Correlation of RECIST, Computed Tomography Morphological Response, and Pathological Regression in Hepatic Metastasis Secondary to Colorectal Cancer: The AVAMET Study

 , , , ,
, , , ,
Abstract
1. Introduction
2. Patients and Methods
2.1. Outcomes
2.2. KRAS Mutation Status Correlation
2.3. Statistical Analysis
3. Results
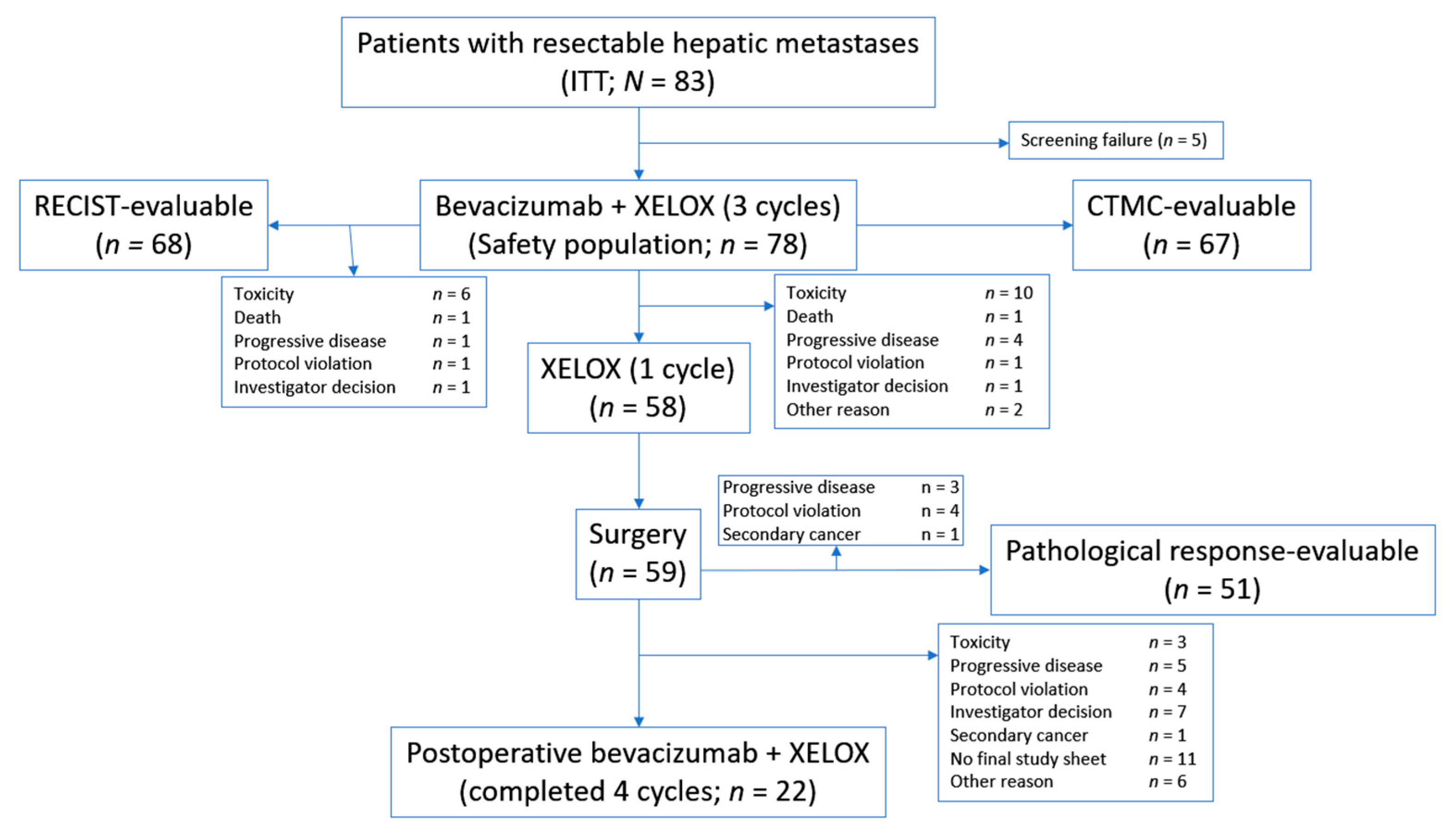
3.1. Patients
3.2. Response to Treatment
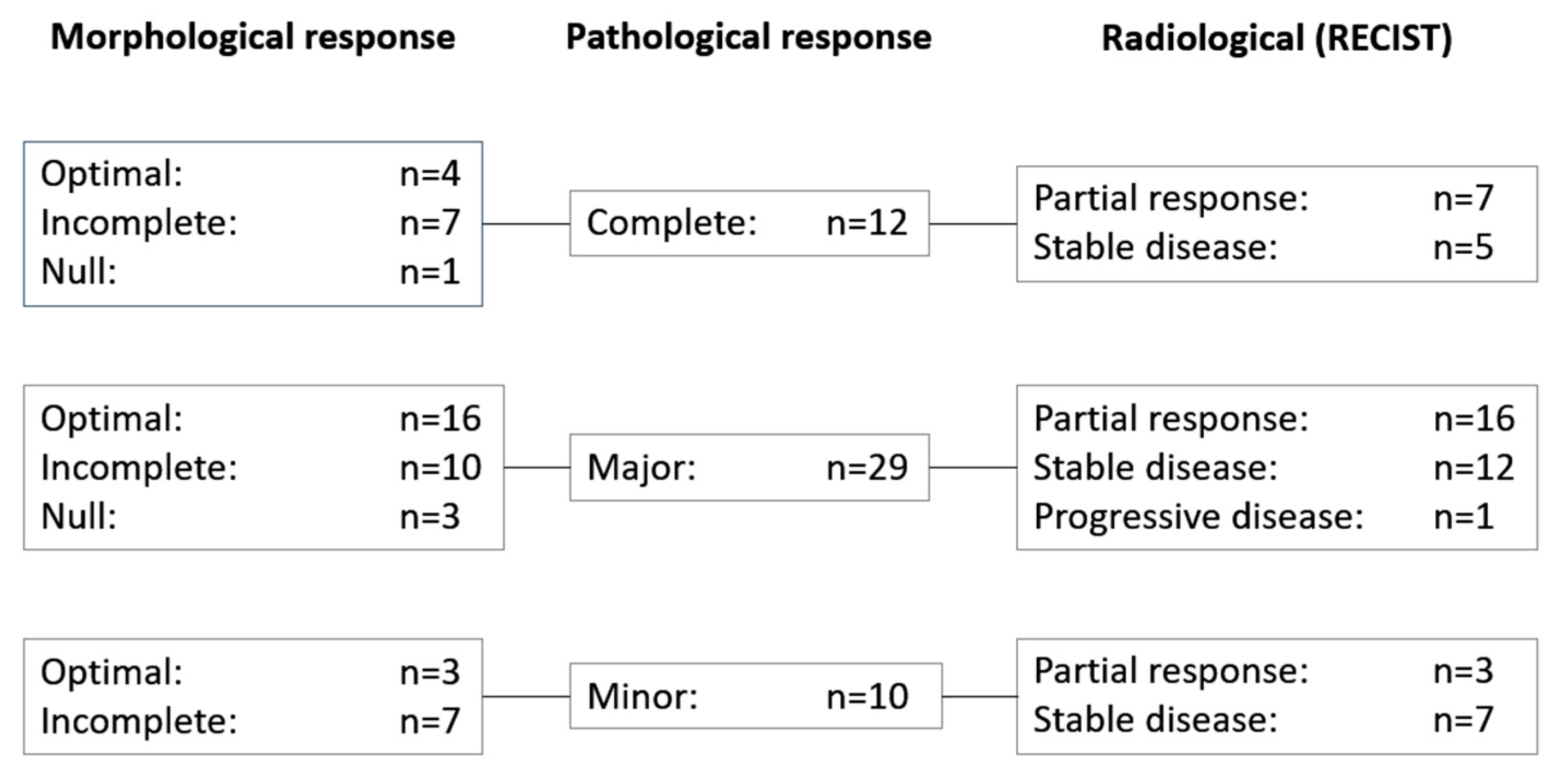
3.3. Correlation of RECIST and Morphological and Pathological Response Data
3.4. Survival
3.5. KRAS Mutation Status Analysis
3.6. Safety
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kemeny, N.; Fata, F. Arterial, portal, or systemic chemotherapy for patients with hepatic metastasis of colorectal carcinoma. J. Hepato. Pancreat. Surg. 1999, 6, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Fong, Y.; Fortner, J.; Sun, R.L.; Brennan, M.F.; Blumgart, L.H. Clinical Score for Predicting Recurrence After Hepatic Resection for Metastatic Colorectal Cancer. Ann. Surg. 1999, 230, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Nordlinger, B.; Adam, R.; Köhne, C.-H.; Pozzo, C.; Poston, G.; Ychou, M.; Rougier, P. Towards a pan-European consensus on the treatment of patients with colorectal liver metastases. Eur. J. Cancer 2006, 42, 2212–2221. [Google Scholar] [CrossRef] [PubMed]
- Adam, R.; Avisar, E.; Ariche, A.; Giachetti, S.; Azoulay, D.; Castaing, D.; Kunstlinger, F.; Levi, F.; Bismuth, F. Five-year survival following hepatic resection after neoadjuvant therapy for nonresectable colorectal. Ann. Surg. 2001, 8, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Kemeny, N.E.; Chou, J.F.; Boucher, T.M.; Capanu, M.; DeMatteo, R.P.; Jarnagin, W.R.; Allen, P.J.; Fong, Y.C.; Cercek, A.; D’Angelica, M.I. Updated long-term survival for patients with metastatic colorectal cancer treated with liver resection followed by hepatic arterial infusion and systemic chemotherapy. J. Surg. Oncol. 2016, 113, 477–484. [Google Scholar] [CrossRef] [PubMed]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; Van Krieken, J.H.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef] [PubMed]
