Primary Resistance to PD-1-Based Immunotherapy—A Study in 319 Patients with Stage IV Melanoma

 , , ,
, , , 
Abstract
1. Introduction
2. Patients and Methods
2.1. Patients Cohort
2.2. Statistical Analysis
3. Results
3.1. Univariate and Multivariate Analysis
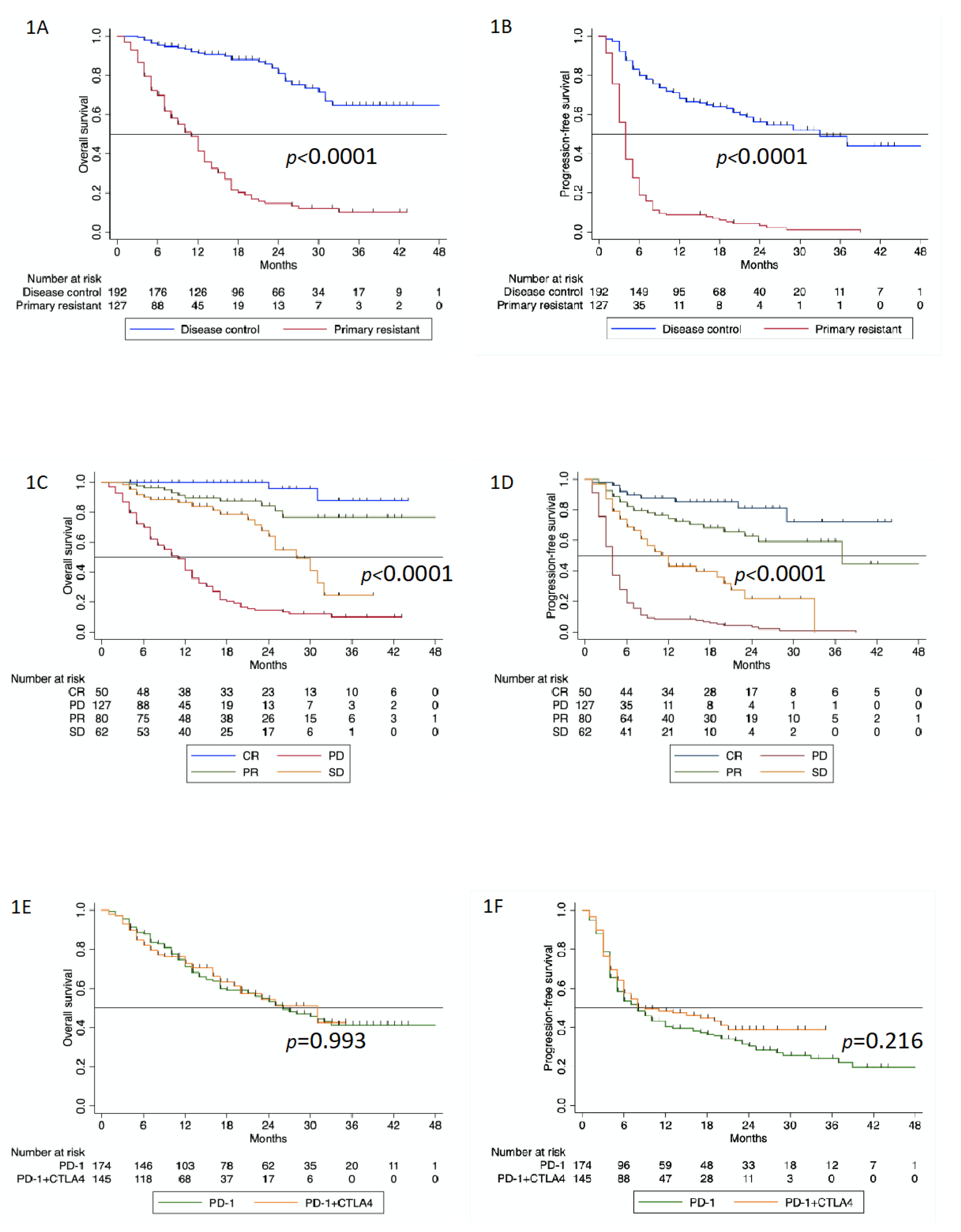
3.2. Survival Analysis
3.3. Second-Line Therapies and Outcomes
3.4. Pseudoprogression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Franken, M.G.; Leeneman, B.; Gheorghe, M.; Uyl-de Groot, C.A.; Haanen, J.B.A.G.; van Baal, P.H.M. A systematic literature review and network meta-analysis of effectiveness and safety outcomes in advanced melanoma. Eur. J. Cancer 2019, 123, 58–71. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; O’Day, S.J.; McDermott, D.F.; Weber, R.W.; Sosman, J.A.; Haanen, J.B.; Gonzalez, R.; Robert, C.; Schadendorf, D.; Hassel, J.C.; et al. Improved survival with ipilimumab in patients with metastatic melanoma. N. Engl. J. Med. 2010, 363, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Robert, C.; Schachter, J.; Long, G.V.; Arance, A.; Grob, J.J.; Mortier, L.; Daud, A.; Carlino, M.S.; McNeil, C.; Lotem, M.; et al. Pembrolizumab versus ipilimumab in advanced melanoma. N. Engl. J. Med. 2015, 372, 2521–2532. [Google Scholar] [CrossRef] [PubMed]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.-J.; Rutkowski, P.; Lao, C.D.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Dummer, R.; et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N. Engl. J. Med. 2019, 381, 1535–1546. [Google Scholar] [CrossRef]
- Maio, M.; Grob, J.-J.; Aamdal, S.; Bondarenko, I.; Robert, C.; Thomas, L.; Garbe, C.; Chiarion-Sileni, V.; Testori, A.; Chen, T.-T.; et al. Five-year survival rates for treatment-naive patients with advanced melanoma who received ipilimumab plus dacarbazine in a phase III trial. J. Clin. Oncol. 2015, 33, 1191–1196. [Google Scholar] [CrossRef]
- Schadendorf, D.; Hodi, F.S.; Robert, C.; Weber, J.S.; Margolin, K.; Hamid, O.; Patt, D.; Chen, T.-T.; Berman, D.M.; Wolchok, J.D. Pooled analysis of long-term survival data from phase II and phase III trials of ipilimumab in unresectable or metastatic melanoma. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2015, 33, 1889–1894. [Google Scholar] [CrossRef]
- Fares, C.M.; Van Allen, E.M.; Drake, C.G.; Allison, J.P.; Hu-Lieskovan, S. Mechanisms of resistance to immune checkpoint blockade: Why does checkpoint inhibitor immunotherapy not work for all patients? Am. Soc. Clin. Oncol. Educ. Book 2019, 39, 147–164. [Google Scholar] [CrossRef]
