Breath Analysis for Early Detection of Malignant Pleural Mesothelioma: Volatile Organic Compounds (VOCs) Determination and Possible Biochemical Pathways

 ,
,  ,
,  , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Breath Sample Collection and Analysis
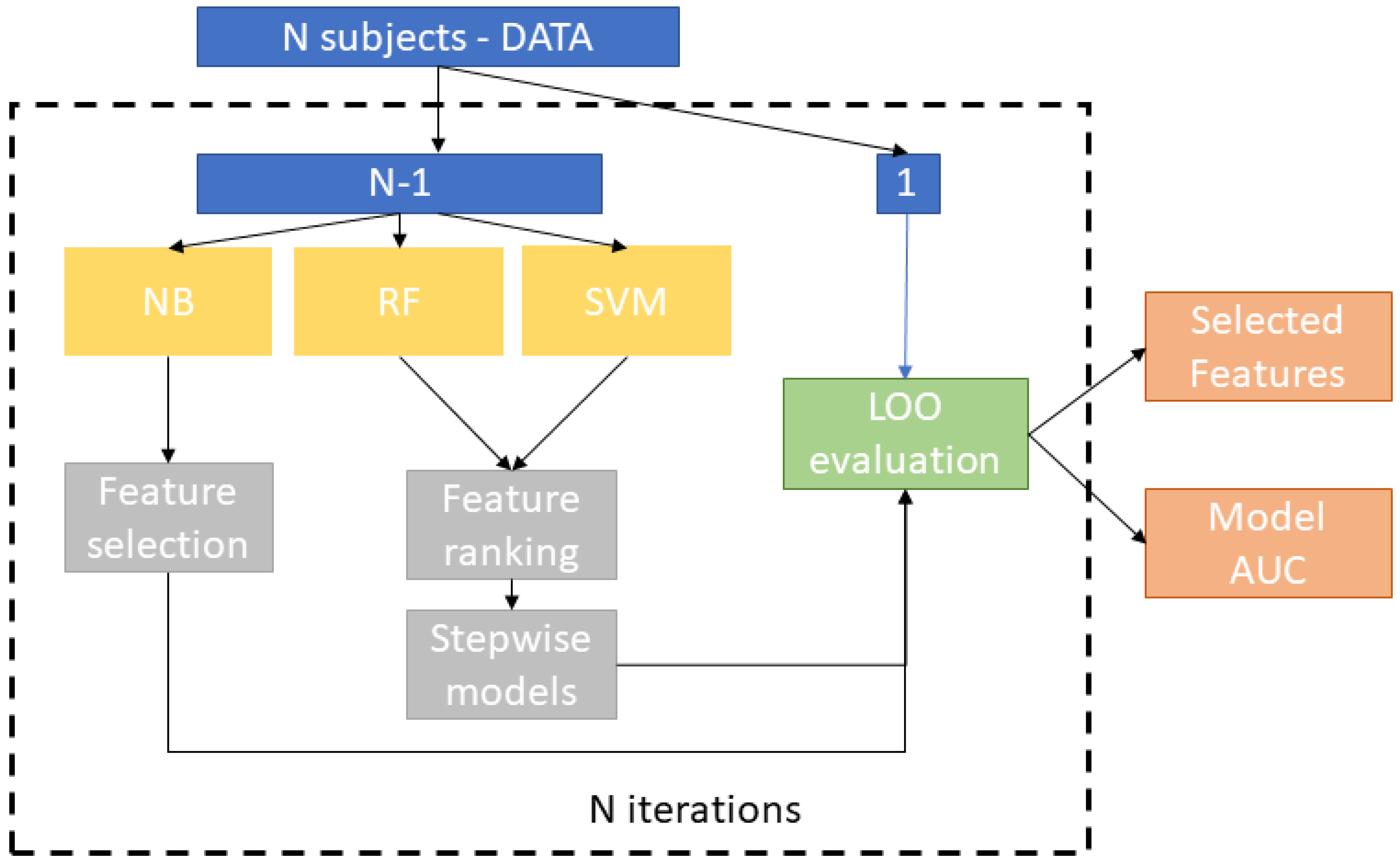
2.3. Statistical Data Analysis
3. Results and Discussion
3.1. Discrimination between Malignant Pleural Mesothelioma Patients and Healthy Controls
3.2. Independent Validation on Asymptomatic Former Asbestos-Exposed Subjects
4. Conclusions and Future Perspectives
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Baumann, F.; Ambrosi, J.P.; Carbone, M. Asbestos is not just asbestos: An unrecognized health hazard. Lancet Oncol. 2013, 14, 576–578. [Google Scholar] [CrossRef]
- Bonifazi, G.; Capobianco, G.; Serranti, S. Asbestos cointaining materials detection and classification by the use of hyperspectral inaging. J. Hazard. Mater. 2018, 344, 981–993. [Google Scholar] [CrossRef] [PubMed]
- Jarvholm, B.; Burdorf, A. Emerging evidence that the ban on asbestos use is reducing the occurrence of pleural mesothelioma in Sweden. Scand. J. Public Health 2015, 43, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Krupoves, A.; Camus, M.; De Guire, L. Incidence of malignant mesothelioma of the pleura in Quebec and Canada from 1984 to 2007, and projections from 2008 to 2032. Am. J. Ind. Med. 2015, 58, 473–482. [Google Scholar] [CrossRef] [PubMed]
- Soeberg, M.J.; Leigh, J.; Driscoli, T.; Armstrong, B.; Young, J.M.; Van Zandwijck, N. Incidence and survival trends for malignant pleural and peritoneal mesothelioma, Australia, 1982-2009. Occup. Environ. Med. 2016, 73, 187–194. [Google Scholar] [CrossRef]
- Marsh, G.M.; Riordan, A.S.; Keeton, K.A.; Benson, S.M. Non-occupational exposure to asbestos and risk of pleural mesothelioma: Review and meta-analysis. Occup. Environ. Med. 2017, 74, 838–846. [Google Scholar] [CrossRef]
- Bermann, D.W.; Crump, K.S. A meta analysis of asbestos-related cancer risk that addresses fiber size and mineral type. Crit. Rev. Toxicol. 2008, 38 (Suppl. 1), 49–73. [Google Scholar] [CrossRef]
- Langniau, S.; Lamote, K.; van Meerbeeck, J.P.; Vermaelen, K.Y. Biomarkers for early diagnosis of malignant mesothelioma: Do we need another moonshot? Oncotarget 2017, 8, 53751–53762. [Google Scholar] [CrossRef][Green Version]