- Gruenberger, T.; Bridgewater, J.; Chau, I.; Alfonso, P.G.; Rivoire, M.; Mudan, S.; Lasserre, S.; Hermann, F.; Waterkamp, D.; Adam, R. Bevacizumab plus mFOLFOX-6 or FOLFOXIRI in patients with initially unresectable liver metastases from colorectal cancer: The OLIVIA multinational randomised phase II trial. Ann. Oncol. 2015, 26, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.; Therasse, P.; Bogaerts, J.; Schwartz, L.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Chun, Y.S.; Vauthey, J.-N.; Boonsirikamchai, P.; Maru, D.M.; Kopetz, S.; Palavecino, M.; Curley, S.A.; Abdalla, I.K.; Kaur, H.; Charnsangavej, C.; et al. Association of computed tomography morphologic criteria with pathologic response and survival in patients treated with bevacizumab for colorectal liver metastases. JAMA 2009, 302, 2338–2344. [Google Scholar] [CrossRef] [PubMed]
- Boonsirikamchai, P.; Kaur, H.; Kuban, D.A.; Jackson, E.; Hou, P.; Choi, H. Use of Maximum Slope Images Generated From Dynamic Contrast-Enhanced MRI to Detect Locally Recurrent Prostate Carcinoma After Prostatectomy: A Practical Approach. Am. J. Roentgenol. 2012, 198, W228–W236. [Google Scholar] [CrossRef] [PubMed]
- Saltz, L.; Clarke, S.; Diaz-Rubio, E.; Scheithauer, W.; Figer, A.; Wong, R.; Koski, S.; Lichinitser, M.; Yang, T.-S.; Rivera, F.; et al. Bevacizumab in Combination With Oxaliplatin-Based Chemotherapy As First-Line Therapy in Metastatic Colorectal Cancer: A Randomized Phase III Study. J. Clin. Oncol. 2008, 26, 2013–2019. [Google Scholar] [CrossRef] [PubMed]
- Gruenberger, B.; Tamandl, D.; Schueller, J.; Scheithauer, W.; Zielinski, C.; Herbst, F.; Gruenberger, T. Bevacizumab, Capecitabine, and Oxaliplatin as Neoadjuvant Therapy for Patients with Potentially Curable Metastatic Colorectal Cancer. J. Clin. Oncol. 2008, 26, 1830–1835. [Google Scholar] [CrossRef] [PubMed]
- Wong, R.; Cunningham, D.; Barbachano, Y.; Saffery, C.; Valle, J.W.; Hickish, T.; Mudan, S.; Brown, G.; Khan, A.; Wotherspoon, A.; et al. A multicentre study of capecitabine, oxaliplatin plus bevacizumab as perioperative treatment of patients with poor-risk colorectal liver-only metastases not selected for upfront resection. Ann. Oncol. 2011, 22, 2042–2048. [Google Scholar] [CrossRef] [PubMed]
