Current Role of Total Laryngectomy in the Era of Organ Preservation


{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
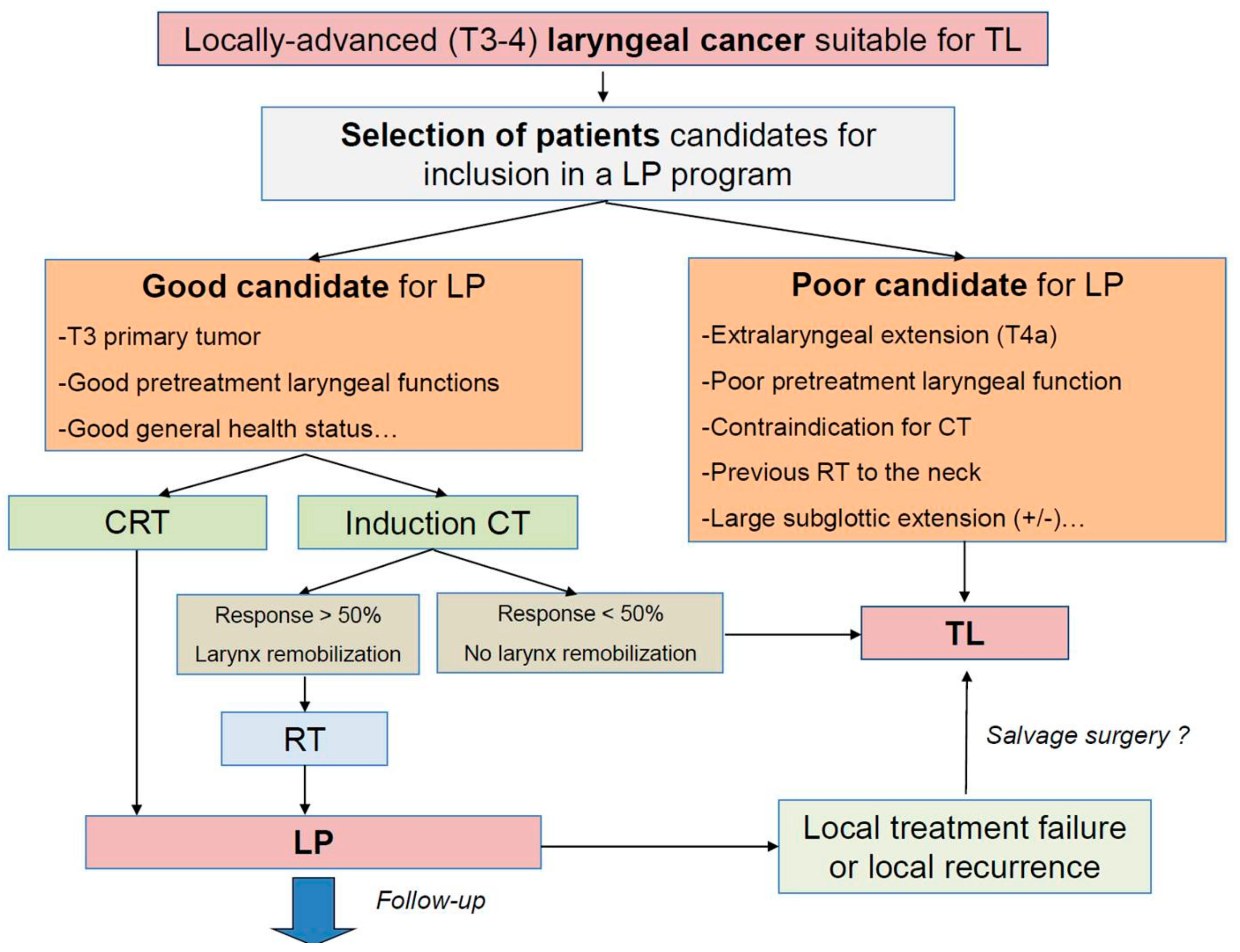
2. Larynx Preservation Strategies
3. Total Laryngectomy as a Primary Therapeutic Option
3.1. T4a Primary Tumors
3.2. Irreversible Loss of Laryngeal Functions
3.3. Subglottic Tumor Subsite or Extension
3.4. Contraindications for a Larynx Preservation Approach
4. Total Laryngectomy as a Salvage Surgical Procedure
5. Total Laryngectomy as a Functional Surgical Procedure
6. Functional Results and Quality of Life after Total Laryngectomy
7. Conclusions
Funding
Conflicts of Interest
Abbreviations
| HNSCC | head and neck squamous cell carcinoma |
| LC | laryngeal cancer |
| TLM | transoral laser microsurgery |
| TROS | transoral robotic surgery |
| RT | radiotherapy |
| IMRT | intensity-modulated radiation therapy |
| TL | total laryngectomy |
| LP | larynx preservation |
| CT | chemotherapy |
| CRT | concurrent chemoradiotherapy |
| SSIs | silent speech interfaces |
| RTOG | Radiation Therapy Oncology Group |
| QoL | quality of life |
| PET | positron emission tomography |
References
- Pezzuto, F.; Buonaguro, L.; Caponigro, F.; Ionna, F.; Starita, N.; Annunziata, C.; Buonaguro, F.M.; Tornesello, M.L. Update on Head and Neck Cancer: Current Knowledge on Epidemiology, Risk Factors, Molecular Features and Novel Therapies. Oncology 2015, 89, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Cohen, N.; Fedewa, S.; Chen, A.Y. Epidemiology and Demographics of the Head and Neck Cancer Population. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 381–395. [Google Scholar] [CrossRef] [PubMed]
- Rudolph, E.; Dyckhoff, G.; Becher, H.; Dietz, A.; Ramroth, H. Effects of tumour stage, comorbidity and therapy on survival of laryngeal cancer patients: A systematic review and a meta-analysis. Eur. Arch. Oto-Rhino-Laryngol. 2010, 268, 165–179. [Google Scholar] [CrossRef] [PubMed]
- Dawson, C.; Pracy, P.; Patterson, J.; Paleri, V. Rehabilitation following open partial laryngeal surgery: Key issues and recommendations from the UK evidence based meeting on laryngeal cancer. J. Laryngol. Otol. 2019, 133, 177–182. [Google Scholar] [CrossRef]
- Piazza, C.; Paderno, A.; Grazioli, P.; Del Bon, F.; Montalto, N.; Perotti, P.; Morello, R.; Filauro, M.; Nicolai, P.; Peretti, G. Laryngeal exposure and margin status in glottic cancer treated by transoral laser microsurgery. Laryngoscope 2017, 128, 1146–1151. [Google Scholar] [CrossRef]
- Gorphe, P. A Contemporary Review of Evidence for Transoral Robotic Surgery in Laryngeal Cancer. Front. Oncol. 2018, 8. [Google Scholar] [CrossRef]
- Jirkovska, M.; Novak, T.; Malinova, B.; Lohynska, R. Three-dimensional conformal radiotherapy versus intensity modulated radiotherapy with simultaneous integrated boost in the treatment of locally advanced head and neck carcinoma. Neoplasma 2019, 66, 830–838. [Google Scholar] [CrossRef]
