The Prognostic Value of MicroRNAs in Thyroid Cancers—A Systematic Review and Meta-Analysis


 , and
, and
Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy
2.2.1. Inclusion Criteria
- Longitudinal studies aiming to investigate the prognostic value of microRNA expression in TC patients;
- Studies with the following types of outcome available: overall survival (OS), tumor-specific survival (TSS), disease-free survival (DFS), recurrence-free survival (RFS), distant metastases-free survival (DMFS), progression-free survival (PFS); parameters of complicated course of the disease, such as residual, persistent, recurrent, and progressive disease;
- Studies with a minimum follow-up period of 12 months for the outcome of interest;
- Studies offering enough information to compute effect size;
- The full-text paper was available in English, French, or Russian (languages known by the authors).
2.2.2. Exclusion Criteria Included the Following:
- Studies about microRNAs expression in patients with other types of malignancies;
- Studies of participants with TC from diseases predisposing to malignancy;
- Review articles (narrative reviews, systematic reviews, and meta-analyses), letter to editor and correspondence without original data, dissertations and conferences abstracts;
- Full texts unavailable for review.
2.3. Data Extraction
- Publication information (first author, year of publication, country of origin),
- Patients’ characteristics (number of participants, age, histopathological typing of TC);
- miRNA detection information (miRNA type, sample type, expression status, assay type, cut-off values, normalization control);
- Prognosis information (the reported outcome, follow-up timing);
- Data for computing the effect size (hazard ratio (HR) or odds ratio (OR) with corresponding 95% confidence interval (CI) and log-rank P-value, reported directly or means, standard deviations, and sample size).
2.4. Assessment of Methodological Quality
2.5. Statistical Methods
2.6. Ethical Approval
3. Results
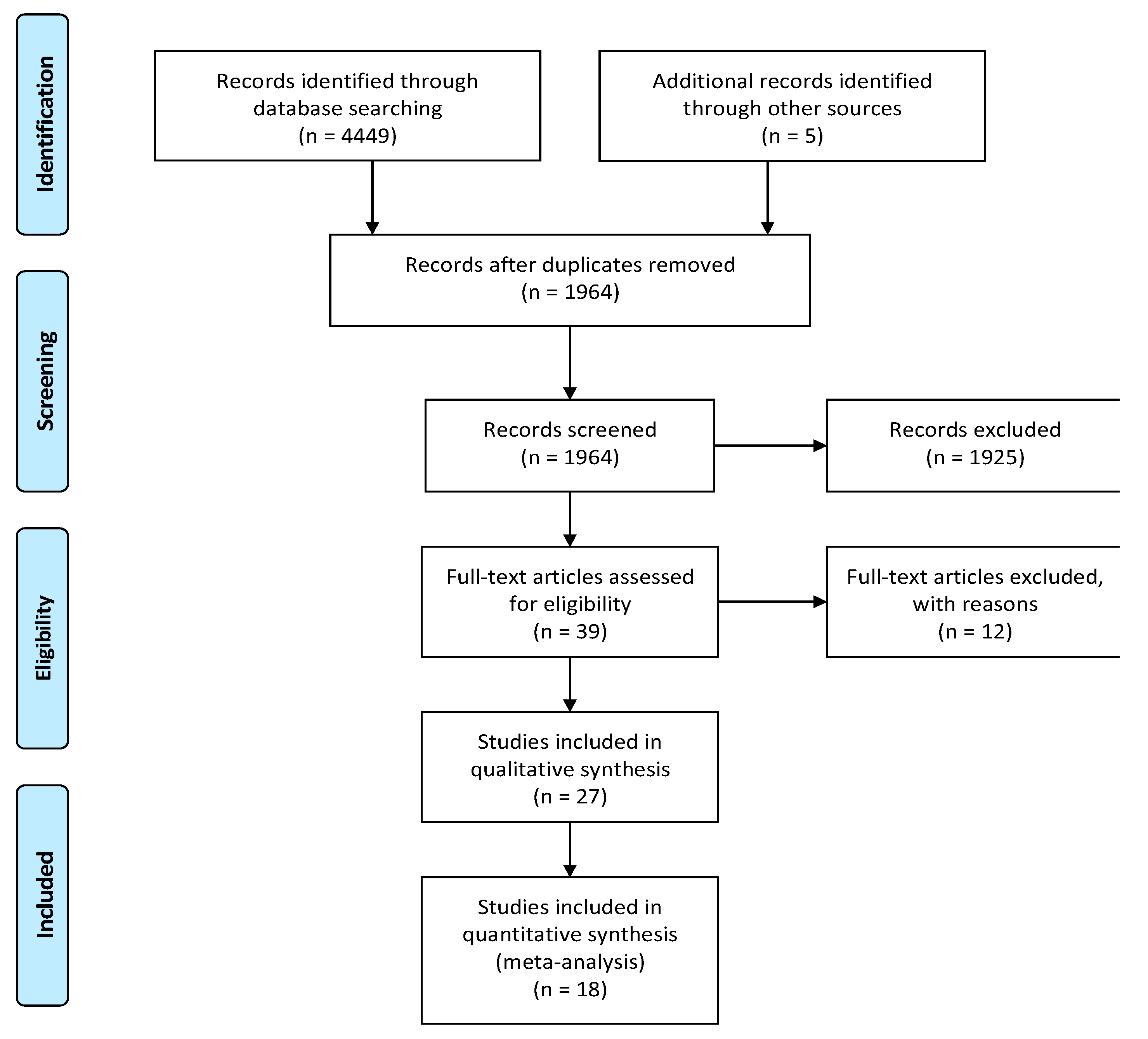