- Mukai, T.; Uehara, K.; Goto, H.; Hiramatsu, K.; Kobayashi, S.; Sakamoto, E.; Maeda, A.; Takeuchi, E.; Okada, Y.; Ebata, T.; et al. Phase II trial of neoadjuvant chemotherapy with S-1 and oxaliplatin plus bevacizumab for colorectal liver metastasis (N-SOG 05 trial). Jpn. J. Clin. Oncol. 2017, 47, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Vera, R.; Gomez Dorronsoro, M.; Lopez-Ben, S.; Viudez, A.; Queralt, B.; Hernandez, I.; Ortiz-Duran, M.R.; Zazpe, C.; Soriano, J.; Amat, I.; et al. Retrospective analysis of pathological response in colorectal cancer liver metastases following treatment with bevacizumab. Clin. Transl. Oncol. 2014, 16, 739–845. [Google Scholar] [CrossRef] [PubMed]
- Feliu, J.; Salud, A.; Safont, M.J.; García-Girón, C.; Aparicio, J.; Vera, R.; Serra, O.; Casado, E.; Jorge, M.; Escudero, P.; et al. First-line bevacizumab and capecitabine–oxaliplatin in elderly patients with mCRC: GEMCAD phase II BECOX study. Br. J. Cancer 2014, 111, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Rubio, E.; Gómez-España, A.; Massuti, B.; Sastre, J.; Abad, A.; Valladares, M.; Rivera, F.; Safont, M.J.; De Prado, P.M.; Gallén, M.; et al. First-Line XELOX Plus Bevacizumab Followed by XELOX Plus Bevacizumab or Single-Agent Bevacizumab as Maintenance Therapy in Patients with Metastatic Colorectal Cancer: The Phase III MACRO TTD Study. Oncologist 2012, 17, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Khoo, E.; O’Neill, S.; Brown, E.; Wigmore, S.J.; Harrison, E.M. Systematic review of systemic adjuvant, neoadjuvant and perioperative chemotherapy for resectable colorectal-liver metastases. HPB 2016, 18, 485–493. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | All (n = 83) | KRAS Mutant (n = 36) a | KRAS Wild Type (n = 43) |
|---|---|---|---|
| Median age, years (IQR) | 66 (58–71) | 67 (57–72) | 66 (58–71) |
| Sex, n (%) | |||
| Male | 55 (66) | 23 (64) | 29 (67) |
| Female | 28 (34) | 13 (36) | 14 (33) |
| ECOG performance status, n (%) | |||