- Zumsteg, Z.S.; Riaz, N.; Jaffery, S.; Hu, M.; Gelblum, D.; Zhou, Y.; Mychalczak, B.; Zelefsky, M.J.; Wolden, S.; Rao, S.; et al. Carotid sparing intensity-modulated radiation therapy achieves comparable locoregional control to conventional radiotherapy in T1-2N0 laryngeal carcinoma. Oral Oncol. 2015, 51, 716–723. [Google Scholar] [CrossRef][Green Version]
- Babin, E.; Blanchard, D.; Hitier, M. Management of total laryngectomy patients over time: From the consultation announcing the diagnosis to long term follow-up. Eur. Arch. Oto-Rhino-Laryngol. 2011, 268, 1407–1419. [Google Scholar] [CrossRef]
- Bozec, A.; Poissonnet, G.; Chamorey, E.; Demard, F.; Santini, J.; Peyrade, F.; Ortholan, C.; Benezery, K.; Thariat, J.; Sudaka, A.; et al. Results of vocal rehabilitation using tracheoesophageal voice prosthesis after total laryngectomy and their predictive factors. Eur. Arch. Oto-Rhino-Laryngol. 2009, 267, 751–758. [Google Scholar] [CrossRef]
- Lefebvre, J.L. Larynx preservation. Curr. Opin. Oncol. 2012, 24, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Licitra, L.; Bonomo, P.; Sanguineti, G.; Bacigalupo, A.; Baldi, G.G.; Valerini, S.; Bruzzi, P. Different View on Larynx Preservation Evidence-Based Treatment Recommendations. J. Clin. Oncol. 2018, 36, 1376–1377. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.A.; Ismaila, N.; Lewin, J.S.; Nathan, C.A.; Adelstein, D.J.; Eisbruch, A.; Fass, G.; Fisher, S.G.; Laurie, S.A.; Le, Q.T.; et al. Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1143–1169. [Google Scholar] [CrossRef] [PubMed]
- Jones, T.M.; De, M.; Foran, B.; Harrington, K.; Mortimore, S. Laryngeal cancer: United Kingdom National Multidisciplinary guidelines. J. Laryngol. Otol. 2016, 130, S75–S82. [Google Scholar] [CrossRef]
- Forastiere, A.A.; Zhang, Q.; Weber, R.S.; Maor, M.H.; Goepfert, H.; Pajak, T.F.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; et al. Long-Term Results of RTOG 91-11: A Comparison of Three Nonsurgical Treatment Strategies to Preserve the Larynx in Patients With Locally Advanced Larynx Cancer. J. Clin. Oncol. 2013, 31, 845–852. [Google Scholar] [CrossRef]
- Forastiere, A.A.; Goepfert, H.; Pajak, T.F.; Weber, R.; Glisson, B.S.; Ridge, J.A.; Chao, C.; Leaf, A.; Ensley, J.; Cooper, J.; et al. Concurrent Chemotherapy and Radiotherapy for Organ Preservation in Advanced Laryngeal Cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef]
- Forastiere, A.A.; Ismaila, N.; Wolf, G.T. Use of Larynx-Preservation Strategies in the Treatment of Laryngeal Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update Summary. J. Clin. Oncol. 2018, 14, 123–128. [Google Scholar]
