First Line Systemic Treatment for MALT Lymphoma—Do We Still Need Chemotherapy? Real World Data from the Medical University Vienna

 ,
, 
 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Patients Characteristics
2.2. Treatment, Response Assessment and Follow-Up
2.3. Stastical Analysis
3. Results
3.1. Treatment Characteristics
3.2. Objective Response to Treatment
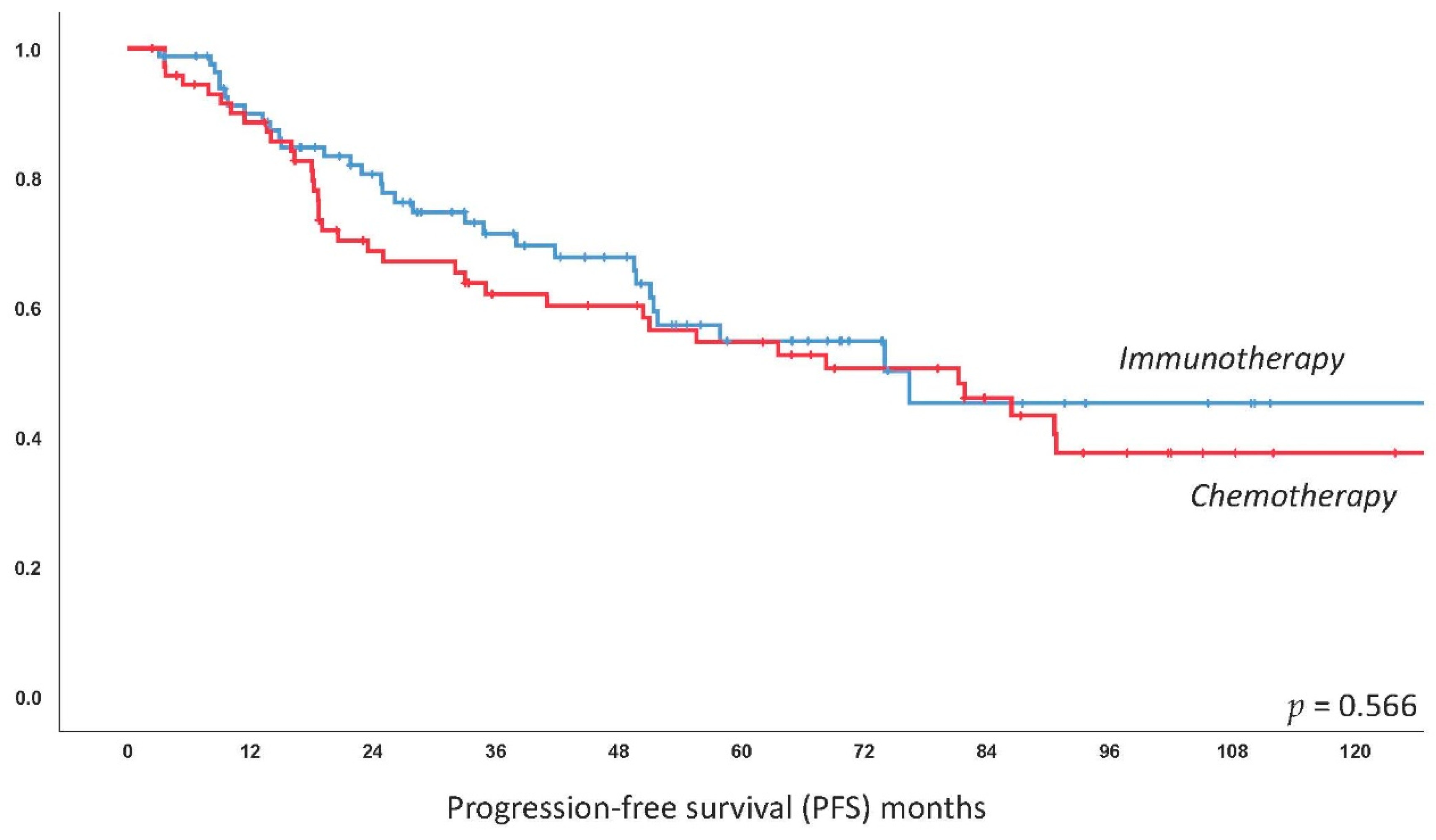
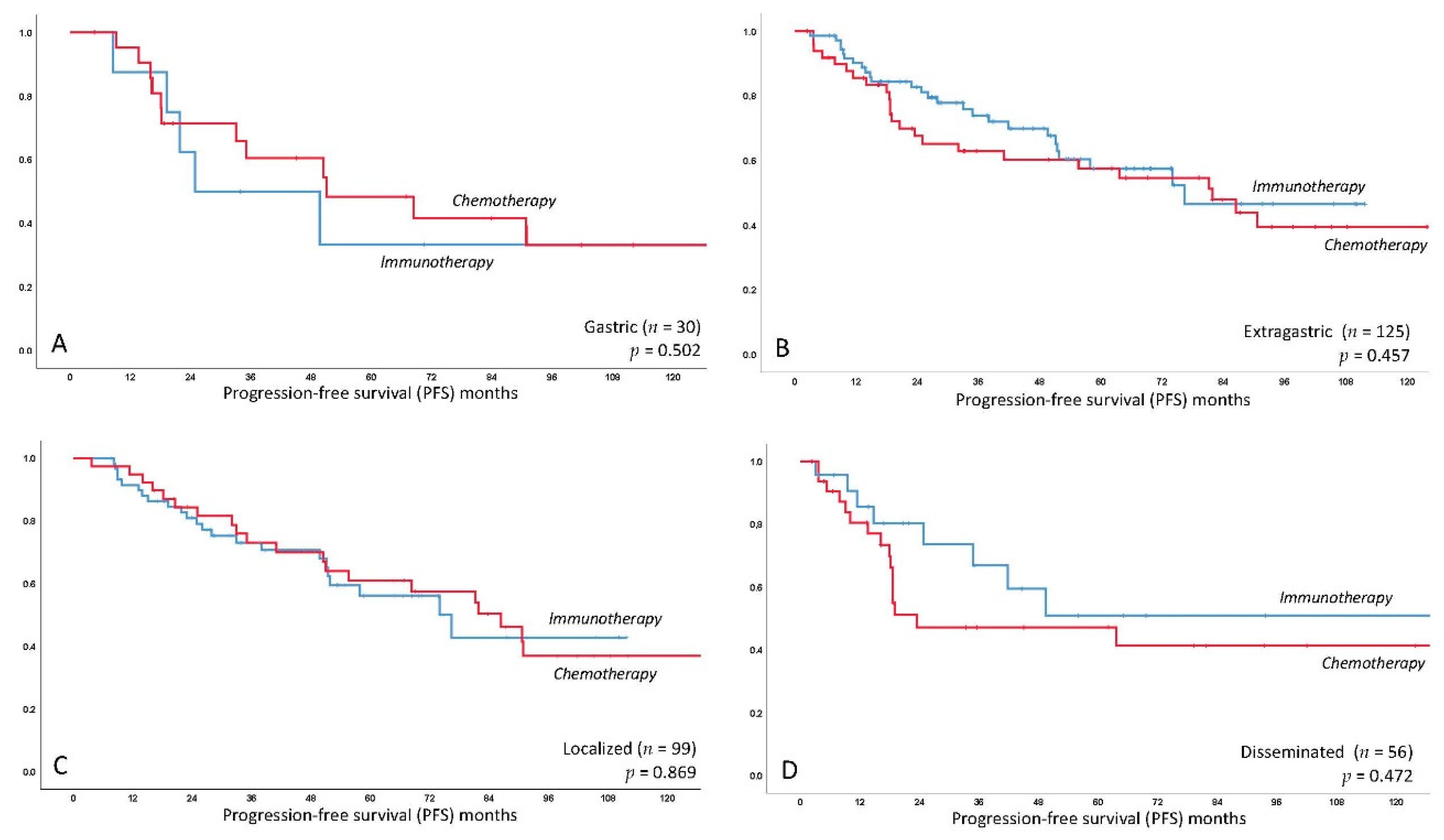
3.3. Progression-Free Survival
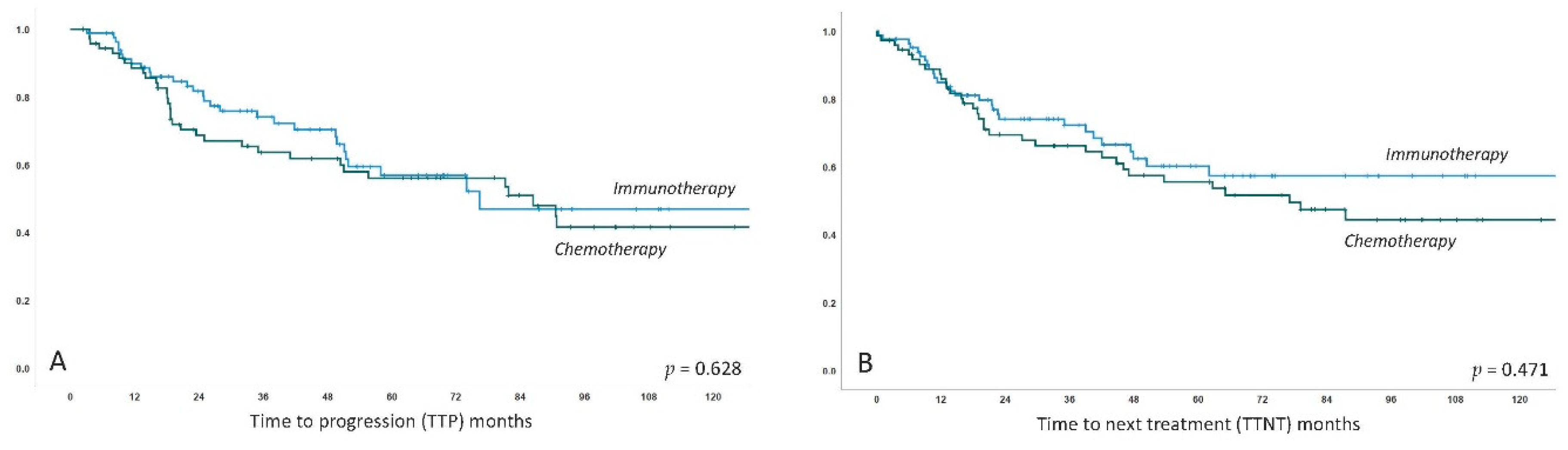
3.4. Long-Term Outcome
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cook, J.R.; Chott, A.; Nakamura, S.; Müller-Hermelink, H.K.; Harris, N.L.; Swerdlow, S.H. Extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma). In WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, Revised 4th ed.; Swerdlow, S.H., Campo, E., Harris, N.L., Jaffe, E.S., Pileri, S.A., Stein, H., Thiele, J., Eds.; IARC: Lyon, France, 2017; pp. 259–262. [Google Scholar]
- Raderer, M.; Kiesewetter, B.; Ferreri, A.J. Clinicopathologic characteristics and treatment of marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT lymphoma). CA Cancer J. Clin. 2016, 66, 153–171. [Google Scholar] [CrossRef] [PubMed]
- Isaacson, P.G.; Du, M.Q. MALT lymphoma: From morphology to molecules. Nat. Rev. Cancer 2004, 4, 644–653. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.H.; Wu, M.S.; Yeh, K.H.; Lin, C.W.; Hsu, P.N.; Chen, L.T.; Cheng, A.L. Novel Insights of Lymphomagenesis of Helicobacter pylori-Dependent Gastric Mucosa-Associated Lymphoid Tissue Lymphoma. Cancers 2019, 11, 547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, M.Q. MALT lymphoma: A paradigm of NF-kappaB dysregulation. Semin. Cancer Biol. 2016, 39, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Zucca, E.; Arcaini, L.; Buske, C.; Johnson, P.W.; Ponzoni, M.; Raderer, M.; Ricardi, U.; Salar, A.; Stamatopoulos, K.; Thieblemont, C.; et al. Marginal zone lymphomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 17–29. [Google Scholar] [CrossRef] [Green Version]
- Ruskone-Fourmestraux, A.; Fischbach, W.; Aleman, B.M.; Boot, H.; Du, M.Q.; Megraud, F.; Montalban, C.; Raderer, M.; Savio, A.; Wotherspoon, A.; et al. EGILS consensus report. Gastric extranodal marginal zone B-cell lymphoma of MALT. Gut 2011, 60, 747–758. [Google Scholar] [CrossRef] [Green Version]