3.1. Literature Search
3.2. Participant and Study Characteristics
3.3. Excluded Studies
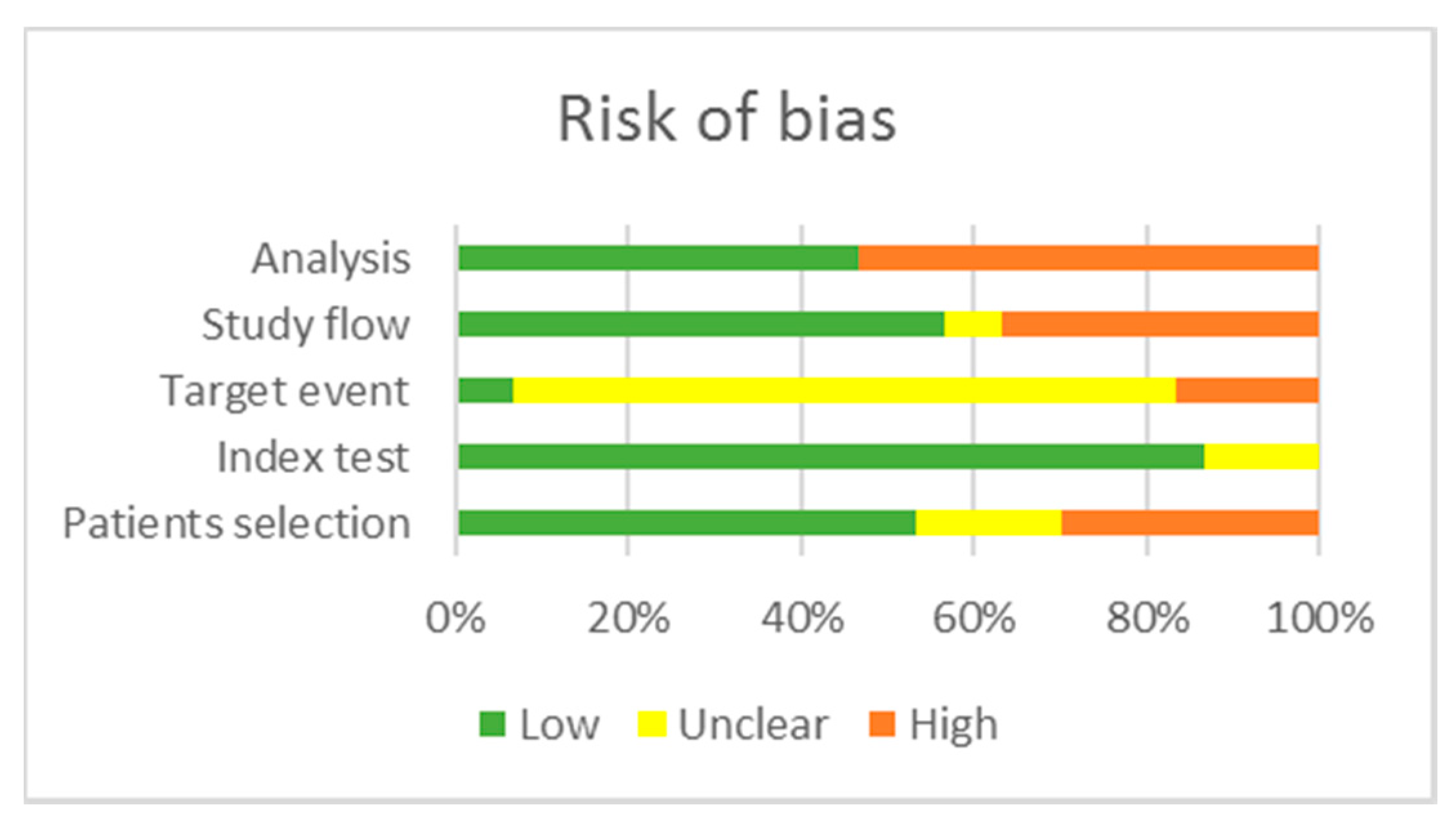
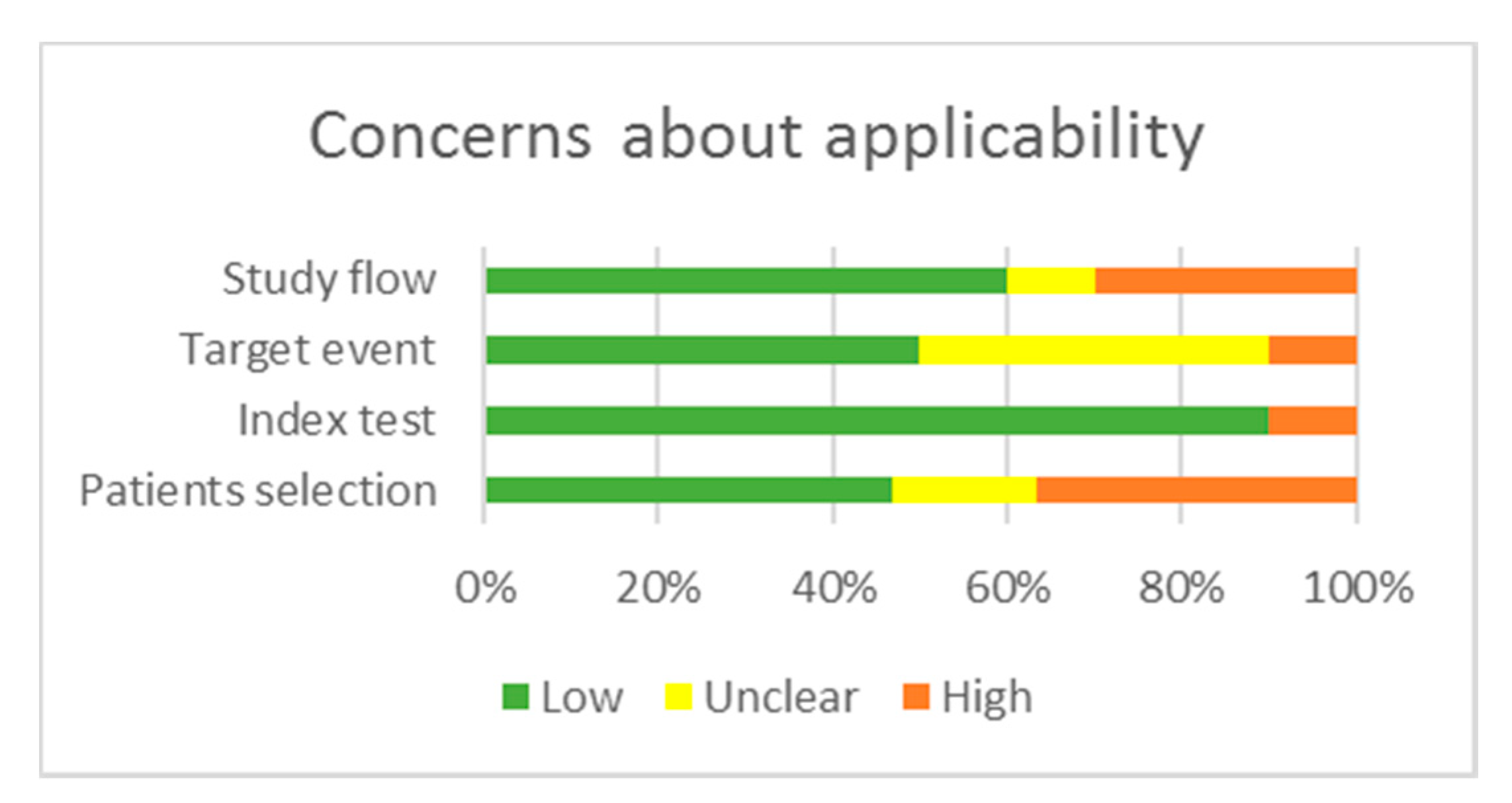
3.4. Quality Assessment
3.5. Key Results Regarding miRNAs and Prognosis
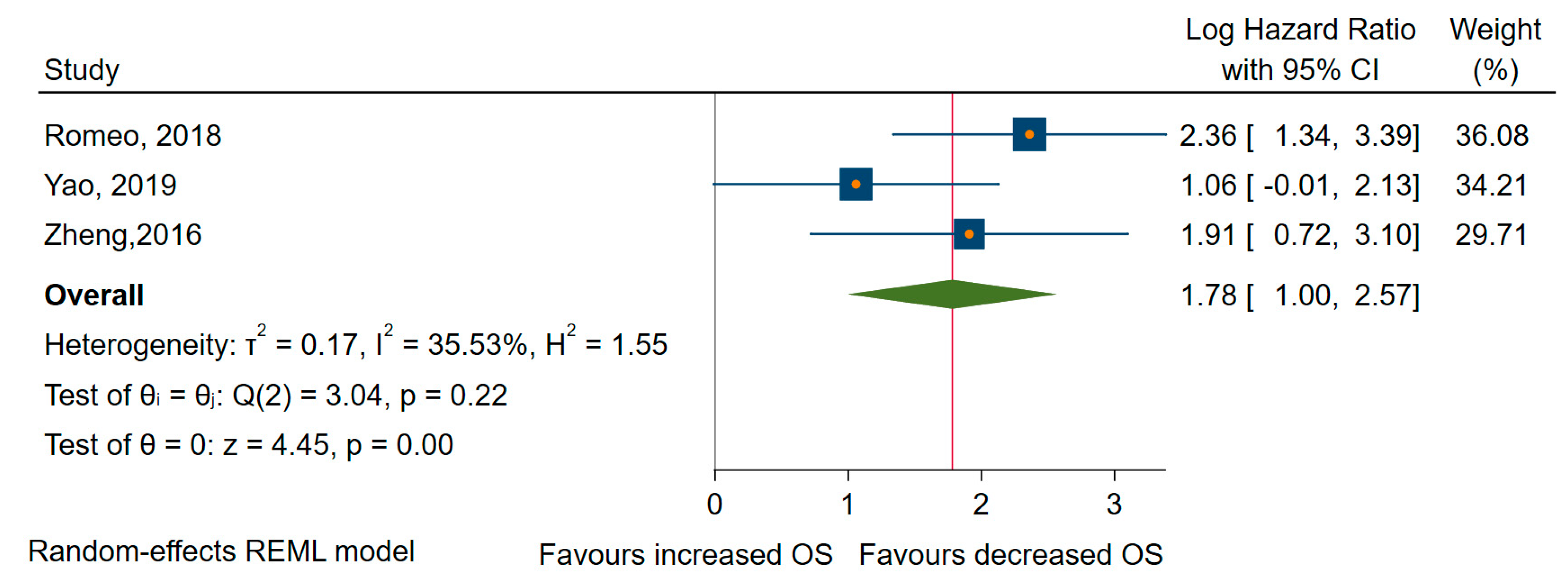
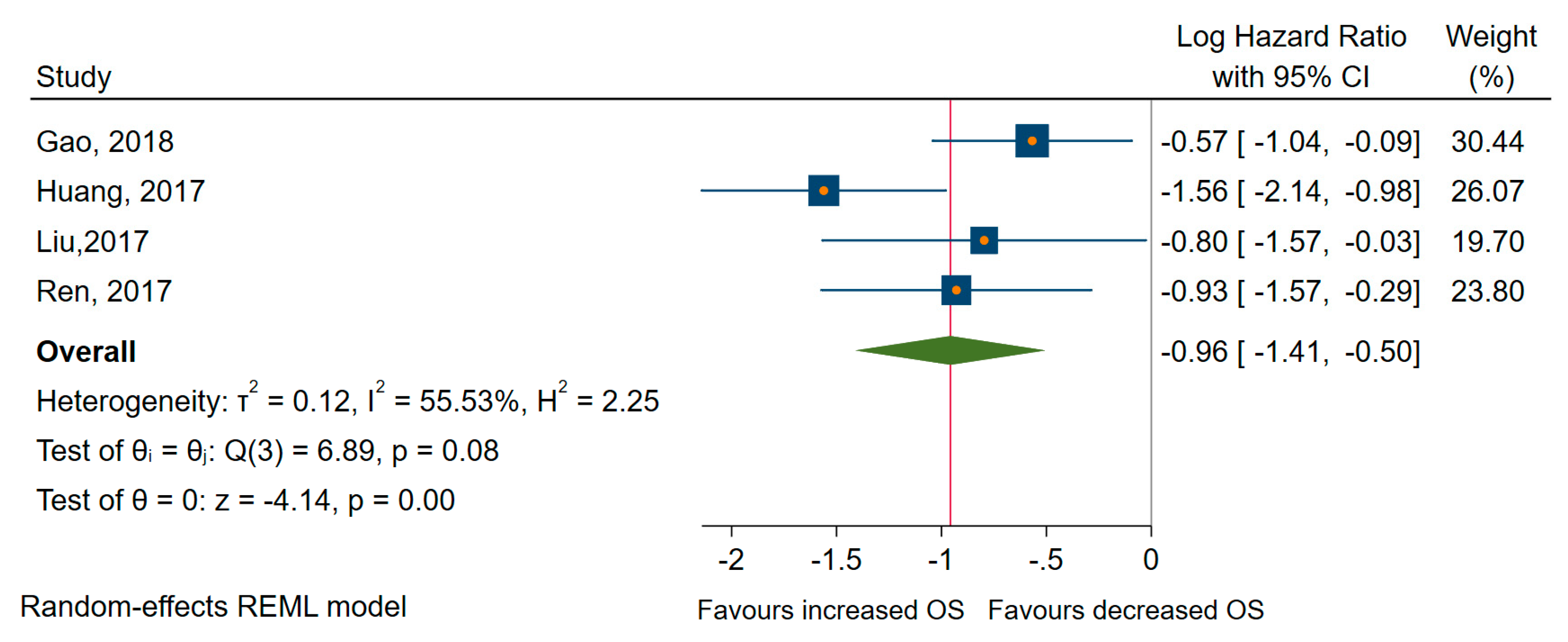
3.5.1. Dysregulated miRNAs Correlated with Survival Outcomes
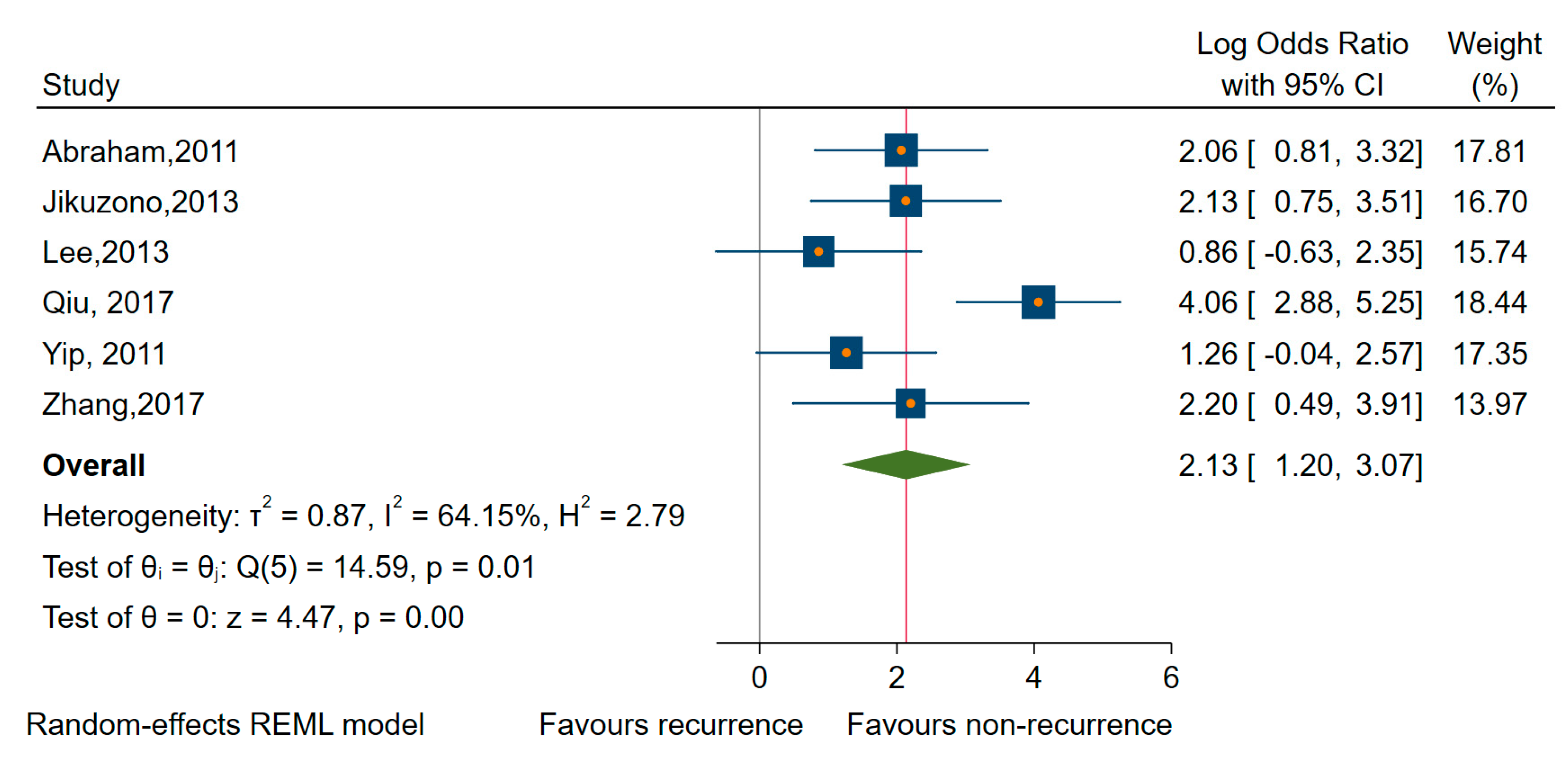
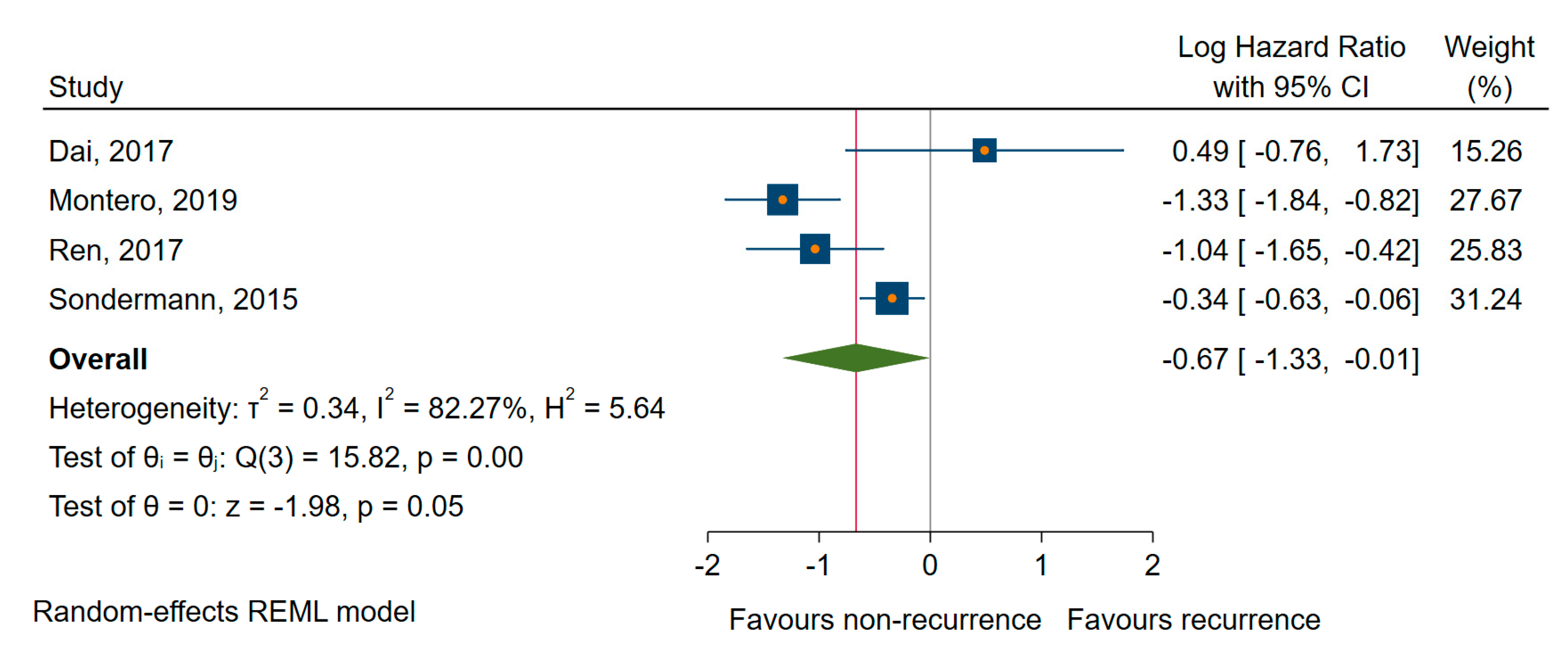
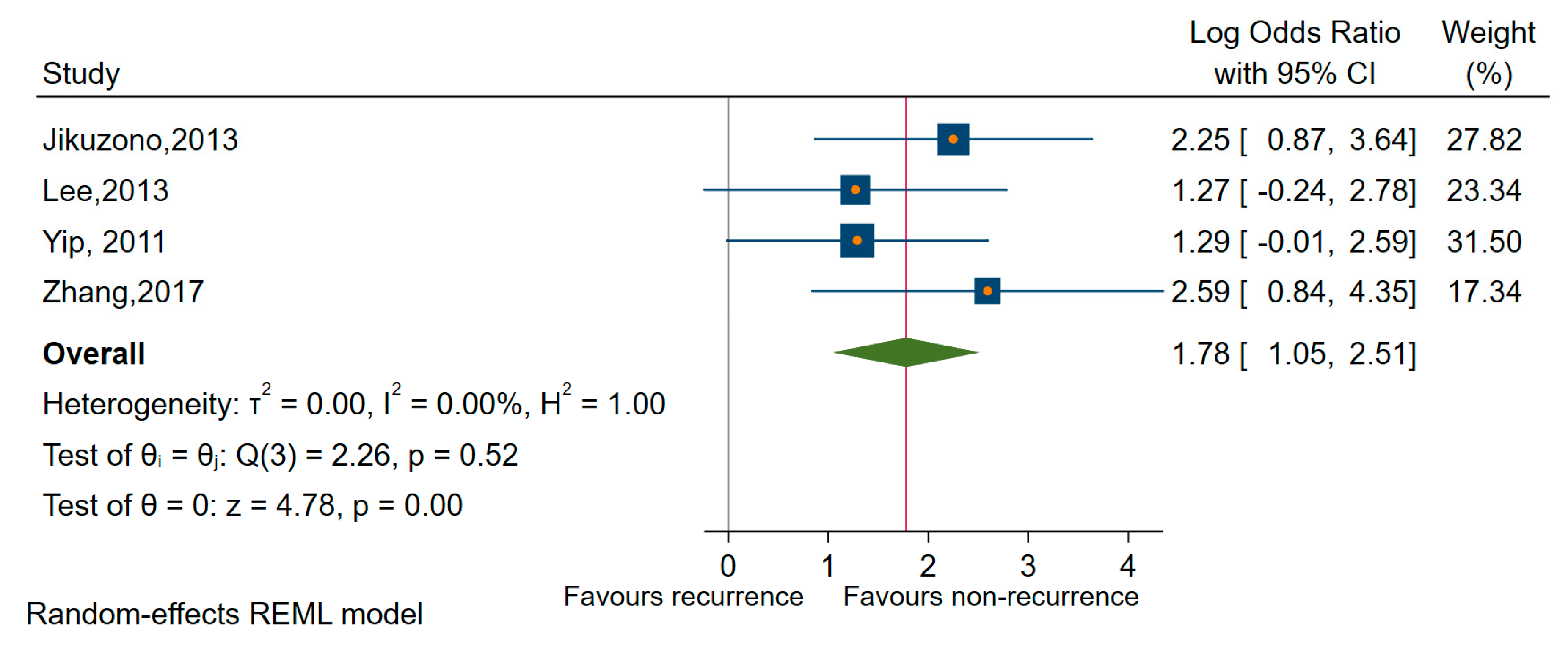
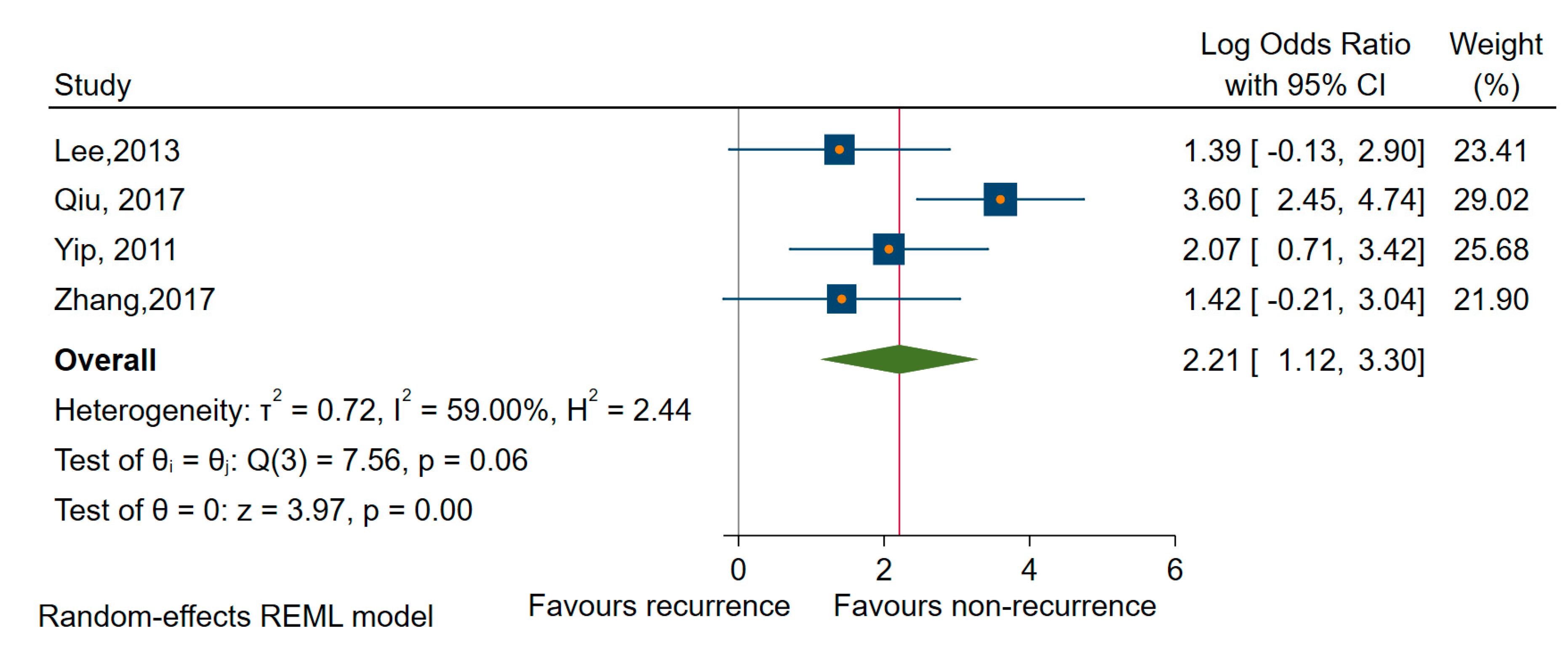
3.5.2. Dysregulated miRNAs Correlated with TC Recurrence
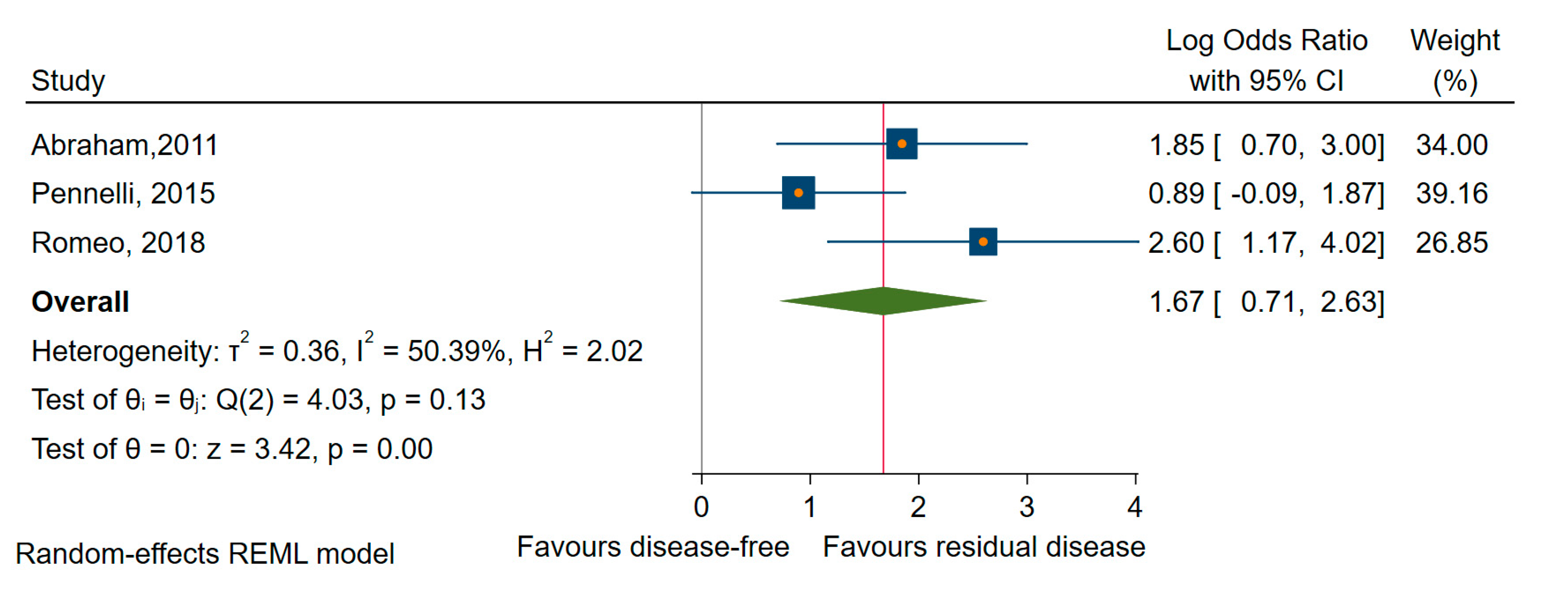
3.5.3. Dysregulated miRNAs Correlated with TC Progression, Persistence, and Residual Disease
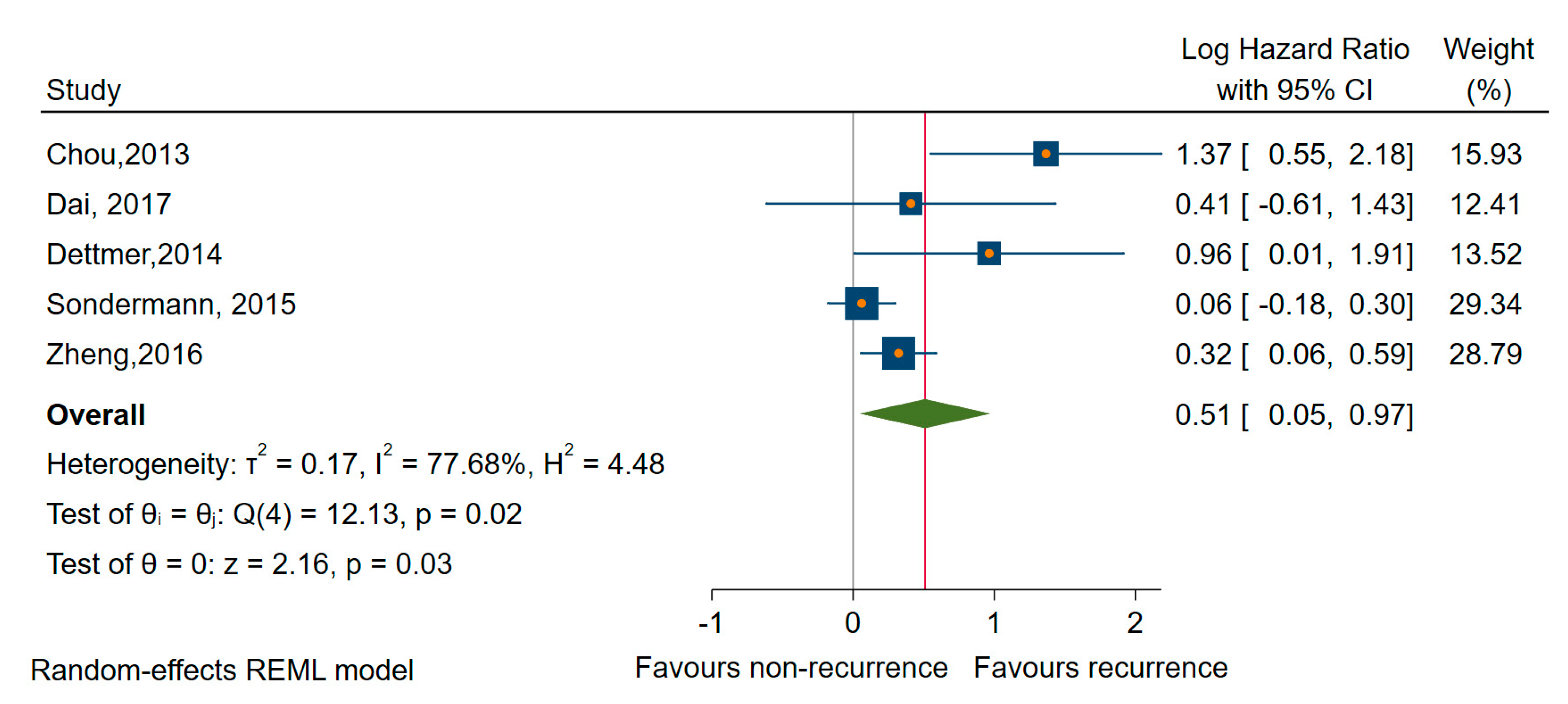
3.6. Meta-Analysis
3.6.1. The Meta-Analysis by the Type of miRNAs Deregulation
Upregulated miRNAs
Downregulated miRNAs
3.6.2. Sensitivity Analysis by Specific Types of miRNA
3.6.3. Sensitivity Analysis by the Histological Subtypes of TC
4. Discussion
5. Conclusions
6. Differences Between Protocol and Review
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Domain | Description | Signaling Question (Yes, No, Unclear) | Risk of Bias (High, Low, Unclear) | Concerns about Applicability (High, Low, Unclear) |
|---|---|---|---|---|
| Participant recruitment | Describe the method for recruiting participants. Describe participants (previous testing, presentation, the intended use of index test and setting) | Was there consecutive or random enrollment of participants? Do the participants represent the intended population? Did the study avoid inappropriate exclusions? | Could the selection of participants have introduced bias? | Are there concerns that the participants do not match the review question? |
