A Matching-Adjusted Indirect Comparison of Pembrolizumab + Chemotherapy vs. Nivolumab + Ipilimumab as First-Line Therapies in Patients with PD-L1 TPS ≥1% Metastatic NSCLC


 ,
,
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Populations
2.2. Outcome Measures
2.3. Statistic Methods
3. Results
3.1. Baseline Characteristics
3.2. Base Case Analysis
3.3. Sensitivity Analyses and Sub-Group Analyses by PD-L1 Expression
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Low, J.L.; Walsh, R.J.; Ang, Y.; Chan, G.; Soo, R.A. The evolving immuno-oncology landscape in advanced lung cancer: first-line treatment of non-small cell lung cancer. Ther. Adv. Med. Oncol. 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Herbst, R.S.; Morgensztern, D.; Boshoff, C. The biology and management of non-small cell lung cancer. Nat. Cell Biol. 2018, 553, 446–454. [Google Scholar] [CrossRef] [PubMed]
- KEYTRUDA: Highlights of Prescribing Information. Available online: https://www.merck.com/product/usa/pi_circulars/k/keytruda/keytruda_pi.pdf (accessed on 30 October 2020).
- European Medicines Agency. Summary of Product Characteristics Keytruda. Available online: https://www.ema.europa.eu/en/documents/product-information/keytruda-epar-product-information_en.pdf (accessed on 30 October 2020).
- Borghaei, H.; Langer, C.J.; Gadgeel, S.; Papadimitrakopoulou, V.A.; Patnaik, A.; Powell, S.F.; Gentzler, R.D.; Martins, R.G.; Stevenson, J.P.; Jalal, S.I.; et al. 24-Month Overall Survival from KEYNOTE-021 Cohort G: Pemetrexed and Carboplatin with or without Pembrolizumab as First-Line Therapy for Advanced Nonsquamous Non–Small Cell Lung Cancer. J. Thorac. Oncol. 2019, 14, 124–129. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus Chemotherapy in Metastatic Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Şenler, F.Ç.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus Chemotherapy for Squamous Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Bristol-Myers Squibb. OPDIVO: Highlights of Prescribing Information. Available online: https://packageinserts.bms.com/pi/pi_opdivo.pdf (accessed on 30 October 2020).
- Hellmann, M.D.; Paz-Ares, L.; Caro, R.B.; Zurawski, B.; Kim, S.-W.; Costa, E.C.; Park, K.; Alexandru, A.; Lupinacci, L.; Jimenez, E.D.L.M.; et al. Nivolumab plus Ipilimumab in Advanced Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef]