- Cowan, D.M.; Cheng, T.J.; Ground, M.; Shamel, J.; Varghese, A.; Madl, A.K. Analysis of work place compliance measurement of asbestos by the U.S. Occupational Safety and Health Administration (1984-2011). Regul. Toxicol. Pharmacol. 2015, 72, 615–629. [Google Scholar] [CrossRef]
- Catino, A.; de Gennaro, G.; Di Gilio, A.; Facchini, L.; Galetta, D.; Palmisani, J.; Porcelli, F.; Varesano, N. Breath Analysis: A Systematic Review of Volatile Organic Compounds (VOCs) in Diagnostic and Therapeutic Management of Pleural Mesothelioma. Cancers 2019, 11, 831. [Google Scholar] [CrossRef]
- Novello, S.; Pinto, C.; Torri, V.; Porcu, L.; Di Maio, M.; Tiseo, M.; Ceresoli, G.; Magnani, C.; Silvestri, S.; Veltri, A.; et al. The third Italian consensus conference for malignant pleural mesothelioma: State of the art and recommendations. Crit. Rev. Oncol. Hematol. 2016, 104, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Matullo, G.; Guarrera, S.; Betti, M.; Fiorito, G.; Ferrante, D.; Voglino, F.; Cadby, G.; Di Gaetano, C.; Rosa, F.; Russo, A.; et al. Genetic variants associated with increased risk of malignant pleural mesothelioma: A genome-wide association study. PLoS ONE 2013, 8, 61253. [Google Scholar] [CrossRef] [PubMed]
- Miekisch, W.; Schubert, J.K.; Noeldge-Schomburg, G.F.E. Diagnostic potential of breath analysis—focus on volatile organic compounds. Clin. Chim. Acta 2004, 347, 25–39. [Google Scholar] [CrossRef] [PubMed]
- Lamote, K.; Hiddinga, B.; Van Cleemput, J.; Nackaerts, K.; Thas, O.; Van Meerbeeck, J.P. A breath test for diagnosing malignant pleural mesothelioma. Ann. Oncol. 2014, 25 (Suppl. 4), 542–545. [Google Scholar] [CrossRef][Green Version]
- Brusselmans, L.; Arnouts, L.; Millevert, C.; Vandersnickt, J.; Van Meerbeeck, J.P.; Lamote, K. Breath analysis as a diagnostic and screening tool for malignant pleural mesothelioma: A systematic review(Review). Transl. Lung Cancer Res. 2018, 7, 520–536. [Google Scholar] [CrossRef] [PubMed]
- Dragonieri, S.; Van der Schee, M.P.; Massaro, T.; Schiavulli, N.; Brinkman, P.; Pinca, A.; Carratú, P.; Spanevello, A.; Resta, O.; Musti, M.; et al. An electronic nose distinguishes exhaled breath of patients with Malignant Pleural Mesothelioma from controls. Lung Cancer 2012, 75, 326–331. [Google Scholar] [CrossRef]
- Chapman, E.A.; Thomas, P.S.; Stone, E.; Lewis, C.; Yates, D.H. A breath test for malignant mesothelioma using an electronic nose. Eur. Respir. J. 2012, 40, 448–454. [Google Scholar] [CrossRef]