| Index test | Describe index test (definition, method of measurement, interpretation) | Was the method and settings for performing the index test valid and reliable? Was the method and settings for performing the index test the same for all participants? If a threshold was used, was it prespecified? | Could the conduct or interpretation of the index test have introduced bias? | Are there concerns that the index test, its conduct, or its interpretation differ from the review question? |
| Target event | A clear definition of outcome is provided, including the duration of follow-up and level and extent of the outcome construct. | Was a clear definition of the outcome provided? Was the method used to measure the target event valid and reliable? Was the method used to measure the target event the same for all participants? Was the target event measured without knowledge of the index test results? | Could the measurement of the target event have introduced bias? | Are there concerns that the target event does not match the review question? |
| Study flow | Describe the time horizon from the index test to the target event. Describe any participants lost to follow-up or excluded from the 2x2 table. | Was the information on the target event available for all participants? Is the loss to follow-up related to the test results? | Could the study flow have introduced bias? | Are there concerns that the time horizon does not match the review question? |
| Analysis | Describe the statistical methods | Were the methods used to account for censoring? Was the statistical method appropriate for the design of the study? Were methods used to account for competing events? | Could analysis have introduced bias? |
Appendix B
| Type of Studies | Study, Reference | Risk of Bias | Applicability Concerns | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | TArget Event | Study Flow | Analysis | Patient Selection | Index Test | Target Event | Study Flow | ||
| Studies reporting time-to-event outcomes | Chen [57] | ↑ | ? | ? | ↑ | ↑ | ↓ | ↓ | ? | ↓ |
| Chou [58] | ↑ | ↓ | ↓ | ↑ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Dai [61] | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Dettmer [56] | ↑ | ↓ | ? | ↓ | ↓ | ↑ | ↑ | ↓ | ↑ | |
| Gao [59] | ↑ | ? | ? | ↑ | ↓ | ? | ↓ | ? | ↓ | |
