Phase I Radiation Dose-Escalation Study to Investigate the Dose-Limiting Toxicity of Concurrent Intra-Arterial Chemotherapy for Unresectable Hepatocellular Carcinoma

 , , ,
, , ,
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Toxicities
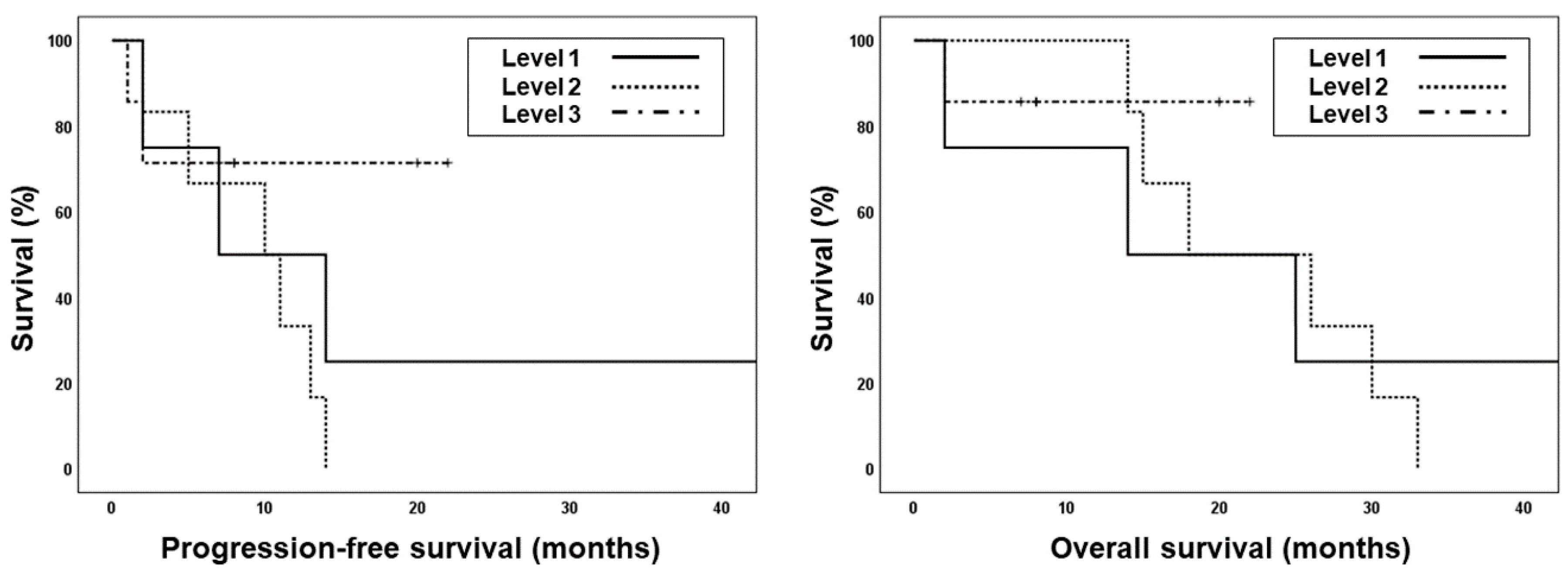
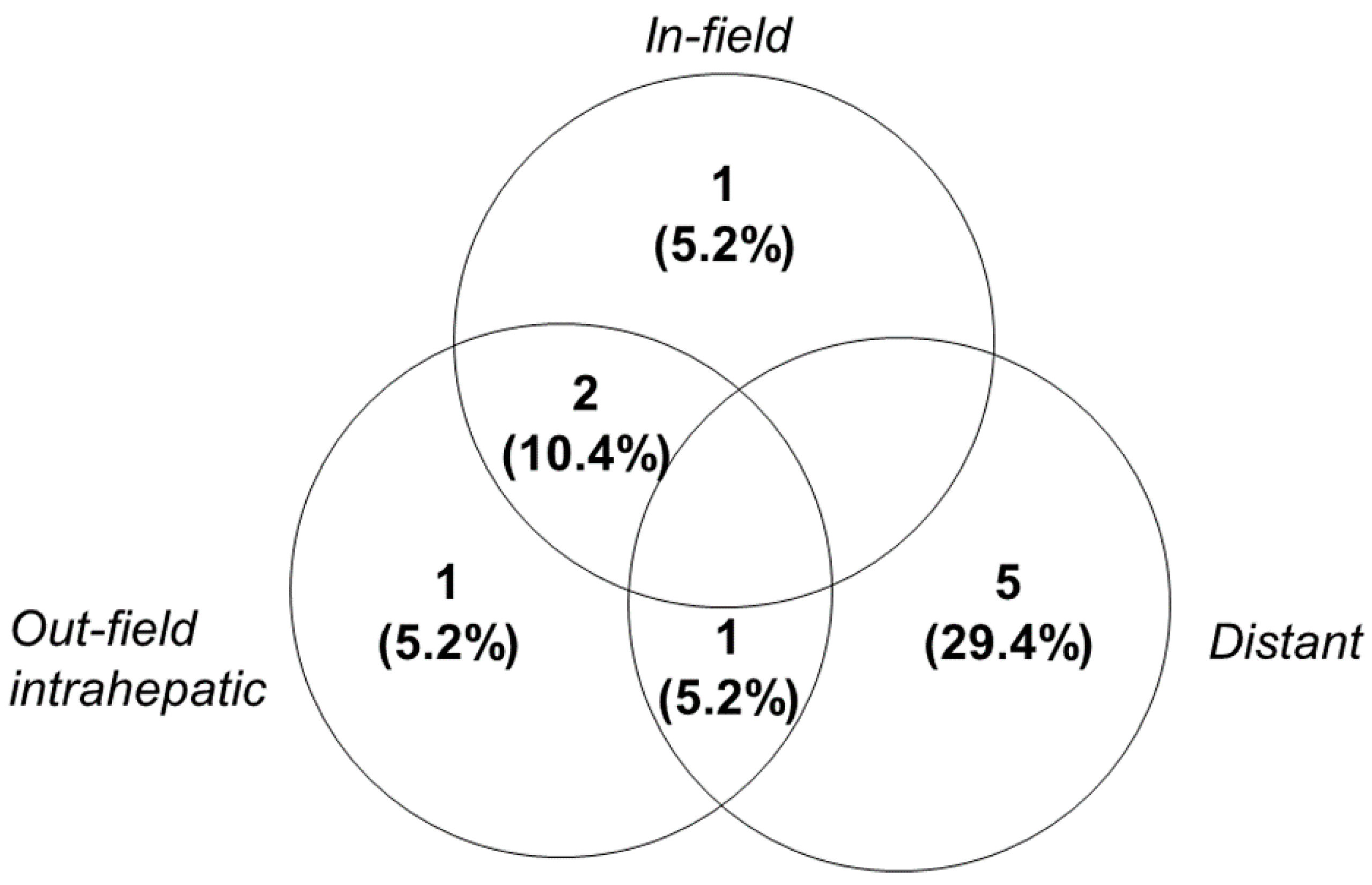
2.3. Treatment Outcomes
3. Discussion
4. Materials and Methods
4.1. Patient Eligibility
4.2. Simulation and Radiotherapy Planning
4.3. Intra-Arterial Chemotherapy
4.4. Dose-Limiting Toxicity
4.5. Follow-Up and Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
Abbreviation
| AFP | α-fetoprotein |
| ALP | Alkaline phosphatase |
| BCLC | Barcelona clinic liver cancer |
| CR | Complete response |
| CT | Computed tomography |
| CTCAE | Common Toxicity Criteria for Adverse Events |
| CTV | Clinical target volume |
| DLT | Dose-limiting toxicity |
| ECOG | Eastern Cooperative Oncology Group |
| HCC | Hepatocellular carcinoma |
| IGRT | Image-guided radiotherapy |
| IMRT | Intensity-modulated radiotherapy |
| INR | International normalized ratio |
| IRB | Institutional Review Board |
| ITV | Internal target volume |
| OAR | Organs at risk |
| OS | Overall survival |
| PD | Progressive disease |
| PFS | Progression-free survival |
| PR | Partial response |
| PTV | Planning target volume |
| RILD | Radiation-induced liver disease |
| SBRT | Stereotactic body radiotherapy |
| SD | Stable disease |
| TACE | Transarterial chemoembolization |
References
- Sherman, M. Epidemiology of hepatocellular carcinoma. Oncology 2010, 78 (Suppl. 1), 7–10. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M. Updated treatment approach to hepatocellular carcinoma. J. Gastroenterol. 2005, 40, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Beaugrand, M. Hepatocellular carcinoma: Present status and future prospects. J. Hepatol. 2003, 38 (Suppl. 1), S136–S149. [Google Scholar] [CrossRef]
- Decadt, B.; Siriwardena, A.K. Radiofrequency ablation of liver tumours: Systematic review. Lancet Oncol. 2004, 5, 550–560. [Google Scholar] [CrossRef]
- Llovet, J.M.; Real, M.I.; Montana, X.; Planas, R.; Coll, S.; Aponte, J.; Ayuso, C.; Sala, M.; Muchart, J.; Sola, R.; et al. Arterial embolisation or chemoembolisation versus symptomatic treatment in patients with unresectable hepatocellular carcinoma: A randomised controlled trial. Lancet 2002, 359, 1734–1739. [Google Scholar] [CrossRef]
- Lo, C.M.; Ngan, H.; Tso, W.K.; Liu, C.L.; Lam, C.M.; Poon, R.T.; Fan, S.T.; Wong, J. Randomized controlled trial of transarterial lipiodol chemoembolization for unresectable hepatocellular carcinoma. Hepatology 2002, 35, 1164–1171. [Google Scholar] [CrossRef]