- Cakir, Y.; Métrailler, L.; Baumbach, J.I.; Ktaus, T. Signals in asbestos related diseases in human breath—Preliminary results. Int. J. Ion. Mobil. Spec. 2014, 17, 87–94. [Google Scholar] [CrossRef]
- Lamote, K.; Vynck, M.; Van Cleemput, J.; Thas, O.; Nackaerts, K.; Van Meerbeeck, J.P. Detection of malignant pleural mesothelioma in exhaled breath by multicapillary column/ion mobility spectrometry (MCC/IMS). J. Breath Res. 2016, 10, 046001. [Google Scholar] [CrossRef]
- Lamote, K.; Vynck, M.; Thas, O.; Van Cleemput, J.; Thas, O.; Nackaerts, K.; Van Meerbeeck, J.P. Exhaled breath to screen for malignant pleural mesothelioma: A validation study. Eur. Respir. J. 2017, 50, 1700919. [Google Scholar] [CrossRef]
- De Gennaro, G.; Dragonieri, S.; Longobardi, F.; Musti, M.; Stallone, G.; Trizio, L.; Tutino, M. Chemical characterization of exhaled breath to differentiate between patients with malignant plueral mesothelioma from subjects with similar professional asbestos exposure. Anal. Bioanal. Chem. 2010, 398, 3043–3050. [Google Scholar] [CrossRef] [PubMed]
- Lamote, K.; Brinkman, P.; Vandermeersch, L.; Vynck, M.; Sterk, P.J.; Van Langenhove, H.; Thas, O.; Van Cleemput, J.; Nackaerts, K.; Van Meerbeeck, J.P. Breath analysis by gas chromatography-mass spectrometry and electronic nose to screen for pleural mesothelioma: A crosssectional case-control study. Oncotarget 2017, 27, 91593–91602. [Google Scholar] [CrossRef] [PubMed]
- de Gennaro, G.; Loiotile, A.D.; Fracchiolla, R.; Palmisani, J.; Saracino, M.R.; Tutino, M. Temporal variation of VOC emission from solvent and water based wood stains. Atmos. Environ. 2015, 115, 53–61. [Google Scholar] [CrossRef]
- Lombardi, A.; Guaragnella, C.; Amoroso, N.; Monaco, A.; Fazio, L.; Taurisano, P.; Pergola, G.; Blasi, G.; Bertolino, A.; Bellotti, R.; et al. Modelling cognitive loads in schizophrenia by means of new functional dynamic indexes. NeuroImage 2019, 195, 150–164. [Google Scholar] [CrossRef]
- Kononenko, I. Inductive and Bayesian learning in medical diagnosis. Appl. Artif. Intell. 1993, 7, 317–337. [Google Scholar] [CrossRef]
- Cortes, C.; Vapnik, V. Support vector machine. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Guyon, I.; Elissee, A. An introduction to variable and feature selection. J. Mach. Learn. Res. 2003, 3, 1157–1182. [Google Scholar]
- Yan, K.; Zhang, D. Feature selection and analysis on correlated gas sensor data with recursive feature elimination. Sens. Actuators B Chem. 2015, 212, 353–363. [Google Scholar] [CrossRef]