| Huang [62] | ↓ | ↓ | ? | ? | ↓ | ↓ | ↓ | ? | ? | |
| Liu [65] | ↓ | ↓ | ? | ↓ | ↓ | ↑ | ↓ | ↓ | ↓ | |
| Montero [55] | ↑ | ↓ | ? | ↑ | ↑ | ↓ | ↑ | ? | ↓ | |
| Qiu [69] | ? | ? | ? | ↑ | ↑ | ↓ | ↓ | ? | ↑ | |
| Ren [75] | ? | ↓ | ? | ↓ | ↓ | ↓ | ↓ | ? | ↓ | |
| Romeo [78] | ↑ | ↓ | ? | ↑ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Sondermann [77] | ↑ | ↓ | ? | ↓ | ↓ | ↓ | ↓ | ↓ | ↓ | |
| Sun [70] | ↑ | ↓ | ? | ↑ | ↑ | ↑ | ↓ | ? | ↓ | |
| Wu [71] | ↓ | ↓ | ? | ↑ | ↑ | ↑ | ↓ | ? | ↓ | |
| Yao [72] | ↑ | ↓ | ? | ↑ | ↓ | ↑ | ↓ | ? | ↓ | |
| Zheng [74] | ↑ | ? | ? | ↓ | ↓ | ↑ | ↓ | ? | ↓ | |
| Studies reporting other parameters ofTC aggressive behavior | Abraham [42] | ? | ↓ | ? | ↑ | ↑ | ? | ↓ | ↓ | ↓ |
| Buda [54] | ↑ | ↓ | ↑ | ↑ | ↑ | ↑ | ↓ | ? | ↓ | |
| Cavedon [53] | ↓ | ↓ | ? | ? | ↑ | ↓ | ↓ | ↓ | ↑ | |
| Galuppini [60] | ↓ | ↓ | ? | ↓ | ↑ | ? | ↓ | ↓ | ↑ | |
| Jikuzono [63] | ↑ | ↓ | ? | ↓ | ↑ | ↑ | ↓ | ↑ | ↓ | |
| Lee [64] | ↓ | ↓ | ? | ↓ | ↓ | ↑ | ↓ | ↓ | ↑ | |
| Liu, Ch. [66] | ? | ↓ | ↑ | ↓ | ↑ | ↑ | ↓ | ↑ | ? | |
| Mian [67] | ↓ | ↓ | ↑ | ↓ | ↑ | ? | ↓ | ↑ | ↑ | |
| Montero [55] | ↑ | ↓ | ? | ? | ↑ | ↓ | ↑ | ↓ | ↑ | |
| Pennelli [68] | ↓ | ↓ | ? | ↓ | ↑ | ? | ↓ | ↓ | ↓ | |
| Qiu [69] | ? | ↓ | ↑ | ↓ | ↓ | ↓ | ↓ | ↓ | ↑ | |
| Romeo [78] | ↑ | ↓ | ? | ↓ | ↑ | ↓ | ↓ | ↓ | ↑ | |
| Yip [76] | ↑ | ↓ | ↑ | ↓ | ↓ | ↓ | ↓ | ? | ? | |
| Zhang [73] | ↑ | ↓ | ? | ↓ | ↑ | ↑ | ↓ | ↓ | ↑ | |
| ↓ Low-Risk ↑ High Risk ? Unclear Risk | ||||||||||
References
- Davies, L.; Welch, H.G. Increasing incidence of thyroid cancer in the United States, 1973–2002. JAMA 2006, 295, 2164–2167. [Google Scholar] [CrossRef]
- James, B.C.; Mitchell, J.M.; Jeon, H.D.; Vasilottos, N.; Grogan, R.H.; Aschebrook-Kilfoy, B. An update in international trends in incidence rates of thyroid cancer, 1973–2007. Cancer Causes Control 2018, 29, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Well Differentiated Thyroid Cancer—PubMed. Available online: https://pubmed.ncbi.nlm.nih.gov/12490765/ (accessed on 16 August 2020).
