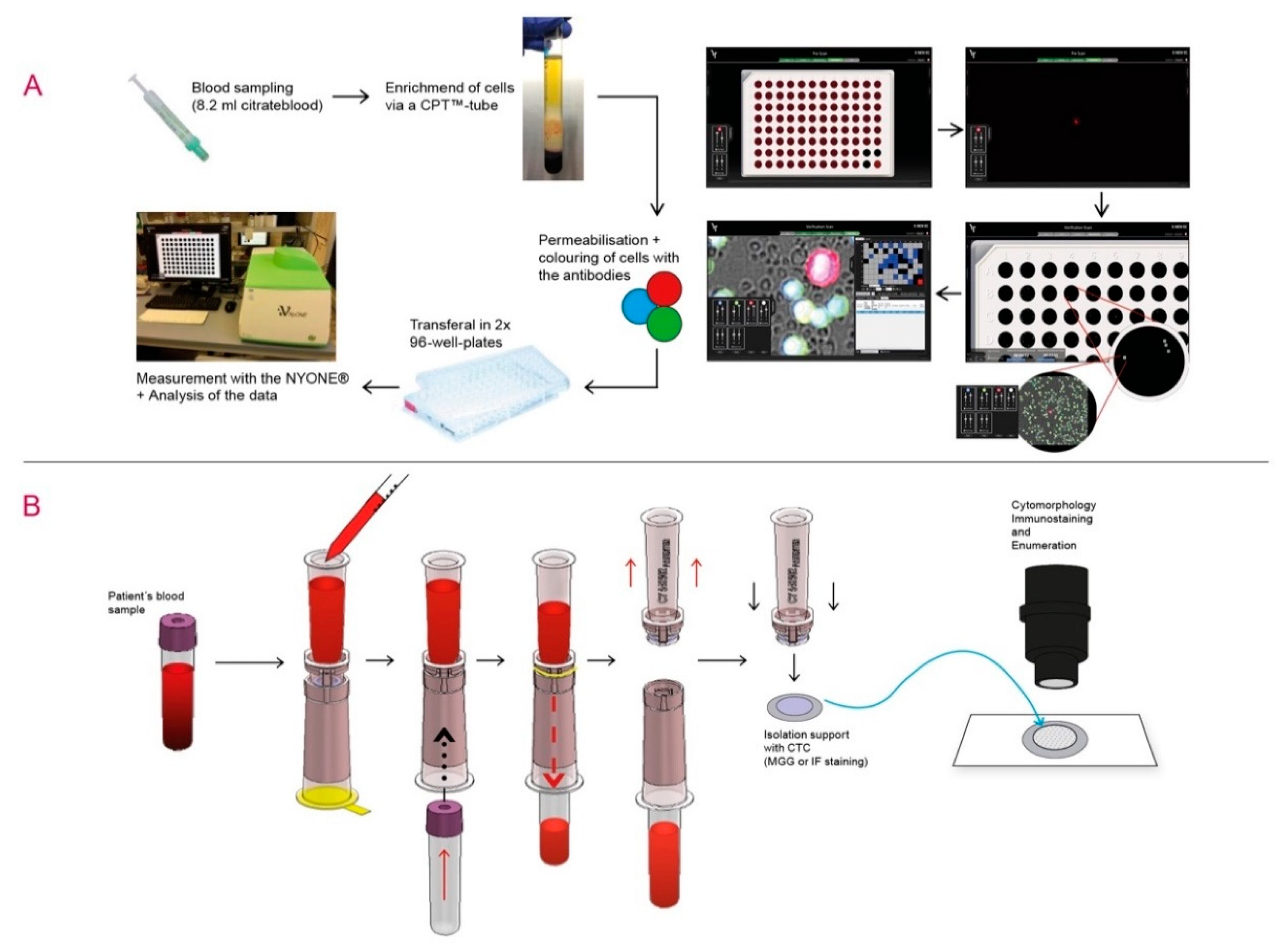
4.2. Sample Analysis by IF Staining and Semi-Automated Microscopy—NYONE®
4.3. Sample Analysis by Size-Dependent Filtration and IF Staining—ScreenCell®
4.4. Sample Analysis by Molecular Analysis of mRNA—Semi-Quantitative CK20 RT-qPCR
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| CK-20 | Cytokeratin-20 |
| CRC | Colorectal cancer |
| CTC | Circulating tumour cells |
| EGFR | Epithelial Growth Factor Receptor |
| EMT | Epithelial-Mesenchymal-Transition |
| EpCAM | Epithelial adhesion molecule |
| EU | expression units |
| pan-CK | pan-Cytokeratin |
| RT-qPCR | Real Time quantitative Polymerase Chain Reaction |
| UICC | Union internationale contre le cancer |
References
- Arnold, M.; Sierra, M.S.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global patterns and trends in colorectal cancer incidence and mortality. Gut 2017, 66, 683–691. [Google Scholar] [CrossRef]
- Schreuders, E.H.; Ruco, A.; Rabeneck, L.; Schoen, R.E.; Sung, J.J.Y.; Young, G.P.; Kuipers, E.J. Colorectal cancer screening: A global overview of existing programmes. Gut 2015, 64, 1637–1649. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef]
- Le Tourneau, C.; Delord, J.-P.; Gonçalves, A.; Gavoille, C.; Dubot, C.; Isambert, N.; Campone, M.; Trédan, O.; Massiani, M.-A.; Mauborgne, C.; et al. Molecularly targeted therapy based on tumour molecular profiling versus conventional therapy for advanced cancer (SHIVA): A multicentre, open-label, proof-of-concept, randomised, controlled phase 2 trial. Lancet Oncol. 2015, 16, 1324–1334. [Google Scholar] [CrossRef]
- Sicklick, J.K.; Kato, S.; Okamura, R.; Schwaederle, M.; Hahn, M.E.; Williams, C.B.; De, P.; Krie, A.; Piccioni, D.E.; Miller, V.A.; et al. Molecular profiling of cancer patients enables personalized combination therapy: The I-PREDICT study. Nat. Med. 2019, 25, 744–750. [Google Scholar] [CrossRef]
- Pantel, K.; Alix-Panabières, C. Liquid biopsy and minimal residual disease—Latest advances and implications for cure. Nat. Rev. Clin. Oncol 2019, 16, 409–424. [Google Scholar] [CrossRef]
- Alix-Panabières, C.; Pantel, K. Circulating tumor cells: Liquid biopsy of cancer. Clin. Chem. 2013, 59, 110–118. [Google Scholar] [CrossRef]
- Hendricks, A.; Eggebrecht, G.-L.; Bernsmeier, A.; Geisen, R.; Dall, K.; Trauzold, A.; Becker, T.; Kalthoff, H.; Schafmayer, C.; Röder, C.; et al. Identifying patients with an unfavorable prognosis in early stages of colorectal carcinoma. Oncotarget 2018, 9, 27423–27434. [Google Scholar] [CrossRef]
