Diffusion-Weighted Imaging in Oncology: An Update

 ,
,  ,
,  ,
,  ,
,  ,
,  ,
,  , and
, and
Abstract
1. Introduction
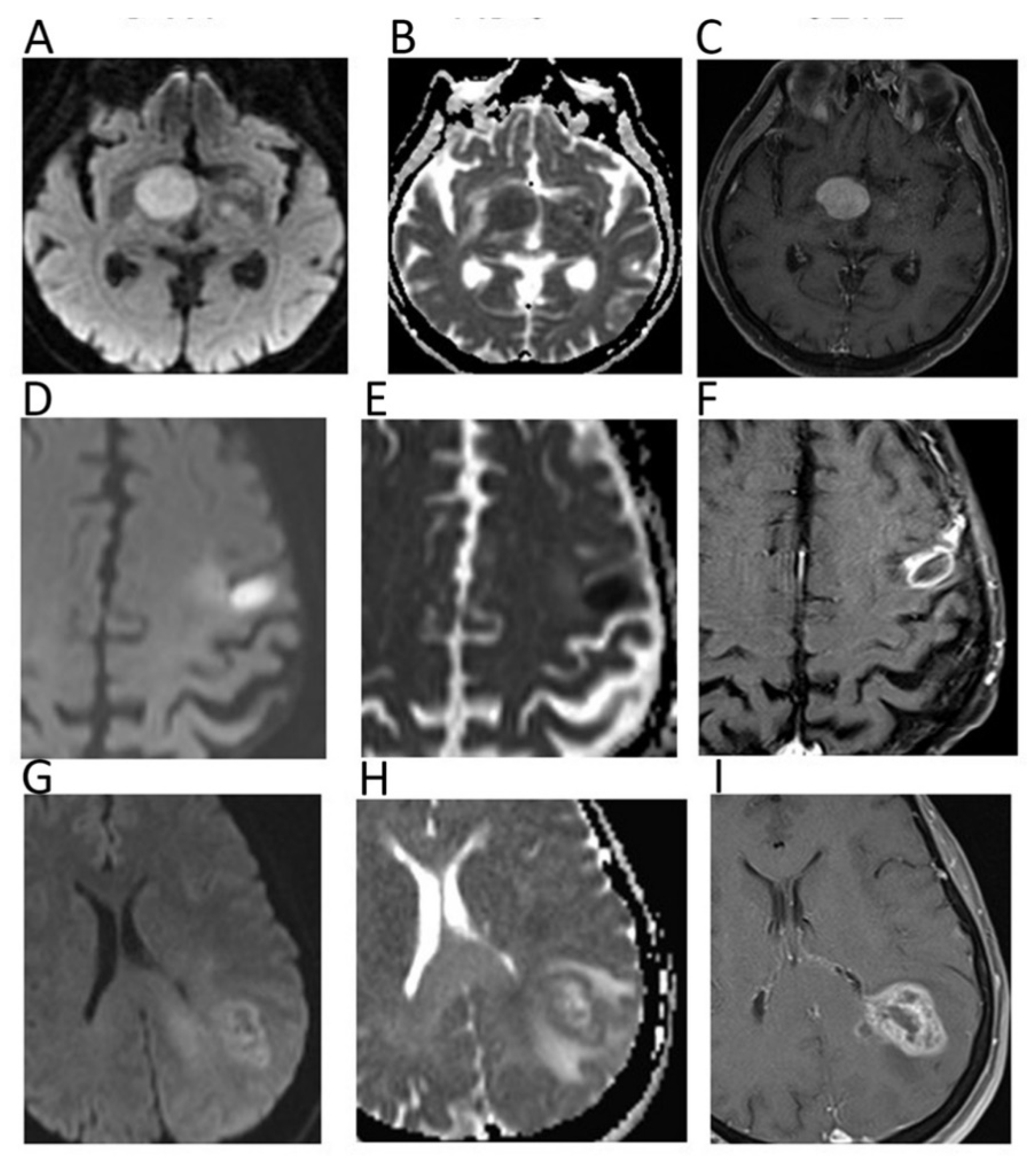
2. Neuro
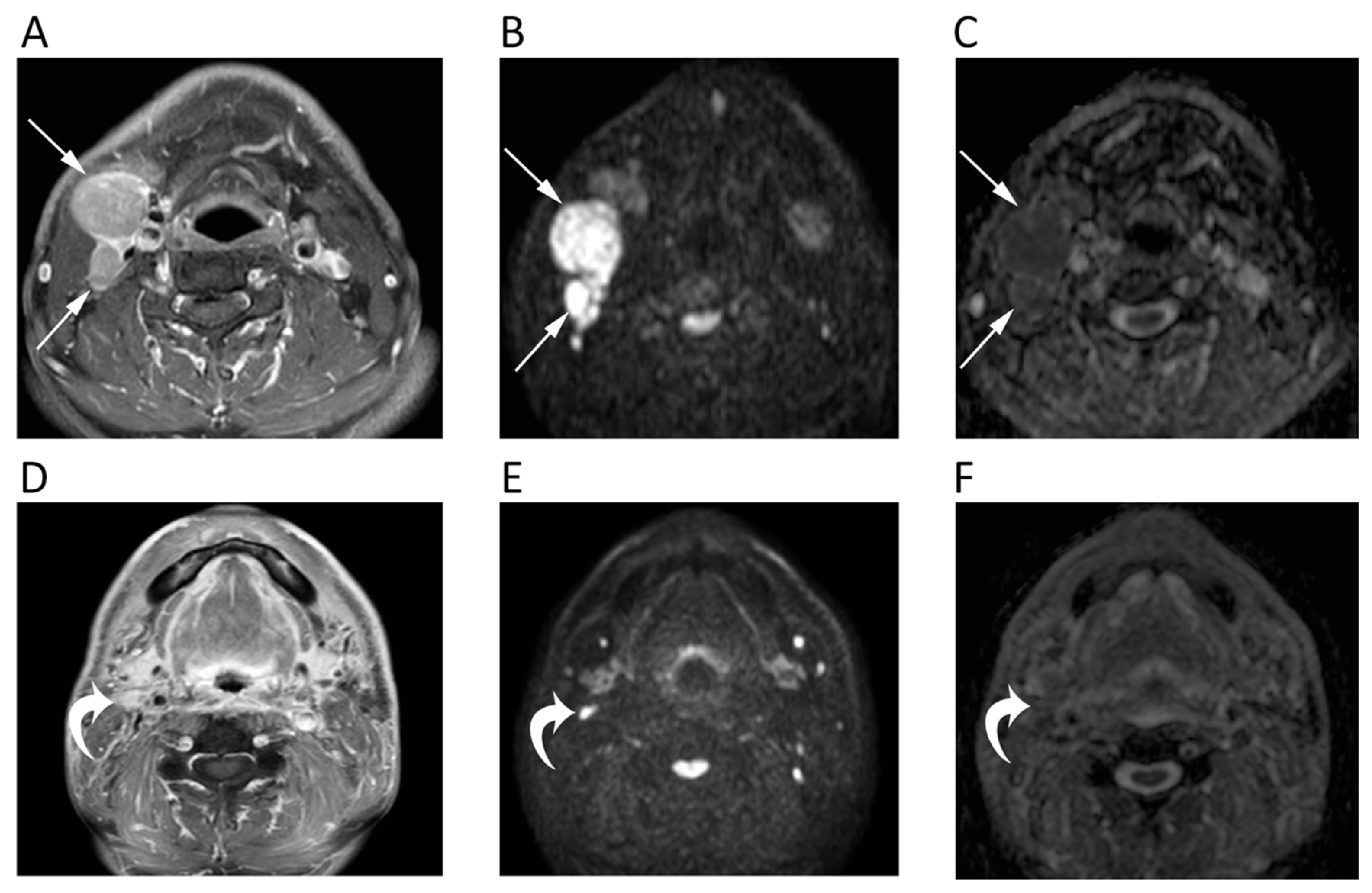
3. Head and Neck
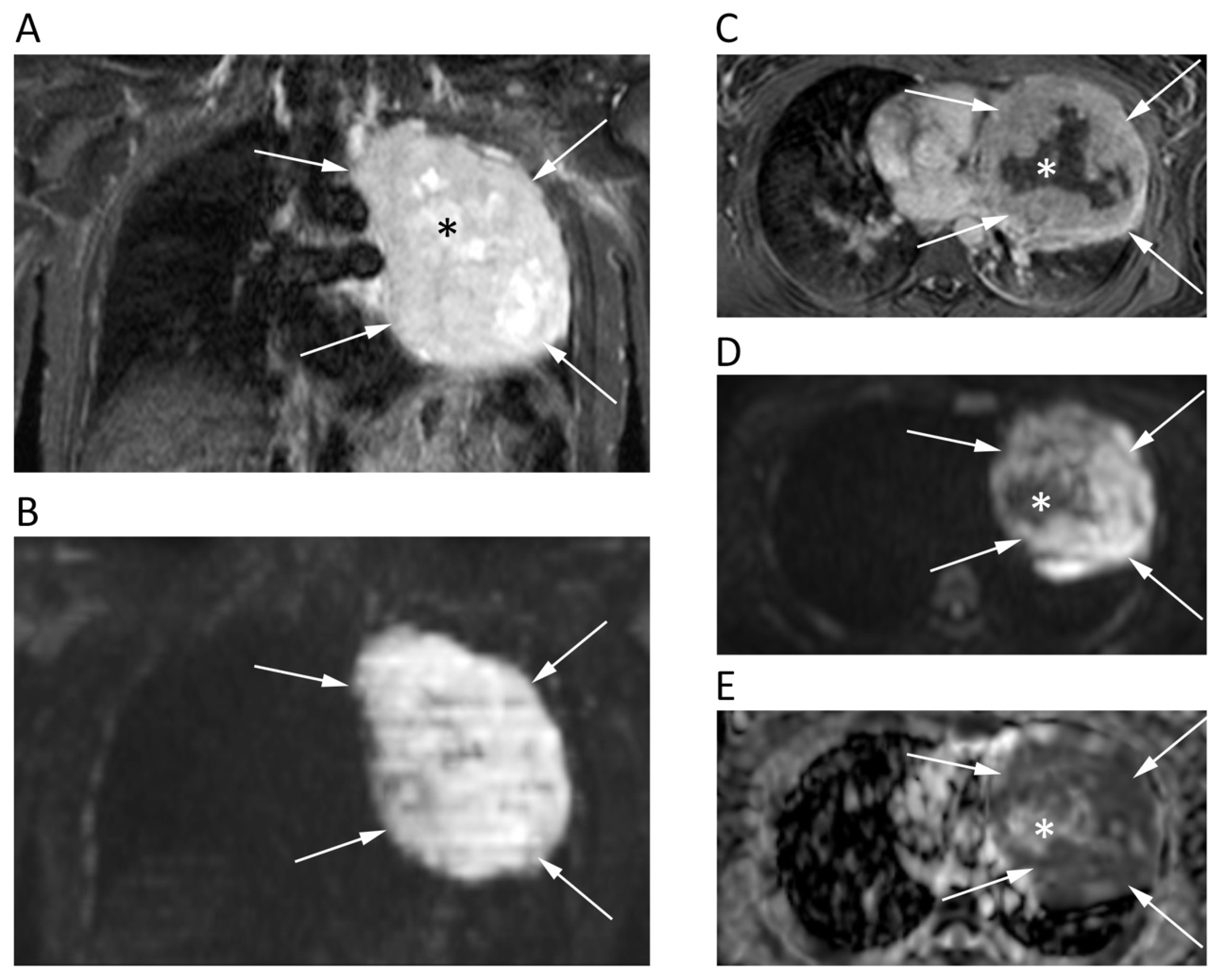
4. Chest
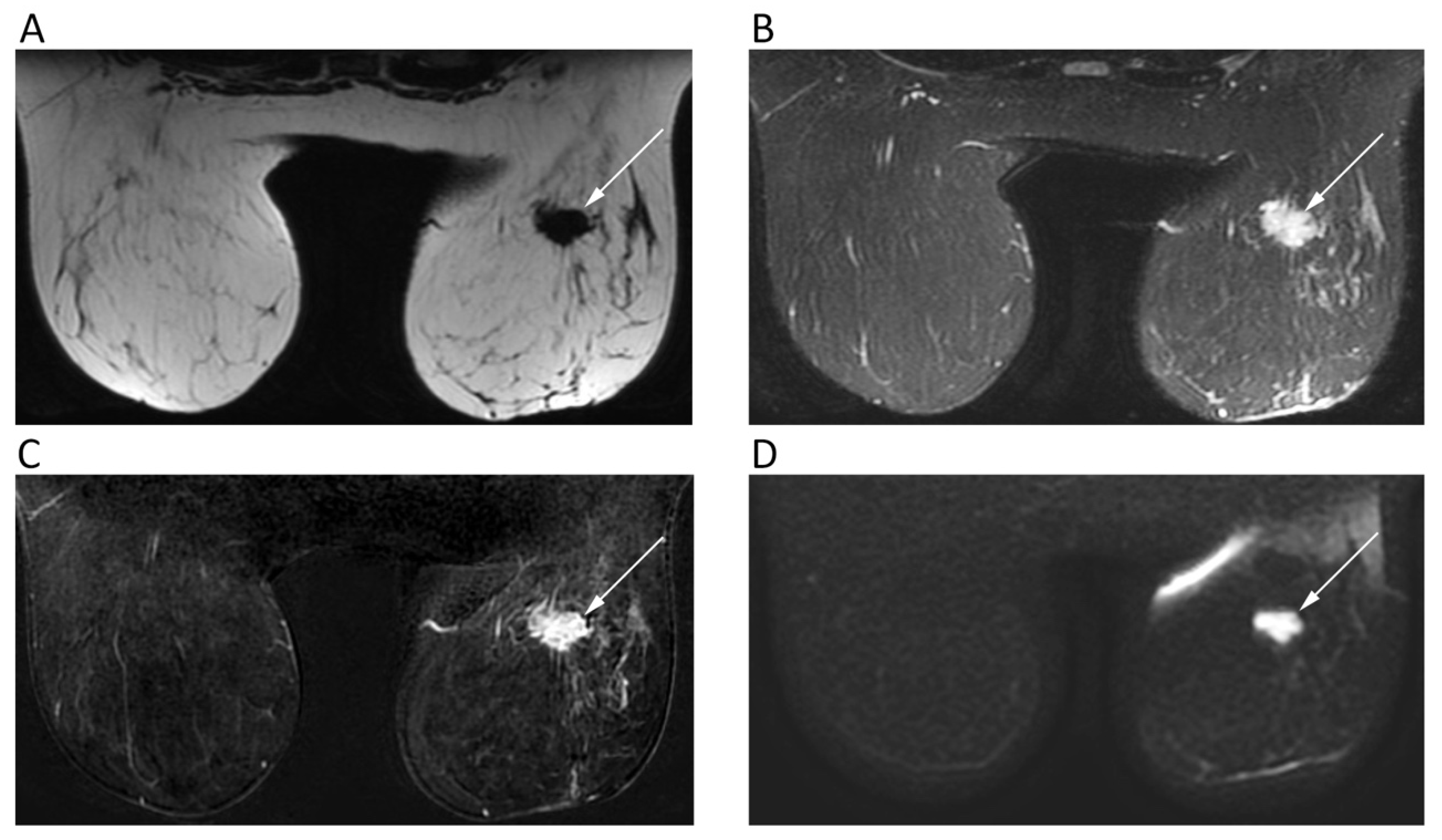
5. Breast
6. Hepatobiliary
7. Pancreas
8. Esophago-Gastro-Intestinal
9. Gynecological
10. Urinary System and Adrenal
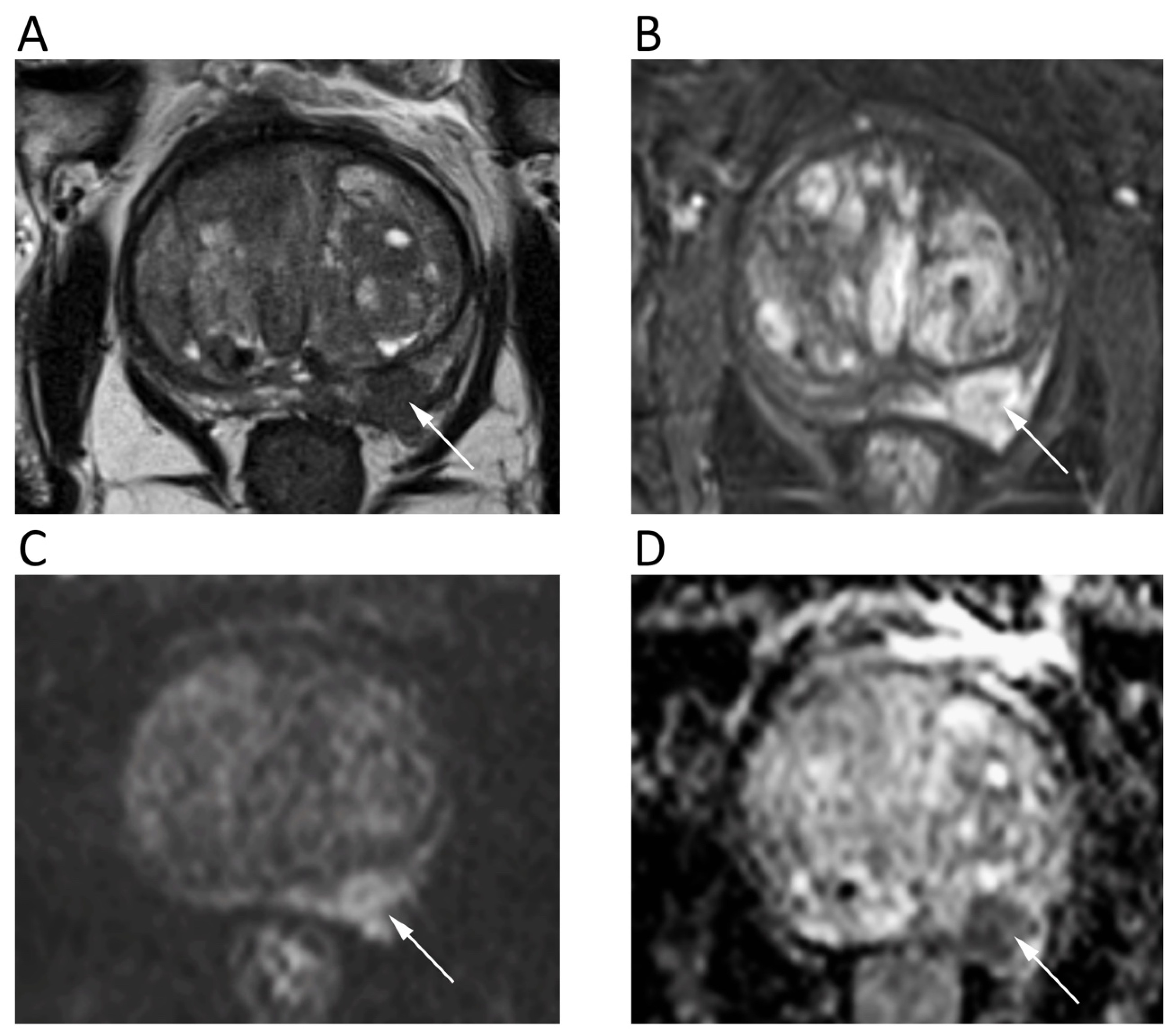
11. Prostate
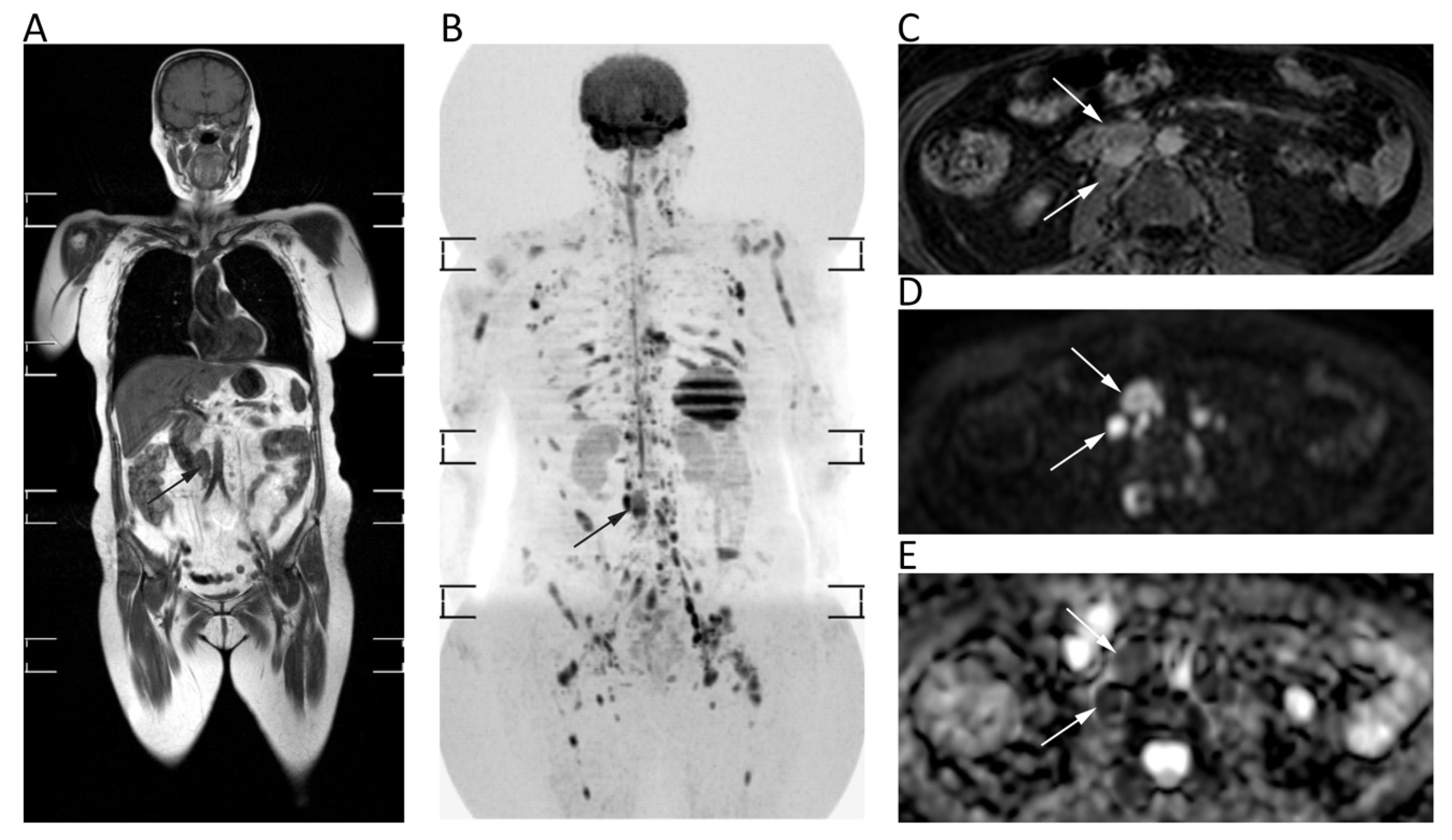
12. Lymph Nodes and Spleen
13. Bone Tumors
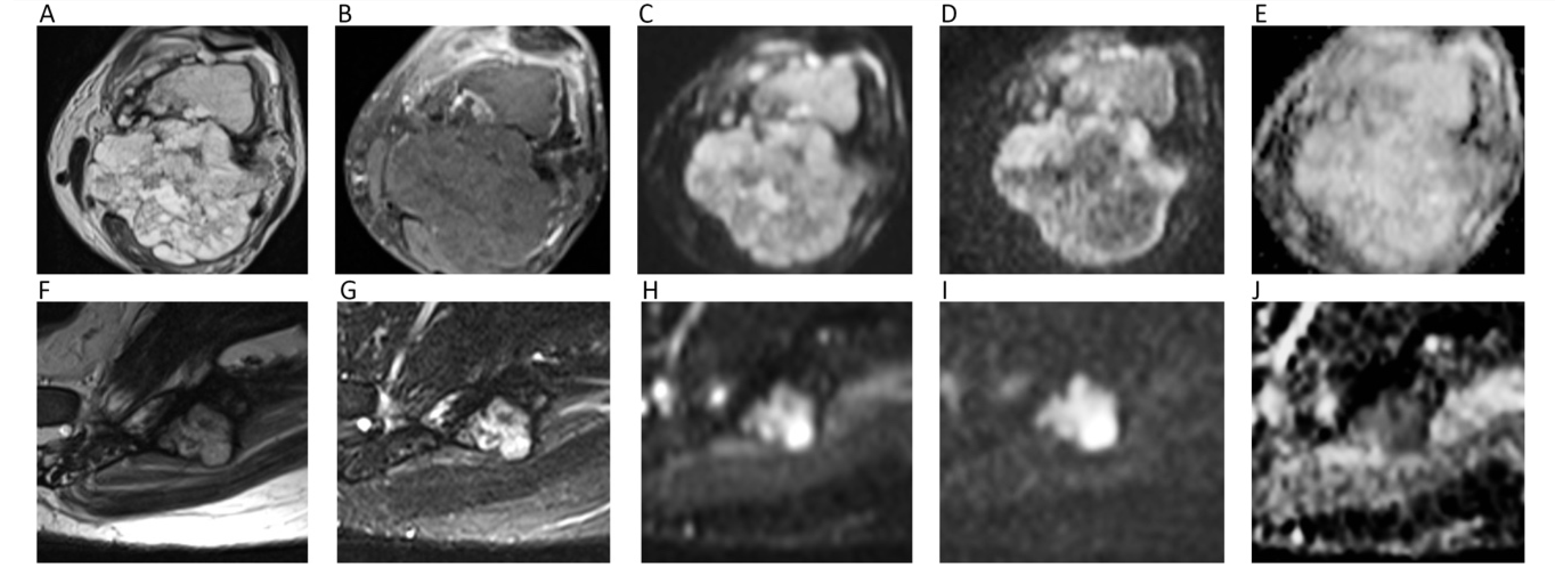
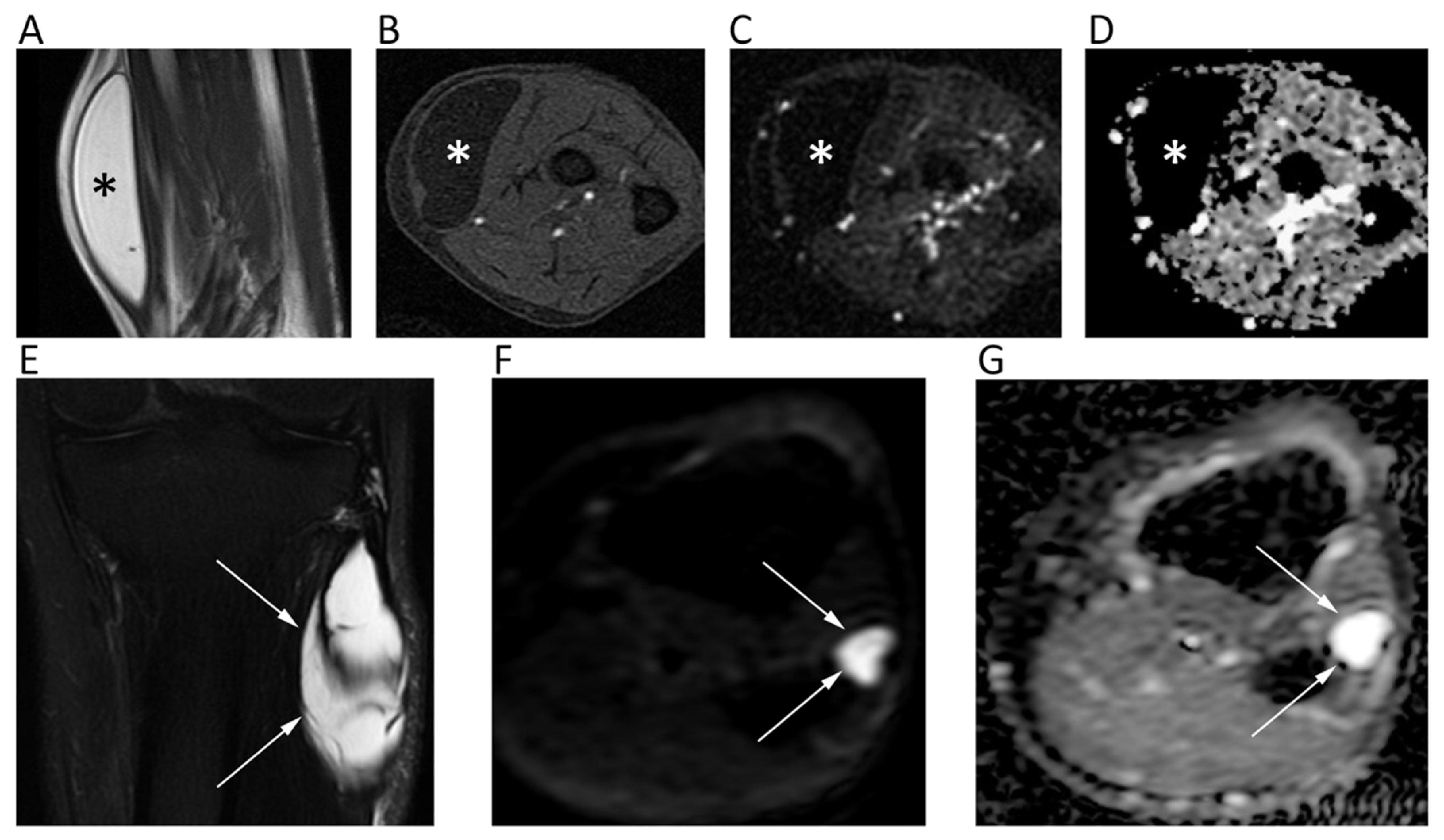
14. Soft Tissue Tumors
15. Conclusions and Future Perspectives
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| DWI | Diffusion weighted imaging |
| MRI | Magnetic Resonance Imaging |
| ADC | Apparent diffusion coefficient |
| HGGs | High-Grade Gliomas |
| IVIM | Intravoxel incoherent motion |
| DKI | Diffusional kurtosis imaging |
| HNT | Head and neck tumor |
| HNSCC | Head and neck squamous cell carcinoma |
| STIR | Short tau inversion recovery |
| DCE | Dynamic contrast enhanced |
| HCC | Hepatocellular carcinoma |
| PPV | Positive predictive value |
| NPV | Negative predictive value |
| pNENs | Pancreatic neuroendocrine neoplasms |
| ccRCC | Clear cell renal cell carcinoma |
| mpMRI | Multi-parametric MRI |
| PCa | Prostate cancer |
| PI-RADS | Prostate imaging reporting and data system |
| WB | Whole-body |
| DWIBS | DWI with background suppression |
| BT | Bone tumors |
| STT | Soft tissue tumors |
References
- Svolos, P.; Kousi, E.; Kapsalaki, E.; Theodorou, K.; Fezoulidis, I.; Kappas, C.; Tsougos, I. The role of diffusion and perfusion weighted imaging in the differential diagnosis of cerebral tumors: A review and future perspectives Tumour charcterisation. Cancer Imaging 2014, 14, 20. [Google Scholar] [CrossRef]
- Muccio, C.F.; Caranci, F.; D’Arco, F.; Cerase, A.; De Lipsis, L.; Esposito, G.; Tedeschi, E.; Andreula, C. Magnetic resonance features of pyogenic brain abscesses and differential diagnosis using morphological and functional imaging studies: A pictorial essay. J. Neuroradiol. 2014, 41, 153–167. [Google Scholar] [CrossRef] [PubMed]
- Yamasaki, F.; Kurisu, K.; Satoh, K.; Arita, K.; Sugiyama, K.; Ohtaki, M.; Takaba, J.; Tominaga, A.; Hanaya, R.; Yoshioka, H.; et al. Apparent diffusion coefficient of human brain tumors at MR imaging. Radiology 2005, 235, 985–991. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Padhani, A.R.; Chenevert, T.L.; Koh, D.-M.; De Keyzer, F.; Taouli, B.; Le Bihan, D. Body diffusion kurtosis imaging: Basic principles, applications, and considerations for clinical practice. J. Magn. Reson. Imaging 2015, 42, 1190–1202. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; terBrugge, K.; Mikulis, D.; Choi, D.S.; Bae, J.M.; Lee, S.K.; Moon, S.Y. Diagnostic value of peritumoral minimum apparent diffusion coefficient for differentiation of glioblastoma multiforme from solitary metastatic lesions. AJR Am. J. Roentgenol. 2011, 196, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Muto, M.; Frauenfelder, G.; Senese, R.; Zeccolini, F.; Schena, E.; Giurazza, F.; Jäger, H.R. Dynamic susceptibility contrast (DSC) perfusion MRI in differential diagnosis between radionecrosis and neoangiogenesis in cerebral metastases using rCBV, rCBF and K2. Radiol. Med. 2018, 123, 545–552. [Google Scholar] [CrossRef]
- Chu, H.H.; Choi, S.H.; Ryoo, I.; Kim, S.C.; Yeom, J.A.; Shin, H.; Jung, S.C.; Lee, A.L.; Yoon, T.J.; Kim, T.M.; et al. Differentiation of true progression from pseudoprogression in glioblastoma treated with radiation therapy and concomitant temozolomide: Comparison study of standard and high-b-value diffusion-weighted imaging. Radiology 2013, 269, 831–840. [Google Scholar] [CrossRef]
- Srinivasan, A.; Dvorak, R.; Perni, K.; Rohrer, S.; Mukherji, S.K. Differentiation of benign and malignant pathology in the head and neck using 3T apparent diffusion coefficient values: Early experience. AJNR Am. J. Neuroradiol. 2008, 29, 40–44. [Google Scholar] [CrossRef]
- Sakamoto, J.; Yoshino, N.; Okochi, K.; Imaizumi, A.; Tetsumura, A.; Kurohara, K.; Kurabayashi, T. Tissue characterization of head and neck lesions using diffusion-weighted MR imaging with SPLICE. Eur. J. Radiol. 2009, 69, 260–268. [Google Scholar] [CrossRef]
- Habermann, C.R.; Gossrau, P.; Graessner, J.; Arndt, C.; Cramer, M.C.; Reitmeier, F.; Jaehne, M.; Adam, G. Diffusion-weighted echo-planar MRI: A valuable tool for differentiating primary parotid gland tumors? RöFo 2005, 177, 940–945. [Google Scholar] [CrossRef]
- Abdel Razek, A.A.K.; Soliman, N.Y.; Elkhamary, S.; Alsharaway, M.K.; Tawfik, A. Role of diffusion-weighted MR imaging in cervical lymphadenopathy. Eur. Radiol. 2006, 16, 1468–1477. [Google Scholar] [CrossRef] [PubMed]