- Kiesewetter, B.; Ferreri, A.J.; Raderer, M. Chemoimmunotherapy for Mucosa-Associated Lymphoid Tissue-Type Lymphoma: A Review of the Literature. Oncologist 2015, 20, 915–925. [Google Scholar] [CrossRef] [Green Version]
- Teckie, S.; Qi, S.; Chelius, M.; Lovie, S.; Hsu, M.; Noy, A.; Portlock, C.; Yahalom, J. Long-term outcome of 487 patients with early-stage extra-nodal marginal zone lymphoma. Ann. Oncol. 2017, 28, 1064–1069. [Google Scholar] [CrossRef]
- Zucca, E.; Conconi, A.; Martinelli, G.; Bouabdallah, R.; Tucci, A.; Vitolo, U.; Martelli, M.; Pettengell, R.; Salles, G.; Sebban, C.; et al. Final Results of the IELSG-19 Randomized Trial of Mucosa-Associated Lymphoid Tissue Lymphoma: Improved Event-Free and Progression-Free Survival With Rituximab Plus Chlorambucil Versus Either Chlorambucil or Rituximab Monotherapy. J. Clin. Oncol. 2017, 35, 1905–1912. [Google Scholar] [CrossRef]
- Salar, A.; Domingo-Domenech, E.; Panizo, C.; Nicolas, C.; Bargay, J.; Muntanola, A.; Canales, M.; Bello, J.L.; Sancho, J.M.; Tomas, J.F.; et al. Long-term results of a phase 2 study of rituximab and bendamustine for mucosa-associated lymphoid tissue lymphoma. Blood 2017, 130, 1772–1774. [Google Scholar] [CrossRef] [Green Version]
- Kiesewetter, B.; Raderer, M. Immunomodulatory treatment for mucosa-associated lymphoid tissue lymphoma (MALT lymphoma). Hematol. Oncol. 2020, 38, 417–424. [Google Scholar] [CrossRef] [PubMed]
- Noy, A.; de Vos, S.; Thieblemont, C.; Martin, P.; Flowers, C.R.; Morschhauser, F.; Collins, G.P.; Ma, S.; Coleman, M.; Peles, S.; et al. Targeting Bruton tyrosine kinase with ibrutinib in relapsed/refractory marginal zone lymphoma. Blood 2017, 129, 2224–2232. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, A.J.; Sassone, M.; Kiesewetter, B.; Govi, S.; Scarfo, L.; Donadoni, G.; Raderer, M. High-dose clarithromycin is an active monotherapy for patients with relapsed/refractory extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue (MALT): The HD-K phase II trial. Ann. Oncol. 2015, 26, 1760–1765. [Google Scholar] [CrossRef] [PubMed]