- Hinz, S.; Röder, C.; Tepel, J.; Hendricks, A.; Schafmayer, C.; Becker, T.; Kalthoff, H. Cytokeratin 20 positive circulating tumor cells are a marker for response after neoadjuvant chemoradiation but not for prognosis in patients with rectal cancer. BMC Cancer 2015, 15, 953. [Google Scholar] [CrossRef]
- Hinz, S.; Hendricks, A.; Wittig, A.; Schafmayer, C.; Tepel, J.; Kalthoff, H.; Becker, T.; Röder, C. Detection of circulating tumor cells with CK20 RT-PCR is an independent negative prognostic marker in colon cancer patients—A prospective study. BMC Cancer 2017, 17, 53. [Google Scholar] [CrossRef]
- Huang, X.; Gao, P.; Song, Y.; Sun, J.; Chen, X.; Zhao, J.; Xu, H.; Wang, Z. Meta-analysis of the prognostic value of circulating tumor cells detected with the CellSearch system in colorectal cancer. BMC Cancer 2015, 15, 202. [Google Scholar] [CrossRef]
- Normanno, N.; Cervantes, A.; Ciardiello, F.; De Luca, A.; Pinto, C. The liquid biopsy in the management of colorectal cancer patients: Current applications and future scenarios. Cancer Treat. Rev. 2018, 70, 1–8. [Google Scholar] [CrossRef]
- Lv, Q.; Gong, L.; Zhang, T.; Ye, J.; Chai, L.; Ni, C.; Mao, Y. Prognostic value of circulating tumor cells in metastatic breast cancer: A systemic review and meta-analysis. Clin. Transl. Oncol. 2016, 18, 322–330. [Google Scholar] [CrossRef]
- Zhou, Y.; Bian, B.; Yuan, X.; Xie, G.; Ma, Y.; Shen, L. Prognostic value of circulating tumor cells in ovarian cancer: A meta-analysis. PLoS ONE 2015, 10, e0130873. [Google Scholar] [CrossRef]
- Ma, X.; Xiao, Z.; Li, X.; Wang, F.; Zhang, J.; Zhou, R.; Wang, J.; Liu, L. Prognostic role of circulating tumor cells and disseminated tumor cells in patients with prostate cancer: A systematic review and meta-analysis. Tumour Biol. 2014, 35, 5551–5560. [Google Scholar] [CrossRef]
- Bork, U.; Rahbari, N.N.; Schölch, S.; Reissfelder, C.; Kahlert, C.; Büchler, M.W.; Weitz, J.; Koch, M. Circulating tumour cells and outcome in non-metastatic colorectal cancer: A prospective study. Br. J. Cancer 2015, 112, 1306–1313. [Google Scholar] [CrossRef]
- Kalluri, R.; Weinberg, R.A. The basics of epithelial-mesenchymal transition. J. Clin. Invest. 2009, 119, 1420–1428. [Google Scholar] [CrossRef]