- Payabvash, S.M.D. Quantitative diffusion magnetic resonance imaging in head and neck tumors. Quant. Imaging Med. Surg. 2018, 8, 1052–1065. [Google Scholar] [CrossRef] [PubMed]
- Meyer, H.J.; Leifels, L.; Hamerla, G.; Höhn, A.K.; Surov, A. ADC-histogram analysis in head and neck squamous cell carcinoma. Associations with different histopathological features including expression of EGFR, VEGF, HIF-1α, Her 2 and p53. A preliminary study. Magn. Reson. Imaging 2018, 54, 214–217. [Google Scholar] [CrossRef] [PubMed]
- King, A.D.; Chow, K.-K.; Yu, K.-H.; Mo, F.K.F.; Yeung, D.K.W.; Yuan, J.; Bhatia, K.S.; Vlantis, A.C.; Ahuja, A.T. Head and neck squamous cell carcinoma: Diagnostic performance of diffusion-weighted MR imaging for the prediction of treatment response. Radiology 2013, 266, 531–538. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; La Grutta, L.; Grassedonio, E.; Patti, C.; Lagalla, R.; Midiri, M.; Galia, M. Pitfalls in whole body MRI with diffusion weighted imaging performed on patients with lymphoma: What radiologists should know. Magn. Reson. Imaging 2016, 34, 922–931. [Google Scholar] [CrossRef]
- Swerkersson, S.; Grundberg, O.; Kölbeck, K.; Carlberg, A.; Nyrén, S.; Skorpil, M. Optimizing diffusion-weighted magnetic resonance imaging for evaluation of lung tumors: A comparison of respiratory triggered and free breathing techniques. Eur. J. Radiol. Open 2018, 5, 189–193. [Google Scholar] [CrossRef]
- Mori, T.; Nomori, H.; Ikeda, K.; Kawanaka, K.; Shiraishi, S.; Katahira, K.; Yamashita, Y. Diffusion-weighted magnetic resonance imaging for diagnosing malignant pulmonary nodules/masses: Comparison with positron emission tomography. J. Thorac. Oncol. 2008, 3, 358–364. [Google Scholar] [CrossRef]
- Cakir, C.; Genchellac, H.; Temizoz, O.; Polat, A.; Sengul, E.; Duygulu, G. Diffusion Weighted Magnetic Resonance Imaging for the Characterization of Solitary Pulmonary Lesions. Balkan. Med. J. 2015, 32, 403–409. [Google Scholar] [CrossRef]
- Karaman, A.; Durur-Subasi, I.; Alper, F.; Durur-Karakaya, A.; Subasi, M.; Akgun, M. Is it better to include necrosis in apparent diffusion coefficient (ADC) measurements? The necrosis/wall ADC ratio to differentiate malignant and benign necrotic lung lesions: Preliminary results. J. Magn. Reson. Imaging 2017, 46, 1001–1006. [Google Scholar] [CrossRef]
- Yang, R.-M.; Li, L.; Wei, X.-H.; Guo, Y.-M.; Huang, Y.-H.; Lai, L.-S.; Chen, A.-M.; Liu, G.-S.; Xiong, W.-F.; Luo, L.-P.; et al. Differentiation of Central Lung Cancer from Atelectasis: Comparison of Diffusion-Weighted MRI with PET/CT. PLoS ONE 2013, 8, e60279. [Google Scholar] [CrossRef]
- Usuda, K.; Iwai, S.; Funasaki, A.; Sekimura, A.; Motono, N.; Matoba, M.; Doai, M.; Yamada, S.; Ueda, Y.; Uramoto, H. Diffusion-weighted magnetic resonance imaging is useful for the response evaluation of chemotherapy and/or radiotherapy to recurrent lesions of lung cancer. Transl. Oncol. 2019, 12, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Coolen, J.; De Keyzer, F.; Nafteux, P.; De Wever, W.; Dooms, C.; Vansteenkiste, J.; Derweduwen, A.; Roebben, I.; Verbeken, E.; De Leyn, P.; et al. Malignant pleural mesothelioma: Visual assessment by using pleural pointillism at diffusion-weighted MR imaging. Radiology 2015, 274, 576–584. [Google Scholar] [CrossRef] [PubMed]
- Sardanelli, F.; Carbonaro, L.A.; Montemezzi, S.; Cavedon, C.; Trimboli, R.M. Clinical Breast MR Using MRS or DWI: Who Is the Winner? Front. Oncol. 2016, 6, 217. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Tang, M.; Min, Z.; Lu, J.; Lei, X.; Zhang, X. Accuracy of combined dynamic contrast-enhanced magnetic resonance imaging and diffusion-weighted imaging for breast cancer detection: A meta-analysis. Acta Radiol. 2016, 57, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.Y.; Chang, Y.-W.; Park, H.J.; Kim, H.J.; Hong, S.S.; Seo, D.Y. Correlation of the apparent diffusion coefficiency values on diffusion-weighted imaging with prognostic factors for breast cancer. Br. J. Radiol. 2012, 85, e474–e479. [Google Scholar] [CrossRef] [PubMed]
- Durur-Subasi, I. DW-MRI of the breast: A pictorial review. Insights Imaging 2019, 10, 6. [Google Scholar] [CrossRef]
- Baltzer, P.; Mann, R.M.; Iima, M.; Sigmund, E.E.; Clauser, P.; Gilbert, F.J.; Martincich, L.; Partridge, S.C.; Patterson, A.; Pinker, K.; et al. Diffusion-weighted imaging of the breast-a consensus and mission statement from the EUSOBI International Breast Diffusion-Weighted Imaging working group. Eur. Radiol. 2020, 30, 1436–1450. [Google Scholar] [CrossRef]
- Song, S.E.; Park, E.K.; Cho, K.R.; Seo, B.K.; Woo, O.H.; Jung, S.P.; Cho, S.B. Additional value of diffusion-weighted imaging to evaluate multifocal and multicentric breast cancer detected using pre-operative breast MRI. Eur. Radiol. 2017, 27, 4819–4827. [Google Scholar] [CrossRef]