- Andy, L.; Wiener, M. Classification and regression by randomForest. R News 2002, 2–3, 18–22. [Google Scholar]
- Bradley, A.P. The use of the area under the ROC curve in the evaluation of machine learning algorithms. Pattern Recognit. 1997, 30, 1145–1159. [Google Scholar] [CrossRef]
- Zahangir, A.; Saifur Rahman, M.; Sohel Rahman, M. A Random Forest based predictor for medical data classification using feature ranking. Inform. Med. Unlocked 2019, 15, 100180. [Google Scholar]
- Bajtarevic, A.; Ager, C.; Pienz, M.; Klieber, M.; Schwarz, K.; Ligor, M.; Ligor, T.; Filipiak, W.; Denz, H.; Fiegl, M.; et al. Noninvasive detection of lung cancer by analysis of exhaled breath. BMC Cancer 2009, 9, 348. [Google Scholar] [CrossRef] [PubMed]
- Ligor, M.; Ligor, T.; Bajtarevic, A.; Ager, C.; Pienz, M.; Klieber, M.; Denz, H.; Fiegl, M.; Hilbe, W.; Weiss, W.; et al. Determination of volatile organic compounds in exhaled breath of patients with lung cancer using solid phase microextraction and gas chromatography mass spectrometry. Clin. Chem. Lab. Med. 2009, 47, 550–560. [Google Scholar] [CrossRef]
- Poli, D.; Goldoni, M.; Caglieri, A.; Ceresa, G.; Acampa, O.; Carbognani, P.; Rusca, M.; Massimo, C. Breath analysis in non small cell lung cancer patients after surgical tumour resection. Acta Biomed. 2008, 79 (Suppl. 1), 64–72. [Google Scholar]
- Jia, Z.; Zhang, H.; Ong, C.N.; Patra, A.; Lu, Y.; Lim, C.T.; Venkatesan, T. Detection of Lung Cancer: Concomitant Volatile Organic Compounds and Metabolomic Profiling of Six Cancer Cell Lines of Different Histological Origins. ACS Omega 2018, 3, 5131–5140. [Google Scholar] [CrossRef]
- Hakim, M.; Broza, Y.Y.; Barash, O.; Peled, N.; Phillips, M.; Amann, A.; Haick, H. Volatile organic compounds of lung cancer and possible biochemical pathways. Chem. Rev. 2012, 112, 5949–5966. [Google Scholar] [CrossRef]
- Sponring, A.; Filipiak, W.; Mikoviny, T.; Ager, C.; Schubert, J.; Miekisch, W.; Amann, A.; Troppmair, J. Release of volatile organic compounds from the lung cancer cell line NCIH2087 in-vitro. Anticancer Res. 2009, 29, 419–426. [Google Scholar]
- Jia, Z.; Patra, A.; Krishnan Kutty, V.; Venkatesan, T. Critical Review of Volatile Organic Compound Analysis in Breath and In Vitro Cell Culture for Detection of Lung Cancer. Metabolites 2019, 9, 52. [Google Scholar] [CrossRef]
- Mamatha, S.; Yoav, Y.B.; Abraham, M.; Hossam, H. Profiling Single Cancer Cells with Volatolomics Approach. iScience 2019, 11, 178–188. [Google Scholar]