- Joosse, S.A.; Hannemann, J.; Spötter, J.; Bauche, A.; Andreas, A.; Müller, V.; Pantel, K. Changes in keratin expression during metastatic progression of breast cancer: Impact on the detection of circulating tumor cells. Clin. Cancer Res. 2012, 18, 993–1003. [Google Scholar] [CrossRef]
- Gorges, T.M.; Tinhofer, I.; Drosch, M.; Röse, L.; Zollner, T.M.; Krahn, T.; von Ahsen, O. Circulating tumour cells escape from EpCAM-based detection due to epithelial-to-mesenchymal transition. BMC Cancer 2012, 12, 178. [Google Scholar] [CrossRef]
- Zhang, D.; Zhao, L.; Zhou, P.; Ma, H.; Huang, F.; Jin, M.; Dai, X.; Zheng, X.; Huang, S.; Zhang, T. Circulating tumor microemboli (CTM) and vimentin+ circulating tumor cells (CTCs) detected by a size-based platform predict worse prognosis in advanced colorectal cancer patients during chemotherapy. Cancer Cell Int. 2017, 17, 6. [Google Scholar] [CrossRef]
- Tsutsuyama, M.; Nakanishi, H.; Yoshimura, M.; Oshiro, T.; Kinoshita, T.; Komori, K.; Shimizu, Y.; Ichinosawa, Y.; Kinuta, S.; Wajima, K.; et al. Detection of circulating tumor cells in drainage venous blood from colorectal cancer patients using a new filtration and cytology-based automated platform. PLoS ONE 2019, 14, e0212221. [Google Scholar] [CrossRef]
- Tan, K.; Leong, S.M.; Kee, Z.; Caramat, P.V.; Teo, J.; Blanco, M.V.M.; Koay, E.S.C.; Cheong, W.K.; Soh, T.I.-P.; Yong, W.P.; et al. Longitudinal monitoring reveals dynamic changes in circulating tumor cells (CTCs) and CTC-associated miRNAs in response to chemotherapy in metastatic colorectal cancer patients. Cancer Lett. 2018, 423, 1–8. [Google Scholar] [CrossRef]
- Yu, M.; Stott, S.; Toner, M.; Maheswaran, S.; Haber, D.A. Circulating tumor cells: Approaches to isolation and characterization. J. Cell Biol. 2011, 192, 373–382. [Google Scholar] [CrossRef]
- Meng, S.; Tripathy, D.; Frenkel, E.P.; Shete, S.; Naftalis, E.Z.; Huth, J.F.; Beitsch, P.D.; Leitch, M.; Hoover, S.; Euhus, D.; et al. Circulating tumor cells in patients with breast cancer dormancy. Clin. Cancer Res. 2004, 10, 8152–8162. [Google Scholar] [CrossRef]
- Wong, S.C.C.; Chan, C.M.L.; Ma, B.B.Y.; Hui, E.P.; Ng, S.S.M.; Lai, P.B.S.; Cheung, M.T.; Lo, E.S.F.; Chan, A.K.C.; Lam, M.Y.Y.; et al. Clinical significance of cytokeratin 20-positive circulating tumor cells detected by a refined immunomagnetic enrichment assay in colorectal cancer patients. Clin. Cancer Res. 2009, 15, 1005–1012. [Google Scholar] [CrossRef]