- Ferreri, A.J.M.; Cecchetti, C.; Kiesewetter, B.; Sassone, M.; Calimeri, T.; Perrone, S.; Ponzoni, M.; Raderer, M. Clarithromycin as a “repurposing drug” against MALT lymphoma. Br. J. Haematol. 2018, 182, 913–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Govi, S.; Dognini, G.P.; Licata, G.; Crocchiolo, R.; Resti, A.G.; Ponzoni, M.; Ferreri, A.J. Six-month oral clarithromycin regimen is safe and active in extranodal marginal zone B-cell lymphomas: Final results of a single-centre phase II trial. Br. J. Haematol. 2010, 150, 226–229. [Google Scholar] [CrossRef] [PubMed]
- Kiesewetter, B.; Troch, M.; Dolak, W.; Mullauer, L.; Lukas, J.; Zielinski, C.C.; Raderer, M. A phase II study of lenalidomide in patients with extranodal marginal zone B-cell lymphoma of the mucosa associated lymphoid tissue (MALT lymphoma). Haematologica 2013, 98, 353–356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiesewetter, B.; Willenbacher, E.; Willenbacher, W.; Egle, A.; Neumeister, P.; Voskova, D.; Mayerhoefer, M.E.; Simonitsch-Klupp, I.; Melchardt, T.; Greil, R.; et al. A phase 2 study of rituximab plus lenalidomide for mucosa-associated lymphoid tissue lymphoma. Blood 2017, 129, 383–385. [Google Scholar] [CrossRef] [Green Version]
- Troch, M.; Jonak, C.; Mullauer, L.; Puspok, A.; Formanek, M.; Hauff, W.; Zielinski, C.C.; Chott, A.; Raderer, M. A phase II study of bortezomib in patients with MALT lymphoma. Haematologica 2009, 94, 738–742. [Google Scholar] [CrossRef] [Green Version]
- Conconi, A.; Martinelli, G.; Lopez-Guillermo, A.; Zinzani, P.L.; Ferreri, A.J.; Rigacci, L.; Devizzi, L.; Vitolo, U.; Luminari, S.; Cavalli, F.; et al. Clinical activity of bortezomib in relapsed/refractory MALT lymphomas: Results of a phase II study of the International Extranodal Lymphoma Study Group (IELSG). Ann. Oncol. 2011, 22, 689–695. [Google Scholar] [CrossRef]
- Thieblemont, C.; Cascione, L.; Conconi, A.; Kiesewetter, B.; Raderer, M.; Gaidano, G.; Martelli, M.; Laszlo, D.; Coiffier, B.; Lopez Guillermo, A.; et al. A MALT lymphoma prognostic index. Blood 2017, 130, 1409–1417. [Google Scholar] [CrossRef] [Green Version]