- Pasieka, J.L. Anaplastic thyroid cancer. Curr. Opin. Oncol. 2003, 15, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Hedayati, M.; Zarif Yeganeh, M.; Sheikhol Eslami, S.; Rezghi Barez, S.; Hoghooghi Rad, L.; Azizi, F. Predominant RET Germline Mutations in Exons 10, 11, and 16 in Iranian Patients with Hereditary Medullary Thyroid Carcinoma. J. Thyroid Res. 2011, 2011, 264248. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Schlumberger, M.J. Papillary and follicular thyroid carcinoma. N. Engl. J. Med. 1998, 338, 297–306. [Google Scholar] [CrossRef] [PubMed]
- Gilliland, F.D.; Hunt, W.C.; Morris, D.M.; Key, C.R. Prognostic factors for thyroid carcinoma. A population-based study of 15,698 cases from the Surveillance, Epidemiology and End Results (SEER) program 1973–1991. Cancer 1997, 79, 564–573. [Google Scholar] [CrossRef]
- Ito, Y.; Kakudo, K.; Hirokawa, M.; Fukushima, M.; Tomoda, C.; Inoue, H.; Kihara, M.; Higashiyama, T.; Uruno, T.; Takamura, Y.; et al. Clinical significance of extrathyroid extension to the parathyroid gland of papillary thyroid carcinoma. Endocr. J. 2009, 56, 251–255. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Hu, J.-L.; Chen, C.; Wang, Q.-L.; Fang, X.-H.; Zhang, Y.; Ge, M.-H. Vascular invasion is an independent prognostic factor for distant recurrence-free survival in papillary thyroid carcinoma: A matched-case comparative study. J. Clin. Pathol. 2016, 69, 872–877. [Google Scholar] [CrossRef]
- Durante, C.; Haddy, N.; Baudin, E.; Leboulleux, S.; Hartl, D.; Travagli, J.P.; Caillou, B.; Ricard, M.; Lumbroso, J.D.; De Vathaire, F.; et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: Benefits and limits of radioiodine therapy. J. Clin. Endocrinol. Metab. 2006, 91, 2892–2899. [Google Scholar] [CrossRef]
- Chrisoulidou, A.; Boudina, M.; Tzemailas, A.; Doumala, E.; Iliadou, P.K.; Patakiouta, F.; Pazaitou-Panayiotou, K. Histological subtype is the most important determinant of survival in metastatic papillary thyroid cancer. Thyroid Res. 2011, 4, 12. [Google Scholar] [CrossRef]
- Pontius, L.N.; Oyekunle, T.O.; Thomas, S.M.; Stang, M.T.; Scheri, R.P.; Roman, S.A.; Sosa, J.A. Projecting Survival in Papillary Thyroid Cancer: A Comparison of the Seventh and Eighth Editions of the American Joint Commission on Cancer/Union for International Cancer Control Staging Systems in Two Contemporary National Patient Cohorts. Thyroid 2017, 27, 1408–1416. [Google Scholar] [CrossRef] [PubMed]
- Verburg, F.A.; Mäder, U.; Kruitwagen, C.L.J.J.; Luster, M.; Reiners, C. A comparison of prognostic classification systems for differentiated thyroid carcinoma. Clin. Endocrinol. 2010, 72, 830–838. [Google Scholar] [CrossRef]
- Gan, T.; Huang, B.; Chen, Q.; Sinner, H.F.; Lee, C.Y.; Sloan, D.A.; Randle, R.W. Risk of Recurrence in Differentiated Thyroid Cancer: A Population-Based Comparison of the 7th and 8th Editions of the American Joint Committee on Cancer Staging Systems. Ann. Surg. Oncol. 2019, 26, 2703–2710. [Google Scholar] [CrossRef] [PubMed]
- Kebebew, E.; Weng, J.; Bauer, J.; Ranvier, G.; Clark, O.H.; Duh, Q.-Y.; Shibru, D.; Bastian, B.; Griffin, A. The Prevalence and Prognostic Value of BRAF Mutation in Thyroid Cancer. Ann. Surg. 2007, 246, 466–471. [Google Scholar] [CrossRef]
- TERT Promoter Mutations and Long-Term Survival in Patients with Thyroid Cancer in: Endocrine-Related Cancer Volume 23 Issue 10. Available online: https://erc.bioscientifica.com/view/journals/erc/23/10/813.xml (accessed on 14 August 2020).
- Punda, A.; Bedeković, V.; Barić, A.; Kontić, M.; Čolović, Z.; Vanjaka Rogošić, L.; Punda, H.; Kunac, N.; Grandić, L.; Pešutić Pisac, V. Ret Expression and its Correlation with Clinicopathologic Data in Papillary Thyroid Carcinoma. Acta Clin Croat. 2018, 57, 646–652. [Google Scholar] [CrossRef] [PubMed]
- Raman, P.; Koenig, R.J. PAX8-PPARγ fusion protein in thyroid carcinoma. Nat. Rev. Endocrinol. 2014, 10, 616–623. [Google Scholar] [CrossRef] [PubMed]
- Nikiforova, M.N.; Wald, A.I.; Roy, S.; Durso, M.B.; Nikiforov, Y.E. Targeted Next-Generation Sequencing Panel (ThyroSeq) for Detection of Mutations in Thyroid Cancer. J. Clin. Endocrinol. Metab. 2013, 98, E1852–E1860. [Google Scholar] [CrossRef]
- Nikiforova, M.N.; Chiosea, S.I.; Nikiforov, Y.E. MicroRNA expression profiles in thyroid tumors. Endocr. Pathol. 2009, 20, 85–91. [Google Scholar] [CrossRef]
- Asa, S.L.; Ezzat, S. The epigenetic landscape of differentiated thyroid cancer. Mol. Cell. Endocrinol. 2018, 469, 3–10. [Google Scholar] [CrossRef]
- Saftencu, M.; Braicu, C.; Cojocneanu, R.; Buse, M.; Irimie, A.; Piciu, D.; Berindan-Neagoe, I. Gene Expression Patterns Unveil New Insights in Papillary Thyroid Cancer. Medicina 2019, 55, 500. [Google Scholar] [CrossRef]
- Tan, W.; Liu, B.; Qu, S.; Liang, G.; Luo, W.; Gong, C. MicroRNAs and cancer: Key paradigms in molecular therapy. Oncol. Lett. 2018, 15, 2735–2742. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Pan, X.; Cobb, G.P.; Anderson, T.A. microRNAs as oncogenes and tumor suppressors. Dev. Biol. 2007, 302, 1–12. [Google Scholar] [CrossRef]
- American Thyroid Association (ATA) Guidelines Taskforce on Thyroid Nodules and Differentiated Thyroid Cancer; Cooper, D.S.; Doherty, G.M.; Haugen, B.R.; Hauger, B.R.; Kloos, R.T.; Lee, S.L.; Mandel, S.J.; Mazzaferri, E.L.; McIver, B.; et al. Revised American Thyroid Association management guidelines for patients with thyroid nodules and differentiated thyroid cancer. Thyroid 2009, 19, 1167–1214. [Google Scholar] [CrossRef]
- Xing, M.; Haugen, B.R.; Schlumberger, M. Progress in molecular-based management of differentiated thyroid cancer. Lancet 2013, 381, 1058–1069. [Google Scholar] [CrossRef]
- Nikiforova, M.N.; Tseng, G.C.; Steward, D.; Diorio, D.; Nikiforov, Y.E. MicroRNA expression profiling of thyroid tumors: Biological significance and diagnostic utility. J. Clin. Endocrinol. Metab. 2008, 93, 1600–1608. [Google Scholar] [CrossRef]
- Keutgen, X.M.; Filicori, F.; Crowley, M.J.; Wang, Y.; Scognamiglio, T.; Hoda, R.; Buitrago, D.; Cooper, D.; Zeiger, M.A.; Zarnegar, R.; et al. A panel of four miRNAs accurately differentiates malignant from benign indeterminate thyroid lesions on fine needle aspiration. Clin. Cancer Res. 2012, 18, 2032–2038. [Google Scholar] [CrossRef]
- Agretti, P.; Ferrarini, E.; Rago, T.; Candelieri, A.; De Marco, G.; Dimida, A.; Niccolai, F.; Molinaro, A.; Di Coscio, G.; Pinchera, A.; et al. MicroRNA expression profile helps to distinguish benign nodules from papillary thyroid carcinomas starting from cells of fine-needle aspiration. Eur. J. Endocrinol. 2012, 167, 393–400. [Google Scholar] [CrossRef]
- Pallante, P.; Battista, S.; Pierantoni, G.M.; Fusco, A. Deregulation of microRNA expression in thyroid neoplasias. Nat. Rev. Endocrinol. 2014, 10, 88–101. [Google Scholar] [CrossRef]
- Schwertheim, S.; Sheu, S.-Y.; Worm, K.; Grabellus, F.; Schmid, K.W. Analysis of deregulated miRNAs is helpful to distinguish poorly differentiated thyroid carcinoma from papillary thyroid carcinoma. Horm. Metab. Res. 2009, 41, 475–481. [Google Scholar] [CrossRef]
- Chou, C.-K.; Chen, R.-F.; Chou, F.-F.; Chang, H.-W.; Chen, Y.-J.; Lee, Y.-F.; Yang, K.D.; Cheng, J.-T.; Huang, C.-C.; Liu, R.-T. miR-146b is highly expressed in adult papillary thyroid carcinomas with high risk features including extrathyroidal invasion and the BRAF(V600E) mutation. Thyroid 2010, 20, 489–494. [Google Scholar] [CrossRef]
- Xing, M.; Westra, W.H.; Tufano, R.P.; Cohen, Y.; Rosenbaum, E.; Rhoden, K.J.; Carson, K.A.; Vasko, V.; Larin, A.; Tallini, G.; et al. BRAF mutation predicts a poorer clinical prognosis for papillary thyroid cancer. J. Clin. Endocrinol. Metab. 2005, 90, 6373–6379. [Google Scholar] [CrossRef] [PubMed]
- Wójcicka, A.; Kolanowska, M.; Jażdżewski, K. Mechanisms in Endocrinology: MicroRNA in diagnostics and therapy of thyroid cancer. Eur. J. Endocrinol. 2016, 174, R89–R98. [Google Scholar] [CrossRef] [PubMed]
- Acibucu, F.; Dökmetaş, H.S.; Tutar, Y.; Elagoz, S.; Kilicli, F. Correlations between the expression levels of micro-RNA146b, 221, 222 and p27Kip1 protein mRNA and the clinicopathologic parameters in papillary thyroid cancers. Exp. Clin. Endocrinol. Diabetes 2014, 122, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Witwer, K.W. Circulating microRNA biomarker studies: Pitfalls and potential solutions. Clin. Chem. 2015, 61, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Weber, F.; Teresi, R.E.; Broelsch, C.E.; Frilling, A.; Eng, C. A limited set of human MicroRNA is deregulated in follicular thyroid carcinoma. J. Clin. Endocrinol. Metab. 2006, 91, 3584–3591. [Google Scholar] [CrossRef]
- Smallridge, R.C.; Copland, J.A. Anaplastic thyroid carcinoma: Pathogenesis and emerging therapies. Clin. Oncol. (R. Coll. Radiol.) 2010, 22, 486–497. [Google Scholar] [CrossRef]
- Visone, R.; Pallante, P.; Vecchione, A.; Cirombella, R.; Ferracin, M.; Ferraro, A.; Volinia, S.; Coluzzi, S.; Leone, V.; Borbone, E.; et al. Specific microRNAs are downregulated in human thyroid anaplastic carcinomas. Oncogene 2007, 26, 7590–7595. [Google Scholar] [CrossRef]
- Takakura, S.; Mitsutake, N.; Nakashima, M.; Namba, H.; Saenko, V.A.; Rogounovitch, T.I.; Nakazawa, Y.; Hayashi, T.; Ohtsuru, A.; Yamashita, S. Oncogenic role of miR-17-92 cluster in anaplastic thyroid cancer cells. Cancer Sci. 2008, 99, 1147–1154. [Google Scholar] [CrossRef]
- de Groot, J.; Plukker, J.; Wolffenbuttel, B.; Wiggers, T.; Sluiter, W.; Links, T. Determinants of life expectancy in medullary thyroid cancer: Age does not matter. Clin. Endocrinol. 2007, 65, 729–736. [Google Scholar] [CrossRef]
- Abraham, D.; Jackson, N.; Gundara, J.S.; Zhao, J.; Gill, A.J.; Delbridge, L.; Robinson, B.G.; Sidhu, S.B. MicroRNA profiling of sporadic and hereditary medullary thyroid cancer identifies predictors of nodal metastasis, prognosis, and potential therapeutic targets. Clin. Cancer Res. 2011, 17, 4772–4781. [Google Scholar] [CrossRef]
- Aragon Han, P.; Weng, C.-H.; Khawaja, H.T.; Nagarajan, N.; Schneider, E.B.; Umbricht, C.B.; Witwer, K.W.; Zeiger, M.A. MicroRNA Expression and Association with Clinicopathologic Features in Papillary Thyroid Cancer: A Systematic Review. Thyroid 2015, 25, 1322–1329. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. PRISMA-P Group Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Vali, Y.; Zafarmand, M.; Bossuyt, P. Quality Assessment of Prognostic Accuracy Studies (QUAPAS): An extension of the Quality Assessment of Diagnostic Accuracy Studies (QUADAS-2) tool for systematic reviews of prognostic test accuracy studies. In: Abstracts of the 26th Cochrane Colloquium, Santiago, Chile. Cochrane Database Syst. Rev. 2020. [Google Scholar] [CrossRef]
- Bristol, U. of QUADAS-2 of QUADAS-2|Bristol Medical School: Population Health Sciences|University of Bristol. Available online: https://www.bristol.ac.uk/population-health-sciences/projects/quadas/quadas-2/ (accessed on 2 July 2020).
