Visceral Adipose Tissue Radiodensity Is Linked to Prognosis in Hepatocellular Carcinoma Patients Treated with Selective Internal Radiation Therapy


Abstract
1. Introduction
2. Results
2.1. Baseline Characteristics of Patients
2.2. Features Associated with Mortality in HCC Patients Post-SIRT
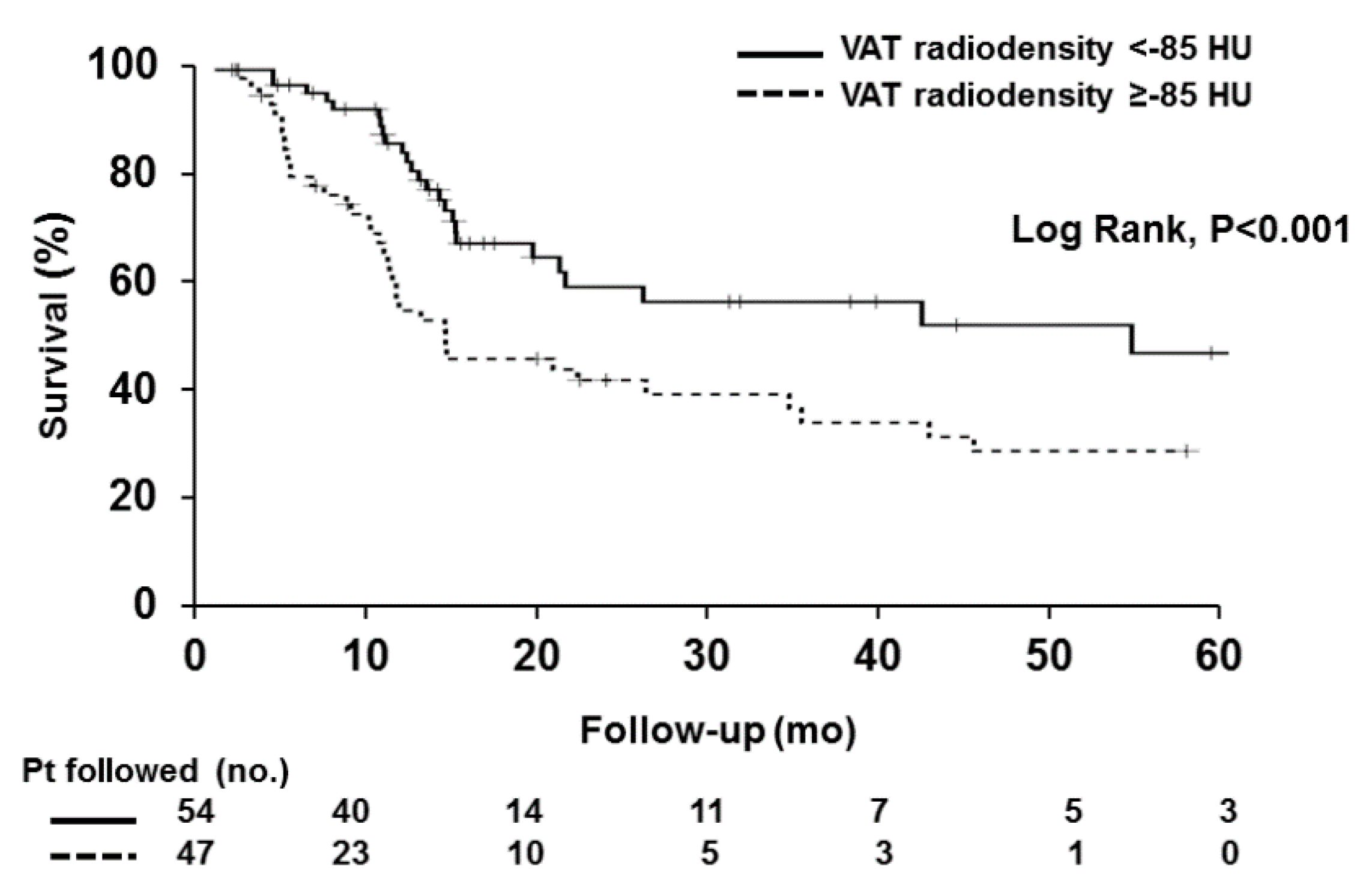
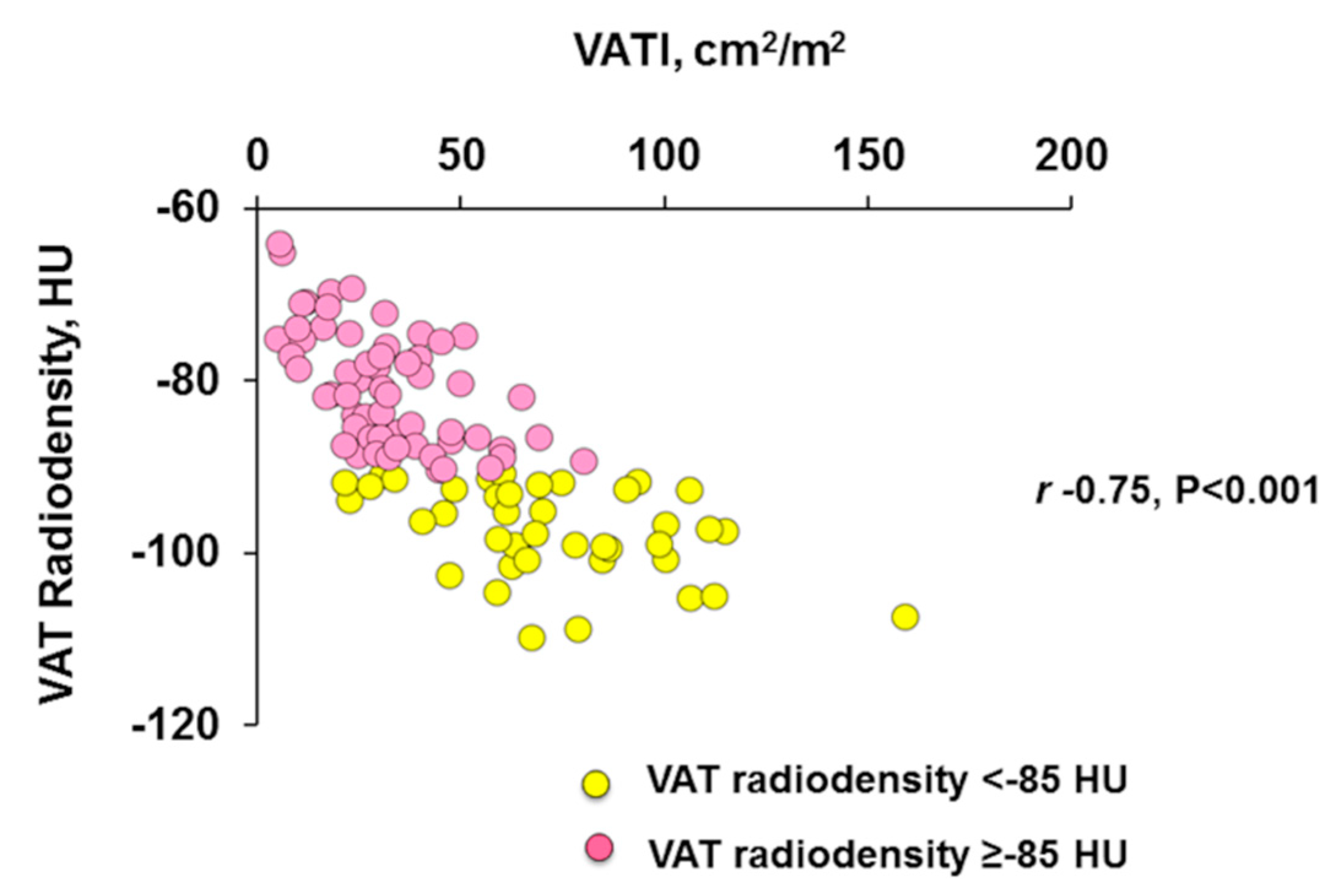
2.3. Characteristics of Patients with High VAT Radiodensity
2.4. Association of VAT Radiodensity with Response Assessment and Toxicities
2.5. Performance High VAT Radiodensity to Predict SAEs after SIRT
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. SIRT Procedure, Toxicities, and Response Assessment
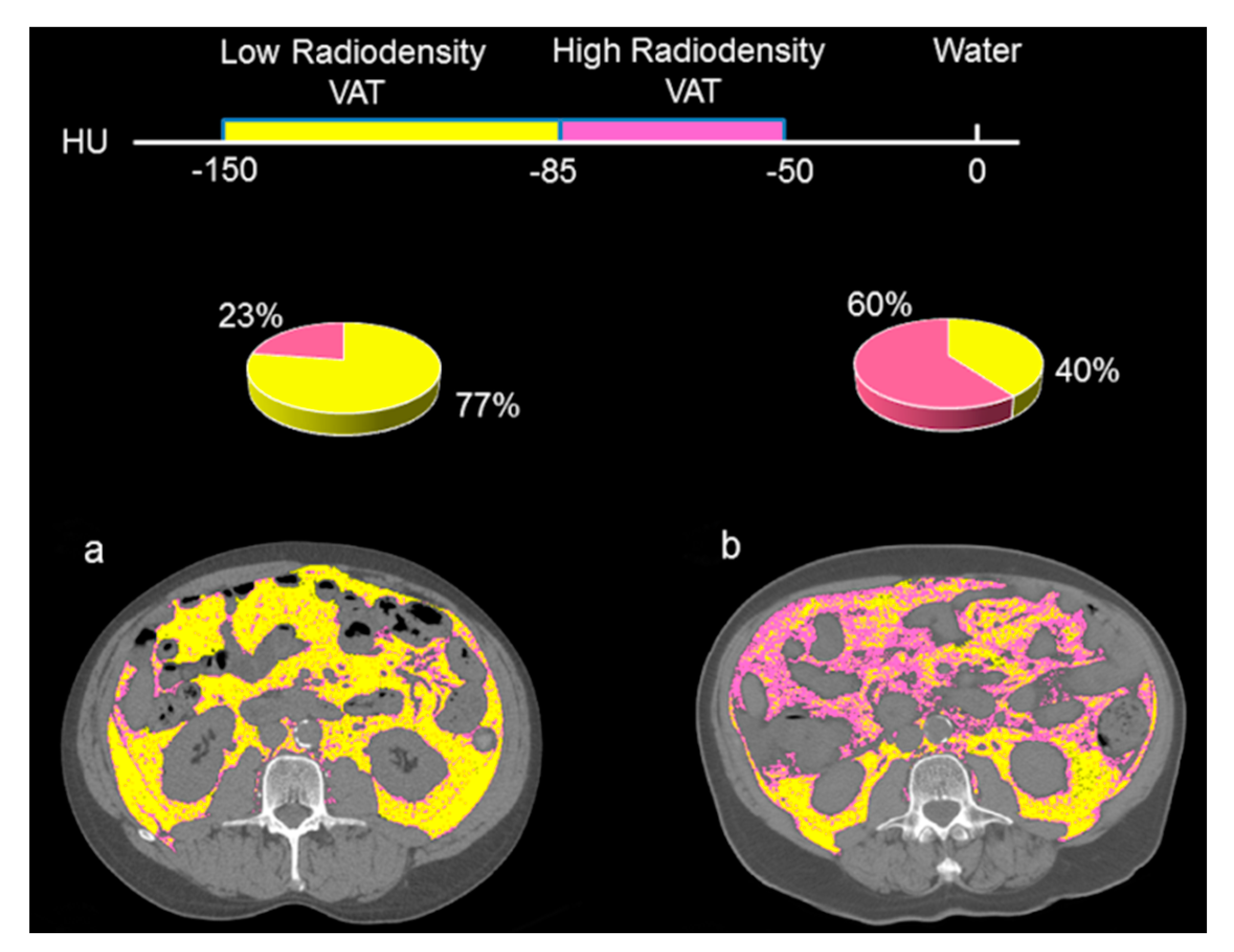
4.3. CT Image Analysis
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Han, K.H. Transarterial chemoembolization versus transarterial radioembolization in hepatocellular carcinoma: Optimization of selecting treatment modality. Hepatol. Int. 2016, 10, 883–892. [Google Scholar] [CrossRef]
- Clark, T.; Maximin, S.; Meier, J.; Pokharel, S.; Bhargava, P. Hepatocellular Carcinoma: Review of Epidemiology, Screening, Imaging Diagnosis, Response Assessment, and Treatment. Curr. Probl. Diagn. Radiol. 2015, 44, 479–486. [Google Scholar]
- Gabrielson, A.; Miller, A.; Banovac, F.; Kim, A.; He, A.R.; Unger, K. Outcomes and Predictors of Toxicity after Selective Internal Radiation Therapy Using Yttrium-90 Resin Microspheres for Unresectable Hepatocellular Carcinoma. Front. Oncol. 2015, 5, 292. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, N.; Nakagawa, H.; Kudo, Y.; Tateishi, R.; Taguri, M.; Watadani, T.; Nakagomi, R.; Kondo, M.; Nakatsuka, T.; Minami, T.; et al. Sarcopenia, intramuscular fat deposition, and visceral adiposity independently predict the outcomes of hepatocellular carcinoma. J. Hepatol. 2015, 63, 131–140. [Google Scholar] [CrossRef]