- Shin, D.S.; Zaretsky, J.M.; Escuin-Ordinas, H.; Garcia-Diaz, A.; Hu-Lieskovan, S.; Kalbasi, A.; Grasso, C.S.; Hugo, W.; Sandoval, S.; Torrejon, D.Y.; et al. Primary Resistance to PD-1 blockade mediated by JAK1/2 mutations. Cancer Discov. 2017, 7, 188–201. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N. Engl. J. Med. 2015, 373, 23–34. [Google Scholar] [CrossRef]
- Robert, C.; Long, G.V.; Brady, B.; Dutriaux, C.; Maio, M.; Mortier, L.; Hassel, J.C.; Rutkowski, P.; McNeil, C.; Kalinka-Warzocha, E.; et al. Nivolumab in previously untreated melanoma without BRAF mutation. N. Engl. J. Med. 2015, 372, 320–330. [Google Scholar] [CrossRef]
- Robert, C.; Thomas, L.; Bondarenko, I.; O’Day, S.; Weber, J.; Garbe, C.; Lebbe, C.; Baurain, J.-F.; Testori, A.; Grob, J.-J.; et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N. Engl. J. Med. 2011, 364, 2517–2526. [Google Scholar] [CrossRef] [PubMed]
- Jenkins, R.W.; Barbie, D.A.; Flaherty, K.T. Mechanisms of resistance to immune checkpoint inhibitors. Br. J. Cancer 2018, 118, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Seto, T.; Sam, D.; Pan, M. Mechanisms of primary and secondary resistance to immune checkpoint inhibitors in cancer. Med. Sci. 2019, 7, 14. [Google Scholar] [CrossRef] [PubMed]
- Fuereder, T. Resistance to immune checkpoint inhibitors. Next steps and combinational approaches. Memo Mag. Eur. Med Oncol. 2019, 12, 123–127. [Google Scholar] [CrossRef]
- Veldman, J.; Visser, L.; Berg, A.v.d.; Diepstra, A. Primary and acquired resistance mechanisms to immune checkpoint inhibition in Hodgkin lymphoma. Cancer Treat. Rev. 2020, 82, 101931. [Google Scholar] [CrossRef]
- Sharma, P.; Hu-Lieskovan, S.; Wargo, J.A.; Ribas, A. Primary, Adaptive, and Acquired Resistance to Cancer Immunotherapy. Cell 2017, 168, 707–723. [Google Scholar] [CrossRef]
- Zaretsky, J.M.; Garcia-Diaz, A.; Shin, D.S.; Escuin-Ordinas, H.; Hugo, W.; Hu-Lieskovan, S.; Torrejon, D.Y.; Abril-Rodriguez, G.; Sandoval, S.; Barthly, L.; et al. Mutations associated with acquired resistance to PD-1 Blockade in Melanoma. N. Engl. J. Med. 2016, 375, 819–829. [Google Scholar] [CrossRef]
- Ladányi, A.; Kiss, J.; Somlai, B.; Gilde, K.; Fejos, Z.; Mohos, A.; Gaudi, I.; Tímár, J. Density of DC-LAMP(+) mature dendritic cells in combination with activated T lymphocytes infiltrating primary cutaneous melanoma is a strong independent prognostic factor. Cancer Immunol. Immunother. CII 2007, 56, 1459–1469. [Google Scholar] [CrossRef]
- Wu, W.; Wang, W.; Wang, Y.; Li, W.; Yu, G.; Li, Z.; Fang, C.; Shen, Y.; Sun, Z.; Han, L.; et al. IL-37b suppresses T cell priming by modulating dendritic cell maturation and cytokine production via dampening ERK/NF-κB/S6K signalings. Acta Biochim. Et Biophys. Sin. 2015, 47, 597–603. [Google Scholar] [CrossRef]