- Aydin, H.; Guner, B.; Esen Bostanci, I.; Bulut, Z.M.; Aribas, B.K.; Dogan, L.; Gulcelik, M.A. Is there any relationship between adc values of diffusion-weighted imaging and the histopathological prognostic factors of invasive ductal carcinoma? Br. J. Radiol. 2018, 91, 20170705. [Google Scholar] [CrossRef]
- Parikh, T.; Drew, S.J.; Lee, V.S.; Wong, S.; Hecht, E.M.; Babb, J.S.; Taouli, B. Focal Liver Lesion Detection and Characterization with Diffusion-weighted MR Imaging: Comparison with Standard Breath-hold T2-weighted Imaging. Radiology 2008, 246, 812–822. [Google Scholar] [CrossRef]
- Lestra, T.; Kanagaratnam, L.; Mulé, S.; Janvier, A.; Brixi, H.; Cadiot, G.; Dohan, A.; Hoeffel, C. Measurement variability of liver metastases from neuroendocrine tumors on different magnetic resonance imaging sequences. Diagn. Interv. Imaging 2018, 99, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.H.; Hammond, N.; Siddiqi, A.J.; Shroff, S.; Khatri, G.; Wang, Y.; Merrick, L.B.; Nikolaidis, P. Utility of diffusion-weighted MRI in distinguishing benign and malignant hepatic lesions. J. Magn. Reson. Imaging 2010, 32, 138–147. [Google Scholar] [CrossRef]
- Zech, C.J.; Reiser, M.F.; Herrmann, K.A. Imaging of Hepatocellular Carcinoma by Computed Tomography and Magnetic Resonance Imaging: State of the Art. Dig. Dis. 2009, 27, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Moriya, T.; Saito, K.; Tajima, Y.; Harada, T.L.; Araki, Y.; Sugimoto, K.; Tokuuye, K. 3D analysis of apparent diffusion coefficient histograms in hepatocellular carcinoma: Correlation with histological grade. Cancer Imaging 2017, 17, 1. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kim, Y.K.; Lee, W.J.; Park, M.J.; Kim, S.H.; Rhim, H.; Choi, D. Hypovascular Hypointense Nodules on Hepatobiliary Phase Gadoxetic Acid–enhanced MR Images in Patients with Cirrhosis: Potential of DW Imaging in Predicting Progression to Hypervascular HCC. Radiology 2012, 265, 104–114. [Google Scholar] [CrossRef]
- Min, J.H.; Kim, Y.K.; Choi, S.Y.; Jeong, W.K.; Lee, W.J.; Ha, S.Y.; Ahn, S.; Ahn, H.S. Differentiation between cholangiocarcinoma and hepatocellular carcinoma with target sign on diffusion-weighted imaging and hepatobiliary phase gadoxetic acid-enhanced MR imaging: Classification tree analysis applying capsule and septum. Eur. J. Radiol. 2017, 92, 1–10. [Google Scholar] [CrossRef] [PubMed]
- You, M.W.; Yun, S.J. Diagnostic performance of diffusion-weighted imaging for differentiating benign and malignant gallbladder lesions: A systematic review and meta-analysis. J. Magn. Reson. Imaging 2018, 48, 1375–1388. [Google Scholar] [CrossRef]
- Koh, D.M.; Scurr, E.; Collins, D.; Kanber, B.; Norman, A.; Leach, M.O.; Husband, J.E. Predicting response of colorectal hepatic metastasis: Value of pretreatment apparent diffusion coefficients. AJR Am. J. Roentgenol. 2007, 188, 1001–1008. [Google Scholar] [CrossRef]
- Schraml, C.; Schwenzer, N.F.; Clasen, S.; Rempp, H.-J.; Martirosian, P.; Claussen, C.D.; Pereira, P.L. Navigator respiratory-triggered diffusion-weighted imaging in the follow-up after hepatic radiofrequency ablation-initial results. J. Magn. Reson. Imaging 2009, 29, 1308–1316. [Google Scholar] [CrossRef]
- Balci, N.C.; Perman, W.H.; Saglam, S.; Akisik, F.; Fattahi, R.; Bilgin, M. Diffusion-Weighted Magnetic Resonance Imaging of the Pancreas. Top. Magn. Reson. Imaging 2009, 20, 43–47. [Google Scholar] [CrossRef]
- De Robertis, R.; Tinazzi Martini, P.; Demozzi, E.; Dal Corso, F.; Bassi, C.; Pederzoli, P.; D’Onofrio, M. Diffusion-weighted imaging of pancreatic cancer. World J. Radiol. 2015, 7, 319–328. [Google Scholar] [CrossRef] [PubMed]
- Kartalis, N.; Lindholm, T.L.; Aspelin, P.; Permert, J.; Albiin, N. Diffusion-weighted magnetic resonance imaging of pancreas tumours. Eur. Radiol. 2009, 19, 1981–1990. [Google Scholar] [CrossRef] [PubMed]
- Zong, R.L.; Geng, L.; Wang, X.; Xie, D. Diagnostic Performance of Apparent Diffusion Coefficient for Prediction of Grading of Pancreatic Neuroendocrine Tumors: A Systematic Review and Meta-analysis. Pancreas 2019, 48, 151–160. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Wang, Y.; Tang, W.; Jiang, M.; Li, K.; Tao, X. Multiparametric MR imaging detects therapy efficacy of radioactive seeds brachytherapy in pancreatic ductal adenocarcinoma xenografts. Radiol. Med. 2018, 123, 481–488. [Google Scholar] [CrossRef]
- Giganti, F.; Ambrosi, A.; Petrone, M.C.; Canevari, C.; Chiari, D.; Salerno, A.; Arcidiacono, P.G.; Nicoletti, R.; Albarello, L.; Mazza, E.; et al. Prospective comparison of MR with diffusion-weighted imaging, endoscopic ultrasound, MDCT and positron emission tomography-CT in the pre-operative staging of oesophageal cancer: Results from a pilot study. Br. J. Radiol. 2016, 89, 20160087. [Google Scholar] [CrossRef]