- Gui, B.; Weiner, A.A.; Nosher, J.; Lu, S.E.; Foltz, G.M.; Hasan, O.; Kim, S.K.; Gendel, V.; Mani, N.B.; Carpizo, D.R.; et al. Assessment of the Albumin-Bilirubin (ALBI) Grade as a Prognostic Indicator for Hepatocellular Carcinoma Patients Treated With Radioembolization. Am. J. Clin. Oncol. 2018, 41, 861–866. [Google Scholar] [CrossRef] [PubMed]
- Jun, C.H.; Yoon, J.H.; Cho, E.; Shin, S.S.; Cho, S.B.; Kim, H.J.; Park, C.H.; Kim, H.S.; Choi, S.K.; Rew, J.S. Barcelona clinic liver cancer-stage C hepatocellular carcinoma: A novel approach to subclassification and treatment. Medicine 2017, 96, e6745. [Google Scholar] [CrossRef]
- Shen, W.; Punyanitya, M.; Wang, Z.; Gallagher, D.; St-Onge, M.P.; Albu, J.; Heymsfield, S.B.; Heshka, S. Total body skeletal muscle and adipose tissue volumes: Estimation from a single abdominal cross-sectional image. J. Appl. Physiol. 2004, 97, 2333–2338. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y.; Kim, D.; Han, S.; Chon, Y.E.; Lee, Y.B.; Kim, M.N.; Lee, J.H.; Park, H.; Rim, K.S.; Hwang, S.G.; et al. Sarcopenia Predicts Prognosis in Patients with Newly Diagnosed Hepatocellular Carcinoma, Independent of Tumor Stage and Liver Function. Cancer Res. Treat. 2018, 50, 843–851. [Google Scholar]
- Montano-Loza, A.J.; Mazurak, V.C.; Ebadi, M.; Meza-Junco, J.; Sawyer, M.B.; Baracos, V.E.; Kneteman, N. Visceral adiposity increases risk for hepatocellular carcinoma in male patients with cirrhosis and recurrence after liver transplant. Hepatology 2018, 67, 914–923. [Google Scholar] [CrossRef]
- Carey, E.J.; Lai, J.C.; Wang, C.W.; Dasarathy, S.; Lobach, I.; Montano-Loza, A.J.; Dunn, M.A. Fitness, Life Enhancement, and Exercise in Liver Transplantation Consortium. A multicenter study to define sarcopenia in patients with end-stage liver disease. Liver Transplant. 2017, 23, 625–633. [Google Scholar] [CrossRef] [PubMed]
- Parikh, N.D.; Zhang, P.; Singal, A.G.; Derstine, B.A.; Krishnamurthy, V.; Barman, P.; Waljee, A.K.; Su, G.L. Body Composition Predicts Survival in Patients with Hepatocellular Carcinoma Treated with Transarterial Chemoembolization. Cancer Res. Treat. 2018, 50, 530–537. [Google Scholar] [CrossRef] [PubMed]