- Kudo, M.; Matsui, O.; Izumi, N.; Kadoya, M.; Okusaka, T.; Miyayama, S.; Yamakado, K.; Tsuchiya, K.; Ueshima, K.; Hiraoka, A.; et al. Transarterial chemoembolization failure/refractoriness: Jsh-lcsgj criteria 2014 update. Oncology 2014, 87 (Suppl. 1), 22–31. [Google Scholar] [CrossRef]
- Lee, J.; Yoon, W.S.; Koom, W.S.; Rim, C.H. Role of local treatment including radiotherapy in barcelona clinic of liver cancer stage c patients: A nationwide cohort analysis in south korea. Cancer Manag. Res. 2019, 11, 1373–1382. [Google Scholar] [CrossRef]
- Yoon, H.I.; Jung, I.; Han, K.H.; Seong, J. The effect of radiotherapy in liver-confined but non-resectable barcelona clinic liver cancer stage c large hepatocellular carcinoma. Oncotarget 2016, 7, 62715–62725. [Google Scholar] [CrossRef][Green Version]
- Do Seon Song, S.H.B. Treatments other than sorafenib for patients with advanced hepatocellular carcinoma. J. Liver Cancer 2016, 16, 1–6. [Google Scholar] [CrossRef]
- Lawrence, T.S.; Robertson, J.M.; Anscher, M.S.; Jirtle, R.L.; Ensminger, W.D.; Fajardo, L.F. Hepatic toxicity resulting from cancer treatment. Int. J. Radiat. Oncol. Biol. Phys. 1995, 31, 1237–1248. [Google Scholar] [CrossRef]
- Hawkins, M.A.; Dawson, L.A. Radiation therapy for hepatocellular carcinoma: From palliation to cure. Cancer 2006, 106, 1653–1663. [Google Scholar] [CrossRef] [PubMed]
- Ben-Josef, E.; Normolle, D.; Ensminger, W.D.; Walker, S.; Tatro, D.; Ten Haken, R.K.; Knol, J.; Dawson, L.A.; Pan, C.; Lawrence, T.S. Phase ii trial of high-dose conformal radiation therapy with concurrent hepatic artery floxuridine for unresectable intrahepatic malignancies. J. Clin. Oncol. 2005, 23, 8739–8747. [Google Scholar] [CrossRef]
- Dawson, L.A.; McGinn, C.J.; Normolle, D.; Ten Haken, R.K.; Walker, S.; Ensminger, W.; Lawrence, T.S. Escalated focal liver radiation and concurrent hepatic artery fluorodeoxyuridine for unresectable intrahepatic malignancies. J. Clin. Oncol. 2000, 18, 2210–2218. [Google Scholar] [CrossRef] [PubMed]
- Seong, J.; Park, H.C.; Han, K.H.; Lee, D.Y.; Lee, J.T.; Chon, C.Y.; Moon, Y.M.; Suh, C.O. Local radiotherapy for unresectable hepatocellular carcinoma patients who failed with transcatheter arterial chemoembolization. Int. J. Radiat. Oncol. Biol. Phys. 2000, 47, 1331–1335. [Google Scholar] [CrossRef]