- Onal, Y.; Samanci, C. The Role of Diffusion-weighted Imaging in Patients with Gastric Wall Thickening. Curr. Med. Imaging Rev. 2018, 15, 965–971. [Google Scholar] [CrossRef]
- Giganti, F.; Orsenigo, E.; Esposito, A.; Chiari, D.; Salerno, A.; Ambrosi, A.; Albarello, L.; Mazza, E.; Staudacher, C.; Del Maschio, A.; et al. Prognostic role of diffusion-weighted MR imaging for resectable gastric cancer. Radiology 2015, 276, 444–452. [Google Scholar] [CrossRef]
- Cai, J.S.; Chen, H.Y.; Chen, J.Y.; Lu, Y.F.; Sun, J.Z.; Zhou, Y.; Yu, R.S. Reduced field-of-view diffusion-weighted imaging (DWI) in patients with gastric cancer: Comparison with conventional DWI techniques at 3.0T: A preliminary study. Medicine 2020, 99, e18616. [Google Scholar] [CrossRef]
- Luo, M.; Song, H.; Liu, G.; Lin, Y.; Luo, L.; Zhou, X.; Chen, B. Comparison of DWI and 18F-FDG PET/CT for assessing preoperative N-staging in gastric cancer: Evidence from a meta-analysis. Oncotarget 2017, 8, 84473–84488. [Google Scholar] [CrossRef]
- Dam, C.; Lindebjerg, J.; Jakobsen, A.; Jensen, L.H.; Rahr, H.; Rafaelsen, S.R. Local staging of sigmoid colon cancer using MRI. Acta Radiol. Open 2017, 6, 205846011772095. [Google Scholar] [CrossRef]
- Nerad, E.; Lambregts, D.M.J.; Kersten, E.L.J.; Maas, M.; Bakers, F.C.H.; van den Bosch, H.C.M.; Grabsch, H.I.; Beets-Tan, R.G.H.; Lahaye, M.J. MRI for Local Staging of Colon Cancer: Can MRI Become the Optimal Staging Modality for Patients With Colon Cancer? Dis. Colon Rectum 2017, 60, 385–392. [Google Scholar] [CrossRef]
- Dresen, R.C.; De Vuysere, S.; De Keyzer, F.; Van Cutsem, E.; Prenen, H.; Vanslembrouck, R.; De Hertogh, G.; Wolthuis, A.; D’Hoore, A.; Vandecaveye, V. Whole-body diffusion-weighted MRI for operability assessment in patients with colorectal cancer and peritoneal metastases. Cancer Imaging 2019, 19, 1. [Google Scholar] [CrossRef]
- Fornell-Perez, R.; Perez-Alonso, E.; Porcel-de-Peralta, G.; Duran-Castellon, A.; Vivas-Escalona, V.; Aranda-Sanchez, J.; Gonzalez-Dominguez, M.C.; Rubio-Garcia, J.; Aleman-Flores, P.; Lozano-Rodriguez, A.; et al. Primary and post-chemoradiotherapy staging using MRI in rectal cancer: The role of diffusion imaging in the assessment of perirectal infiltration. Abdom. Radiol. 2019, 44, 3674–3682. [Google Scholar] [CrossRef]
- Beets-Tan, R.G.H.; Lambregts, D.M.J.; Maas, M.; Bipat, S.; Barbaro, B.; Curvo-Semedo, L.; Fenlon, H.M.; Gollub, M.J.; Gourtsoyianni, S.; Halligan, S.; et al. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur. Radiol. 2018, 28, 1465–1475. [Google Scholar] [CrossRef] [PubMed]
- van der Paardt, M.P.; Zagers, M.B.; Beets-Tan, R.G.H.; Stoker, J.; Bipat, S. Patients who undergo preoperative chemoradiotherapy for locally advanced rectal cancer restaged by using diagnostic MR imaging: A systematic review and meta-analysis. Radiology 2013, 269, 101–112. [Google Scholar] [CrossRef] [PubMed]
- Maas, M.; Lambregts, D.M.J.; Nelemans, P.J.; Heijnen, L.A.; Martens, M.H.; Leijtens, J.W.A.; Sosef, M.; Hulsewé, K.W.E.; Hoff, C.; Breukink, S.O.; et al. Assessment of Clinical Complete Response After Chemoradiation for Rectal Cancer with Digital Rectal Examination, Endoscopy, and MRI: Selection for Organ-Saving Treatment. Ann. Surg. Oncol. 2015, 22, 3873–3880. [Google Scholar] [CrossRef] [PubMed]
- Dhanda, S.; Thakur, M.; Kerkar, R.; Jagmohan, P. Diffusion-weighted imaging of gynecologic tumors: Diagnostic pearls and potential pitfalls. Radiographics 2014, 34, 1393–1416. [Google Scholar] [CrossRef] [PubMed]
- Woo, S.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Apparent diffusion coefficient for prediction of parametrial invasion in cervical cancer: A critical evaluation based on stratification to a Likert scale using T2-weighted imaging. Radiol. Med. 2018, 123, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Addley, H.; Moyle, P.; Freeman, S. Diffusion-weighted imaging in gynaecological malignancy. Clin. Radiol. 2017, 72, 981–990. [Google Scholar] [CrossRef]
- Thomassin-Naggara, I.; Toussaint, I.; Perrot, N.; Rouzier, R.; Cuenod, C.A.; Bazot, M.; Daraï, E. Characterization of complex adnexal masses: Value of adding perfusion- and diffusion-weighted MR imaging to conventional MR imaging. Radiology 2011, 258, 793–803. [Google Scholar] [CrossRef]
- Motoshima, S.; Irie, H.; Nakazono, T.; Kamura, T.; Kudo, S. Diffusion-weighted MR imaging in gynecologic cancers. J. Gynecol. Oncol. 2011, 22, 275–287. [Google Scholar] [CrossRef] [PubMed]
- Thomassin-Naggara, I.; Daraï, E.; Cuenod, C.A.; Fournier, L.; Toussaint, I.; Marsault, C.; Bazot, M. Contribution of diffusion-weighted MR imaging for predicting benignity of complex adnexal masses. Eur. Radiol. 2009, 19, 1544–1552. [Google Scholar] [CrossRef] [PubMed]