- European Association for The Study of The Liver; European Organisation for Research and Treatment of Cancer. EASL-EORTC clinical practice guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2012, 56, 908–943. [Google Scholar] [CrossRef] [PubMed]
- Ripoll, C.; Groszmann, R.; Garcia-Tsao, G.; Grace, N.; Burroughs, A.; Planas, R.; Escorsell, A.; Garcia-Pagan, J.C.; Makuch, R.; Patch, D.; et al. Hepatic venous pressure gradient predicts clinical decompensation in patients with compensated cirrhosis. Gastroenterology 2007, 133, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Gifford, A.; Walker, R.C.; Towse, T.F.; Brian Welch, E. Correlations between quantitative fat-water magnetic resonance imaging and computed tomography in human subcutaneous white adipose tissue. J. Med. Imaging 2015, 2, 046001. [Google Scholar] [CrossRef] [PubMed]
- Weyer, C.; Foley, J.E.; Bogardus, C.; Tataranni, P.A.; Pratley, R.E. Enlarged subcutaneous abdominal adipocyte size, but not obesity itself, predicts type II diabetes independent of insulin resistance. Diabetologia 2000, 43, 1498–1506. [Google Scholar] [CrossRef]
- Din, M.U.; Raiko, J.; Saari, T.; Saunavaara, V.; Kudomi, N.; Solin, O.; Parkkola, R.; Nuutila, P.; Virtanen, K.A. Human Brown Fat Radiodensity Indicates Underlying Tissue Composition and Systemic Metabolic Health. J. Clin. Endocrinol. Metab. 2017, 102, 2258–2267. [Google Scholar] [CrossRef]
- Ahmadi, N.; Hajsadeghi, F.; Conneely, M.; Mingos, M.; Arora, R.; Budoff, M.; Ebrahimi, R. Accurate detection of metabolically active “brown” and “white” adipose tissues with computed tomography. Acad. Radiol. 2013, 20, 1443–1447. [Google Scholar] [CrossRef]
- Petruzzelli, M.; Schweiger, M.; Schreiber, R.; Campos-Olivas, R.; Tsoli, M.; Allen, J.; Swarbrick, M.; Rose-John, S.; Rincon, M.; Robertson, G.; et al. A switch from white to brown fat increases energy expenditure in cancer-associated cachexia. Cell Metab. 2014, 20, 433–447. [Google Scholar] [CrossRef]