| 0 | 64 (77) | 27 (75) | 34 (79) |
| 1 | 18 (22) | 9 (25) | 9 (21) |
| Missing | 1 (1) | 0 | 0 |
| Tumor location, n (%) | |||
| Colon | 46 (55) | 21 (58) | 24 (56) |
| Rectum | 26 (31) | 10 (28) | 15 (35) |
| Both | 2 (2) | 1 (3) | 1 (2) |
| Other | 9 (11) | 4 (11) | 3 (7) |
| Histological grade, n (%) | |||
| Grade 1 | 17 (20) | 8 (22) | 8 (19) |
| Grade 2 | 45 (54) | 20 (56) | 24 (56) |
| Grade 3 | 8 (10) | 6 (17) | 2 (5) |
| Grade 4 | 2 (2) | 0 | 2 (5) |
| Grade X | 11 (13) | 2 (6) | 7 (16) |
| Disease stage, n (%) | |||
| Not classified | 7 (8) | 2 (6) | 4 (9) |
| I | 1 (1) | 1 (3) | 0 |
| IIA | 10 (12) | 6 (17) | 4 (9) |
| IIB | 1 (1) | 1 (3) | 0 |
| III | 3 (4) | 2 (6) | 1 (2) |
| IIIA | 1 (1) | 1 (3) | 0 |
| IIIB | 2 (2) | 1 (3) | 1 (2) |
| IV | 58 (70) | 22 (61) | 33 (77) |
| Prior systemic chemotherapy, n (%) | 13 (16) | 8 (22) | 5 (12) |
| Response Category, n (%) | Overall | KRAS Mutant | KRAS Wild Type |
|---|---|---|---|
| Radiological response a | (n = 66) | (n = 31) | (n = 35) |
| Complete | 0 | 0 | 0 |
| Partial | 32 (48) | 16 (52) | 16 (45) |
| Stable disease | 29 (44) | 12 (39) | 17 (49) |
| Progressive disease | 5 (7) | 3 (9) | 2 (9) |
| Morphological response | (N = 65) | (N = 30) | (N = 35) |
| Optimal | 26 (40) | 14 (47) | 12 (34) |
| Incomplete | 33 (50) | 14 (47) | 19 (54) |
| Null | 6 (9) | 2 (6) | 4 (11) |
| Pathological response | (N = 51) | (N = 22) | (N = 29) |
| Complete | 12 (24) | 3 (14) | 9 (31) |
| Major | 29 (57) | 14 (64) | 15 (52) |
| Minor (no response) | 10 (19) | 5 (22) | 5 (17) |
| Adverse Event, n (%) | All Grades | Grade 1/2 | Grade 3/4 |
|---|---|---|---|
| Diarrhoea | 51 (65) | 41 (53) | 10 (13) |
| Asthenia | 45 (58) | 40 (51) | 5 (6) |
| Nausea | 31 (40) | 31 (40) | 0 |
| Neurotoxicity | 28 (36) | 22 (28) | 6 (8) |
| Paresthesia | 26 (33) | 26 (33) | 0 |
| Vomiting | 24 (31) | 21 (27) | 3 (4) |
| Reduced appetite | 23 (29) | 22 (28) | 1 (1) |
| Peripheral neuropathy | 13 (17) | 12 (15) | 1 (1) |
| Mucosal inflammation | 13 (17) | 12 (15) | 1 (1) |
| Abdominal pain | 12 (15) | 11 (14) | 1 (1) |
| Palmar-plantar erythrodysesthesia | 11 (14) | 8 (10) | 3 (4) |