- Galia, M.; Albano, D.; Bruno, A.; Agrusa, A.; Romano, G.; Di Buono, G.; Agnello, F.; Salvaggio, G.; La Grutta, L.; Midiri, M.; et al. Imaging features of solid renal masses. Br. J. Radiol. 2017, 90, 20170077. [Google Scholar] [CrossRef] [PubMed]
- Inci, E.; Hocaoglu, E.; Aydin, S.; Cimilli, T. Diffusion-weighted magnetic resonance imaging in evaluation of primary solid and cystic renal masses using the Bosniak classification. Eur. J. Radiol. 2012, 81, 815–820. [Google Scholar] [CrossRef]
- Kang, S.K.; Zhang, A.; Pandharipande, P.V.; Chandarana, H.; Braithwaite, R.S.; Littenberg, B. DWI for Renal Mass Characterization: Systematic Review and Meta-Analysis of Diagnostic Test Performance. AJR Am. J. Roentgenol. 2015, 205, 317–324. [Google Scholar] [CrossRef]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H. Diagnostic Performance of DWI for Differentiating High- From Low-Grade Clear Cell Renal Cell Carcinoma: A Systematic Review and Meta-Analysis. AJR Am. J. Roentgenol. 2017, 209, W374–W381. [Google Scholar] [CrossRef]
- Ding, Y.; Tan, Q.; Mao, W.; Dai, C.; Hu, X.; Hou, J.; Zeng, M.; Zhou, J. Differentiating between malignant and benign renal tumors: Do IVIM and diffusion kurtosis imaging perform better than DWI? Eur. Radiol. 2019, 29, 6930–6939. [Google Scholar] [CrossRef]
- Aslan, M.; Aslan, A.; Arıöz Habibi, H.; Kalyoncu Uçar, A.; Özmen, E.; Bakan, S.; Kuruğoğlu, S.; Adaletli, İ. Diffusion-weighted MRI for differentiating Wilms tumor from neuroblastoma. Diagn. Interv. Radiol. 2017, 23, 403–406. [Google Scholar] [CrossRef]
- Goyal, A.; Razik, A.; Kandasamy, D.; Seth, A.; Das, P.; Ganeshan, B.; Sharma, R. Role of MR texture analysis in histological subtyping and grading of renal cell carcinoma: A preliminary study. Abdom. Radiol. 2019, 44, 3336–3349. [Google Scholar] [CrossRef]
- Takeuchi, M.; Sasaki, S.; Ito, M.; Okada, S.; Takahashi, S.; Kawai, T.; Suzuki, K.; Oshima, H.; Hara, M.; Shibamoto, Y. Urinary Bladder Cancer: Diffusion-weighted MR Imaging—Accuracy for Diagnosing T Stage and Estimating Histologic Grade. Radiology 2009, 251, 112–121. [Google Scholar] [CrossRef]
- Wang, H.; Pui, M.H.; Guo, Y.; Li, S.; Guan, J.; Zhang, X.; Cai, H. Multiparametric 3-T MRI for differentiating low-versus high-grade and category T1 versus T2 bladder urothelial carcinoma. AJR Am. J. Roentgenol. 2015, 204, 330–334. [Google Scholar] [CrossRef]
- Thoeny, H.C.; Froehlich, J.M.; Triantafyllou, M.; Huesler, J.; Bains, L.J.; Vermathen, P.; Fleischmann, A.; Studer, U.E. Metastases in normal-sized pelvic lymph nodes: Detection with diffusion-weighted MR imaging. Radiology 2014, 273, 125–135. [Google Scholar] [CrossRef] [PubMed]
- Wu, G.Y.; Lu, Q.; Wu, L.M.; WenKong; Chen, X.X.; Xu, J.R. Imaging of upper urinary tract cancer: Using conventional MRI and diffusion-weighted MRI with different b values. Acta Radiol. 2014, 55, 882–889. [Google Scholar] [CrossRef]
- Roy, C.; Labani, A.; Alemann, G.; Bierry, G.; Lang, H.; Ohana, M. DWI in the etiologic diagnosis of excretory upper urinary tract lesions: Can it help in differentiating benign from malignant tumors? A retrospective study of 98 patients. Am. J. Roentgenol. 2016, 207, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Galia, M.; Albano, D.; Narese, D.; Patti, C.; Chianca, V.; Di Pietto, F.; Mulè, A.; Grassedonio, E.; La Grutta, L.; Lagalla, R.; et al. Whole-body MRI in patients with lymphoma: Collateral findings. Radiol. Med. 2016, 121, 793–800. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Agnello, F.; Midiri, F.; Pecoraro, G.; Bruno, A.; Alongi, P.; Toia, P.; Di Buono, G.; Agrusa, A.; Sconfienza, L.M.; et al. Imaging features of adrenal masses. Insights Imaging 2019, 10, 1. [Google Scholar] [CrossRef] [PubMed]
- Miller, F.H.; Wang, Y.; McCarthy, R.J.; Yaghmai, V.; Merrick, L.; Larson, A.; Berggruen, S.; Casalino, D.D.; Nikolaidis, P. Utility of Diffusion-Weighted MRI in Characterization of Adrenal Lesions. AJR Am. J. Roentgenol. 2010, 194, W179–W185. [Google Scholar] [CrossRef]
- Sandrasegaran, K.; Patel, A.A.; Ramaswamy, R.; Samuel, V.P.; Northcutt, B.G.; Frank, M.S.; Francis, I.R. Characterization of adrenal masses with diffusion-weighted imaging. AJR Am. J. Roentgenol. 2011, 197, 132–138. [Google Scholar] [CrossRef]
- Dong, Y.; Liu, Q. Differentiation of malignant from benign pheochromocytomas with diffusion-weighted and dynamic contrast-enhanced magnetic resonance at 3.0 T. J. Comput. Assist. Tomogr. 2012, 36, 361–366. [Google Scholar] [CrossRef]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef]
- Beyhan, M.; Sade, R.; Koc, E.; Adanur, S.; Kantarci, M. The evaluation of prostate lesions with IVIM DWI and MR perfusion parameters at 3T MRI. Radiol. Med. 2019, 124, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Surov, A.; Meyer, H.J.; Wienke, A. Correlations between Apparent Diffusion Coefficient and Gleason Score in Prostate Cancer: A Systematic Review. Eur. Urol. Oncol. 2019, S2588-9311(18)30214-1. [Google Scholar] [CrossRef] [PubMed]