- Pointreau, Y.; Garaud, P.; Chapet, S.; Sire, C.; Tuchais, C.; Tortochaux, J.; Faivre, S.; Guerrif, S.; Alfonsi, M.; Calais, G. Randomized trial of induction chemotherapy with cisplatin and 5-fluorouracil with or without docetaxel for larynx preservation. J. Natl. Cancer Inst. 2009, 101, 498–506. [Google Scholar] [CrossRef]
- Janoray, G.; Pointreau, Y.; Garaud, P.; Chapet, S.; Alfonsi, M.; Sire, C.; Jadaud, E.; Calais, G. Long-Term Results of a Multicenter Randomized Phase III Trial of Induction Chemotherapy With Cisplatin, 5-fluorouracil, ± Docetaxel for Larynx Preservation. J. Natl. Cancer Inst. 2015, 108. [Google Scholar] [CrossRef]
- Lefebvre, J.-L.; Pointreau, Y.; Rolland, F.; Alfonsi, M.; Baudoux, A.; Sire, C.; De Raucourt, D.; Malard, O.; Degardin, M.; Tuchais, C.; et al. Induction Chemotherapy Followed by Either Chemoradiotherapy or Bioradiotherapy for Larynx Preservation: The TREMPLIN Randomized Phase II Study. J. Clin. Oncol. 2013, 31, 853–859. [Google Scholar] [CrossRef]
- Choi, Y.S.; Park, S.G.; Song, E.-K.; Cho, S.-H.; Park, M.-R.; Park, K.U.; Lee, K.H.; Song, I.-C.; Lee, H.J.; Jo, D.-Y.; et al. Comparison of the therapeutic effects of total laryngectomy and a larynx-preservation approach in patients with T4a laryngeal cancer and thyroid cartilage invasion: A multicenter retrospective review. Head Neck 2016, 38, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; Halpern, M. Factors Predictive of Survival in Advanced Laryngeal Cancer. Arch. Otolaryngol.-Head Neck Surg. 2007, 133, 1270–1276. [Google Scholar] [CrossRef] [PubMed]
- Grover, S.; Swisher-McClure, S.; Mitra, N.; Li, J.; Cohen, R.B.; Ahn, P.H.; Lukens, J.N.; Chalian, A.A.; Weinstein, G.S.; O’Malley, B.W.; et al. Total Laryngectomy Versus Larynx Preservation for T4a Larynx Cancer: Patterns of Care and Survival Outcomes. Int. J. Radiat. Oncol. 2015, 92, 594–601. [Google Scholar] [CrossRef] [PubMed]
- Gourin, C.G.; Conger, B.T.; Sheils, W.C.; Bilodeau, P.A.; Coleman, T.A.; Porubsky, E.S. The Effect of treatment on survival in patients with advanced laryngeal carcinoma. Laryngoscope 2009, 119, 1312–1317. [Google Scholar] [CrossRef]
- Rosenthal, D.I.; Mohamed, A.S.R.; Weber, R.S.; Garden, A.S.; Sevak, P.R.; Kies, M.S.; Morrison, W.H.; Lewin, J.; El-Naggar, A.K.; Ginsberg, L.E.; et al. Long-term outcomes after surgical or nonsurgical initial therapy for patients with T4 squamous cell carcinoma of the larynx: A 3-decade survey. Cancer 2015, 121, 1608–1619. [Google Scholar] [CrossRef]
- Roux, M.; Dassonville, O.; Ettaiche, M.; Chamorey, E.; Poissonnet, G.; Bozec, A. Primary total laryngectomy and pharyngolaryngectomy in T4 pharyngolaryngeal cancers: Oncologic and functional results and prognostic factors. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2017, 134, 151–154. [Google Scholar] [CrossRef]