- Song, J.E.; Jung, K.S.; Kim, D.Y.; Song, K.; Won, J.Y.; Lee, H.W.; Kim, B.K.; Kim, S.U.; Park, J.Y.; Ahn, S.H.; et al. Transarterial radioembolization versus concurrent chemoradiation therapy for locally advanced hepatocellular carcinoma: A propensity score matching analysis. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 396–406. [Google Scholar] [CrossRef]
- Park, M.S.; Kim, S.U.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.H.; Chon, C.Y.; Seong, J. Combination treatment of localized concurrent chemoradiation therapy and transarterial chemoembolization in locally advanced hepatocellular carcinoma with intrahepatic metastasis. Cancer Chemother. Pharmacol. 2013, 71, 165–173. [Google Scholar] [CrossRef]
- Korean Liver Cancer Association; National Cancer Center. 2018 korean liver cancer association-national cancer center korea practice guidelines for the management of hepatocellular carcinoma. Gut Liver 2019, 13, 227–299. [Google Scholar] [CrossRef]
- Byun, H.K.; Kim, H.J.; Im, Y.R.; Kim, D.Y.; Han, K.H.; Seong, J. Dose escalation in radiotherapy for incomplete transarterial chemoembolization of hepatocellular carcinoma. Strahlenther. Onkol. 2019. [Google Scholar] [CrossRef]
- Choi, C.; Koom, W.S.; Kim, T.H.; Yoon, S.M.; Kim, J.H.; Lee, H.S.; Nam, T.K.; Seong, J. A prospective phase 2 multicenter study for the efficacy of radiation therapy following incomplete transarterial chemoembolization in unresectable hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 1051–1060. [Google Scholar] [CrossRef]
- Koo, J.E.; Kim, J.H.; Lim, Y.S.; Park, S.J.; Won, H.J.; Sung, K.B.; Suh, D.J. Combination of transarterial chemoembolization and three-dimensional conformal radiotherapy for hepatocellular carcinoma with inferior vena cava tumor thrombus. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 180–187. [Google Scholar] [CrossRef]
- Oh, D.; Lim, D.H.; Park, H.C.; Paik, S.W.; Koh, K.C.; Lee, J.H.; Choi, M.S.; Yoo, B.C.; Lim, H.K.; Lee, W.J.; et al. Early three-dimensional conformal radiotherapy for patients with unresectable hepatocellular carcinoma after incomplete transcatheter arterial chemoembolization: A prospective evaluation of efficacy and toxicity. Am. J. Clin. Oncol. 2010, 33, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.W.; Oh, D.; Park, H.C.; Lim, D.H.; Shin, S.W.; Cho, S.K.; Gwak, G.Y.; Choi, M.S.; Paik, Y.H.; Paik, S.W. Transcatheter arterial chemoembolization and radiation therapy for treatment-naive patients with locally advanced hepatocellular carcinoma. Radiat. Oncol. J. 2014, 32, 14–22. [Google Scholar] [CrossRef]