- Lindenberg, J.J.; van de Ven, R.; Lougheed, S.M.; Zomer, A.; Santegoets, S.J.A.M.; Griffioen, A.W.; Hooijberg, E.; van den Eertwegh, A.J.M.; Thijssen, V.L.; Scheper, R.J.; et al. Functional characterization of a STAT3-dependent dendritic cell-derived CD14+ cell population arising upon IL-10-driven maturation. Oncoimmunology 2013, 2, e23837. [Google Scholar] [CrossRef]
- Strauss, L.; Bergmann, C.; Szczepanski, M.; Gooding, W.; Johnson, J.T.; Whiteside, T.L. A Unique Subset of CD4+CD25highFoxp3+ T cells secreting interleukin-10 and transforming growth factor-β1 mediates suppression in the tumor microenvironment. Clin. Cancer Res. 2007, 13, 4345. [Google Scholar] [CrossRef]
- Viguier, M.; Lemaître, F.; Verola, O.; Cho, M.-S.; Gorochov, G.; Dubertret, L.; Bachelez, H.; Kourilsky, P.; Ferradini, L. Foxp3 expressing CD4+CD25high regulatory T cells are overrepresented in human metastatic melanoma lymph nodes and inhibit the function of infiltrating T cells. J. Immunol. 2004, 173, 1444. [Google Scholar] [CrossRef] [PubMed]
- Togashi, Y.; Shitara, K.; Nishikawa, H. Regulatory T cells in cancer immunosuppression-implications for anticancer therapy. Nat. Rev. Clin. Oncol. 2019, 16, 356–371. [Google Scholar] [CrossRef] [PubMed]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Chen, W.; Xu, Z.P.; Gu, W. PD-L1 Distribution and perspective for cancer immunotherapy—Blockade, knockdown, or inhibition. Front. Immunol. 2019, 10, 2022. [Google Scholar] [CrossRef]
- Snyder, A.; Makarov, V.; Merghoub, T.; Yuan, J.; Zaretsky, J.M.; Desrichard, A.; Walsh, L.A.; Postow, M.A.; Wong, P.; Ho, T.S.; et al. Genetic basis for clinical response to CTLA-4 blockade in melanoma. N. Engl. J. Med. 2014, 371, 2189–2199. [Google Scholar] [CrossRef] [PubMed]
- McGranahan, N.; Furness, A.J.S.; Rosenthal, R.; Ramskov, S.; Lyngaa, R.; Saini, S.K.; Jamal-Hanjani, M.; Wilson, G.A.; Birkbak, N.J.; Hiley, C.T.; et al. Clonal neoantigens elicit T cell immunoreactivity and sensitivity to immune checkpoint blockade. Science (N. Y.) 2016, 351, 1463. [Google Scholar] [CrossRef] [PubMed]
- del Campo, A.B.; Kyte, J.A.; Carretero, J.; Zinchencko, S.; Méndez, R.; González-Aseguinolaza, G.; Ruiz-Cabello, F.; Aamdal, S.; Gaudernack, G.; Garrido, F.; et al. Immune escape of cancer cells with beta2-microglobulin loss over the course of metastatic melanoma. Int. J. Cancer 2014, 134, 102–113. [Google Scholar] [CrossRef] [PubMed]