- Antoniou, S.; Gaude, E.; Ruparel, M.; van der Schee, M.P.; Janes, S.M.; Rintoul, R.C. The potential of breath analysis to improve outcome for patients with lung cancer. J. Breath Res. 2019, 13, 034002. [Google Scholar] [CrossRef]
- Vander Heiden, M.G.; Cantley, L.; Cand Thompson, C.B. Understanding the Warburg effect: The metabolic requirements of cell proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef]
- Warburg, O. On respiratory impairment in cancer cells. Science 1952, 124, 69–270. [Google Scholar]
- Fan, T.W.; Lane, A.N.; Higashi, R.M.; Farag, M.A.; Gao, H.; Bousamra, M.; Miller, D.M. Altered regulation of metabolic pathways in human lung cancer discerned by 13C stable isotoperesolved metabolomics (SIRM). Mol. Cancer 2009, 8, 41. [Google Scholar] [CrossRef]
- Sellers, K.; Fox, M.P.; Bousamra, M.; Slone, S.P.; Higashi, R.M.; Miller, D.M.; Wang, Y.; Yan, J.; Yuneva, M.O.; Deshpande, R.; et al. Pyruvate carboxylase is critical for non–small-cell lung cancer proliferation. J. Clin. Investig. 2015, 125, 687–698. [Google Scholar] [CrossRef]
- Hensley, C.T.; Faubert, B.; Yuan, Q. Metabolic heterogeneity in human lung tumors. Cell 2016, 164, 681–694. [Google Scholar] [CrossRef]
- Faubert, B.; Li, K.; Cai, L.; Hensley, C.T.; Kim, J.; Zacharias, L.G.; Yang, C.; Do, Q.; Doucette, S.; Burguete, D.; et al. Lactate metabolism in human lung tumors. Cell 2017, 171, 358–371. [Google Scholar] [CrossRef]
- Murphy, M.P. How mitochondria produce reactive oxygen species. J. Biochem. 2009, 417, 1–13. [Google Scholar] [CrossRef]
- Abeti, R.; Parkinson, M.H.; Hargreaves, I.P.; Angelova, P.R.; Sandi, C.; Pook, M.A.; Giunti, P.; Abramov, A.Y. Mitochondrial energy imbalance and lipid peroxidation cause cell death in Friedreich’s ataxia. Cell Death Dis. 2016, 7, 2237. [Google Scholar] [CrossRef]
- Marien, E.; Meister, M.; Muley, T.; Fieuws, S.; Bordel, S.; Derua, R.; Spraggins, J.; Van de Plas, R.; Dehairs, J. Non-small cell lung cancer is characterized by dramatic changes in phospholipid profiles. Int. J. Cancer 2015, 137, 1539–1548. [Google Scholar] [CrossRef]
- Eggers, L.F.; Müller, J.; Marella, C.; Scholz, V.; Watz, H.; Kugler, C.; Rabe, K.F.; Goldmann, T.; Schwudke, D. Lipidomes of lung cancer and tumour free lung tissues reveal distinct molecular signatures for cancer differentiation, age, inflammation, and pulmonary emphysema. Sci. Rep. 2017, 7, 11087. [Google Scholar] [CrossRef]