- Davis, A.A.; Patel, V. The role of PD-L1 expression as a predictive biomarker: an analysis of all US Food and Drug Administration (FDA) approvals of immune checkpoint inhibitors. J. Immunother. Cancer 2019, 7, 1–8. [Google Scholar] [CrossRef]
- Atkins, M.B.; Tarhini, A.; Rael, M.; Gupte-Singh, K.; O’Brien, E.; Ritchings, C.; Rao, S.; McDermott, D.F. Comparative efficacy of combination immunotherapy and targeted therapy in the treatment of BRAF-mutant advanced melanoma: a matching-adjusted indirect comparison. Immunotherapy 2019, 11, 617–629. [Google Scholar] [CrossRef]
- Cortes, J.E.; Muresan, B.; Mamolo, C.; Cappelleri, J.C.; Crescenzo, R.J.; Su, Y.; Gambacorti-Passerini, C.; Heeg, B.; Smith, B.D. Matching-adjusted indirect comparison of bosutinib, dasatinib and nilotinib effect on survival and major cytogenetic response in treatment of second-line chronic phase chronic myeloid leukemia. Curr. Med. Res. Opin. 2019, 35, 1615–1622. [Google Scholar] [CrossRef]
- Signorovitch, J.; Swallow, E.; Kantor, E.; Wang, X.; Klimovsky, J.; Haas, T.; Devine, E.B.; Metrakos, P. Everolimus and sunitinib for advanced pancreatic neuroendocrine tumors: a matching-adjusted indirect comparison. Exp. Hematol. Oncol. 2013, 2, 32. [Google Scholar] [CrossRef]
- Van Sanden, S.; Ito, T.; Diels, J.; Vogel, M.; Belch, A.; Oriol, A. Comparative Efficacy of Daratumumab Monotherapy and Pomalidomide Plus Low-Dose Dexamethasone in the Treatment of Multiple Myeloma: A Matching Adjusted Indirect Comparison. Oncology 2017, 23, 279–287. [Google Scholar] [CrossRef] [PubMed]
- Phillippo, D.; Ades, T.; Dias, S.; Palmer, S.; Abrams, K.R.; Welton, N. NICE DSU Technical Support Document 18: Methods for population-adjusted indirect comparisons in submissions to NICE; NICE Decision Support Unit: Sheffield, UK, 2016. [Google Scholar]
- Rodriguez-Abreu, D.; Powell, S.F.; Hochmair, M.; Gadgeel, S.M.; Esteban, E.; Felip, E.; Speranza, G.; Gomez, M.D.; Cheng, S.Y.; Bischoff, H.; et al. Final analysis of KEYNOTE-189: Pemetrexed-platinum chemotherapy (chemo) with or without pembrolizumab (pembro) in patients (pts) with previously untreated metastatic nonsquamous non-small cell lung cancer (NSCLC). J. Clin. Oncol. 2020, 38, 9582. [Google Scholar] [CrossRef]