- Forschner, A.; Battke, F.; Hadaschik, D.; Schulze, M.; Weißgraeber, S.; Han, C.-T.; Kopp, M.; Frick, M.; Klumpp, B.; Tietze, N.; et al. Tumor mutation burden and circulating tumor DNA in combined CTLA-4 and PD-1 antibody therapy in metastatic melanoma–results of a prospective biomarker study. J. Immunother. Cancer 2019, 7, 180. [Google Scholar] [CrossRef] [PubMed]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA A Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Grassadonia, A.; Sperduti, I.; Vici, P.; Iezzi, L.; Brocco, D.; Gamucci, T.; Pizzuti, L.; Maugeri-Saccà, M.; Marchetti, P.; Cognetti, G.; et al. Effect of Gender on the Outcome of Patients Receiving Immune Checkpoint Inhibitors for Advanced Cancer: A Systematic Review and Meta-Analysis of Phase III Randomized Clinical Trials. J. Clin. Med. 2018, 7, 542. [Google Scholar] [CrossRef]
- Wu, Y.; Ju, Q.; Jia, K.; Yu, J.; Shi, H.; Wu, H.; Jiang, M. Correlation between sex and efficacy of immune checkpoint inhibitors (PD-1 and CTLA-4 inhibitors). Int. J. Cancer 2018, 143, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Conforti, F.; Pala, L.; Bagnardi, V.; De Pas, T.; Martinetti, M.; Viale, G.; Gelber, R.D.; Goldhirsch, A. Cancer immunotherapy efficacy and patients’ sex: A systematic review and meta-analysis. Lancet Oncol. 2018, 19, 737–746. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Gonzalez, R.; Rutkowski, P.; Grob, J.-J.; Cowey, C.L.; Lao, C.D.; Wagstaff, J.; Schadendorf, D.; Ferrucci, P.F.; et al. Overall Survival with Combined Nivolumab and Ipilimumab in Advanced Melanoma. N. Engl. J. Med. 2017, 377, 1345–1356. [Google Scholar] [CrossRef] [PubMed]
- Bilen, M.A.; Shabto, J.M.; Martini, D.J.; Liu, Y.; Lewis, C.; Collins, H.; Akce, M.; Kissick, H.; Carthon, B.C.; Shaib, W.L.; et al. Sites of metastasis and association with clinical outcome in advanced stage cancer patients treated with immunotherapy. BMC Cancer 2019, 19, 857. [Google Scholar] [CrossRef]
- Tumeh, P.C.; Hellmann, M.D.; Hamid, O.; Tsai, K.K.; Loo, K.L.; Gubens, M.A.; Rosenblum, M.; Harview, C.L.; Taube, J.M.; Handley, N.; et al. Liver Metastasis and Treatment Outcome with Anti-PD-1 Monoclonal Antibody in Patients with Melanoma and NSCLC. Cancer Immunol. Res. 2017, 5, 417–424. [Google Scholar] [CrossRef]
- Weide, B.; Elsässer, M.; Büttner, P.; Pflugfelder, A.; Leiter, U.; Eigentler, T.K.; Bauer, J.; Witte, M.; Meier, F.; Garbe, C. Serum markers lactate dehydrogenase and S100B predict independently disease outcome in melanoma patients with distant metastasis. Br. J. Cancer 2012, 107, 422–428. [Google Scholar] [CrossRef]