| Neutropenia | 10 (13) | 8 (10) | 2 (3) |
| Anemia | 9 (12) | 8 (10) | 1 (1) |
| Epistaxis | 5 (6) | 4 (5) | 1 (1) |
| Hypertension | 5 (6) | 4 (5) | 1 (1) |
| Rectal hemorrhage | 4 (5) | 4 (5) | 0 |
| Proteinuria | 4 (5) | 4 (5) | 0 |
| Pulmonary embolism | 4 (5) | 1 (1) | 3 (4) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vera, R.; Gómez, M.L.; Ayuso, J.R.; Figueras, J.; García-Alfonso, P.; Martínez, V.; Lacasta, A.; Ruiz-Casado, A.; Safont, M.J.; Aparicio, J.; et al. Correlation of RECIST, Computed Tomography Morphological Response, and Pathological Regression in Hepatic Metastasis Secondary to Colorectal Cancer: The AVAMET Study. Cancers 2020, 12, 2259. https://doi.org/10.3390/cancers12082259
Vera R, Gómez ML, Ayuso JR, Figueras J, García-Alfonso P, Martínez V, Lacasta A, Ruiz-Casado A, Safont MJ, Aparicio J, et al. Correlation of RECIST, Computed Tomography Morphological Response, and Pathological Regression in Hepatic Metastasis Secondary to Colorectal Cancer: The AVAMET Study. Cancers. 2020; 12(8):2259. https://doi.org/10.3390/cancers12082259
Chicago/Turabian StyleVera, Ruth, María Luisa Gómez, Juan Ramón Ayuso, Joan Figueras, Pilar García-Alfonso, Virginia Martínez, Adelaida Lacasta, Ana Ruiz-Casado, María José Safont, Jorge Aparicio, and et al. 2020. "Correlation of RECIST, Computed Tomography Morphological Response, and Pathological Regression in Hepatic Metastasis Secondary to Colorectal Cancer: The AVAMET Study" Cancers 12, no. 8: 2259. https://doi.org/10.3390/cancers12082259
APA StyleVera, R., Gómez, M. L., Ayuso, J. R., Figueras, J., García-Alfonso, P., Martínez, V., Lacasta, A., Ruiz-Casado, A., Safont, M. J., Aparicio, J., Campos, J. M., Cámara, J. C., Martín-Richard, M., Montagut, C., Pericay, C., Vieitez, J. M., Falcó, E., Jorge, M., Marín, M., ... Viúdez, A., on behalf of the Spanish Multidisciplinary Group on Digestive Cancer (GEMCAD). (2020). Correlation of RECIST, Computed Tomography Morphological Response, and Pathological Regression in Hepatic Metastasis Secondary to Colorectal Cancer: The AVAMET Study. Cancers, 12(8), 2259. https://doi.org/10.3390/cancers12082259