- Copie-Bergman, C.; Wotherspoon, A.C.; Capella, C.; Motta, T.; Pedrinis, E.; Pileri, S.A.; Bertoni, F.; Conconi, A.; Zucca, E.; Ponzoni, M.; et al. Gela histological scoring system for post-treatment biopsies of patients with gastric MALT lymphoma is feasible and reliable in routine practice. Br. J. Haematol. 2013, 160, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Pfistner, B.; Juweid, M.E.; Gascoyne, R.D.; Specht, L.; Horning, S.J.; Coiffier, B.; Fisher, R.I.; Hagenbeek, A.; Zucca, E.; et al. Revised response criteria for malignant lymphoma. J. Clin. Oncol. 2007, 25, 579–586. [Google Scholar] [CrossRef] [PubMed]
- Thieblemont, C.; Berger, F.; Dumontet, C.; Moullet, I.; Bouafia, F.; Felman, P.; Salles, G.; Coiffier, B. Mucosa-associated lymphoid tissue lymphoma is a disseminated disease in one third of 158 patients analyzed. Blood 2000, 95, 802–806. [Google Scholar] [CrossRef] [PubMed]
- Raderer, M.; Streubel, B.; Woehrer, S.; Puespoek, A.; Jaeger, U.; Formanek, M.; Chott, A. High relapse rate in patients with MALT lymphoma warrants lifelong follow-up. Clin. Cancer Res. 2005, 11, 3349–3352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teckie, S.; Qi, S.; Lovie, S.; Navarrett, S.; Hsu, M.; Noy, A.; Portlock, C.; Yahalom, J. Long-term outcomes and patterns of relapse of early-stage extranodal marginal zone lymphoma treated with radiation therapy with curative intent. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 130–137. [Google Scholar] [CrossRef]
- Raderer, M.; Vorbeck, F.; Formanek, M.; Osterreicher, C.; Valencak, J.; Penz, M.; Kornek, G.; Hamilton, G.; Dragosics, B.; Chott, A. Importance of extensive staging in patients with mucosa-associated lymphoid tissue (MALT)-type lymphoma. Br. J. Cancer 2000, 83, 454–457. [Google Scholar] [CrossRef]
- Morschhauser, F.; Fowler, N.H.; Feugier, P.; Bouabdallah, R.; Tilly, H.; Palomba, M.L.; Fruchart, C.; Libby, E.N.; Casasnovas, R.O.; Flinn, I.W.; et al. Rituximab plus Lenalidomide in Advanced Untreated Follicular Lymphoma. N. Engl. J. Med. 2018, 379, 934–947. [Google Scholar] [CrossRef]
- Rummel, M.J.; Niederle, N.; Maschmeyer, G.; Banat, G.A.; von Grünhagen, U.; Losem, C.; Kofahl-Krause, D.; Heil, G.; Welslau, M.; Balser, C.; et al. Bendamustine plus rituximab versus CHOP plus rituximab as first-line treatment for patients with indolent and mantle-cell lymphomas: An open-label, multicentre, randomised, phase 3 non-inferiority trial. Lancet 2013, 381, 1203–1210. [Google Scholar] [CrossRef]