- Wagner, N.B.; Forschner, A.; Leiter, U.; Garbe, C.; Eigentler, T.K. S100B and LDH as early prognostic markers for response and overall survival in melanoma patients treated with anti-PD-1 or combined anti-PD-1 plus anti-CTLA-4 antibodies. Br. J. Cancer 2018, 119, 339–346. [Google Scholar] [CrossRef]
- Schadendorf, D.; Hassel, J.C.; Fluck, M.; Eigentler, T.; Loquai, C.; Berneburg, M.; Gutzmer, R.; Meier, F.; Mohr, P.; Hauschild, A.; et al. Adjuvant immunotherapy with nivolumab (nivo) alone or in combination with ipilimumab (ipi) versus placebo in stage iv melanoma patients with no evidence of disease (ned): A randomized, double-blind phase 2 trial (immuned). Ann. Oncol. 2019, 30 (Suppl. 5), v851–v934. [Google Scholar] [CrossRef]
- Kugel, C.H.; Douglass, S.M.; Webster, M.R.; Kaur, A.; Liu, Q.; Yin, X.; Weiss, S.A.; Darvishian, F.; Al-Rohil, R.N.; Ndoye, A.; et al. Age Correlates with Response to Anti-PD1, Reflecting Age-Related Differences in Intratumoral Effector and Regulatory T-Cell Populations. Clin. Cancer Res. 2018, 24, 5347–5356. [Google Scholar] [CrossRef] [PubMed]
- Czarnecka, A.M.; Teterycz, P.; Mariuk-Jarema, A.; Lugowska, I.; Rogala, P.; Dudzisz-Sledz, M.; Switaj, T.; Rutkowski, P. Treatment Sequencing and Clinical Outcomes in BRAF-Positive and BRAF-Negative Unresectable and Metastatic Melanoma Patients Treated with new systemic therapies in routine practice. Target. Oncol. 2019, 14, 729–742. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.B.; Pectasides, E.; Feld, E.; Ye, F.; Zhao, S.; Johnpulle, R.; Merritt, R.; McDermott, D.F.; Puzanov, I.; Lawrence, D.; et al. Sequencing Treatment in BRAFV600 Mutant Melanoma: Anti-PD-1 Before and After BRAF Inhibition. J. Immunother. (Hagerstown Md. 1997) 2017, 40, 31–35. [Google Scholar] [CrossRef]
- Schilling, B.; Martens, A.; Geukes Foppen, M.H.; Gebhardt, C.; Hassel, J.C.; Rozeman, E.A.; Gesierich, A.; Gutzmer, R.; Kähler, K.C.; Livingstone, E.; et al. First-line therapy-stratified survival in BRAF-mutant melanoma: A retrospective multicenter analysis. Cancer Immunol. Immunother. CII 2019, 68, 765–772. [Google Scholar] [CrossRef] [PubMed]
- Moser, J.C.; Chen, D.; Hu-Lieskovan, S.; Grossmann, K.F.; Patel, S.; Colonna, S.V.; Ying, J.; Hyngstrom, J.R. Real-world survival of patients with advanced BRAF V600 mutated melanoma treated with front-line BRAF/MEK inhibitors, anti-PD-1 antibodies, or nivolumab/ipilimumab. Cancer Med. 2019, 8, 7637–7643. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | ICI Cohort n = 319 n (%) | n (%) | Univariate Analysis Test  | Multivariate Logistic Regression Analysis | |
|---|---|---|---|---|---|
| Primary Resistance n = 127 (40) | DC (CR, PR, SD) n = 192 (60) | ||||
| Age Distribution | 0.732 | ||||