- Mimica, X.; Hanson, M.; Patel, S.G.; McGill, M.; McBride, S.; Lee, N.; Dunn, L.A.; Cracchiolo, J.R.; Shah, J.P.; Wong, R.J.; et al. Salvage surgery for recurrent larynx cancer. Head Neck 2019, 41, 3906–3915. [Google Scholar] [CrossRef]
- Milliet, F.; Gal, J.; Chamorey, E.; Dassonville, O.; Poissonnet, G.; Peyrade, F.; Benezery, K.; Hechema, R.; Sudaka, A.; Sanchez-Luini, M.; et al. Total pharyngolaryngectomy in the elderly: The impact of age on postoperative complications and oncologic and functional outcomes. Surg. Oncol. 2018, 27, 767–772. [Google Scholar] [CrossRef]
- Levy, A.; Blanchard, P.; Temam, S.; Maison, M.M.; Janot, F.; Mirghani, H.; Bidault, F.; Guigay, J.; Lusinchi, A.; Bourhis, J.; et al. Squamous cell carcinoma of the larynx with subglottic extension: Is larynx preservation possible? Strahlenther. Onkol. 2014, 190, 654–660. [Google Scholar] [CrossRef]
- Laccourreye, O.; Malinvaud, D.; Menard, M.; Consoli, S.; Giraud, P.; Bonfils, P. Total laryngectomy or laryngeal preservation for advanced laryngeal cancer. Impact of the functional risk upon the patient’s preferences. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2014, 131, 93–97. [Google Scholar] [CrossRef]
- De Virgilio, A.; Pellini, R.; Mercante, G.; Cristalli, G.; Manciocco, V.; Giannarelli, D.; Spriano, G. Supracricoid partial laryngectomy for radiorecurrent laryngeal cancer: A systematic review of the literature and meta-analysis. Eur. Arch. Oto-Rhino-Laryngol. 2018, 275, 1671–1680. [Google Scholar] [CrossRef] [PubMed]
- Lin, D.; Lam, A.; Warner, L.; Paleri, V. Elective neck dissection in patients with radio-recurrent and radio-residual squamous cell carcinoma of the larynx undergoing salvage total laryngectomy: Systematic review and meta-analysis. Head Neck 2019, 41, 4026–4035. [Google Scholar] [CrossRef] [PubMed]
- Asimakopoulos, P.; Thompson, C.S.G.; Hogg, G.E.; Evans, A.S.; Adamson, R.M.; Vernham, G.A.; Nixon, I. Surgical and pathological outcomes of elective neck dissection during salvage total laryngectomy. Clin. Otolaryngol. 2018, 44, 375–378. [Google Scholar] [CrossRef] [PubMed]
- Zafereo, M. Surgical Salvage of Recurrent Cancer of the Head and Neck. Curr. Oncol. Rep. 2014, 16. [Google Scholar] [CrossRef] [PubMed]
- Mehanna, H.; Kong, A.; Ahmed, S. Recurrent head and neck cancer: United Kingdom National Multidisciplinary Guidelines. J. Laryngol. Otol. 2016, 130, S181–S190. [Google Scholar] [CrossRef]
- Li, M.; Lorenz, R.R.; Khan, M.J.; Burkey, B.B.; Adelstein, D.J.; Greskovich, J.F.; Koyfman, S.A.; Scharpf, J. Salvage Laryngectomy in Patients with Recurrent Laryngeal Cancer in the Setting of Nonoperative Treatment Failure. Otolaryngol. Neck Surg. 2013, 149, 245–251. [Google Scholar] [CrossRef]