- Yoon, S.M.; Ryoo, B.Y.; Lee, S.J.; Kim, J.H.; Shin, J.H.; An, J.H.; Lee, H.C.; Lim, Y.S. Efficacy and safety of transarterial chemoembolization plus external beam radiotherapy vs sorafenib in hepatocellular carcinoma with macroscopic vascular invasion: A randomized clinical trial. JAMA Oncol. 2018, 4, 661–669. [Google Scholar] [CrossRef] [PubMed]
- Seong, J.; Keum, K.C.; Han, K.H.; Lee, D.Y.; Lee, J.T.; Chon, C.Y.; Moon, Y.M.; Suh, C.O.; Kim, G.E. Combined transcatheter arterial chemoembolization and local radiotherapy of unresectable hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 393–397. [Google Scholar] [CrossRef]
- Yamada, K.; Izaki, K.; Sugimoto, K.; Mayahara, H.; Morita, Y.; Yoden, E.; Matsumoto, S.; Soejima, T.; Sugimura, K. Prospective trial of combined transcatheter arterial chemoembolization and three-dimensional conformal radiotherapy for portal vein tumor thrombus in patients with unresectable hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2003, 57, 113–119. [Google Scholar] [CrossRef]
- Yoon, H.I.; Lee, I.J.; Han, K.H.; Seong, J. Improved oncologic outcomes with image-guided intensity-modulated radiation therapy using helical tomotherapy in locally advanced hepatocellular carcinoma. J. Cancer Res. Clin. Oncol. 2014, 140, 1595–1605. [Google Scholar] [CrossRef]
- Han, K.H.; Seong, J.; Kim, J.K.; Ahn, S.H.; Lee, D.Y.; Chon, C.Y. Pilot clinical trial of localized concurrent chemoradiation therapy for locally advanced hepatocellular carcinoma with portal vein thrombosis. Cancer 2008, 113, 995–1003. [Google Scholar] [CrossRef]
- Park, H.C.; Seong, J.; Han, K.H.; Chon, C.Y.; Moon, Y.M.; Suh, C.O. Dose-response relationship in local radiotherapy for hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2002, 54, 150–155. [Google Scholar] [CrossRef]
- Byun, H.K.; Kim, H.J.; Im, Y.R.; Kim, D.Y.; Han, K.H.; Seong, J. Dose escalation by intensity modulated radiotherapy in liver-directed concurrent chemoradiotherapy for locally advanced bclc stage c hepatocellular carcinoma. Radiother. Oncol. 2019, 133, 1–8. [Google Scholar] [CrossRef]
- Tse, R.V.; Hawkins, M.; Lockwood, G.; Kim, J.J.; Cummings, B.; Knox, J.; Sherman, M.; Dawson, L.A. Phase i study of individualized stereotactic body radiotherapy for hepatocellular carcinoma and intrahepatic cholangiocarcinoma. J. Clin. Oncol. 2008, 26, 657–664. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Seong, J.; Lee, I.J.; Woo, J.Y.; Han, K.H. Phase i dose escalation study of helical intensity-modulated radiotherapy-based stereotactic body radiotherapy for hepatocellular carcinoma. Oncotarget 2016, 7, 40756–40766. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Kim, D.Y.; Han, K.H.; Seong, J. Phase i/ii trial of helical imrt-based stereotactic body radiotherapy for hepatocellular carcinoma. Dig. Liver Dis. 2019, 51, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Bae, S.H.; Park, H.C.; Yoon, W.S.; Yoon, S.M.; Jung, I.H.; Lee, I.J.; Kim, J.W.; Seong, J.; Kim, T.H.; Nam, T.K.; et al. Treatment outcome after fractionated conformal radiotherapy for hepatocellular carcinoma in patients with child-pugh classification b in korea (krog 16-05). Cancer Res. Treat. 2019, 51, 1589–1599. [Google Scholar] [CrossRef]
- Milano, M.T.; Constine, L.S.; Okunieff, P. Normal tissue toxicity after small field hypofractionated stereotactic body radiation. Radiat. Oncol. 2008, 3, 36. [Google Scholar] [CrossRef]
- Guha, C.; Kavanagh, B.D. Hepatic radiation toxicity: Avoidance and amelioration. Semin. Radiat. Oncol. 2011, 21, 256–263. [Google Scholar] [CrossRef]
- Toyoda, H.; Lai, P.B.; O’Beirne, J.; Chong, C.C.; Berhane, S.; Reeves, H.; Manas, D.; Fox, R.P.; Yeo, W.; Mo, F.; et al. Long-term impact of liver function on curative therapy for hepatocellular carcinoma: Application of the albi grade. Br. J. Cancer 2016, 114, 744–750. [Google Scholar] [CrossRef]
- Johnson, P.J.; Berhane, S.; Kagebayashi, C.; Satomura, S.; Teng, M.; Reeves, H.L.; O’Beirne, J.; Fox, R.; Skowronska, A.; Palmer, D.; et al. Assessment of liver function in patients with hepatocellular carcinoma: A new evidence-based approach-the albi grade. J. Clin. Oncol. 2015, 33, 550–558. [Google Scholar] [CrossRef]
- Su, T.S.; Yang, H.M.; Zhou, Y.; Huang, Y.; Liang, P.; Cheng, T.; Chen, L.; Li, L.Q.; Liang, S.X. Albumin—Bilirubin (albi) versus child-turcotte-pugh (ctp) in prognosis of hcc after stereotactic body radiation therapy. Radiat. Oncol. 2019, 14, 50. [Google Scholar] [CrossRef]
- Ronald, J.; Wang, Q.; Choi, S.S.; Suhocki, P.V.; Hall, M.D.; Smith, T.P.; Kim, C.Y. Albumin-bilirubin grade versus meld score for predicting survival after transjugular intrahepatic portosystemic shunt (tips) creation. Diagn. Interv. Imaging 2018, 99, 163–168. [Google Scholar] [CrossRef]
- Wang, Y.Y.; Zhong, J.H.; Su, Z.Y.; Huang, J.F.; Lu, S.D.; Xiang, B.D.; Ma, L.; Qi, L.N.; Ou, B.N.; Li, L.Q. Albumin-bilirubin versus child-pugh score as a predictor of outcome after liver resection for hepatocellular carcinoma. Br. J. Surg. 2016, 103, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Chopra, S.; George, K.; Engineer, R.; Rajamanickam, K.; Nojin, S.; Joshi, K.; Swamidas, J.; Shetty, N.; Patkar, S.; Patil, P.; et al. Stereotactic body radio therapy for inoperable large hepatocellular cancers: Results from a clinical audit. Br. J. Radiol. 