- Frederickson, A.M.; Arndorfer, S.; Zhang, I.; Lorenzi, M.; Insinga, R.; Arunachalam, A.; A Burke, T.; Simon, G.R. Pembrolizumab plus chemotherapy for first-line treatment of metastatic nonsquamous non-small-cell lung cancer: A network meta-analysis. Immunotherapy 2019, 11, 407–428. [Google Scholar] [CrossRef] [PubMed]
- Guyot, P.; E Ades, A.; Ouwens, M.J.N.M.; Welton, N.J. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med. Res. Methodol. 2012, 12, 9. [Google Scholar] [CrossRef]
- Abbasi, S.; Badheeb, A. Prognostic Factors in Advanced Non-Small-Cell Lung Cancer Patients: Patient Characteristics and Type of Chemotherapy. Lung Cancer Int. 2011, 2011, 1–4. [Google Scholar] [CrossRef]
- Carter, G.C.; Barrett, A.M.; A Kaye, J.; Liepa, A.M.; Winfree, K.B.; John, W.J. A comprehensive review of nongenetic prognostic and predictive factors influencing the heterogeneity of outcomes in advanced non-small-cell lung cancer. Cancer Manag. Res. 2014, 6, 437–449. [Google Scholar] [CrossRef][Green Version]
- Kawaguchi, T.; Takada, M.; Kubo, A.; Matsumura, A.; Fukai, S.; Tamura, A.; Saito, R.; Maruyama, Y.; Kawahara, M.; Ou, S.-H.I. Performance Status and Smoking Status Are Independent Favorable Prognostic Factors for Survival in Non-small Cell Lung Cancer: A Comprehensive Analysis of 26,957 Patients with NSCLC. J. Thorac. Oncol. 2010, 5, 620–630. [Google Scholar] [CrossRef]
- Standfield, L.; Weston, A.R.; Barraclough, H.; Van Kooten, M.; Pavlakis, N. Histology as a treatment effect modifier in advanced non-small cell lung cancer: A systematic review of the evidence. Respirology 2011, 16, 1210–1220. [Google Scholar] [CrossRef]
- Signorovitch, J.E.; Wu, E.Q.; Yu, A.P.; Gerrits, C.M.; Kantor, E.; Bao, Y.; Gupta, S.R.; Mulani, M.P. Comparative effectiveness without head-to-head trials: a method for matching-adjusted indirect comparisons applied to psoriasis treatment with adalimumab or etanercept. Pharmacoeconomics 2010, 28, 935–945. [Google Scholar] [CrossRef]
- Bucher, H.C.; Guyatt, G.H.; Griffith, L.E.; Walter, S.D. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 1997, 50, 683–691. [Google Scholar] [CrossRef]