- Chen, X.; Xu, F.J.; Wang, Y.; Pan, Y.F.; Lu, D.J.; Wang, P.; Ying, K.; Chen, E.; Zhang, W. A study of the volatile organic compounds exhaled by lung cancer cells in vitro for breath diagnosis. Cancer 2007, 110, 835–844. [Google Scholar] [CrossRef]
- Al Hafid, N.; Christodoulou, J. Phenylketonuria: A review of current and future treatments. Transl. Pediatr. 2015, 4, 304–317. [Google Scholar]
- Agmon, I.N.; Abud, M.; Liran, O.; Gai-Mor, N.; Ilouze, M.; Onn, A.; Bar, J.; Navon, R.; Shlomi, D.; Haick, H.; et al. Exhaled breath analysis for monitoring response to treatment in advanced lung cancer. J. Thorac. Oncol. 2016, 11, 827–837. [Google Scholar] [CrossRef]
- O’Neill, H.J.; Gordon, S.M.; O’Neill, M.H.; Gibbons, R.D.; Szidon, J.P. A computerized classification technique for screening for the presence of breath biomarkers in lung cancer. Clin. Chem. 1998, 8, 1613–1618. [Google Scholar] [CrossRef]
- Tunek, A.; Platt, K.L.; Bentley, P.; Oesch, F. Microsomal metabolism of benzene to species irreversibly binding to microsomal protein and effects of modifications of this metabolism. Mol. Pharmacol. 1978, 14, 920. [Google Scholar]
- Tunek, A.; Platt, K.L.; Przybylski, M.; Oesch, F. Multi-step metabolic activation of benzene. Effect of superoxide dismutase on covalent binding to microsomal macromolecules, and identification of glutathione conjugates using high pressure liquid chromatography and field desorption mass spectrometry. Chem.-Biol. Interact. 1980, 33, 1–17. [Google Scholar] [CrossRef]
- Lunte, S.M.; Kissinger, P.T. Detection and identification of sulfhydryl conjugates of p-benzoquinone in microsomal incubations of benzene and phenol. Chem.-Biol. Interact. 1983, 47, 195. [Google Scholar] [CrossRef]
- Sánchez Mdel, N.; García, E.H.; Pavón, J.L.; Cordero, B.M. Fast analytical methodology based on mass spectrometry for the determination of volatile biomarkers in saliva. Anal. Chem. 2012, 84, 379–385. [Google Scholar] [CrossRef]
- Kohlmuller, D. Is n-pentane really an index of lipid peroxidation in humans and animals? A methodological reevaluation. Anal. Biochem. 1993, 210, 268. [Google Scholar] [CrossRef]
- Risby, T. Clinical application of breath biomarkers of oxidative stress status. Free Radical Biol. Med. 1999, 27, 1182. [Google Scholar] [CrossRef]
- Halliwel, B. Free radicals, antioxidants, and human disease: Where are we now? J. Lab. Clin. Med. 1992, 119, 598. [Google Scholar]
- Karjalainen, A.; Pukkala, E.; Kauppinen, T.; Partanen, T. Incidence of cancer among Finnish patients. Cancer Causes Control. 1999, 10, 51–57. [Google Scholar] [CrossRef]