2019, 92, 20181053. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.H.; Kim, M.S.; Chang, J.S.; Han, K.H.; Kim, D.Y.; Seong, J. Therapeutic benefit of radiotherapy in huge (>/=10 cm) unresectable hepatocellular carcinoma. Liver Int. 2014, 34, 784–794. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Fukumitsu, N.; Kamizawa, S.; Numajiri, H.; Nemoto Murofushi, K.; Ohnishi, K.; Aihara, T.; Ishikawa, H.; Okumura, T.; Tsuboi, K.; et al. A validated proton beam therapy patch-field protocol for effective treatment of large hepatocellular carcinoma. J. Radiat. Res. 2018, 59, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Sugahara, S.; Oshiro, Y.; Nakayama, H.; Fukuda, K.; Mizumoto, M.; Abei, M.; Shoda, J.; Matsuzaki, Y.; Thono, E.; Tokita, M.; et al. Proton beam therapy for large hepatocellular carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Park, H.C.; Yu, J.I.; Cheng, J.C.; Zeng, Z.C.; Hong, J.H.; Wang, M.L.; Kim, M.S.; Chi, K.H.; Liang, P.C.; Lee, R.C.; et al. Consensus for radiotherapy in hepatocellular carcinoma from the 5th asia-pacific primary liver cancer expert meeting (apple 2014): Current practice and future clinical trials. Liver Cancer 2016, 5, 162–174. [Google Scholar] [CrossRef]
- Kim, J.W.; Seong, J.; Park, M.S.; Kim, K.S.; Park, Y.N.; Han, K.H.; Keum, K.C.; Lee, I.J. Radiological-pathological correlation study of hepatocellular carcinoma undergoing local chemoradiotherapy and surgery. J. Gastroenterol. Hepatol. 2016, 31, 1619–1627. [Google Scholar] [CrossRef]
- Lee, I.J.; Seong, J.; Koom, W.S.; Kim, Y.B.; Jeon, B.C.; Kim, J.H.; Han, K.H. Selection of the optimal radiotherapy technique for locally advanced hepatocellular carcinoma. Jpn. J. Clin. Oncol. 2011, 41, 882–889. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Median | (Range) | No. of Patients (n = 17) | (%) |
|---|---|---|---|---|
| Age | 63 | (33–80) | ||
| Sex | ||||
| Male | 15 | (88.2) | ||
| Female | 2 | (11.8) | ||
| ECOG PS | ||||
| 0 | 8 | (47.1) | ||
| 1 | 9 | (52.9) | ||
| Underlying liver disease | ||||
| HBV | 12 | (70.6) | ||
| HCV | 1 | (5.9) | ||
| Without viral infections | 4 | (23.5) | ||
| Underlying liver cirrhosis | ||||
| No | 4 | 23.5 | ||
| Yes | 13 | 76.5 | ||
| AFP (ng/mL) | 45 | (2.2–38,300) | ||
| >9 ng/mL | 12 | 70.6 | ||
| PIVKA-II (mIU/mL) | 381.4 | (23–185,072) | ||
| >35 mIU/mL | 13 | 76.5 | ||
| Child-Pugh class | ||||
| A5 | 14 | 82.4 | ||
| A6 | 3 | 17.6 | ||
| Platelet count | 163 k | (55–408 k) | 5 | 29.4 |