- Birkeland, A.C.; Beesley, L.J.; Bellile, E.; Rosko, A.J.; Hoesli, R.; Chinn, S.B.; Shuman, A.G.; Prince, M.E.; Wolf, G.T.; Bradford, C.R.; et al. Predictors of survival after total laryngectomy for recurrent/persistent laryngeal squamous cell carcinoma. Head Neck 2017, 39, 2512–2518. [Google Scholar] [CrossRef]
- Pescetto, B.; Gál, J.; Chamorey, E.; Dassonville, O.; Poissonnet, G.; Bozec, A. Role of supracricoid partial laryngectomy with cricohyoidoepiglottopexy in glottic carcinoma with anterior commissure involvement. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2018, 135, 249–253. [Google Scholar] [CrossRef]
- Benito, J.; Holsinger, F.C.; Martin, A.P.; Garcia, M.; Weinstein, G.S.; Laccourreye, O. Aspiration after supracricoid partial laryngectomy: Incidence, risk factors, management, and outcomes. Head Neck 2010, 33, 679–685. [Google Scholar] [CrossRef]
- Zacharek, M.A.; Pasha, R.; Meleca, R.J.; Dworkin, J.P.; Stachler, R.J.; Jacobs, J.R.; Marks, S.C.; Garfield, I. Functional Outcomes After Supracricoid Laryngectomy. Laryngoscope 2001, 111, 1558–1564. [Google Scholar] [CrossRef]
- Ward, M.C.; Adelstein, D.J.; Bhateja, P.; Nwizu, T.I.; Scharpf, J.; Houston, N.; Lamarre, E.D.; Lorenz, R.; Burkey, B.B.; Greskovich, J.F.; et al. Severe late dysphagia and cause of death after concurrent chemoradiation for larynx cancer in patients eligible for RTOG 91-11. Oral Oncol. 2016, 57, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Anschuetz, L.; Shelan, M.; Dematte, M.; Schubert, A.D.; Giger, R.; Elicin, O. Long-term functional outcome after laryngeal cancer treatment. Radiat. Oncol. 2019, 14, 101. [Google Scholar] [CrossRef] [PubMed]
- Raol, N.; Hutcheson, K.A.; Lewin, J.S.; Kupferman, M.E. Surgical Management of the Non-functional Larynx after Organ Preservation Therapy. J. Otol. Rhinol. 2013, 2, 1. [Google Scholar] [CrossRef]
- Maddox, P.T.; Davies, L. Trends in Total Laryngectomy in the Era of Organ Preservation. Otolaryngol. Neck Surg. 2012, 147, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Zenga, J.; Goldsmith, T.; Bunting, G.; Deschler, D.G. State of the art: Rehabilitation of speech and swallowing after total laryngectomy. Oral Oncol. 2018, 86, 38–47. [Google Scholar] [CrossRef]
- Búa, B.A.; Pendleton, H.; Westin, U.; Rydell, R. Voice and swallowing after total laryngectomy. Acta Oto-Laryngol. 2017, 138, 170–174. [Google Scholar]
- Fakhry, N.; Chamorey, E.; Michel, J.; Collet, C.; Santini, L.; Poissonnet, G.; Santini, J.; Dessi, P.; Giovanni, A.; Dassonville, O.; et al. Salvage Circular Laryngopharyngectomy and Radial Forearm Free Flap for Recurrent Hypopharyngeal Cancer. Laryngoscope 2013, 123, 910–915. [Google Scholar] [CrossRef]
- Tang, C.G.; Sinclair, C.F. Voice Restoration After Total Laryngectomy. Otolaryngol. Clin. N. Am. 2015, 48, 687–702. [Google Scholar] [CrossRef]