- Kamiyama, H.; Noda, H.; Konishi, F.; Rikiyama, T. Molecular biomarkers for the detection of metastatic colorectal cancer cells. World J. Gastroenterol. 2014, 20, 8928–8938. [Google Scholar] [CrossRef]
- Gorges, T.M.; Stein, A.; Quidde, J.; Hauch, S.; Röck, K.; Riethdorf, S.; Joosse, S.A.; Pantel, K. Improved detection of circulating tumor cells in metastatic colorectal cancer by the combination of the CellSearch® system and the AdnaTest®. PLoS ONE 2016, 11, e0155126. [Google Scholar] [CrossRef]
- Van der Toom, E.E.; Verdone, J.E.; Gorin, M.A.; Pienta, K.J. Technical challenges in the isolation and analysis of circulating tumor cells. Oncotarget 2016, 7, 62754–62766. [Google Scholar] [CrossRef]
- Todenhöfer, T.; Hennenlotter, J.; Feyerabend, S.; Aufderklamm, S.; Mischinger, J.; Kühs, U.; Gerber, V.; Fetisch, J.; Schilling, D.; Hauch, S.; et al. Preliminary experience on the use of the Adnatest® system for detection of circulating tumor cells in prostate cancer patients. Anticancer Res. 2012, 32, 3507–3513. [Google Scholar]
- Obermayr, E.; Bednarz-Knoll, N.; Orsetti, B.; Weier, H.-U.; Lambrechts, S.; Castillo-Tong, D.C.; Reinthaller, A.; Braicu, E.I.; Mahner, S.; Sehouli, J.; et al. Circulating tumor cells: Potential markers of minimal residual disease in ovarian cancer? A study of the OVCAD consortium. Oncotarget 2017, 8, 106415–106428. [Google Scholar] [CrossRef]
- Nicolazzo, C.; Raimondi, C.; Francescangeli, F.; Ceccarelli, S.; Trenta, P.; Magri, V.; Marchese, C.; Zeuner, A.; Gradilone, A.; Gazzaniga, P. EpCAM-expressing circulating tumor cells in colorectal cancer. Int. J. Biol. Markers 2017, 32, e415–e420. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Total N (%) | NYONE® N (%) | ScreenCell® N (%) | CK20 RT-qPCR N (%) |
|---|---|---|---|---|
| 57 (100) | 44 (100) | 31 (100) | 41 (100) | |
| Gender | ||||
| Male | 36 (63.2) | 26 (59.1) | 21 (67.7) | 24 (58.5) |
| Female | 21 (36.8) | 18 (40.9) | 10 (32.3) | 17 (41.5) |
| Age | ||||
| Median (range) | 66 (42–89) | 66 (45–89) | 66 (42–89) | 68 (45–89) |
| <65 | 27 (47.4) | 18 (40.9) | 15 (48.4) | 17 (41.5) |
| ≥65 | 30 (52.6) | 26 (59.1) | 16 (51.6) | 24 (58.5) |
| Tumour site | ||||
| colon | 38 (66.7) | 32 (72.7) | 22 (71.0) | 29 (70.7) |
| right | 17 (44.7) | 16 (50.0) | 9 (40.9) | 15 (51.7) |