| Mild thrombocytopenia (75–150 k/uL) | 3 | 15.8 | ||
| Moderate thrombocytopenia (50–75 k/μL) | 2 | 11.8 | ||
| UICC stage | ||||
| T2 | 2 | 11.8 | ||
| T3 | 8 | 47.1 | ||
| T4 | 7 | 41.2 | ||
| N0 | 16 | 94.1 | ||
| N1 | 1 | 5.9 | ||
| Primary tumor size (cm) | 8 | (2.6–16) | ||
| Number of tumor(s) | ||||
| 1 | 8 | 47.1 | ||
| 2–4 | 7 | 41.2 | ||
| ≥5 | 2 | 11.8 | ||
| Involved site | ||||
| Right Lobe | 11 | 64.7 | ||
| Left Lobe | 2 | 11.8 | ||
| Both Lobes | 4 | 23.5 | ||
| Vascular invasion | ||||
| No | 3 | 17.6 | ||
| Yes | 14 | 82.4 | ||
| Previous treatment | ||||
| None | 13 | 76.5 | ||
| TACE | 4 | 23.5 | ||
| TACI | 1 | 5.9 | ||
| RFA | 1 | 5.9 |
| Level 1 | Level 2 | Level 3 | Total | |||||
|---|---|---|---|---|---|---|---|---|
| (n = 4) | (n = 6) | (n = 7) | (n = 17) | |||||
| Parameters | Median | (Range) | Median | (Range) | Median | (Range) | Median | (Range) |
| PTV1 (cc) | 398 | (277–467) | 490 | (69–2086) | 355 | (260–909) | 398 | (69–2086) |
| PTV2 (cc) | 819 | (561–2066) | 717 | (209–2814) | 758 | (525–1634) | 784 | (209–2814) |
| Uninvolved liver volume (cc) | 1018 | (876–1643) | 1138 | (814–1393) | 1176 | (855–1511) | 1122 | (814–1643) |
| Mean dose of whole liver (Gy) | 30.4 | (20.5–42.1) | 28.1 | (18.8–38.2) | 30.1 | (17.7–39.6) | 30.4 | (18.8–42.1) |
| Mean dose of uninvolved liver (Gy) | 21.3 | (15.35–27.4) | 21.6 | (19.2–25.7) | 18.2 | (11.5–24.4) | 20.4 | (11.5–27.4) |
| Maximum dose of stomach (Gy) | 42.6 | (20.3–55.4) | 27.9 | (15.1–54.0) | 51.2 | (26.8–56.3) | 40.9 | (15.1–56.3) |
| Maximum dose of duodenum (Gy) | 40.0 | (21.4–52.2) | 37.8 | (2.1–54.6) | 48.5 | (15.1–54.1) | 40 | (2.1–54.6) |
| Maximum dose of spinal cord (Gy) | 29.8 | (26.8–35.2) | 25.7 | (18.7–37.4) | 36.8 | (24.7–44.0) | 30.5 | (18.7–44.0) |
| Mean dose of right kidney (Gy) | 5.6 | (2.5–19.4) | 6.4 | (1.1–20.4) | 2.8 | (1.3–17.5) | 6.4 | (1.1–20.4) |
| Mean dose of left kidney (Gy) | 4.6 | (0.8–16.9) | 3.2 | (0.6–6.9) | 2.4 | (0.6–7.5) | 3.2 | (0.6–16.9) |
| Level 1 (n = 4) | Level 2 (n = 6) | Level 3 (n = 7) | Total (n = 17) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | ||||||||||
| Toxicities | G1 | G2 | G3 | G1 | G2 | G3 | G1 | G2 | G3 | G1 | G2 | G3 | |
| GI toxicity | Nausea | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 (14.3) | 0 | 0 | 1 (5.9) | 0 |
| Vomiting | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |
| Pain | 1 (25) | 0 | 0 | 1 (16.7) | 1 (16.7) | 0 | 1 (14.3) | 0 | 0 | 3 (17.6) | 1 (5.9) | 0 | |
| Liver function | AST | 2 (50) | 1 (25) | 0 | 5 (83.3) | 0 | 0 | 6 (85.7) | 0 | 0 | 13 (76.5) | 1 (5.9) | 0 |