- Flinn, I.W.; van der Jagt, R.; Kahl, B.S.; Wood, P.; Hawkins, T.E.; Macdonald, D.; Hertzberg, M.; Kwan, Y.L.; Simpson, D.; Craig, M.; et al. Randomized trial of bendamustine-rituximab or R-CHOP/R-CVP in first-line treatment of indolent NHL or MCL: The BRIGHT study. Blood 2014, 123, 2944–2952. [Google Scholar] [CrossRef]
- Kiesewetter, B.; Lamm, W.; Neuper, O.; Mayerhoefer, M.E.; Simonitsch-Klupp, I.; Raderer, M. Prolonged follow-up on lenalidomide-based treatment for mucosa-associated lymphoid tissue lymphoma (MALT lymphoma)-Real-world data from the Medical University of Vienna. Hematol. Oncol. 2019, 37, 345–351. [Google Scholar] [CrossRef] [Green Version]
- Becnel, M.R.; Nastoupil, L.J.; Samaniego, F.; Davis, R.E.; You, M.J.; Green, M.; Hagemeister, F.B.; Fanale, M.A.; Fayad, L.E.; Westin, J.R.; et al. Lenalidomide plus rituximab (R(2)) in previously untreated marginal zone lymphoma: Subgroup analysis and long-term follow-up of an open-label phase 2 trial. Br. J. Haematol. 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Nuffel, A.M.; Sukhatme, V.; Pantziarka, P.; Meheus, L.; Sukhatme, V.P.; Bouche, G. Repurposing Drugs in Oncology (ReDO)-clarithromycin as an anti-cancer agent. Ecancermedicalscience 2015, 9, 513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kiesewetter, B.; Neuper, O.; Mayerhoefer, M.E.; Dolak, W.; Lukas, J.; Simonitsch-Klupp, I.; Raderer, M. A pilot phase II study of ofatumumab monotherapy for extranodal marginal zone B-cell lymphoma of the mucosa-associated lymphoid tissue (MALT) lymphoma. Hematol. Oncol. 2018, 36, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Fischbach, W.; Goebeler, M.E.; Ruskone-Fourmestraux, A.; Wundisch, T.; Neubauer, A.; Raderer, M.; Savio, A.; Group, E. Most patients with minimal histological residuals of gastric MALT lymphoma after successful eradication of Helicobacter pylori can be managed safely by a watch and wait strategy: Experience from a large international series. Gut 2007, 56, 1685–1687. [Google Scholar] [CrossRef] [Green Version]
- Conconi, A.; Thieblemont, C.; Cascione, L.; Torri, V.; Kiesewetter, B.; Margiotta Casaluci, G.; Gaidano, G.; Raderer, M.; Cavalli, F.; Lopez Guillermo, A.; et al. Early progression of disease predicts shorter survival in MALT lymphoma patients receiving systemic treatment. Haematologica 2020. [Google Scholar] [CrossRef] [Green Version]