- Bhanji, R.A.; Moctezuma-Velazquez, C.; Duarte-Rojo, A.; Ebadi, M.; Ghosh, S.; Rose, C.; Montano-Loza, A.J. Myosteatosis and sarcopenia are associated with hepatic encephalopathy in patients with cirrhosis. Hepatol. Int. 2018, 12, 377–386. [Google Scholar] [CrossRef]
- Kalafateli, M.; Karatzas, A.; Tsiaoussis, G.; Koutroumpakis, E.; Tselekouni, P.; Koukias, N.; Konstantakis, C.; Assimakopoulos, S.; Gogos, C.; Thomopoulos, K.; et al. Muscle fat infiltration assessed by total psoas density on computed tomography predicts mortality in cirrhosis. Ann. Gastroenterol. 2018, 31, 491–498. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, S.G.; Brabandt, B.; Stirnimann, G.; Maurer, M.H.; Berzigotti, A. Adipopenia correlates with higher portal pressure in patients with cirrhosis. Liver Int. 2019, 39, 1672–1681. [Google Scholar] [CrossRef] [PubMed]
- European Association for the Study of the Liver. Electronic address eee, European Association for the Study of the L. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed]
- Meza-Junco, J.; Montano-Loza, A.J.; Liu, D.M.; Sawyer, M.B.; Bain, V.G.; Ma, M.; Owen, R. Locoregional radiological treatment for hepatocellular carcinoma; Which, when and how? Cancer Treat. Rev. 2012, 38, 54–62. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.; Punyanitya, M.; Wang, Z.; Gallagher, D.; St-Onge, M.P.; Albu, J.; Heymsfield, S.B.; Heshka, S. Visceral adipose tissue: Relations between single-slice areas and total volume. Am. J. Clin. Nutr. 2004, 80, 271–278. [Google Scholar] [CrossRef]
- Miller, K.D.; Jones, E.; Yanovski, J.A.; Shankar, R.; Feuerstein, I.; Falloon, J. Visceral abdominal-fat accumulation associated with use of indinavir. Lancet 1998, 351, 871–875. [Google Scholar] [CrossRef]