- Mayo-Yanez, M. Analysis of Factors Affecting the Longevity of Voice Prosthesis Following Total Laryngectomy with a Review of Literature. Indian J. Surg. Oncol. 2019, 10, 219. [Google Scholar] [CrossRef]
- Galli, A.; Giordano, L.; Biafora, M.; Tulli, M.; Di Santo, D.; Bussi, M. Voice prosthesis rehabilitation after total laryngectomy: Are satisfaction and quality of life maintained over time? Acta Otorhinolaryngol. Ital. 2019, 39, 162–168. [Google Scholar] [CrossRef]
- Gitomer, S.A.; Hutcheson, K.; Christianson, B.L.; Samuelson, M.B.; Barringer, D.A.; Roberts, D.B.; Hessel, A.C.; Weber, R.S.; Lewin, J.; Zafereo, M.; et al. Influence of timing, radiation, and reconstruction on complications and speech outcomes with tracheoesophageal puncture. Head Neck 2016, 38, 1765–1771. [Google Scholar] [CrossRef] [PubMed]
- Hutcheson, K.; Lewin, J.; Sturgis, E.M.; Risser, J. Multivariable analysis of risk factors for enlargement of the tracheoesophageal puncture after total laryngectomy. Head Neck 2011, 34, 557–567. [Google Scholar] [CrossRef] [PubMed]
- Dewey, E.H.; Castro, J.R.; Mojica, J.; Lazarus, C.L.; Su, H.K.; Alpert, E.H.; Dos Reis, L.L.; Urken, M.L. Reconstruction of expanding tracheoesophageal fistulae in post-radiation therapy patients who undergo total laryngectomy with a bipaddled radial forearm free flap: Report of 8 cases. Head Neck 2015, 38, E172–E178. [Google Scholar] [CrossRef] [PubMed]
- Patel, R.S.; Mohr, T.; Hartman, C.; Stach, C.; Sikora, A.G.; Zevallos, J.P.; Sandulache, V.C. Tracheoesophageal Prosthesis Use Is Associated With Improved Overall Quality of Life in Veterans With Laryngeal Cancer. Ann. Otol. Rhinol. Laryngol. 2018, 127, 421–428. [Google Scholar] [CrossRef] [PubMed]
- Luu, K.; Chang, B.A.; Valenzuela, D.; Anderson, D. Primary versus secondary tracheoesophageal puncture for voice rehabilitation in laryngectomy patients: A systematic review. Clin. Otolaryngol. 2018, 43, 1250–1259. [Google Scholar] [CrossRef]
- Bozec, A.; Schultz, P.; Gal, J.; Chamorey, E.; Chateau, Y.; Dassonville, O.; Poissonnet, G.; Demard, F.; Peyrade, F.; Saada, E.; et al. Evolution and predictive factors of quality of life in patients undergoing oncologic surgery for head and neck cancer: A prospective multicentric study. Surg. Oncol. 2019, 28, 236–242. [Google Scholar] [CrossRef]
- Singer, S.; Danker, H.; Guntinas-Lichius, O.; Oeken, J.; Pabst, F.; Schock, J.; Vogel, H.-J.; Meister, E.F.; Wulke, C.; Dietz, A. Quality of life before and after total laryngectomy: Results of a multicenter prospective cohort study. Head Neck 2013, 36, 359–368. [Google Scholar] [CrossRef]
- Sanabria, A.; Sanchez, D.; Chala, A.; Alvarez, A. Quality of life in patients with larynx cancer in Latin America: Comparison between laryngectomy and organ preservation protocols. Ear Nose Throat J. 2018, 97, 83–90. [Google Scholar] [CrossRef]