- Roberts, H.C.; Patsios, D.A.; Paul, N.S.; de Perrot, M.; Teel, W.; Bayanati, H.; Shepherd, F.; Johnston, M.R. Screening for Malignant Pleural Mesothelioma and Lung Cancer in Individuals with a History of Asbestos Exposure. J. Thorac. Oncol. 2009, 4, 620–628. [Google Scholar] [CrossRef]
- Bayram, M.; Dongel, I.; Akbaş, A.; Benli, I.; Akkoyunlu, M.E.; Bakan, N.D. Serum Biomarkers in Patients with Mesothelioma and Pleural Plaques and Healthy Subjects Exposed to Naturally Occurring Asbestos. Lung 2014, 192, 197–203. [Google Scholar] [CrossRef]
- Pairon, J.; Laurent, F.; Rinaldo, M.; Clin, B.; Andujar, P.; Ameille, J.; Brochard, P.; Chammings, S.; Ferretti, G.; Galateau-Sallè, F.; et al. Pleural Plaques and the Risk of Pleural Mesothelioma. J. Natl. Cancer Inst. 2013, 105, 293–301. [Google Scholar] [CrossRef]
- Peng, G.; Hakim, M.; Broza, Y.Y.; Billan, S.; Abdah-Bortnyak, R.; Kuten, A.; Tisch, U.; Haick, H. Detection of lung, breast, colorectal, and prostate cancers from exhaled breath using a single array of nanosensors. Br. J. Cancer 2010, 103, 542–551. [Google Scholar] [CrossRef]
- Mazzone, P.J.; Hammel, J.; Dweik, R.; Na, J. Diagnosis of lung cancer by the analysis of exhaled breath with a colorimetric sensor array. Thorax 2007, 62, 565–568. [Google Scholar] [CrossRef]
- Phillips, M.; Greenberg, J.; Sabas, M. Alveolar gradient of pentane in normal human breath. Free Radic. Res. 1994, 20, 333–337. [Google Scholar] [CrossRef]
- Amann, A.; Mochalski, P.; Ruzsanyi, V.; Broza, Y.Y.; Haick, H. Assessment of the exhalation kinetics of volatile cancer biomarkers based on their physicochemical properties. J. Breath Res. 2014, 8, 016003. [Google Scholar] [CrossRef]
- Jia, C.; Yu, X.; Masiak, W. Blood/air distribution of volatile organic compounds (VOCs) in a nationally representative sample. Sci. Total Environ. 2012, 419, 225–232. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variation | MPM * | HC * | AEx * |
|---|---|---|---|
| Subject | 14 | 20 | 5 |
| Male/female | 6/8 | 10/10 | 2/3 |
| Age | 73.6 (57–82) | 53.6 (37–68) | 63.5 (53–81) |
| Body Mass Index | 24.9 | 24.0 | 24.4 |
| BMI (Kg/m2) | (19.2–29.4) | (21.6–27.8) | (20.8–25.9) |
| Smoking status | |||
| Current | 0 | 3 (15%) | 0 |
| Ex | 4 (29%) | 4(20%) | 2 (40%) |
| Never | 10 (71%) | 13 (65%) | 3 (60%) |
| Pack/years | 34.7 (19–62) | 40.5 (21–73) | 36.2 (32–55) |
| Step | Parameters | Value |