| Median (years [IQR]) | 68 (56–77) | 65 (55–78) | 68 (56–77) | ||
| <60y | 101 (32) | 37 (29) | 64 (33) | ||
| 60y–75y | 114 (36) | 47 (37) | 67 (35) | ||
| >75y | 104 (32) | 43 (34) | 61 (32) | ||
| Sex | 0.049 | 0.822 | |||
| Male | 192 (60) | 68 (54) | 124 (65) | ||
| Female | 127 (40) | 59 (46) | 68 (35) | ||
| Tumor localization * | 0.000 | 0.001 | |||
| Head and neck | 54 (22) | 12 (13) | 42 (27) | ||
| Trunk | 73 (29) | 18 (20) | 55 (34) | ||
| Extremity | 109 (43) | 54 (59) | 55 (34) | ||
| Other | 15 (6) | 7 (8) | 8 (5) | ||
| Histological subtype * | 0.007 | 0.452 | |||
| SSM | 76 (32) | 31(37) | 45 (29) | ||
| NM | 72 (30) | 18(21) | 54 (35) | ||
| LMM | 13 (6) | 0 | 13 (9) | ||
| ALM | 30 (12) | 15 (18) | 15 (10) | ||
| Mucosal | 15 (6) | 7 (8) | 8 (5) | ||
| Other | 32 (14) | 14 (16) | 18 (12) | ||
| Stage at initial diagnosis * | 0.114 | ||||
| I | 48 (17) | 19 (18) | 29 (17) | ||
| II | 84 (31) | 25 (23) | 59 (35) | ||
| III | 95 (35) | 38 (37) | 57 (34) | ||
| IV | 47 (17) | 24 (22) | 23 (14) | ||
| Number of organs with metastases | 0.098 | 0.470 | |||
| 1-3 | 285 (89) | 109 (86) | 176 (92) | ||
| >3 | 34 (11) | 18 (14) | 16 (8) | ||
| Brain metastases | 0.618 | ||||
| No | 258 (81) | 101 (79) | 157 (82) | ||
| Yes | 61 (19) | 26 (21) | 35 (18) | ||
| Liver metastases | 0.139 | ||||
| No | 204 (64) | 75 (59) | 129 (67) | ||
| Yes | 115 (36) | 52 (41) | 63 (33) | ||
| BRAF mutation * | 0.844 | ||||
| BRAFmut | 88 (45) | 32 (44) | 56 (46) | ||
| BRAFwt | 106 (56) | 40 (56) | 66 (54) | ||
| LDH level * | 0.029 | 0.532 | |||
| Normal | 190 (68) | 67 (60) | 123 (73) | ||
| Elevated | 90 (32) | 44 (40) | 46 (27) | ||
| S100B level * | 0.000 | 0.008 | |||
| Normal | 157 (56) | 44 (40) | 113 (65) | ||
| Elevated | 125 (44) | 65 (60) | 60 (35) | ||
Chi-square test performed between the two groups—primary resistance and disease control; ICI = immune-checkpoint inhibitors cohort—145 patients received first-line treatment with nivolumab plus ipilimumab and 174 received antiPD-1 antibodies monotherapy (nivolumab n = 46 and pembrolizumab n = 128).; y = years; SSM = superficial spreading melanoma; NM = nodular melanoma; LMM = lentigo malignant melanoma; ALM = acral lentiginous melanoma; BRAFmut = presence of BRAFV600E/K mutation; BRAFwt = BRAF wild-type; LDH = lactate dehydrogenase; S100B = tumor marker protein S100B. p-values that are statistically significant are noted in bold.| Best Response | Median OS (Months; 95% CI) | OS (%; 95% CI) | ||
|---|---|---|---|---|
| 1-Year | 2-Year | 3-Year | ||
| CR n = 50 (15.7%) | not reached | 100% | 95.7 (87.3–100) | 87.7 (70.8–100) |