- Manetta, R.; Palumbo, P.; Gianneramo, C.; Bruno, F.; Arrigoni, F.; Natella, R.; Maggialetti, N.; Agostini, A.; Giovagnoni, A.; Di Cesare, E.; et al. Correlation between ADC values and Gleason score in evaluation of prostate cancer: Multicentre experience and review of the literature. Gland. Surg. 2019, 8, S216–S222. [Google Scholar] [CrossRef]
- Woo, S.; Suh, C.H.; Kim, S.Y.; Cho, J.Y.; Kim, S.H.; Moon, M.H. Head-to-Head Comparison Between Biparametric and Multiparametric MRI for the Diagnosis of Prostate Cancer: A Systematic Review and Meta-Analysis. AJR Am. J. Roentgenol. 2018, 211, W226–W241. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Xu, M.; Fang, M.; Yu, X.; Zou, J.; Yang, S.; Wang, Y.; Fang, X.; He, B.; Tian, J.; et al. Noninvasive Prediction of High-Grade Prostate Cancer via Biparametric MRI Radiomics. J. Magn. Reson. Imaging 2020. [Google Scholar] [CrossRef]
- Stéphane, V.; Samuel, B.; Vincent, D.; Joelle, G.; Remy, P.; Francois, G.G.; Jean-Pierre, T. Comparison of PET-CT and magnetic resonance diffusion weighted imaging with body suppression (DWIBS) for initial staging of malignant lymphomas. Eur. J. Radiol. 2013, 82, 2011–2017. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Patti, C.; La Grutta, L.; Agnello, F.; Grassedonio, E.; Mulè, A.; Cannizzaro, G.; Ficola, U.; Lagalla, R.; Midiri, M.; et al. Comparison between whole-body MRI with diffusion-weighted imaging and PET/CT in staging newly diagnosed FDG-avid lymphomas. Eur. J. Radiol. 2016, 85, 313–318. [Google Scholar] [CrossRef]
- Balbo-Mussetto, A.; Cirillo, S.; Bruna, R.; Gueli, A.; Saviolo, C.; Petracchini, M.; Fornari, A.; Lario, C.V.; Gottardi, D.; De Crescenzo, A.; et al. Whole-body MRI with diffusion-weighted imaging: A valuable alternative to contrast-enhanced CT for initial staging of aggressive lymphoma. Clin. Radiol. 2016, 71, 271–279. [Google Scholar] [CrossRef]
- Fitzpatrick, J.J.; Ryan, M.A.; Bruzzi, J.F. Diagnostic accuracy of diffusion-weighted imaging- magnetic resonance imaging compared to positron emission tomography/computed tomography in evaluating and assessing pathological response to treatment in adult patients with lymphoma: A systematic review. J. Med. Imaging Radiat. Oncol. 2018, 62, 530–539. [Google Scholar] [CrossRef]
- Jang, K.M.; Kim, S.H.; Hwang, J.; Lee, S.J.; Kang, T.W.; Lee, M.W.; Choi, D. Differentiation of malignant from benign focal splenic lesions: Added value of diffusion-weighted MRI. AJR Am. J. Roentgenol. 2014, 203, 803–812. [Google Scholar] [CrossRef]
- Littooij, A.S.; Kwee, T.C.; Barber, I.; Granata, C.; de Keizer, B.; Beek, F.J.; Hobbelink, M.G.; Fijnheer, R.; Stoker, J.; Nievelstein, R.A. Accuracy of whole-body MRI in the assessment of splenic involvement in lymphoma. Acta Radiol. 2016, 57, 142–151. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Messina, C.; Gitto, S.; Papakonstantinou, O.; Sconfienza, L.M. Differential Diagnosis of Spine Tumors: My Favorite Mistake. Semin. Musculoskelet. Radiol. 2019, 23, 26–35. [Google Scholar] [CrossRef] [PubMed]
- Fukuda, T.; Wengler, K.; de Carvalho, R.; Boonsri, P.; Schweitzer, M.E. MRI biomarkers in osseous tumors. J. Magn. Reson. Imaging 2019, 50, 702–718. [Google Scholar] [CrossRef] [PubMed]
- Nonomura, Y.; Yasumoto, M.; Yoshimura, R.; Haraguchi, K.; Ito, S.; Akashi, T.; Ohashi, I. Relationship between bone marrow cellularity and apparent diffusion coefficient. J. Magn. Reson. Imaging 2001, 13, 757–760. [Google Scholar] [CrossRef]
- Wang, T.; Wu, X.; Cui, Y.; Chu, C.; Ren, G.; Li, W. Role of apparent diffusion coefficients with diffusion-weighted magnetic resonance imaging in differentiating between benign and malignant bone tumors. World J. Surg. Oncol. 2014, 12, 365. [Google Scholar] [CrossRef]
- Wang, J.; Sun, M.; Liu, D.; Hu, X.; Pui, M.H.; Meng, Q.; Gao, Z. Correlation between apparent diffusion coefficient and histopathology subtypes of osteosarcoma after neoadjuvant chemotherapy. Acta Radiol. 2017, 58, 971–976. [Google Scholar] [CrossRef]
- Douis, H.; Jeys, L.; Grimer, R.; Vaiyapuri, S.; Davies, A.M. Is there a role for diffusion-weighted MRI (DWI) in the diagnosis of central cartilage tumors? Skeletal Radiol. 2015, 44, 963–969. [Google Scholar] [CrossRef]
- Pozzi, G.; Albano, D.; Messina, C.; Angileri, S.A.; Al-Mnayyis, A.; Galbusera, F.; Luzzati, A.; Perrucchini, G.; Scotto, G.; Parafioriti, A.; et al. Solid bone tumors of the spine: Diagnostic performance of apparent diffusion coefficient measured using diffusion-weighted MRI using histology as a reference standard. J. Magn. Reson. Imaging 2018, 47, 1034–1042. [Google Scholar] [CrossRef]
- Luo, Z.; Litao, L.; Gu, S.; Luo, X.; Li, D.; Yu, L.; Ma, Y. Standard-b-value vs. low-b-value DWI for differentiation of benign and malignant vertebral fractures: A meta-analysis. Br. J. Radiol. 2016, 89, 20150384. [Google Scholar] [CrossRef]