- Stefanovic, A.; Lossos, I.S. Extranodal marginal zone lymphoma of the ocular adnexa. Blood 2009, 114, 501–510. [Google Scholar] [CrossRef] [Green Version]
- Pinnix, C.C.; Dabaja, B.S.; Milgrom, S.A.; Smith, G.L.; Abou, Z.; Nastoupil, L.; Romaguera, J.; Turturro, F.; Fowler, N.; Fayad, L.; et al. Ultra-low-dose radiotherapy for definitive management of ocular adnexal B-cell lymphoma. Head Neck 2017, 39, 1095–1100. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Feature | Entire Collective | Immunotherapy | Chemotherapy | p-Value |
|---|---|---|---|---|
| n = 159 | n = 85 | n = 74 | ||
| Sex | ||||
| Female | 57% (90/159) | 61% (52/85) | 51% (38/74) | p = 0.212 |
| Male | 43% (69/159) | 39% (33/85) | 49% (36/74) | |
| Age (median) | 65 years | 66 years | 64 years | p = 0.764 |
| Age 70+ | 33% (53/159) | 37% (31/85) | 30% (22/74) | p = 0.368 |
| Primary localization | ||||
| Gastric | 20% (32/159) | 11% (9/85) | 31% (23/74) | p = 0.001 |
| Extragastric | 80% (127/159) | 89% (76/85) | 69% (51/74) | |
| Stage of disease | ||||
| Localized (I/IIE) | 64% (102/159) | 72% (61/85) | 55% (41/74) | p = 0.032 |
| Disseminated (III/IVE) | 36% (57/159) | 28% (24/85) | 45% (33/74) | |
| MALT-IPI | ||||
| Low risk | 39% (58/149) | 40% (33/83) | 38% (25/66) | p = 0.815 |
| Intermediate/high risk | 61% (91/149) | 60% (50/83) | 62% (41/66) | |
| Further clinical features | ||||
| Autoimmune disorder * | 36% (50/141) | 32% (27/84) | 40% (23/57) | p = 0.371 |
| Plasmacytic diff. | 38% (47/125) | 35% (26/75) | 42% (21/50) | p = 0.407 |
| LDH > ULN | 7% (11/149) | 5% (4/83) | 11% (7/66) | p = 0.180 |
| Performance status > 1 | 5% (8/156) | 4% (3/85) | 7% (5/71) | p = 0.472 |
| Viral hepatitis (B/C) | 2% (3/132) | 0% (0/79) | 6% (3/53) | p = 0.063 |
| Beta2-micorglobulin > ULN | 45% (59/131) | 38% (29/77) | 56% (30/54) | p = 0.043 |
| Paraproteinemia | 34% (36/107) | 29% (19/65) | 40% (17/42) | p = 0.229 |
| Time to treatment (median) | 2.0 months | 2.2 months | 1.8 months | p = 0.013 |
| Follow-up time (median) | 66.5 months | 57.4 months | 87.3 months | p = 0.002 |
| Treatment Characteristics | |
|---|---|
| First line immunotherapy | 54% (85/159): |