- Nana-Sinkam, P.; Herbst, R.S.; Baas, P.; Kim, D.W.; Felip, E.; Pérez-Gracia, J.L.; Han, J.Y.; Molina, J.; Kim, J.H.; Arvis, C.D.; et al. Faculty Opinions recommendation of Pembrolizumab versus docetaxel for previously treated, PD-L1-positive, advanced non-small-cell lung cancer (KEYNOTE-010): A randomised controlled trial. Faculty Opin. Post-Publ. Peer Rev. Biomed. Literature 2017, 387, 1540–1550. [Google Scholar] [CrossRef]
- Borghaei, H.; Paz-Ares, L.; Horn, L.; Spigel, D.R.; Steins, M.; Ready, N.E.; Chow, L.Q.; Vokes, E.E.; Felip, E.; Holgado, E.; et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2015, 373, 1627–1639. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, F.R.; McElhinny, A.; Stanforth, D.; Ranger-Moore, J.; Jansson, M.; Kulangara, K.; Richardson, W.; Towne, P.; Hanks, D.; Vennapusa, B.; et al. PD-L1 Immunohistochemistry Assays for Lung Cancer: Results from Phase 1 of the Blueprint PD-L1 IHC Assay Comparison Project. J. Thorac. Oncol. 2017, 12, 208–222. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Category | CheckMate 227 Part 1A | KEYNOTE-021G | KEYNOTE-189 | KEYNOTE-407 |
|---|---|---|---|---|
| Study design and timeframe | ||||
| Study phase | III | II | III | III |
| Masking | Open-label | Open-label | Double-blind | Double-blind |
| Stratification factors | Tumor histology | PD-L1 TPS | PD-L1 TPS, platinum-based drug and smoking history | Paclitaxel vs nab-paclitaxel, PD-L1 status and region of enrollment |
| Patient enrollment period | August 2015–November 2016 | November 2014–January 2016 | February 2016–March 2017 | August 2016–December 2017 |
| Median duration of follow-up | Not reported (Minimum follow-up duration 29.3 months) | 31.0 months (range: 0.8–55.4) | 18.8 months (range: 0.2–38.8) | 14.3 months (range: 0.1–31.3) |
| Maximum permitted duration of immunotherapy | 2 years | 2 years | 2 years | 2 years |
| Key inclusion criteria | ||||
| Minimum age (years) | 18 | 18 | 18 | 18 |
| ECOG performance score | ≤1 | ≤1 | ≤1 | ≤1 |
| Disease stage | IV or recurrent | IIIb or IV | IV | IV |
| EGFR mutation and/or ALK rearrangement positive patients excluded | Yes | Yes | Yes | Not applicable a |
| Cross-over | ||||
| Cross-over allowed within trial | Not permitted | Permitted | Permitted | Permitted |