| PR n = 80 (25.1%) | not reached | 89.5 (82.1–96.9) | 84.4 (74.4–94.4) | 84.4 (74.4–94.4) |
| SD n = 62 (19.4%) | 28 (22.9–33.1) | 86.3 (77.5–95.1) | 63.8 (47.7–79.9) | 24.6 (2.6–46.5) |
| PD n = 127 (39.8%) | 11 (9.0–13.0) | 41.3 (31.9–50.7) | 14.7 (7.4–22.0) | 10.1 (3.4–16.8) |
| DC n = 192 (60.2%) | not reached | 91.3 (87.0–95.6) | 81.0 (73.7–88.3) | 64.6 (53.2–76) |
| PD-1 monotherapy n = 174 (66.2%) | 26 (19.7–32.3) | 71.1 (64.0–78.2) | 53.3 (45.1–61.5) | 41.3 (32.1–50.5) |
| PD-1 + CTLA4 n = 145 (54.6%) | 31 (17.2–44.8) | 72.8 (65–80.6) | 54.5 (42.9–66.1) | 42.5 (24.1–60.9) |
| Best Response | Median PFS (Months; 95% CI) | PFS (%; 95% CI) | ||
|---|---|---|---|---|
| 1-Year | 2-Year | 3-Year | ||
| CR n = 50 (15.7%) | Not reached | 87.6 (78.4–96.8) | 81.2 (68.9–93.5) | 72.2 (52.2–92.2) |
| PR n = 80 (25.1%) | 37 (14.97–59.03) | 74.4 (64.2–85.0) | 62.7 (50.0–75.4) | 62.7 (50.0–75.4) |
| SD n = 62 (19.4%) | 12 (8.97–15.03) | 43.0 (29.3–56.7) | 21.8 (6.3–37.3) | - |
| PD n = 127 (39.8%) | 4 (3.56–4.44) | 8.7 (3.8–13.6) | 3.2 (0–6.5) | 1.1 (0–3.1) |
| DC n = 192(60.2%) | 33 (20.4–45.6) | 68.1 (61.0–75.2) | 56.2 (51.8–64.8) | 48.7 (37.7–59.7) |
| PD-1 monotherapy n = 174 (66.2%) | 8 (5.5–10.5) | 40.3 (32.7–47.9) | 30.5 (23.1–37.9) | 24.1 (16.3–31.9) |
| PD-1 + CTLA4 n = 145 (54.6%) | 9 (1.8–16.2) | 48.5 (40.1–56.9) | 39 (29.2–78.8) | - |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amaral, T.; Seeber, O.; Mersi, E.; Sanchez, S.; Thomas, I.; Meiwes, A.; Forschner, A.; Leiter, U.; Eigentler, T.; Keim, U.; et al. Primary Resistance to PD-1-Based Immunotherapy—A Study in 319 Patients with Stage IV Melanoma. Cancers 2020, 12, 1027. https://doi.org/10.3390/cancers12041027
Amaral T, Seeber O, Mersi E, Sanchez S, Thomas I, Meiwes A, Forschner A, Leiter U, Eigentler T, Keim U, et al. Primary Resistance to PD-1-Based Immunotherapy—A Study in 319 Patients with Stage IV Melanoma. Cancers. 2020; 12(4):1027. https://doi.org/10.3390/cancers12041027
Chicago/Turabian StyleAmaral, Teresa, Olivia Seeber, Edgar Mersi, Stephanie Sanchez, Ioannis Thomas, Andreas Meiwes, Andrea Forschner, Ulrike Leiter, Thomas Eigentler, Ulrike Keim, and et al. 2020. "Primary Resistance to PD-1-Based Immunotherapy—A Study in 319 Patients with Stage IV Melanoma" Cancers 12, no. 4: 1027. https://doi.org/10.3390/cancers12041027
APA StyleAmaral, T., Seeber, O., Mersi, E., Sanchez, S., Thomas, I., Meiwes, A., Forschner, A., Leiter, U., Eigentler, T., Keim, U., & Garbe, C. (2020). Primary Resistance to PD-1-Based Immunotherapy—A Study in 319 Patients with Stage IV Melanoma. Cancers, 12(4), 1027. https://doi.org/10.3390/cancers12041027