| IMiDs +/−R | 37% (31/85) (+R in 18/31) |
| CD20-antibody monotherapy | 27% (23/85) |
| Macrolides | 27% (23/85) |
| Bortezomib | 9% (8/85) |
| First line chemotherapy +/− R | 46% (74/159) (+ R in 42/74) |
| Purine analogs +/−R | 31% (23/74) (+ R in 15/23) |
| CHOP-based +/−R | 28% (21/74) (+ R in 13/21) |
| Bendamustine + R | 18% (13/74) (+ R in 13/13) |
| Chlorambucil +/−R | 11% (8/74) (+ R in 1/8) |
| Other | 12% (9/74) |
| Per localization (primary sites >10%) | |
| Ocular adnexal MALT lymphoma (n = 52, 33%) | |
| First line immunotherapy | 29% (15/52) |
| First line chemotherapy | 71% (37/52) |
| Gastric MALT lymphoma (n = 32, 20%) | |
| First line immunotherapy | 72% (23/32) |
| First line chemotherapy | 28% (9/32) |
| Pulmonary MALT lymphoma (n = 27, 17%) | |
| First line immunotherapy | 44% (12/27) |
| First line chemotherapy | 56% (15/27) |
| Parotid gland MALT lymphoma (n = 18, 11%) | |
| First line immunotherapy | 44% (8/18) |
| First line chemotherapy | 56% (10/18) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kiesewetter, B.; Simonitsch-Klupp, I.; Mayerhoefer, M.E.; Dolak, W.; Lukas, J.; Raderer, M. First Line Systemic Treatment for MALT Lymphoma—Do We Still Need Chemotherapy? Real World Data from the Medical University Vienna. Cancers 2020, 12, 3533. https://doi.org/10.3390/cancers12123533
Kiesewetter B, Simonitsch-Klupp I, Mayerhoefer ME, Dolak W, Lukas J, Raderer M. First Line Systemic Treatment for MALT Lymphoma—Do We Still Need Chemotherapy? Real World Data from the Medical University Vienna. Cancers. 2020; 12(12):3533. https://doi.org/10.3390/cancers12123533
Chicago/Turabian StyleKiesewetter, Barbara, Ingrid Simonitsch-Klupp, Marius E. Mayerhoefer, Werner Dolak, Julius Lukas, and Markus Raderer. 2020. "First Line Systemic Treatment for MALT Lymphoma—Do We Still Need Chemotherapy? Real World Data from the Medical University Vienna" Cancers 12, no. 12: 3533. https://doi.org/10.3390/cancers12123533
APA StyleKiesewetter, B., Simonitsch-Klupp, I., Mayerhoefer, M. E., Dolak, W., Lukas, J., & Raderer, M. (2020). First Line Systemic Treatment for MALT Lymphoma—Do We Still Need Chemotherapy? Real World Data from the Medical University Vienna. Cancers, 12(12), 3533. https://doi.org/10.3390/cancers12123533