| Condition for within trial cross-over | Not applicable | Progressive disease defined by RECIST v1.1, investigator assessed | Progression verified by blinded, independent central radiologic review | Progression verified by blinded, independent central radiologic review |
| Cross-over from | Not applicable | Chemotherapy | Chemotherapy | Chemotherapy |
| Cross-over to | Not applicable | Pembrolizumab monotherapy | Pembrolizumab monotherapy | Pembrolizumab monotherapy |
| Number of patients crossed over to PD1 inhibitor within trial | Not applicable | 28/63 (44.4%) | 84/206 (40.8%) | 114/281 (40.6%) |
| Subsequent immunotherapy or PD-1/PD-L1-directed therapy in the control group (within trial + outside of trial crossover) | 171/397 (43.1%) | 43/63 (68.3%) | 113/206 (54.9%) | 138/281 (49.1%) |
| Category | Nivolumab + Ipilimumab and Chemotherapy Arms CheckMate 227 Part 1A (n = 793) | Pembrolizumab + Chemotherapy and Chemotherapy Arms KN021G/KN189/KN407 | |
|---|---|---|---|
| Before Matching (n = 816) | After Matching (n = 456 a) | ||
| Age Group (years) | |||
| ≤64 | 51.20 | 46.69 | 51.20 |
| 65–74 | 38.59 | 42.77 | 38.59 |
| ≥75 | 10.21 | 10.54 | 10.21 |
| Sex | |||
| Male | 64.94 | 66.30 | 64.94 |
| Female | 35.06 | 33.70 | 35.06 |
| Region | |||
| North America | 11.98 | 25.86 | 11.98 |
| Europe | 50.44 | 48.65 | 50.44 |
| Asia | 20.43 | 8.46 | 20.43 |
| Rest of World | 17.15 | 17.03 | 17.15 |
| Smoking Status b | |||
| Current/Former | 86.30 | 88.85 | 86.30 |
| Never | 13.70 | 11.15 | 13.70 |
| ECOG Status | |||
| 0 | 33.92 | 37.25 | 33.92 |
| 1 | 65.45 | 62.25 | 65.45 |
| Other score or missing data | 0.63 | 0.49 | 0.63 |
| Histology | |||
| Non-Squamous | 70.62 | 56.74 | 70.62 |
| Squamous | 29.38 | 43.26 | 29.38 |
| Metastases | |||
| Bone | 26.23 | 32.97 | 26.23 |
| CNS | 10.21 | 11.89 | 10.21 |
| Liver | 19.67 | 18.14 | 19.67 |
| PD-L1 TPS Group | |||
| 1–49 | 49.94 | 53.19 | 49.94 |
| ≥50 | 50.06 | 46.81 | 50.06 |
| Category | Outcomes | |
|---|---|---|
| Overall Survival | Progression-Free Survival | |
| ITC HR (95% CI), p value a | ||
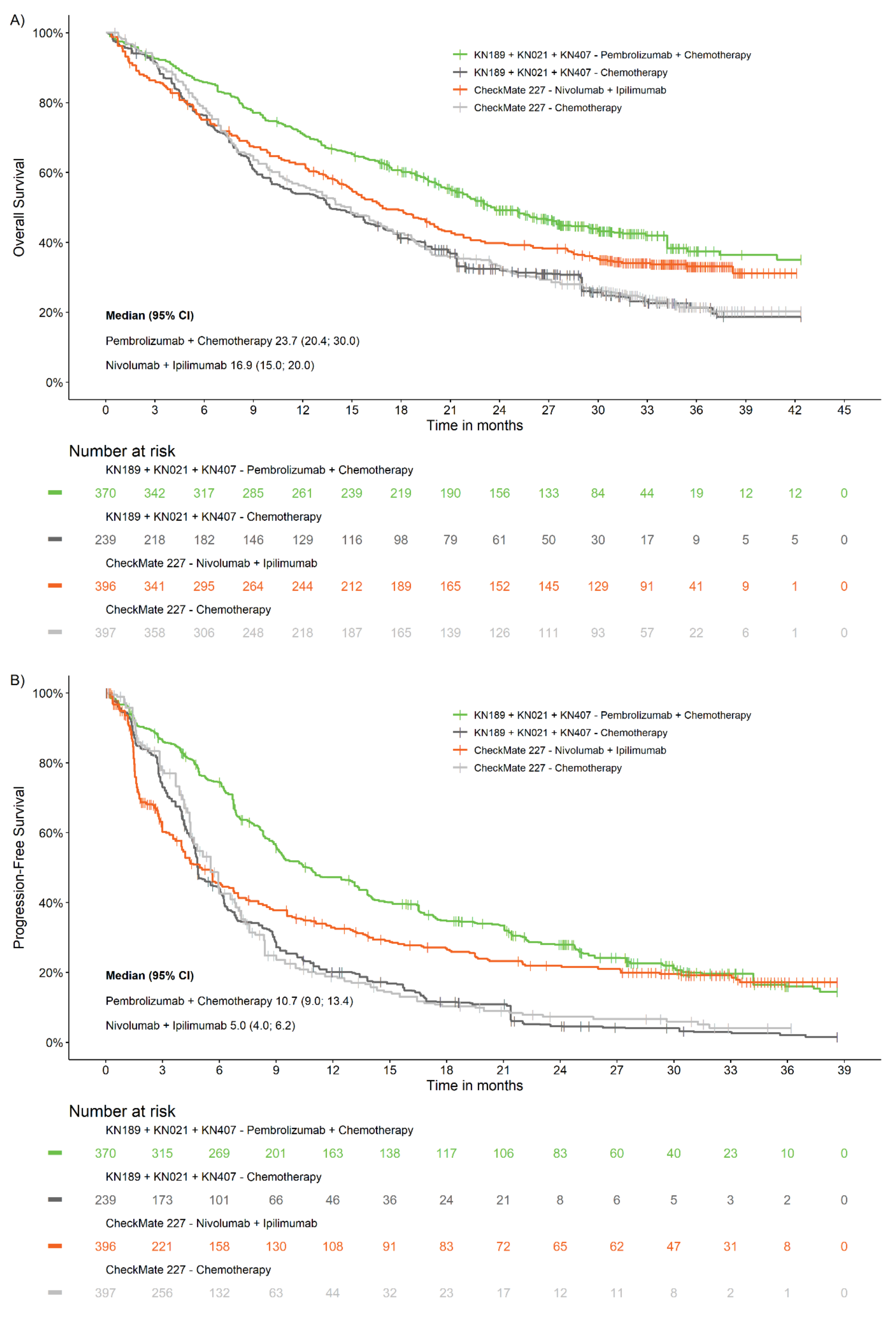
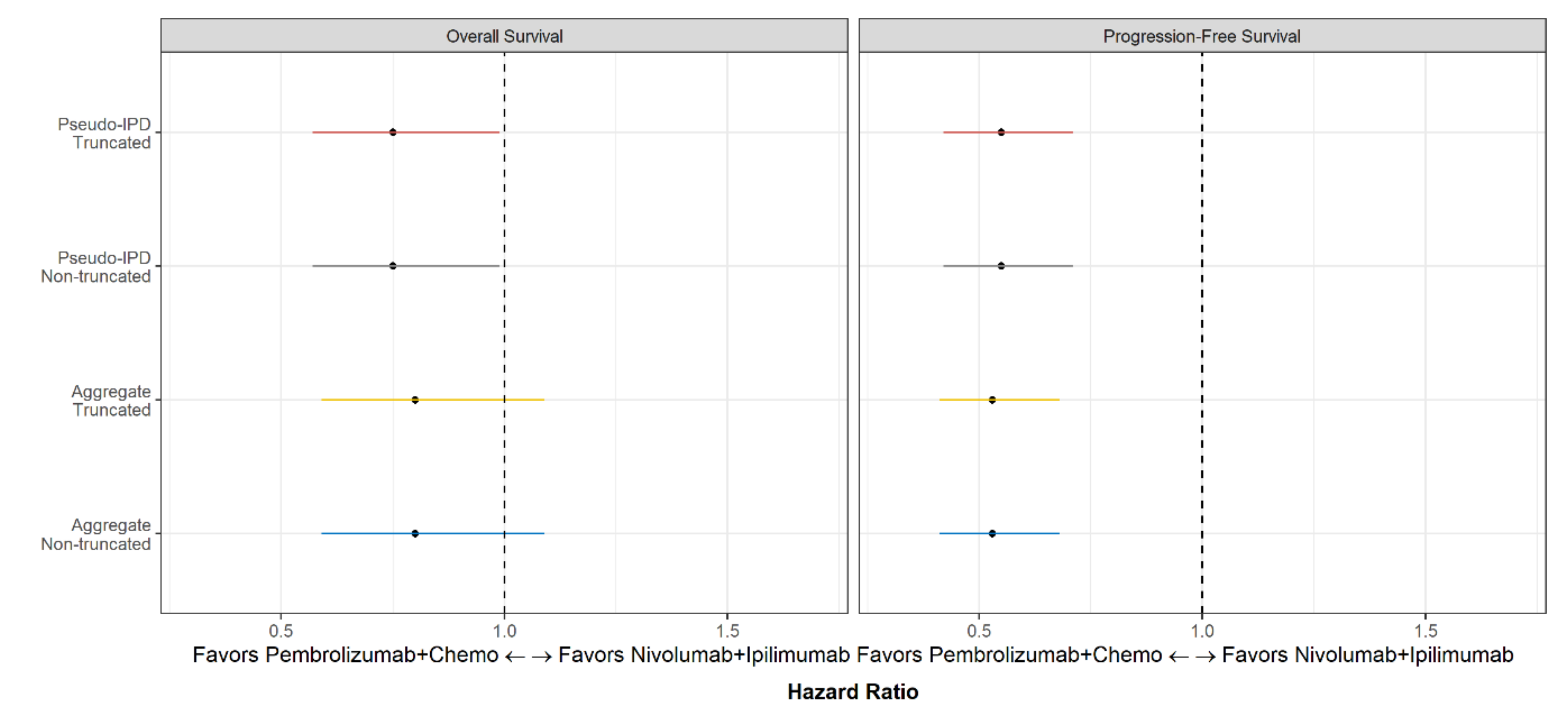
| Primary approach b | 0.80 (0.59, 1.09), 0.152 | 0.53 (0.41, 0.68), <0.001 |
| Secondary approach c | 0.75 (0.57, 0.99), 0.039 | 0.55 (0.42, 0.71), <0.001 |