- Mitsiopoulos, N.; Baumgartner, R.N.; Heymsfield, S.B.; Lyons, W.; Gallagher, D.; Ross, R. Cadaver validation of skeletal muscle measurement by magnetic resonance imaging and computerized tomography. J. Appl. Physiol. 1998, 85, 115–122. [Google Scholar] [CrossRef]
- Paris, M.T.; Furberg, H.F.; Petruzella, S.; Akin, O.; Hötker, A.M.; Mourtzakis, M. Influence of Contrast Administration on Computed Tomography-Based Analysis of Visceral Adipose and Skeletal Muscle Tissue in Clear Cell Renal Cell Carcinoma. JPEN J. Parenter. Enteral Nutr. 2018, 42, 1148–1155. [Google Scholar] [CrossRef]
- Cruz, R.J., Jr.; Dew, M.A.; Myaskovsky, L.; Goodpaster, B.; Fox, K.; Fontes, P.; DiMartini, A. Objective radiologic assessment of body composition in patients with end-stage liver disease: Going beyond the BMI. Transplantation 2013, 95, 617–622. [Google Scholar] [CrossRef]
- Devika, S.; Jeyaseelan, L.; Sebastian, G. Analysis of sparse data in logistic regression in medical research: A newer approach. J. Postgrad. Med. 2016, 62, 26–31. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Univariate | Multivariate | ||||||
|---|---|---|---|---|---|---|---|
| Characteristics | All patients (n = 101) | Censored (n = 36) | Dead (n = 65) | HR (95% CI) | p-value | HR (95% CI) | p-value |
| Sex, male | 89 (88) | 32 (89) | 57 (88) | 0.92 (0.44–1.94) | 0.83 | ||
| Age at SIRT, years | 62 ± 12 | 61 ± 19 | 62 ± 11 | 0.996 (0.98–1.01) | 0.66 | ||
| Cirrhosis etiology | |||||||
| 14 (14) | 5 (14) | 9 (14) | 1.04 (0.51–2.10) | 0.92 | ||
| 31 (31) | 8 (22) | 23 (35) | 2.43 (1.43–4.13) | 0.001 | 2.28 (1.28–4.04) | 0.005 |
| 12 (12) | 3 (8) | 9 (14) | 1.92 (0.86–4.27) | 0.11 | ||
| 21 (21) | 10 (28) | 11 (17) | 0.69 (0.35–1.35) | 0.28 | ||
| 6 (6) | 4 (11) | 2 (3) | 0.23 (0.05–0.94) | 0.04 | 0.88 (0.19–4.16) | 0.87 |
| 17 (17) | 6 (17) | 11 (17) | 0.62 (0.32–1.18) | 0.15 | ||
| Vascular invasion b | 19 (19) | 5 (14) | 14 (22) | 1.78 (0.96–3.32) | 0.07 | ||
| Extrahepatic spread | 4 (4) | 0 (0) | 4 (6) | 1.12 (0.41–3.12) | 0.82 | ||