- Grooten, W.J.A.; Tseli, E.; Äng, B.O.; Boersma, K.; Stålnacke, B.-M.; Gerdle, B.; Enthoven, P. Elaborating on the assessment of the risk of bias in prognostic studies in pain rehabilitation using QUIPS—Aspects of interrater agreement. Diagn. Progn. Res. 2019, 3, 5. [Google Scholar] [CrossRef]
- Higgins, J.; Thomas, J.; Chandler, J.; Welch, V. Cochrane Handbook for Systematic Reviews of Interventions. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Cochrane, UK, 2019; p. 144. [Google Scholar]
- Borenstein, M.; Hedges, L.V.; Higgins, J.P.T.; Rothstein, H.R. Introduction to Meta-Analysis, 1st ed.; Wiley & Sons Ltd.: Hoboken, NJ, USA, 2009. [Google Scholar]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trial. 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Orsini, N.; Bottai, M.; Higgins, J.; Buchan, I. HETEROGI: Stata Module to Quantify Heterogeneity in a Meta-Analysis; Boston College Department of Economics: Chestnut Hill, MA, USA, 2006. [Google Scholar]
- Cavedon, E.; Barollo, S.; Bertazza, L.; Pennelli, G.; Galuppini, F.; Watutantrige-Fernando, S.; Censi, S.; Iacobone, M.; Benna, C.; Vianello, F.; et al. Prognostic Impact of miR-224 and RAS Mutations in Medullary Thyroid Carcinoma. Int. J. Endocrinol. 2017, 2017, 4915736. [Google Scholar] [CrossRef]
- Buda, I.; Bachar, G.; Gilham, A.; Buda, I.; Bachar, G.; Gilam, A.; Modai, S.; Strenov, Y.; Pasmanik-Chor, M.; Feinmesser, R.; et al. Differential expression of microRNAs between aggressive and non-aggressive papillary thyroid carcinoma. Head Neck Oncol. 2012, 4, 52. Available online: http://www.oapublishinglondon.com/article/226 (accessed on 16 June 2020).
- Montero-Conde, C.; Graña-Castro, O.; Martín-Serrano, G.; Martínez-Montes, Á.M.; Zarzuela, E.; Muñoz, J.; Torres-Perez, R.; Pita, G.; Cordero-Barreal, A.; Leandro-García, L.J.; et al. Hsa-miR-139-5p is a prognostic thyroid cancer marker involved in HNRNPF-mediated alternative splicing. Int. J. Cancer 2020, 146, 521–530. [Google Scholar] [CrossRef]
- Dettmer, M.S.; Perren, A.; Moch, H.; Komminoth, P.; Nikiforov, Y.E.; Nikiforova, M.N. MicroRNA profile of poorly differentiated thyroid carcinomas: New diagnostic and prognostic insights. J. Mol. Endocrinol. 2014, 52, 181–189. [Google Scholar] [CrossRef]
- Chen, Y.; Hao, S.-A.; Jiang, Y.; Gao, B.; Tian, W.-G.; Zhang, S.; Guo, L.-J.; Wang, L.-L.; Luo, D.-L. MicroRNA-1271 inhibits the progression of papillary thyroid carcinoma by targeting IRS1 and inactivating AKT pathway. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 7989–7999. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-K.; Yang, K.D.; Chou, F.-F.; Huang, C.-C.; Lan, Y.-W.; Lee, Y.-F.; Kang, H.-Y.; Liu, R.-T. Prognostic implications of miR-146b expression and its functional role in papillary thyroid carcinoma. J. Clin. Endocrinol. Metab. 2013, 98, E196–E205. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.-B.; Chen, C.-L.; Tian, Z.-L.; Yuan, F.-K.; Jia, G.-L. MicroRNA-791 is an independent prognostic factor of papillary thyroid carcinoma and inhibits the proliferation of PTC cells. Eur. Rev. Med. Pharm. Sci. 2018, 22, 5562–5568. [Google Scholar] [CrossRef]
- Galuppini, F.; Bertazza, L.; Barollo, S.; Cavedon, E.; Rugge, M.; Guzzardo, V.; Sacchi, D.; Watutantrige-Fernando, S.; Vianello, F.; Mian, C.; et al. MiR-375 and YAP1 expression profiling in medullary thyroid carcinoma and their correlation with clinical-pathological features and outcome. Virchows Arch. 2017, 471, 651–658. [Google Scholar] [CrossRef]
- Dai, L.; Wang, Y.; Chen, L.; Zheng, J.; Li, J.; Wu, X. MiR-221, a potential prognostic biomarker for recurrence in papillary thyroid cancer. World J. Surg. Oncol. 2017, 15, 11. [Google Scholar] [CrossRef]
- Huang, T.; Yi, D.; Xu, L.; Bu, E.; Zhu, C.; Sang, J.; Zhang, Y. Downregulation of miR-381 is associated with poor prognosis in papillary thyroid carcinoma. Int. J. Clin. Exp. Pathol. 2017, 10, 11610–11616. [Google Scholar]
- Jikuzono, T.; Kawamoto, M.; Yoshitake, H.; Kikuchi, K.; Akasu, H.; Ishikawa, H.; Hirokawa, M.; Miyauchi, A.; Tsuchiya, S.; Shimizu, K.; et al. The miR-221/222 cluster, miR-10b and miR-92a are highly upregulated in metastatic minimally invasive follicular thyroid carcinoma. Int. J. Oncol. 2013, 42, 1858–1868. [Google Scholar] [CrossRef]
- Lee, J.C.; Zhao, J.T.; Clifton-Bligh, R.J.; Gill, A.; Gundara, J.S.; Ip, J.C.; Glover, A.; Sywak, M.S.; Delbridge, L.W.; Robinson, B.G.; et al. MicroRNA-222 and microRNA-146b are tissue and circulating biomarkers of recurrent papillary thyroid cancer. Cancer 2013, 119, 4358–4365. [Google Scholar] [CrossRef]
- Liu, N.; Zhou, Q.; Qi, Y.-H.; Wang, H.; Yang, L.; Fan, Q.-Y. Effects of long non-coding RNA H19 and microRNA let7a expression on thyroid cancer prognosis. Exp. Mol. Pathol. 2017, 103, 71–77. [Google Scholar] [CrossRef]
- Liu, C.; Xing, M.; Wang, L.; Zhang, K. miR-199a-3p downregulation in thyroid tissues is associated with invasion and metastasis of papillary thyroid carcinoma. Br. J. Biomed. Sci. 2017, 74, 90–94. [Google Scholar] [CrossRef]
- Mian, C.; Pennelli, G.; Fassan, M.; Balistreri, M.; Barollo, S.; Cavedon, E.; Galuppini, F.; Pizzi, M.; Vianello, F.; Pelizzo, M.R.; et al. MicroRNA profiles in familial and sporadic medullary thyroid carcinoma: Preliminary relationships with RET status and outcome. Thyroid 2012, 22, 890–896. [Google Scholar] [CrossRef]
- Pennelli, G.; Galuppini, F.; Barollo, S.; Cavedon, E.; Bertazza, L.; Fassan, M.; Guzzardo, V.; Pelizzo, M.R.; Rugge, M.; Mian, C. The PDCD4/miR-21 pathway in medullary thyroid carcinoma. Hum. Pathol. 2015, 46, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Qiu, Z.; Li, H.; Wang, J.; Sun, C. miR-146a and miR-146b in the diagnosis and prognosis of papillary thyroid carcinoma. Oncol. Rep. 2017, 38, 2735–2740. [Google Scholar] [CrossRef] [PubMed]
- Sun, Y.-H.; Liu, Z.-F.; Yang, B.-B.; Yu, B. MicroRNA-486 inhibits cell proliferation, invasion and migration via down-regulating the TENM1 expressions and affecting ERK and Akt signaling pathways and epithelial-to-mesenchymal transition in papillary thyroid carcinoma. Eur. Rev. Med. Pharm. Sci 2019, 23, 8429–8439. [Google Scholar] [CrossRef]
- Wu, Y.-C.; Li, S.-Y.; Jia, Y.-F. MicroRNA-26a suppresses the malignant biological behaviors of papillary thyroid carcinoma by targeting ROCK1 and regulating PI3K/AKT signaling pathway. Eur. Rev. Med. Pharm. Sci. 2019, 23, 8940–8949. [Google Scholar] [CrossRef]
- Yao, X.-G.; Tan, Q.; Liu, P.-P.; Feng, L.-J. Tissue microRNA-182 expression level and its potential prognostic value for papillary thyroid carcinoma. Int. J. Clin Exp. Pathol. 2019, 12, 3128–3133. [Google Scholar]
- Zhang, Y.; Xu, D.; Pan, J.; Yang, Z.; Chen, M.; Han, J.; Zhang, S.; Sun, L.; Qiao, H. Dynamic monitoring of circulating microRNAs as a predictive biomarker for the diagnosis and recurrence of papillary thyroid carcinoma. Oncol. Lett. 2017, 13, 4252–4266. [Google Scholar] [CrossRef]
- Zheng, J.; Li, J. Serum miRNA-203 expression, a potential biomarker for recurrence and prognosis in papillary thyroid carcinoma. Int. J. Clin. Exp. Med. 2016, 9, 14980–14986. [Google Scholar] [CrossRef]
- Ren, G.; Li, H.; He, X.; Zhang, J. Downregulation of serum miR-26a predicts poor clinical outcome of papillary thyroid carcinoma. Int. J. Clin Exp. Pathol. 2017, 10, 9042–9047. [Google Scholar]
- Yip, L.; Kelly, L.; Shuai, Y.; Armstrong, M.J.; Nikiforov, Y.E.; Carty, S.E.; Nikiforova, M.N. MicroRNA signature distinguishes the degree of aggressiveness of papillary thyroid carcinoma. Ann. Surg. Oncol. 2011, 18, 2035–2041. [Google Scholar] [CrossRef]
- Sondermann, A.; Andreghetto, F.M.; Moulatlet, A.C.B.; da Silva Victor, E.; de Castro, M.G.; Nunes, F.D.; Brandão, L.G.; Severino, P. MiR-9 and miR-21 as prognostic biomarkers for recurrence in papillary thyroid cancer. Clin. Exp. Metastasis 2015, 32, 521–530. [Google Scholar] [CrossRef] [PubMed]
- Romeo, P.; Colombo, C.; Granata, R.; Calareso, G.; Gualeni, A.V.; Dugo, M.; De Cecco, L.; Rizzetti, M.G.; Zanframundo, A.; Aiello, A.; et al. Circulating miR-375 as a novel prognostic marker for metastatic medullary thyroid cancer patients. Endocr. Relat. Cancer 2018, 25, 217–231. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Pérez, A.M.; Cornejo Pareja, I.M.; García Alemán, J.; Coín Aragüez, L.; Sebastián Ochoa, A.; Alcaide Torres, J.; Molina Vega, M.; Clu Fernández, C.; Mancha Doblas, I.; Tinahones, F.J. New molecular biomarkers in differentiated thyroid carcinoma: Impact of miR-146, miR-221 and miR-222 levels in the evolution of the disease. Clin. Endocrinol. 2019, 91, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Chengfeng, X.; Gengming, C.; Junjia, Z.; Yunxia, L. MicroRNA signature predicts survival in papillary thyroid carcinoma. J. Cell. Biochem. 2019, 120, 17050–17058. [Google Scholar] [CrossRef]
- Lee, J.C.; Zhao, J.; Clifton-Bligh, R.J.; Robinson, B.G.; Sidhu, S.B. Plasma MiRNA Profile as Circulating Biomarkers of Papillary Thyroid Carcinoma. J. Surg. Res. 2013, 179, 248. [Google Scholar] [CrossRef]
- Bonichon, F.; Cao, C.; Guyetant, S.; Schvartz, C.; Soubeyran, I.; Rohmer, V.; Toubeau, M.; Savagner, F. Hurhtle Cell Thyroid Carcinoma: A Multicentric Retrospective Study with Mirna Profiling: P40. Eur. Thyr. J. 2013, 2, 40. [Google Scholar]
- Castelblanco, E.; Rosado, V.; Martinez, M.; Santos, M.D.; Mancikova, V.; Robledo, M.; Matias-Guiu, X.; Maravall, J.; Mauricio, D. Differential miRNAs expression in papillary thyroid cancer is associated with clinico-pathological features and BRAF mutation. BioScientifica 2014, 35, 1095. [Google Scholar] [CrossRef]
- Guo, Z.; Hardin, H.; Montemayor-Garcia, C.; Asioli, S.; Righi, A.; Maletta, F.; Sapino, A.; Lloyd, R.V. In Situ Hybridization Analysis of miR-146b-5p and miR-21 in Thyroid Nodules: Diagnostic Implications. Endocr. Pathol. 2015, 26, 157–163. [Google Scholar] [CrossRef]
- Nikiforova, M.N.; Dipaola, J.; Aspden, L.; Nikiforov, Y.E. miRNA Markers of Aggressive Behavior of Papillary Thyroid Carcinoma. Labor. Invest. 2009, 89, 115–222. [Google Scholar]
- Rosignolo, F.; Memeo, L.; Monzani, F.; Colarossi, C.; Pecce, V.; Verrienti, A.; Durante, C.; Grani, G.; Lamartina, L.; Forte, S.; et al. MicroRNA-based molecular classification of papillary thyroid carcinoma. Int. J. Oncol. 2017, 50, 1767–1777. [Google Scholar] [CrossRef]
- Rosignolo, F.; Sponziello, M.; Giacomelli, L.; Russo, D.; Pecce, V.; Biffoni, M.; Bellantone, R.; Lombardi, C.P.; Lamartina, L.; Grani, G.; et al. Identification of Thyroid-Associated Serum microRNA Profiles and Their Potential Use in Thyroid Cancer Follow-Up. J. Endocr. Soc. 2017, 1, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Zhang, H.; Zhang, P.; Li, J.; Shan, Z.; Teng, W. Upregulation of miR-2861 and miR-451 expression in papillary thyroid carcinoma with lymph node metastasis. Med. Oncol. 2013, 30, 577. [Google Scholar] [CrossRef]
- Wei, W.-J.; Lu, Z.-W.; Li, D.-S.; Wang, Y.; Zhu, Y.-X.; Wang, Z.-Y.; Wu, Y.; Wang, Y.-L.; Ji, Q.-H. Association of the miR-149 Rs2292832 polymorphism with papillary thyroid cancer risk and clinicopathologic characteristics in a Chinese population. Int. J. Mol. Sci. 2014, 15, 20968–20981. [Google Scholar] [CrossRef] [PubMed]
- Kotlarek, M.; Kubiak, A.; Czetwertyńska, M.; Świerniak, M.; Gierlikowski, W.; Kolanowska, M.; Bakuła-Zalewska, E.; Jhiang, S.M.; Jażdżewski, K.; Wójcicka, A. The rs2910164 Genetic Variant of miR-146a-3p Is Associated with Increased Overall Mortality in Patients with Follicular Variant Papillary Thyroid Carcinoma. Int. J. Mol. Sci. 2018, 19, 655. [Google Scholar] [CrossRef]
- Sun, M.; Fang, S.; Li, W.; Li, C.; Wang, L.; Wang, F.; Wang, Y. Associations of miR-146a and miR-146b Expression and Clinical Characteristics in Papillary Thyroid Carcinoma. Available online: https://pubmed.ncbi.nlm.nih.gov/25524940/ (accessed on 12 July 2020).