| left | 21 (55.3) | 16 (50.0) | 13 (59.1) | 14 (48.3) |
| Rectum | 19 (33.3) | 12 (27.3) | 9 (29.0) | 12 (29.3) |
| UICC stage | ||||
| I | 15 (26.3) | 12 (27.3) | 9 (29.0) | 12 (29.3) |
| II | 10 (17.5) | 9 (20.5) | 6 (19.4) | 8 (19.5) |
| III | 24 (42.1) | 18 (40.9) | 12 (38.7) | 16 (39.0) |
| IV | 8 (14.0) | 5 (11.4) | 4 (12.9) | 5 (12.2) |
| Parameters | NYONE® | ScreenCell® | CK20 RT-qPCR | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Positive N (%) | Mean (SD) | p | Positive N (%) | Mean (SD) | p | Positive N (%) | Mean (SD) | p | |
| Total | 16/44 (36.4) | 0.89 (1.57) | 31/31 (100) | 3.25 (3.10) | 33/41 (80.5) | 3.11 (3.81) | |||
| Gender | |||||||||
| Male | 10/26 (38.5) | 0.96 (1.71) | 0.708 | 21/21 (100) | 3.69 (3.52) | 0.257 | 20/24 (83.3) | 2.67 (2.19) | 0.383 |
| Female | 6/18 (33.3) | 0.78 (1.40) | 10/10 (100) | 2.32 (1.74) | 13/17 (76.5) | 3.74 (5.35) | |||
| Age | |||||||||
| <65 | 8/18 (44.4) | 1.39 (2.06) | 0.078 | 15/15 (100) | 3.23 (3.62) | 0.980 | 12/17 (70.6) | 2.48 (2.31) | 0.379 |
| ≥65 | 8/26 (30.8) | 0.54 (1.03) | 16/16 (100) | 3.26 (2.65) | 21/24 (87.5) | 3.56 (4.58) | |||
| Tumour site | |||||||||
| Rectum | 5/12 (41.7) | 0.92 (1.31) | 0.939 | 9/9 (100) | 2.81 (2.39) | 0.624 | 8/12 (66.7) | 2.43 (2.20) | 0.466 |
| colon | 11/32 (34.4) | 0.88 (1.68) | 22/22 (100) | 3.43 (3.38) | 25/29 (86.2) | 3.40 (4.30) | |||
| right | 5/16 (31.3) | 0.50 (1.03) | 0.212 | 9/9 (100) | 2.26 (1.46) | 0.182 | 12/15 (80.0) | 3.69 (5.37) | 0.713 |
| left | 6/16 (37.5) | 1.25 (2.11) | 13/13 (100) | 4.24 (4.10) | 13/14 (92.9) | 3.08 (2.94) | |||
| UICC stage | |||||||||
| I + II | 3/12 (25.0) | 0.58 (1.24) | 0.503 | 15/15 (100) | 2.35 (2.24) | 0.039 | 11/12 (91.7) | 3.54 (4.70) | 0.491 |
| III + IV | 6/18 (33.3) | 1.06 (1.89) | 16/16 (100) | 4.09 (3.60) | 13/16 (81.3) | 2.71 (2.76) | |||
| Parameters | NYONE® | ScreenCell® | CK20 RT-qPCR | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Positive N (%) | Mean (SD) | p | Positive N (%) | Mean (SD) | p | Positive N (%) | Mean (SD) | p | |
| Total | 11/21 (52.4) | 0.90 (1.03) | 21/21 (100) | 3.01 (3.16) | 15/21 (71.4) | 2.90 (3.81) | |||
| Gender | |||||||||
| Male | 7/14 (50.0) | 0.86 (0.95) | 0.785 | 14/14 (100) | 3.34 (3.97) | 0.541 | 10/14 (71.4) | 2.16 (2.13) | 0.328 |
| Female | 4/7 (57.1) | 1.00 (1.41) | 7/7 (100) | 2.36 (1.69) | 5/7 (71.4) | 4.37 (7.88) | |||
| Age | |||||||||