- Hanna, E.; Sherman, A.; Cash, D.; Adams, D.; Vural, E.; Fan, C.-Y.; Suen, J.Y. Quality of Life for Patients Following Total Laryngectomy vs Chemoradiation for Laryngeal Preservation. Arch. Otolaryngol.-Head Neck Surg. 2004, 130, 875. [Google Scholar] [CrossRef]
- Fung, K.; Lyden, T.H.; Lee, J.; Urba, S.G.; Worden, F.; Eisbruch, A.; Tsien, C.; Bradford, C.R.; Chepeha, D.B.; Hogikyan, N.D.; et al. Voice and swallowing outcomes of an organ-preservation trial for advanced laryngeal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 1395–1399. [Google Scholar] [CrossRef]
- Oridate, N.; Homma, A.; Suzuki, S.; Nakamaru, Y.; Suzuki, F.; Hatakeyama, H.; Taki, S.; Sakashita, T.; Nishizawa, N.; Furuta, Y.; et al. Voice-Related Quality of Life After Treatment of Laryngeal Cancer. Arch. Otolaryngol.-Head Neck Surg. 2009, 135, 363–368. [Google Scholar] [CrossRef] [PubMed]
- Heutte, N.; Abouzayd, M.; Plisson, L.; Trocmé, M.; Seillier, M.; Christophe, V.; Guittet, L.; Grandazzi, G.; Babin, E. French Therapeutic Education Programme Aimed at Improving the Quality of Life of Laryngectomised Patients and their Close Relations: The Three Stages (Observational and Interventional Randomised) of the Study “PETAL”. J. Cancer Educ. 2018, 34, 823–830. [Google Scholar] [CrossRef] [PubMed]
- Bozec, A.; Schultz, P.; Gal, J.; Chamorey, E.; Chateau, Y.; Dassonville, O.; Poissonnet, G.; Peyrade, F.; Saada, E.; Guigay, J.; et al. Evaluation of the information given to patients undergoing total pharyngolaryngectomy and quality of life: A prospective multicentric study. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 2531–2539. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.; Cao, B.; Mau, T.; Wang, J. Speaker-Independent Silent Speech Recognition From Flesh-Point Articulatory Movements Using an LSTM Neural Network. IEEE/ACM Trans. Audio Speech Lang. Process. 2017, 25, 2323–2336. [Google Scholar] [CrossRef]



© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bozec, A.; Culié, D.; Poissonnet, G.; Dassonville, O. Current Role of Total Laryngectomy in the Era of Organ Preservation. Cancers 2020, 12, 584. https://doi.org/10.3390/cancers12030584
Bozec A, Culié D, Poissonnet G, Dassonville O. Current Role of Total Laryngectomy in the Era of Organ Preservation. Cancers. 2020; 12(3):584. https://doi.org/10.3390/cancers12030584
Chicago/Turabian StyleBozec, Alexandre, Dorian Culié, Gilles Poissonnet, and Olivier Dassonville. 2020. "Current Role of Total Laryngectomy in the Era of Organ Preservation" Cancers 12, no. 3: 584. https://doi.org/10.3390/cancers12030584
APA StyleBozec, A., Culié, D., Poissonnet, G., & Dassonville, O. (2020). Current Role of Total Laryngectomy in the Era of Organ Preservation. Cancers, 12(3), 584. https://doi.org/10.3390/cancers12030584