- Wang, Z.; Zhang, H.; He, L.; Dong, W.; Li, J.; Shan, Z.; Teng, W. Association between the expression of four upregulated miRNAs and extrathyroidal invasion in papillary thyroid carcinoma. Onco Targets 2013, 6, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Yuan, Z.; Fan, Y.; Deng, X.; Zheng, Q. Integrated analyses of microRNA and mRNA expression profiles in aggressive papillary thyroid carcinoma. Mol. Med. Rep. 2013, 8, 1353–1358. [Google Scholar] [CrossRef]
- MicroRNA Targeted Cancer Therapy; Sarkar, F.H., Ed.; Springer International Publishing: New York, NY, USA, 2014; ISBN 978-3-319-05133-8. [Google Scholar]
- Aubert, S.; Berdelou, A.; Gnemmi, V.; Behal, H.; Caiazzo, R.; D’herbomez, M.; Pigny, P.; Wemeau, J.L.; Carnaille, B.; Renaud, F.; et al. Large sporadic thyroid medullary carcinomas: Predictive factors for lymph node involvement. Virchows Arch. 2018, 472, 461–468. [Google Scholar] [CrossRef]
- Wojtas, B.; Ferraz, C.; Stokowy, T.; Hauptmann, S.; Lange, D.; Dralle, H.; Musholt, T.; Jarzab, B.; Paschke, R.; Eszlinger, M. Differential miRNA expression defines migration and reduced apoptosis in follicular thyroid carcinomas. Mol. Cell. Endocrinol. 2014, 388, 1–9. [Google Scholar] [CrossRef]
- Li, J.; Fu, H.; Xu, C.; Tie, Y.; Xing, R.; Zhu, J.; Qin, Y.; Sun, Z.; Zheng, X. miR-183 inhibits TGF-β1-induced apoptosis by downregulation of PDCD4 expression in human hepatocellular carcinoma cells. BMC Cancer 2010, 10, 354. [Google Scholar] [CrossRef]
- Lin, W.M.; Baker, A.C.; Beroukhim, R.; Winckler, W.; Feng, W.; Marmion, J.M.; Laine, E.; Greulich, H.; Tseng, H.; Gates, C.; et al. Modeling genomic diversity and tumor dependency in malignant melanoma. Cancer Res. 2008, 68, 664–673. [Google Scholar] [CrossRef]
- Motoyama, K.; Inoue, H.; Takatsuno, Y.; Tanaka, F.; Mimori, K.; Uetake, H.; Sugihara, K.; Mori, M. Over- and under-expressed microRNAs in human colorectal cancer. Int. J. Oncol. 2009, 34, 1069–1075. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wang, G.; Mao, W.; Zheng, S. MicroRNA-183 regulates Ezrin expression in lung cancer cells. FEBS Lett. 2008, 582, 3663–3668. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Zhao, S.; Luo, Y.; Zhang, A.; Wei, L.; Xie, Z.; Li, Y.; Ma, W. MiR-375: A prospective regulator in medullary thyroid cancer based on microarray data and bioinformatics analyses. Pathol. Res. Prac. 2017, 213, 1344–1354. [Google Scholar] [CrossRef]
- Lassalle, S.; Zangari, J.; Popa, A.; Ilie, M.; Hofman, V.; Long, E.; Patey, M.; Tissier, F.; Belléannée, G.; Trouette, H.; et al. MicroRNA-375/SEC23A as biomarkers of the in vitro efficacy of vandetanib. Oncotarget 2016, 7, 30461–30478. [Google Scholar] [CrossRef] [PubMed]
- Ringel, M.D.; Nabhan, F. Approach to Follow-Up of the Patient with Differentiated Thyroid Cancer and Positive Anti-Thyroglobulin Antibodies. J. Clin. Endocrinol. Metab. 2013, 98, 3104–3110. [Google Scholar] [CrossRef]
- Wells, S.A.; Asa, S.L.; Dralle, H.; Elisei, R.; Evans, D.B.; Gagel, R.F.; Lee, N.; Machens, A.; Moley, J.F.; Pacini, F.; et al. Revised American Thyroid Association Guidelines for the Management of Medullary Thyroid Carcinoma. Thyroid 2015, 25, 567–610. [Google Scholar] [CrossRef]
- Papp, S.; Asa, S.L. When Thyroid Carcinoma Goes Bad: A Morphological and Molecular Analysis. Head Neck Pathol. 2015, 9, 16–23. [Google Scholar] [CrossRef]
- Riesco-Eizaguirre, G.; Wert-Lamas, L.; Perales-Patón, J.; Sastre-Perona, A.; Fernández, L.P.; Santisteban, P. The miR-146b-3p/PAX8/NIS Regulatory Circuit Modulates the Differentiation Phenotype and Function of Thyroid Cells during Carcinogenesis. Cancer Res. 2015, 75, 4119–4130. [Google Scholar] [CrossRef]
- Jaber, T.; Waguespack, S.G.; Cabanillas, M.E.; Elbanan, M.; Vu, T.; Dadu, R.; Sherman, S.I.; Amit, M.; Santos, E.B.; Zafereo, M.; et al. Targeted Therapy in Advanced Thyroid Cancer to Resensitize Tumors to Radioactive Iodine. J. Clin. Endocrinol. Metab. 2018, 103, 3698–3705. [Google Scholar] [CrossRef]
- McShane, L.M.; Altman, D.G.; Sauerbrei, W.; Taube, S.E.; Gion, M.; Clark, G.M. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK). J. Natl. Cancer. Inst. 2005, 97, 1180–1184. [Google Scholar] [CrossRef]











| First Author, Year, Reference | Country | TC Subtype | Sample | Follow-Up, Months | Age | Female (%) | Number | Assay | Control | Cut-Off | miRNA, Expression | Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Abraham, 2011 [42] | Australia | MTC | thyroid | 82.8 | 51.8 | 46 | 44 | qRT-PCR | RNU48 | None | 185↑, 375↑ | D/R-Recurrence |
| Residual disease | ||||||||||||
| Buda, 2012 [54] | Israel | PTC | thyroid | 60 | 51.8 | 100 | 8 | qRT-PCR | RNU6 | None | 155↑, 15a↑, 19b↑, 200a↑, 21↑, 483-5p↓ | Recurrence |
| Cavedon, 2017 [53] | Italy | MTC | thyroid | 40 | 58.5 | 59 | 121 | qRT-PCR | RNU6B | None | 224↓ | Persistence |
| 133 | Progression | |||||||||||
| Chen, 2019 [57] | China | PTC | thyroid | 60 | N/A | 63 | 44 | qRT-PCR | RNU6 | N/A | 1271↓ | OS |
| Chou, 2013 [58] | Taiwan | PTC | thyroid | 127 | 43.7 | 70 | 71 | qRT-PCR | RNU6 | Median | 146b↑ | DFS |
| Dai, 2017 [61] | China | PTC | thyroid | 68 | 45.8 | 76 | 78 | qRT-PCR | RNU48 | Median | 146b↑, 21↓, 220↑, 221↑, 222↑, 9↓ | RFS |
| Dettmer, 2014 [56] | Switzerland | PD+oPD | thyroid | <202 | 65.4/71.5 | 62 | 27 | Microarray | RNU44RNU6 | 0.2-fold | 150↑ | TSS |
| <82.7 | 0.5-fold | 23b↑ | DFS | |||||||||
| Galuppini, 2017 [60] | Italy | MTC | thyroid | 39 | 58 | 60 | 130 | qRT-PCR | RNU6B | None | 375↑ | Progression |
| Gao, 2018 [59] | China | PTC | thyroid | 80 | N/A | N/A | 160 | qRT-PCR | RNU6 | N/A | 791↓ | OS |
| Huang, 2017 [62] | China | PTC | serum | 60 | N/A | 79 | 87 | qRT-PCR | N/A | Median | 381↓ | OS |
| Jikuzono, 2013 [63] | Japan | MI-FTC | thyroid | 120 | 47.2 | 67 | 34 | qRT-PCR | RNU44 | None | 10b↑, 221↑, 221*↑, 222↑, 222*↑, 375↑, 92a↑ | D-Recurrence |
| Lee, 2013 [64] | Australia | PTC | thyroid | 40.6 | 57/44 | 69 | 26 | qRT-PCR | RNU48 | None | 1299↑, 146b↑, 155↑, 193b↑, 221↑, 222↑ | Recurrence |
| Liu, 2017 [65] | China | TC | thyroid | 60 | 45.3 | 67 | 131 | qRT-PCR | GAPDH | ROC (0.87-fold) | let 7a↓ | OS |
| Liu, Ch., 2017 [66] | China | PTC | thyroid | N/A | N/A | 78 | 136 | qRT-PCR | RNU6 | None | 199a-3p↓ | R-Recurrence |
| Mian, 2012 [67] | Italy | MTC | thyroid | 48 | 60 | 40 | 40 | qRT-PCR | RNU6 | None | 224↓ | Persistence |
| Montero, 2019 [55] | Spain | DTC | thyroid | 96 | 51.1 | N/A | 24 | MiRNome profiling | N/A | median | 139-5p↓ | DFS |
| 36 | 60 | None | Residual disease | |||||||||
| Pennelli, 2015 [68] | Italy | MTC | thyroid | 48 | 59.1 | 56 | 57 | qRT-PCR | RNU6B | None | 21↑ | Persistence |
| Qiu, 2017 [69] | China | PTC | thyroid | 12 | 38-67 | 53 | 73 | qRT-PCR | Beta-actin | N/A | 146a↑146b↑ | OS |
| None | Recurrence | |||||||||||
| Ren, 2017 [75] | China | PTC | serum | 60 | N/A | 61 | 84 | qRT-PCR | RNU6 | Mean | 26a↓ | DFS |
| OS | ||||||||||||
| Romeo, 2018 [78] | Italy | mMTC | plasma | 36 | 50/48 | 41 | 31 | qRT-PCR | RNU6B | Median | 375↑ | OS |
| 65 | 45 | None | Residual disease | |||||||||
| Sondermann, 2015 [77] | Brazil | PTC | thyroid | 120 | 46.9/46.5 | 83 | 66 | qRT-PCR | RNU48 | median | 10b↓, 146b↑, 21↓, 9↓ | LNM-RFS |
| Sun, 2019 [70] | China | PTC | thyroid | < 60 | N/A | 51 | 56 | qRT-PCR | RNU6 | Mean | 486↓ | OS |