|---|---|---|
| Tube desorption | Purge time | 3 min at 5 mL/min–trap in line |
| Desorption time | 10 min | |
| Desorption temperature | 300 °C | |
| Temperature of cold trap | 20 °C | |
| Desorption flow | 30 mL/min, no split | |
| Focusing trap desorption | Temperature of cold trap desorption | 300 °C |
| Split low | 5 mL/min | |
| Transfer Line Temperature | 200 °C | |
| GC analysis | Gas carrier | He |
| Gas flow | 1.7 mL/min | |
| Analytical column | VOCOL® (Supelco), diphenyl dimethyl polysiloxane with crosslinking moieties, 60 m × 0.25 mm ID, 1.5 μm stationary phase thickness | |
| Oven temperature | 37 °C hold for 5 min | |
| 37–190 °C at 6 °C/min | ||
| 190–200 °C at 2 °C/min | ||
| 220–220 °C at 15 °C/min | ||
| 220 °C hold for 3 min |
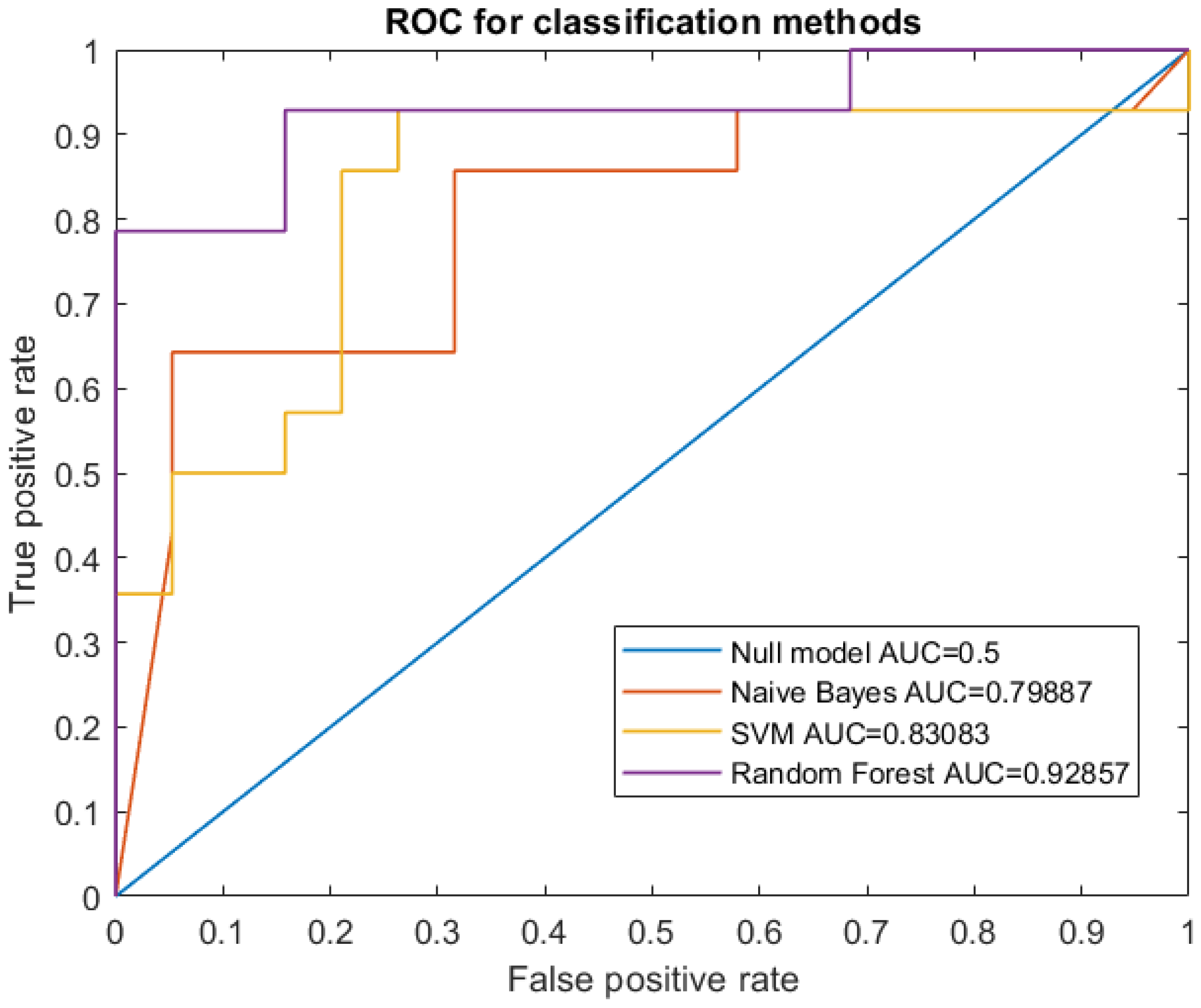
| Naive Bayes | SVM | RF |
|---|---|---|
| 0.80 | 0.83 | 0.93 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Gilio, A.; Catino, A.; Lombardi, A.; Palmisani, J.; Facchini, L.; Mongelli, T.; Varesano, N.; Bellotti, R.; Galetta, D.; de Gennaro, G.; et al. Breath Analysis for Early Detection of Malignant Pleural Mesothelioma: Volatile Organic Compounds (VOCs) Determination and Possible Biochemical Pathways. Cancers 2020, 12, 1262. https://doi.org/10.3390/cancers12051262
Di Gilio A, Catino A, Lombardi A, Palmisani J, Facchini L, Mongelli T, Varesano N, Bellotti R, Galetta D, de Gennaro G, et al. Breath Analysis for Early Detection of Malignant Pleural Mesothelioma: Volatile Organic Compounds (VOCs) Determination and Possible Biochemical Pathways. Cancers. 2020; 12(5):1262. https://doi.org/10.3390/cancers12051262
Chicago/Turabian StyleDi Gilio, Alessia, Annamaria Catino, Angela Lombardi, Jolanda Palmisani, Laura Facchini, Teresa Mongelli, Niccolò Varesano, Roberto Bellotti, Domenico Galetta, Gianluigi de Gennaro, and et al. 2020. "Breath Analysis for Early Detection of Malignant Pleural Mesothelioma: Volatile Organic Compounds (VOCs) Determination and Possible Biochemical Pathways" Cancers 12, no. 5: 1262. https://doi.org/10.3390/cancers12051262
APA StyleDi Gilio, A., Catino, A., Lombardi, A., Palmisani, J., Facchini, L., Mongelli, T., Varesano, N., Bellotti, R., Galetta, D., de Gennaro, G., & Tangaro, S. (2020). Breath Analysis for Early Detection of Malignant Pleural Mesothelioma: Volatile Organic Compounds (VOCs) Determination and Possible Biochemical Pathways. Cancers, 12(5), 1262. https://doi.org/10.3390/cancers12051262