| ALBI score b | −2.3 ± 0.6 | −2.5 ± 0.5 | -2.2±0.6 | 2.82 (1.78–4.47) | <0.001 | ||
| Child–Pugh b | |||||||
| 69 (68) | 31 (86) | 38 (59) | ||||
| 32 (32) | 5 (14) | 27 (42) | 2.79 (1.68–4.63) | <0.001 | ||
| Number of tumors b | 4 ± 5 | 3 ± 4 | 5±6 | 1.1 (1.02–1.19) | 0.02 | ||
| Largest dimension of tumors | 7 ± 4 | 8 ± 5 | 7 ± 4 | 0.97 (0.87–1.09) | 0.62 | ||
| BCLC stage | |||||||
| 29 (29) | 17 (47) | 12 (19) | ||||
| 47 (46) | 14 (39) | 33 (51) | 2.74 (1.40–5.34) | 0.003 | 2.80 (1.37–5.73) | 0.005 |
| 25 (25) | 5 (14) | 20 (31) | 2.93 (1.42–6.06) | 0.004 | 2.40 (1.07–5.40) | 0.04 |
| Previous treatment | 38 (38) | 8 (22) | 30 (46) | 2.33 (1.41–3.85) | 0.001 | 1.58 (0.90–2.76) | 0.11 |
| Markers of portal hypertension c | 60 (60) | 19 (53) | 41 (63) | 2.07 (1.24–3.45) | 0.005 | 1.38 (0.80–2.37) | 0.25 |
| Body Composition | |||||||
| BMI, kg/m2 | 26 ± 4 | 25 ± 4 | 26 ± 6 | 1.04 (0.97–1.11) | 0.29 | ||
| SMI (cm2/m2) | 47 ± 10 | 47 ± 9 | 48 ± 10 | 1.01 (0.98–1.03) | 0.64 | ||
| VATI (cm2/m2) | 47 ± 30 | 53 ± 35 | 43 ± 27 | 0.996 (0.99–1.004) | 0.32 | ||
| SATI (cm2/m2) | 55 ± 34 | 61 ± 43 | 51 ± 27 | 1.002 (0.99–1.01) | 0.73 | ||
| Muscle radiodensity, (HU) | 33 ± 8 | 32 ± 8 | 34 ± 8 | 1.00 (0.97–1.03) | 0.96 | ||
| Visceral adipose radiodensity, (HU) | −85 ± 9 | −90 ± 10 | −83 ± 8 | 1.06 (1.03–1.09) | <0.001 | 1.05 (1.01–1.08) | 0.01 |
| Subcutaneous adipose radiodensity, (HU) | −93 ± 12 | −96 ± 13 | −92 ± 11 | 1.02 (0.996–1.04) | 0.12 | ||
| Sarcopenia d | 57 (56) | 22 (61) | 35 (54) | 1.44 (0.75–2.79) | 0.28 | ||
| Characteristic | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HR (95% CI) | p-value | HR (95% CI) | p-value | |
| HCV-induced HCC | 2.43 (1.43–4.13) | 0.001 | 2.17 (1.21–3.87) | 0.009 |
| NASH-induced HCC | 0.23 (0.05–0.94) | 0.04 | 0.74 (0.16–3.43) | 0.70 |
| BCLC stage | ||||
| ||||
| 2.74 (1.40–5.34) | 0.003 | 2.82 (1.37–5.81) | 0.005 |
| 2.93 (1.42–6.06) | 0.004 | 2.72 (1.22–6.05) | 0.01 |
| Previous treatment | 2.33 (1.41–3.85) | 0.001 | 1.66 (0.96–2.86) | 0.07 |