| Number of events, (%) d | ||
| Pembrolizumab + chemotherapy | 206 (55.9) | 277 (75.1) |
| Nivolumab + ipilimumab | 259 (65.4) | 289 (73.0) |
| KN021G/KN189/KN407: Chemotherapy e | 174 (72.6) | 222 (92.8) |
| Checkmate 227: Chemotherapy e | 299 (75.3) | 286 (72.0) |
| Median Months, (95% CI) | ||
| Pembrolizumab + chemotherapy | 23.7 (20.4; 30.0) | 10.7 (9.0; 13.4) |
| Nivolumab + ipilimumab | 16.9 (15.0; 20.0) | 5.0 (4.0; 6.2) |
| KN021G/KN189/KN407: Chemotherapy e | 13.7 (10.1; 17.8) | 4.9 (4.6; 6.1) |
| Checkmate 227: Chemotherapy e | 14.9 (12.5; 16.8) | 5.5 (4.8; 5.9) |
| Landmark rate (%)–Pembrolizumab + chemotherapy vs nivolumab + ipilimumab | ||
| 6-month | 85.8 vs. 75.2 | 74.5 vs. 45.6 |
| 1-year | 71.0 vs. 62.4 | 47.2 vs. 32.8 |
| 2-year | 49.2 vs. 39.8 | 28.0 vs. 22.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halmos, B.; Burke, T.; Kalyvas, C.; Insinga, R.; Vandormael, K.; Frederickson, A.; Piperdi, B. A Matching-Adjusted Indirect Comparison of Pembrolizumab + Chemotherapy vs. Nivolumab + Ipilimumab as First-Line Therapies in Patients with PD-L1 TPS ≥1% Metastatic NSCLC. Cancers 2020, 12, 3648. https://doi.org/10.3390/cancers12123648
Halmos B, Burke T, Kalyvas C, Insinga R, Vandormael K, Frederickson A, Piperdi B. A Matching-Adjusted Indirect Comparison of Pembrolizumab + Chemotherapy vs. Nivolumab + Ipilimumab as First-Line Therapies in Patients with PD-L1 TPS ≥1% Metastatic NSCLC. Cancers. 2020; 12(12):3648. https://doi.org/10.3390/cancers12123648
Chicago/Turabian StyleHalmos, Balazs, Thomas Burke, Chrysostomos Kalyvas, Ralph Insinga, Kristel Vandormael, Andrew Frederickson, and Bilal Piperdi. 2020. "A Matching-Adjusted Indirect Comparison of Pembrolizumab + Chemotherapy vs. Nivolumab + Ipilimumab as First-Line Therapies in Patients with PD-L1 TPS ≥1% Metastatic NSCLC" Cancers 12, no. 12: 3648. https://doi.org/10.3390/cancers12123648
APA StyleHalmos, B., Burke, T., Kalyvas, C., Insinga, R., Vandormael, K., Frederickson, A., & Piperdi, B. (2020). A Matching-Adjusted Indirect Comparison of Pembrolizumab + Chemotherapy vs. Nivolumab + Ipilimumab as First-Line Therapies in Patients with PD-L1 TPS ≥1% Metastatic NSCLC. Cancers, 12(12), 3648. https://doi.org/10.3390/cancers12123648