- Wang, C.-S.; Du, L.-J.; Si, M.-J.; Yin, Q.-H.; Chen, L.; Shu, M.; Yuan, F.; Fei, X.-C.; Ding, X.-Y. Noninvasive assessment of response to neoadjuvant chemotherapy in osteosarcoma of long bones with diffusion-weighted imaging: An initial in vivo study. PLoS ONE 2013, 8, e72679. [Google Scholar] [CrossRef]
- Perez-Lopez, R.; Mateo, J.; Mossop, H.; Blackledge, M.D.; Collins, D.J.; Rata, M.; Morgan, V.A.; Macdonald, A.; Sandhu, S.; Lorente, D.; et al. Diffusion-weighted Imaging as a Treatment Response Biomarker for Evaluating Bone Metastases in Prostate Cancer: A Pilot Study. Radiology 2017, 283, 168–177. [Google Scholar] [CrossRef] [PubMed]
- Petralia, G.; Padhani, A.R.; Pricolo, P.; Zugni, F.; Martinetti, M.; Summers, P.E.; Bellomi, M.; Grazioli, L.; Colagrande, S.; Giovagnoni, A.; et al. Whole-body magnetic resonance imaging (WB-MRI) in oncology: Recommendations and key uses. Radiol. Med. 2019, 124, 218–233. [Google Scholar] [CrossRef] [PubMed]
- Vilanova, J.C.; Baleato-Gonzalez, S.; Romero, M.J.; Carrascoso-Arranz, J.; Luna, A. Assessment of Musculoskeletal Malignancies with Functional MR Imaging. Magn. Reson. Imaging Clin. N. Am. 2016, 24, 239–259. [Google Scholar] [CrossRef] [PubMed]
- Robba, T.; Chianca, V.; Albano, D.; Clementi, V.; Piana, R.; Linari, A.; Comandone, A.; Regis, G.; Stratta, M.; Faletti, C.; et al. Diffusion-weighted imaging for the cellularity assessment and matrix characterization of soft tissue tumour. Radiol. Med. 2017, 122, 871–879. [Google Scholar] [CrossRef]
- Subhawong, T.K.; Jacobs, M.A.; Fayad, L.M. Insights Into Quantitative Diffusion-Weighted MRI for Musculoskeletal Tumor Imaging. AJR Am. J. Roentgenol. 2014, 203, 560–572. [Google Scholar] [CrossRef]
- Yao, K.; Troupis, J.M. Diffusion-weighted imaging and the skeletal system: A literature review. Clin. Radiol. 2016, 71, 1071–1082. [Google Scholar] [CrossRef]
- Choi, Y.J.; Lee, I.S.; Song, Y.S.; Il Kim, J.; Choi, K.-U.; Song, J.W. Diagnostic performance of diffusion-weighted (DWI) and dynamic contrast-enhanced (DCE) MRI for the differentiation of benign from malignant soft-tissue tumors. J. Magn. Reson. Imaging 2019, 50, 798–809. [Google Scholar] [CrossRef]
- Bruno, F.; Arrigoni, F.; Mariani, S.; Splendiani, A.; Di Cesare, E.; Masciocchi, C.; Barile, A. Advanced magnetic resonance imaging (MRI) of soft tissue tumors: Techniques and applications. Radiol. Med. 2019, 124, 243–252. [Google Scholar] [CrossRef]
- Oka, K.; Yakushiji, T.; Sato, H.; Yorimitsu, S.; Hayashida, Y.; Yamashita, Y.; Mizuta, H. Ability of diffusion-weighted imaging for the differential diagnosis between chronic expanding hematomas and malignant soft tissue tumors. J. Magn. Reson. Imaging 2008, 28, 1195–1200. [Google Scholar] [CrossRef]
- Soldatos, T.; Ahlawat, S.; Montgomery, E.; Chalian, M.; Jacobs, M.A.; Fayad, L.M. Multiparametric Assessment of Treatment Response in High-Grade Soft-Tissue Sarcomas with Anatomic and Functional MR Imaging Sequences. Radiology 2016, 278, 831–840. [Google Scholar] [CrossRef]
- Del Grande, F.; Subhawong, T.; Weber, K.; Aro, M.; Mugera, C.; Fayad, L.M. Detection of Soft-Tissue Sarcoma Recurrence: Added Value of Functional MR Imaging Techniques at 3.0 T. Radiology 2014, 271, 499–511. [Google Scholar] [CrossRef] [PubMed]
- Il Kim, J.; Lee, I.S.; Song, Y.S.; Park, S.K.; Choi, K.-U.; Song, J.W. Short-term follow-up MRI after unplanned resection of malignant soft-tissue tumours; quantitative measurements on dynamic contrast enhanced and diffusion-weighted MR images. Br. J. Radiol. 2016, 89, 20160302. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Field | Study | Methodology | Findings |
|---|---|---|---|
| Neuroradiology | Yamasaki, F.; et al. Radiology. 2005 [3] | Retrospective; 275 patients with brain tumors; 1.5T MRI. | Mean ADC values are useful for differentiating brain tumors such DNT (2.546 × 10−3 mm2/s) and malignant lymphomas (0.725 × 10−3 mm2/s) versus glioblastomas (1.079 × 10−3 mm2/s) and metastatic tumors (1.149 × 10−3 mm2/s), and ependymomas (1.230 × 10−3 mm2/s) versus PNETs (1.079 × 10−3 mm2/s). |
| Head and Neck | Srinivasan, A.; et al. AJNR. Am. J. Neuroradiol, 2008 [8] | Retrospective; 33 patients (17 benign and 16 malignant lesions); 3.0T MRI. | Significant difference (p = 0.004) between mean ADC (10−3 mm2/s) of benign (1.505 ± 0.487) and malignant lesions (1.071 ± 0.293). Suggested threshold for differentiating benign vs. malignant = 1.3 × 10−3 mm2/s. |
| Chest | Cakir, C.; et al., Balkan. Med. J, 2015 [18] | Prospective; 48 solitary pulmonary nodules/masses (18 benign, 30 malignant); 1.5T MRI. | Mean ADC of malignant lesions (1.195 × 10−3 mm2/s) was significantly lower than that of benign lesions (2.02 × 10−3 mm2/s). ADC cut-off value of 1.5 × 10−3 mm2/s with sensitivity = 86.7% and specificity = 88.9% to differentiate benign from malignant lesions. |