| Wu, 2019 [71] | China | PTC | thyroid | < 60 | N/A | 52 | 51 | qRT-PCR | RNU6 | Mean | 26a↓ | OS |
| Yao, 2019 [72] | China | PTC | thyroid | 60 | N/A | 55 | 151 | qRT-PCR | RNU6 | Median | 182↑ | OS |
| Yip, 2011 [76] | USA | PTC | thyroid | 73.2 | 42/44 | 76 | 32 | qRT-PCR | RNU44 | None | 1↓, 130-b↓, 138↓, 146b↑, 155↑, 221↑, 222↑, 31↓, 34b↓ | Recurrence |
| Zhang, 2017 [73] | China | PTC | serum | 52 | 49.7/47.7 | 61 | 21 | qRT-PCR | miR-16 | None | 146b↑, 221↑, 222↑ | Recurrence |
| Zheng, 2017 [74] | China | PTC | serum | 60 | 45.8/48.7 | 68 | 165 | qRT-PCR | GAPDH | ROC (3.56-fold) | 203↑ | OS, RFS |
| Upregulated miRNAs | |||||
|---|---|---|---|---|---|
| miRNA | Outcome | Analysis | HR/OR and 95% CI | Source | Study |
| 10b | D-Recurrence | OR | 19.8 (4.6–85.2) | Estimated | Jikuzono, 2013 [63] |
| 15a | Recurrence | N/A | N/A | N/A | Buda, 2012 [54] |
| 19b | Recurrence | N/A | N/A | N/A | Buda, 2012 [54] |
| 23b | DFS | HR | 2.6 (1.0–6.7) | Provided | Dettmer, 2014 [56] |
| 92a | D-Recurrence | OR | 7.4(1.9–29.2) | Estimated | Jikuzono, 2013 [63] |
| 146a | OS. | N/A | N/A | N/A | Qiu, 2017 [69] |
| Recurrence | OR | 92.5 (27.0–315.8) | Estimated | Qiu, 2017 [69] | |
| 146b | DFS | HR | 3.9 (1.7–8.8) | Provided | Chou, 2013 [58] |
| LNM-RFS | HR | 0.9 (0.7–1.1) | Provided | Sondermann, 2015 [77] | |
| OS. | N/A | N/A | N/A | Qiu, 2017 [69] | |
| Recurrence | OR | 4.0 (0.8–18.1) | Estimated | Lee, 2013 [64] | |
| Recurrence | OR | 36.5 (11.6–114.8) | Estimated | Qiu, 2017 [69] | |
| Recurrence | OR | 7.9 (2.0–30.7) | Estimated | Yip, 2011 [76] | |
| Recurrence | OR | 4.1 (0.8–20.9) | Estimated | Zhang, 2017 [73] | |
| RFS | HR | 1.1 (0.2–4.6) | Provided | Dai, 2017 [61] | |
| 150 | TSS | HR | 5.0 (1.2–19.6) | Provided | Dettmer, 2014 [56] |
| 155 | Recurrence | N/A | N/A | N/A | Buda, 2012 [54] |
| Recurrence | OR | 1.5 (0.3–6.7) | Estimated | Lee, 2013 [64] | |
| Recurrence | OR | 1.5 (0.4–5.3) | Estimated | Yip, 2011 [54] | |
| 182 | OS | HR | 2.8 (0.9–8.3) | Provided | Yao, 2019 [72] |
| 183 | D-Recurrence | OR | 7.3 (1.9-26.9) | Estimated | Abraham, 2011 [42] |
| R-Recurrence | OR | 7.5 (2.2–24.7) | Estimated | Abraham, 2011 [42] | |
| residual disease | OR | 7.0 (2.2–22.4) | Estimated | Abraham, 2011 [42] | |
| 193b | Recurrence | OR | 1.2 (0.2–5.4) | Estimated | Lee, 2013 [64] |
| 200a | Recurrence | N/A | N/A | N/A | Buda, 2012 [54] |
| 203 | OS | HR | 6.7 (2.0–22.1) | Provided | Zheng, 2017 [74] |
| RFS | HR | 1.38 (1.0–1.7) | Provided | Zheng, 2017 [74] | |
| 220 | RFS | HR | 1.1 (0.3–3.4) | Provided | Dai, 2017 [61] |
| 221 | D-Recurrence | OR | 7.9 2.0–31.0 | Estimated | Jikuzono, 2013 [63] |
| RFS | HR | 1.4 (1.1–1.8) | Provided | Dai, 2017 [61] | |
| Recurrence | OR | 2.2 (0.5–9.7) | Estimated | Lee, 2013 [64] | |
| Recurrence | OR | 2.6 (0.7–9.4) | Estimated | Yip, 2011 [76] | |
| Recurrence | OR | 14.4 (2.4–84.2) | Estimated | Zhang, 2017 [73] | |
| 221* | D-Recurrence | OR | 8.0 (2.0–31.8) | Estimated | Jikuzono, 2013 [63] |
| 222 | D-Recurrence | OR | 8.9 (2.2-35.4) | Estimated | Jikuzono, 2013 [63] |
| Recurrence | OR | 5.7 (1.2–26.8) | Estimated | Lee, 2013 [64] | |
| Recurrence | OR | 5.0 (1.3–18.7) | Estimated | Yip, 2011 [76] | |
| Recurrence | OR | 12.4 (2.1–70.8) | Estimated | Zhang, 2017 [73] | |
| RFS | HR | 2.8 (1.1–7.1) | Provided | Dai, 2017 [61] | |
| 222* | D-Recurrence | OR | 13.0 (3.1–53.8) | Estimated | Jikuzono, 2013 [63] |
| 375 | D-Recurrence | OR | 9.3 (2.4–35.0) | Estimated | Abraham, 2011 [42] |
| R-Recurrence | OR | 7.5 (2.2–24.7) | Estimated | Abraham, 2011 [42] | |
| residual disease | OR | 5.6 (1.8–17.8) | Estimated | Abraham, 2011 [42] | |
| Progression | OR | 3.4 (1.2–9.9) | Estimated | Galuppini, 2017 [60] | |
| D-Recurrence | OR | 2.4 (0.6–9.0) | Estimated | Jikuzono, 2013 [63] | |
| OS | HR | 10.6 (3.8–29.5) | Provided | Romeo, 2018 [78] | |
| residual disease | OR | 13.4 (3.2–55.9) | Estimated | Romeo, 2018 [78] | |
| 1299 | Recurrence | OR | 1.7 (0.4–7.6) | Estimated | Lee, 2013 [64] |
| Downregulated miRNAs | |||||
|---|---|---|---|---|---|
| miRNA | Outcome | Analysis | HR/OR and 95% CI | Source | Study |
| 1 | Recurrence | OR | 2.5 (0.7–9.1) | Estimated | Yip, 2011 [76] |
| 9 | RFS | HR | 1.3 (0.4–3.8) | Provided | Dai, 2017 [61] |
| LNM-RFS | HR | 1.4 (1.2–1.7) | Estimated | Sondermann, 2015 [77] | |
| 10b | LNM-RFS | HR | 1.2 (0.8–1.8) | Provided | Sondermann, 2015 [77] |
| 26a | DFS | HR | 2.8 (1.5–5.1) | Provided | Ren, 2017 [75] |
| OS | HR | 2.5 (1.3–4.8) | Provided | Ren, 2017 [75] | |
| OS. | N/A | N/A | N/A | Wu, 2019 [71] | |
| 31 | Recurrence | OR | 1.8 (0.5–6.7) | Estimated | Yip, 2019 [76] |
| 34b | Recurrence | OR | 5.0 (1.3–18.9) | Estimated | Zhang, 2017 [73] |
| 130-b | Recurrence | OR | 4.8 (1.3–18.1) | Estimated | Yip, 2011 [76] |
| 138 | Recurrence | OR | 2.3 (0.6–8.5) | Estimated | Yip, 2011 [76] |
| 139-5p | DFS | HR | 0.2 (0.1–0.4) | Estimated | Montero, 2019 [55] |
| Residual disease | OR | 7.0 (2.6–18.9) | Estimated | Montero, 2019 [55] | |
| 199a-3p | R-Recurrence | OR | 3.3 (1.1–9.8) | Estimated | Liu, Ch., 2017 [66] |
| 224 | Persistence | OR | 3.4 (1.6–7.0) | Estimated | Cavedon, 2017 [53] |
| Persistence | OR | 4.7 (1.4–15.3) | Estimated | Mian, 2012 [67] | |
| Progression | OR | 0.7 (0.5–0.9) | Provided | Cavedon, 2017 [53] | |
| 381 | OS | HR | 4.7 (2.6–8.5) | Provided | Huang, 2017 [62] |
| 483-5p | Recurrence | N/A | N/A | N/A | Buda, 2012 [54] |
| 486 | OS | N/A | N/A | N/A | Sun, 2019 [70] |
| 791 | OS | HR | 0.5 (0.3–0.9) | Provided | Gao, 2018 [59] |
| 1271 | OS | N/A | N/A | N/A | Chen, 2019 [57] |
| let 7a | OS | HR | 0.4 (0.2–0.9) | Provided | Liu, 2017 [65] |
| MiRNAs with Inconsistent Expression Direction | ||||||
|---|---|---|---|---|---|---|
| miRNA | ↑/↓ | Outcome | Analysis | HR/OR and 95% CI | Source | Study |
| 21 | ↑ | Recurrence | N/A | N/A | N/A | Buda, 2012 [54] |
| ↑ | Persistence | OR | 2.4 (0.9–6.5) | Estimated | Pennelli, 2015 [68] | |
| ↓ | RFS | HR | 2.0 (0.4–8.1) | Provided | Dai, 2017 [61] | |
| ↓ | LNM-RFS | HR | 1.5 (1.1–1.9) | Provided | Sondermann, 2015 [77] | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silaghi, C.A.; Lozovanu, V.; Silaghi, H.; Georgescu, R.D.; Pop, C.; Dobrean, A.; Georgescu, C.E. The Prognostic Value of MicroRNAs in Thyroid Cancers—A Systematic Review and Meta-Analysis. Cancers 2020, 12, 2608. https://doi.org/10.3390/cancers12092608
Silaghi CA, Lozovanu V, Silaghi H, Georgescu RD, Pop C, Dobrean A, Georgescu CE. The Prognostic Value of MicroRNAs in Thyroid Cancers—A Systematic Review and Meta-Analysis. Cancers. 2020; 12(9):2608. https://doi.org/10.3390/cancers12092608
Chicago/Turabian StyleSilaghi, Cristina Alina, Vera Lozovanu, Horatiu Silaghi, Raluca Diana Georgescu, Cristina Pop, Anca Dobrean, and Carmen Emanuela Georgescu. 2020. "The Prognostic Value of MicroRNAs in Thyroid Cancers—A Systematic Review and Meta-Analysis" Cancers 12, no. 9: 2608. https://doi.org/10.3390/cancers12092608
APA StyleSilaghi, C. A., Lozovanu, V., Silaghi, H., Georgescu, R. D., Pop, C., Dobrean, A., & Georgescu, C. E. (2020). The Prognostic Value of MicroRNAs in Thyroid Cancers—A Systematic Review and Meta-Analysis. Cancers, 12(9), 2608. https://doi.org/10.3390/cancers12092608