| ALT | 2 (50) | 0 | 0 | 0 | 0 | 0 | 4 (57.1) | 0 | 0 | 6 (35.3) | 0 | 0 | |
| Albumin | 3 (75) | 1 (25) | 0 | 4 (66.7) | 1 (16.7) | 0 | 4 (57.1) | 1 (14.3) | 0 | 11 (64.7) | 3 (17.6) | 0 | |
| Bilirubin | 0 | 0 | 1 (25) | 0 | 2 (33.3) | 0 | 0 | 0 | 1 (14.3) | 0 | 2 (11.8) | 2 (11.8) | |
| INR | 4 (100) | 0 | 0 | 6 (100) | 0 | 0 | 5 (71.4) | 0 | 0 | 15 (88.2) | 0 | 0 | |
| ALP | 2 (50) | 1 (25) | 0 | 5 (83.3) | 0 | 0 | 4 (57.1) | 3 (42.9) | 0 | 11 (64.7) | 4 (23.5) | 0 | |
| Hematologic | Hemoglobin | 2 (50) | 2 (50) | 0 | 2 (33.3) | 0 | 0 | 3 (42.9) | 0 | 1 (14.3) | 7 (41.2) | 2 (11.8) | 1 (5.9) |
| WBC | 1 (25) | 2 (50) | 0 | 2 (33.3) | 0 | 0 | 2 (28.6) | 3 (42.9) | 0 | 5 (29.4) | 5 (29.4) | 0 | |
| ANC | 2 (50) | 0 | 1 (25) | 1 (16.7) | 1 (16.7) | 0 | 0 | 4 (57.1) | 1 (14.3) | 3 (17.6) | 5 (29.4) | 2 (11.8) | |
| Platelet | 2 (50) | 1 (25) | 1 (25) | 0 | 1 (16.7) | 1 (16.7) | 0 | 2 (28.6) | 0 | 2 (11.8) | 4 (23.5) | 2 (11.8) | |
| Other | General weakness | 0 | 1 (25) | 0 | 3 (50) | 0 | 0 | 0 | 1 (14.3) | 0 | 3 (17.6) | 2 (11.8) | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, Y.; Kim, J.W.; Kim, J.K.; Lee, K.S.; Lee, J.I.; Lee, H.W.; Lee, K.-H.; Joo, S.-M.; Lim, J.H.; Lee, I.J. Phase I Radiation Dose-Escalation Study to Investigate the Dose-Limiting Toxicity of Concurrent Intra-Arterial Chemotherapy for Unresectable Hepatocellular Carcinoma. Cancers 2020, 12, 1612. https://doi.org/10.3390/cancers12061612
Cho Y, Kim JW, Kim JK, Lee KS, Lee JI, Lee HW, Lee K-H, Joo S-M, Lim JH, Lee IJ. Phase I Radiation Dose-Escalation Study to Investigate the Dose-Limiting Toxicity of Concurrent Intra-Arterial Chemotherapy for Unresectable Hepatocellular Carcinoma. Cancers. 2020; 12(6):1612. https://doi.org/10.3390/cancers12061612
Chicago/Turabian StyleCho, Yeona, Jun Won Kim, Ja Kyung Kim, Kwan Sik Lee, Jung Il Lee, Hyun Woong Lee, Kwang-Hun Lee, Seung-Moon Joo, Jin Hong Lim, and Ik Jae Lee. 2020. "Phase I Radiation Dose-Escalation Study to Investigate the Dose-Limiting Toxicity of Concurrent Intra-Arterial Chemotherapy for Unresectable Hepatocellular Carcinoma" Cancers 12, no. 6: 1612. https://doi.org/10.3390/cancers12061612
APA StyleCho, Y., Kim, J. W., Kim, J. K., Lee, K. S., Lee, J. I., Lee, H. W., Lee, K.-H., Joo, S.-M., Lim, J. H., & Lee, I. J. (2020). Phase I Radiation Dose-Escalation Study to Investigate the Dose-Limiting Toxicity of Concurrent Intra-Arterial Chemotherapy for Unresectable Hepatocellular Carcinoma. Cancers, 12(6), 1612. https://doi.org/10.3390/cancers12061612