| Breast | Choi, S.Y.; et al. Br. J. Radiol. 2012 [25] | Retrospective; 335 patients with IDC NOS and DCIS; 1.5T MRI. | Mean ADC of IDC NOS (0.907 ± 0.160 × 10−3 mm2/s) was significantly lower than that of DCIS (1.113 ± 0.231 × 10−3 mm2/s). Mean ADC of ER-positive cancers was significantly lower than in ER-negative. |
| Hepatobiliary | Miller, F.H.; et al. J. Magn. Reson. Imaging 2010 [32] | Retrospective; 542 focal liver lesions in 382 patients; 1.5T MRI. | Mean ADC (10−3 mm2/s) of hemangiomas = 2.26, FNH = 1.79, adenomas = 1.49, abscesses = 1.97, HCC = 1.53, and metastases = 1.50. Mean ADC of benign lesions = 2.50, malignant lesions = 1.52. Overlap reported between solid benign and malignant lesions. |
| Pancreas | Kartalis, N.; et al. Eur. Radiol. 2009 [42] | Retrospective; 36 patients with pancreatic lesions (12 malignant, 24 benign); 1.5T MRI. | DWI sensitivity = 92%, specificity = 97%, accuracy = 96%, PPV = 85%, NPV = 98%. Mean ADC (10−3 mm2/s) of malignant lesions (1.40 ± 0.30) was significantly lower than that of benign (2.57 ± 1.17). |
| Esophago-Gastro-Intestinal | Giganti, F.; et al. Radiology, 2015 [47] | Prospective study; 99 biopsy-proved gastric cancers; 1.5T MRI | ADC ≤ 1.5 × 10−3 mm2/s was associated with negative prognosis. Low ADC is a strong independent prognostic factor of the aggressiveness of gastric cancer. |
| Gynecological | Thomassin-Naggara, I. et al. Radiology. 2011 [60] | Retrospective; 87 women with complex adnexal masses (excluding endometriomas and cystic teratomas); 1.5T MRI. | High signal intensity within the solid component at b = 1000 s/mm was among the significant features predictive of malignancy. The use of DWI sequences (combined to perfusion) improved the accuracy to characterize complex adnexal masses |
| Urinary System and Adrenal | Ding, Y.; et al. Eur. Radiol. 2019 [67] | Retrospective; 180 patients with renal tumors (ccRCC, non-ccRCC, benign tumors); 1.5T MRI. | Mean ADC (10−3 mm2/s) of ccRCCs (1.78 ± 0.29) was significantly higher than that of non-RCC (1.31 ± 0.34) and benign renal tumors (1.35 ± 0.29). Non-ccRCCs and benign tumors had not significantly different ADC (p > 0.05). |
| Prostate | Woo, S.; et al. Am. J. Roentgenol. 2018 [84] | Meta-analysis including 20 studies (2242 patients with histologic-proven Prostate cancer); 1.5T and 3.0T MRI. | Biparametric MRI (T2-w and DWI) and multiparametric MRI (T2-w, DWI, and DCE) had not significantly different diagnostic performance (pooled sensitivity and specificity of 0.74 and 0.90 vs. 0.76 and 0.89, respectively). |
| Lymph Nodes and Spleen | Albano, D.; et al., Eur. J. Radiol. 2016 [87] | Prospective; 68 patients with FDG-avid lymphoma. Comparison between WB-MRI with DWI and FDG-PET/CT. 1.5T MRI. | Excellent agreement between WB-MRI and FDG-PET/CT stage (k = 0.88; p < 0.05); WB-MRI stage was equal to FDG-PET/CT stage in 91.2% (62/68; in particular, 35/37 Hodgkin lymphoma, 27/31 Non Hodgkin lymphoma). Sensitivity of WB-MRI for splenic involvement was 100%. |
| Bone Tumors | Wang, T.; et al. World J. Surg. Oncol. 2014 [96] | Retrospective; 187 patients; 3.0T MRI. | Mean ADC (×10−3 mm2/s) of benign tumors (1.17 ± 0.36) significantly higher than that of malignant (0.87 ± 0.20). |
| Soft Tissue Tumors | Choi, Y.J.; et al. J. Magn. Reson. Imaging 2019 [107] | Retrospective; 136 patients; 3.0T MRI. | Significant difference between mean ADC (×10−3 mm2/s) of benign (1.44 ± 0.46) and malignant (0.9 ± 0.40) soft tissue tumors. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Messina, C.; Bignone, R.; Bruno, A.; Bruno, A.; Bruno, F.; Calandri, M.; Caruso, D.; Coppolino, P.; De Robertis, R.; Gentili, F.; et al. Diffusion-Weighted Imaging in Oncology: An Update. Cancers 2020, 12, 1493. https://doi.org/10.3390/cancers12061493
Messina C, Bignone R, Bruno A, Bruno A, Bruno F, Calandri M, Caruso D, Coppolino P, De Robertis R, Gentili F, et al. Diffusion-Weighted Imaging in Oncology: An Update. Cancers. 2020; 12(6):1493. https://doi.org/10.3390/cancers12061493
Chicago/Turabian StyleMessina, Carmelo, Rodolfo Bignone, Alberto Bruno, Antonio Bruno, Federico Bruno, Marco Calandri, Damiano Caruso, Pietro Coppolino, Riccardo De Robertis, Francesco Gentili, and et al. 2020. "Diffusion-Weighted Imaging in Oncology: An Update" Cancers 12, no. 6: 1493. https://doi.org/10.3390/cancers12061493
APA StyleMessina, C., Bignone, R., Bruno, A., Bruno, A., Bruno, F., Calandri, M., Caruso, D., Coppolino, P., De Robertis, R., Gentili, F., Grazzini, I., Natella, R., Scalise, P., Barile, A., Grassi, R., Albano, D., & on behalf of the Young SIRM Working Group. (2020). Diffusion-Weighted Imaging in Oncology: An Update. Cancers, 12(6), 1493. https://doi.org/10.3390/cancers12061493