| <65 | 6/9 (66.7) | 1.44 (1.33) | 0.047 | 9/9 (100) | 3.30 (4.50) | 0.746 | 5/9 (55.6) | 1.99 (2.22) | 0.464 |
| ≥65 | 5/12 (41.7) | 0.50 (0.67) | 12/12 (100) | 2.80 (2.40) | 10/12 (83.3) | 3.58 (6.04) | |||
| Tumour site | |||||||||
| Rectum | 5/7 (71.4) | 1.57 (1.40) | 0.045 | 7/7 (100) | 2.03 (2.06) | 0.356 | 4/7 (57.1) | 2.33 (2.39) | 0.709 |
| colon | 6/14 (42.9) | 0.57 (0.76) | 14/14 (100) | 3.51 (3.84) | 11/14 (78.6) | 3.18 (5.66) | |||
| right | 3/7 (42.9) | 0.43 (0.54) | 0.502 | 7/7 (100) | 2.24 (1.67) | 0.834 | 4/7 (57.1) | 4.22 (7.96) | 0.517 |
| left | 3/7 (42.9) | 0.71 (0.95) | 7/7 (100) | 2.03 (2.06) | 7/7 (100) | 2.15 (1.85) | |||
| UICC stage | |||||||||
| I + II | 4/12 (33.3) | 0.42 (0.67) | 0.017 | 8/8 (100) | 2.08 (1.64) | 0.148 | 7/8 (87.5) | 3.50 (6.05) | 0.521 |
| III + IV | 7/9 (77.8) | 1.56 (1.24) | 6/6 (100) | 4.26 (4.65) | 4/6 (66.7) | 2.10 (2.28) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendricks, A.; Brandt, B.; Geisen, R.; Dall, K.; Röder, C.; Schafmayer, C.; Becker, T.; Hinz, S.; Sebens, S. Isolation and Enumeration of CTC in Colorectal Cancer Patients: Introduction of a Novel Cell Imaging Approach and Comparison to Cellular and Molecular Detection Techniques. Cancers 2020, 12, 2643. https://doi.org/10.3390/cancers12092643
Hendricks A, Brandt B, Geisen R, Dall K, Röder C, Schafmayer C, Becker T, Hinz S, Sebens S. Isolation and Enumeration of CTC in Colorectal Cancer Patients: Introduction of a Novel Cell Imaging Approach and Comparison to Cellular and Molecular Detection Techniques. Cancers. 2020; 12(9):2643. https://doi.org/10.3390/cancers12092643
Chicago/Turabian StyleHendricks, Alexander, Burkhard Brandt, Reinhild Geisen, Katharina Dall, Christian Röder, Clemens Schafmayer, Thomas Becker, Sebastian Hinz, and Susanne Sebens. 2020. "Isolation and Enumeration of CTC in Colorectal Cancer Patients: Introduction of a Novel Cell Imaging Approach and Comparison to Cellular and Molecular Detection Techniques" Cancers 12, no. 9: 2643. https://doi.org/10.3390/cancers12092643
APA StyleHendricks, A., Brandt, B., Geisen, R., Dall, K., Röder, C., Schafmayer, C., Becker, T., Hinz, S., & Sebens, S. (2020). Isolation and Enumeration of CTC in Colorectal Cancer Patients: Introduction of a Novel Cell Imaging Approach and Comparison to Cellular and Molecular Detection Techniques. Cancers, 12(9), 2643. https://doi.org/10.3390/cancers12092643