| Markers of portal hypertension a | 2.07 (1.24–3.45) | 0.005 | 1.37 (0.79–2.38) | 0.26 |
| High visceral adipose Radiodensity (VAT HU≥ −85 HU) | 2.56 (1.54–4.26) | 0.002 | 2.01 (1.14–3.54) | 0.02 |
| Characteristics | High VAT radiodensity (n = 47) | Low VAT radiodensity (n = 54) | p-value |
|---|---|---|---|
| Sex, male | 39 (83) | 50 (93) | 0.22 |
| Age at SIRT, years | 60 ± 14 | 65 ± 11 | 0.046 |
| Cirrhosis etiology | |||
| 6 (13) | 8 (15) | 1.00 |
| 17 (36) | 14 (26) | 0.29 |
| 7 (15) | 5 (9) | 1.00 |
| 9 (19) | 12 (22) | 0.81 |
| 0 (0) | 6 (11) | 0.03 |
| 8 (17) | 9 (17) | 1.00 |
| Vascular invasion | 10 (21) | 9 (17) | 0.62 |
| Extrahepatic spread | 3 (6) | 1 (2) | 0.34 |
| ALBI score | −2.1 ± 0.7 | −2.5 ± 0.5 | <0.001 |
| Child–Pugh | |||
| 25 (53) | 44 (82) | 0.003 |
| 22 (47) | 10 (18) | |
| BCLC stage | |||
| 12 (26) | 17 (32) | 0.13 |
| 19 (40) | 28 (52) | |
| 16 (34) | 9 (17) | |
| Previous treatment | 22 (47) | 16 (30) | 0.10 |
| Type of previous treatment | |||
| 3 (14) | 1 (6) | 0.62 |
| 1 (4) | 2 (13) | 0.57 |
| 8 (37) | 9 (56) | 0.34 |
| 3 (14) | 2 (13) | 1.00 |
| 7 (32) | 2 (13) | 0.26 |
| Splenomegaly | 24 (51) | 8 (15) | <0.001 |
| Ascites | 19 (40) | 6 (11) | 0.001 |
| Esophageal varices | 20 (43) | 13 (24) | 0.06 |
| Encephalopathy | 2 (4) | 1 (2) | 0.60 |
| Thrombocytopenia | 19 (40) | 14 (26) | 0.14 |
| Body Composition | |||
| BMI | 24 ± 4 | 26 ± 4 | 0.02 |
| SMI (cm2/m2) | 47 ± 9 | 48 ± 10 | 0.35 |
| VATI (cm2/m2) | 27 ± 16 | 64 ± 29 | <0.001 |
| SATI (cm2/m2) | 44 ± 26 | 65 ± 37 | 0.002 |
| Muscle radiodensity, (HU) | 36 ± 7 | 31 ± 8 | <0.001 |
| Visceral Adipose Radiodensity, (HU) | −77 ± 5 | −93 ± 5 | <0.001 |
| Subcutaneous Adipose Radiodensity, (HU) | −87 ± 13 | −99 ± 6 | <0.001 |
| Sarcopenia a | 27 (57) | 30 (56) | 1.00 |
| Characteristics | Univariate | Multivariate | ||
|---|---|---|---|---|
| OR (95% CI) | p-value | OR (95% CI) | p-value | |
| Sex, male | 0.78 (0.14–8.19) | 1.00 | ||
| Child–Pugh B | 4.92 (1.32–20.74) | 0.01 | 2.48 (0.57–11.84) | 0.28 |
| BCLC stage | 1.56 (0.37–9.40) | 0.77 | ||
| Previous treatment | 2.51 (0.69–9.66) | 0.19 | ||
| Markers of portal hypertension a | 4.81 (0.98–46.82) | 0.05 | 2.34 (0.37–25.68) | 0.53 |
| High visceral adipose radiodensity b | 8.74 (1.78–85.14) | 0.003 | 5.61 (1.05–56.89) | 0.04 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ebadi, M.; Moctezuma-Velazquez, C.; Meza-Junco, J.; Baracos, V.E.; DunichandHoedl, A.R.; Ghosh, S.; Sarlieve, P.; Owen, R.J.; Kneteman, N.; Montano-Loza, A.J. Visceral Adipose Tissue Radiodensity Is Linked to Prognosis in Hepatocellular Carcinoma Patients Treated with Selective Internal Radiation Therapy. Cancers 2020, 12, 356. https://doi.org/10.3390/cancers12020356
Ebadi M, Moctezuma-Velazquez C, Meza-Junco J, Baracos VE, DunichandHoedl AR, Ghosh S, Sarlieve P, Owen RJ, Kneteman N, Montano-Loza AJ. Visceral Adipose Tissue Radiodensity Is Linked to Prognosis in Hepatocellular Carcinoma Patients Treated with Selective Internal Radiation Therapy. Cancers. 2020; 12(2):356. https://doi.org/10.3390/cancers12020356
Chicago/Turabian StyleEbadi, Maryam, Carlos Moctezuma-Velazquez, Judith Meza-Junco, Vickie E. Baracos, Abha R. DunichandHoedl, Sunita Ghosh, Philippe Sarlieve, Richard J. Owen, Norman Kneteman, and Aldo J. Montano-Loza. 2020. "Visceral Adipose Tissue Radiodensity Is Linked to Prognosis in Hepatocellular Carcinoma Patients Treated with Selective Internal Radiation Therapy" Cancers 12, no. 2: 356. https://doi.org/10.3390/cancers12020356
APA StyleEbadi, M., Moctezuma-Velazquez, C., Meza-Junco, J., Baracos, V. E., DunichandHoedl, A. R., Ghosh, S., Sarlieve, P., Owen, R. J., Kneteman, N., & Montano-Loza, A. J. (2020). Visceral Adipose Tissue Radiodensity Is Linked to Prognosis in Hepatocellular Carcinoma Patients Treated with Selective Internal Radiation Therapy. Cancers, 12(2), 356. https://doi.org/10.3390/cancers12020356