Perceived Cognitive Impairment in Breast Cancer Survivors and Its Relationships with Psychological Factors


 and
and
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Participant Characteristics
2.2. Univariable Analyses
2.2.1. Questionnaires and Associated Factors
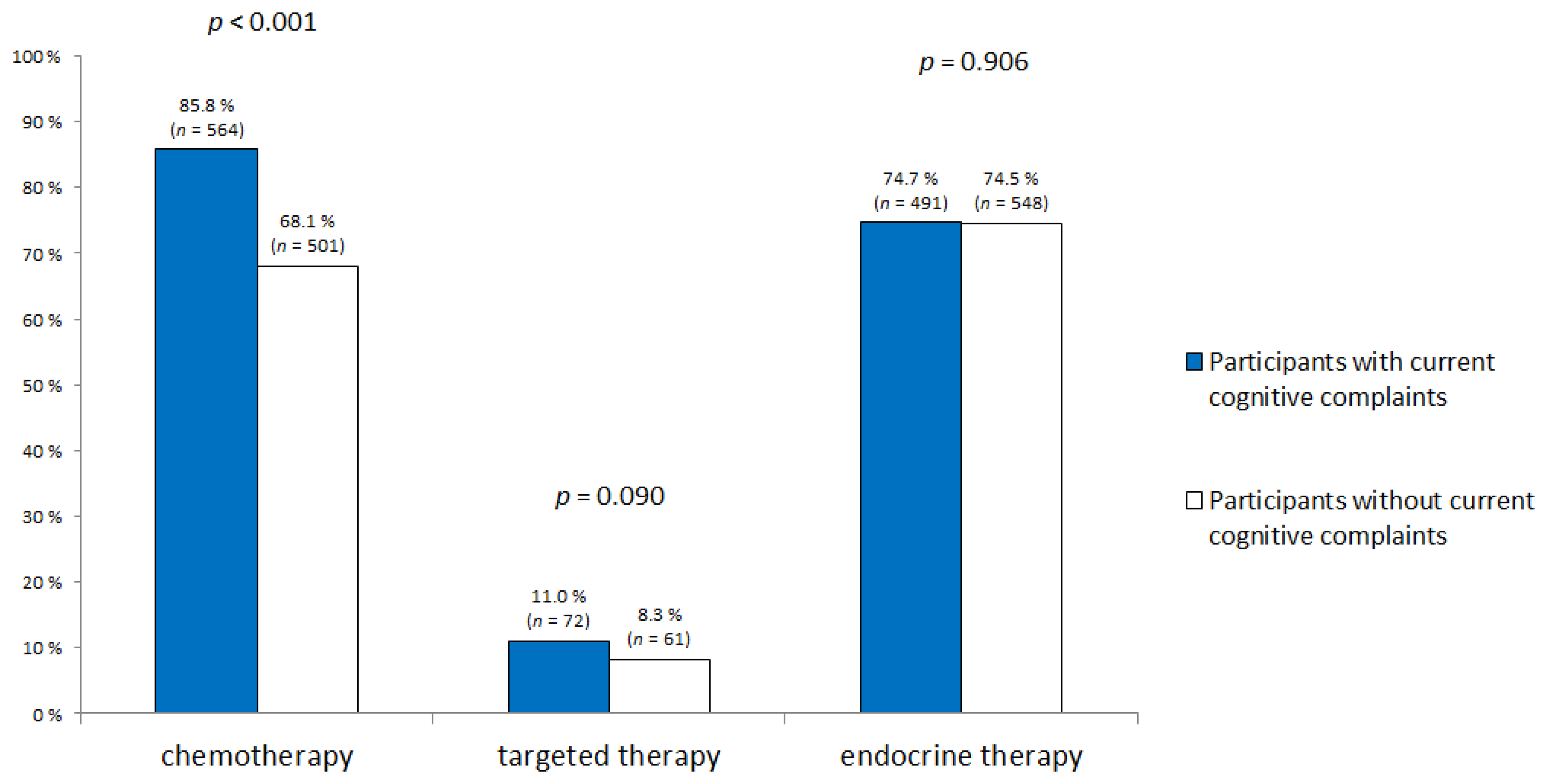
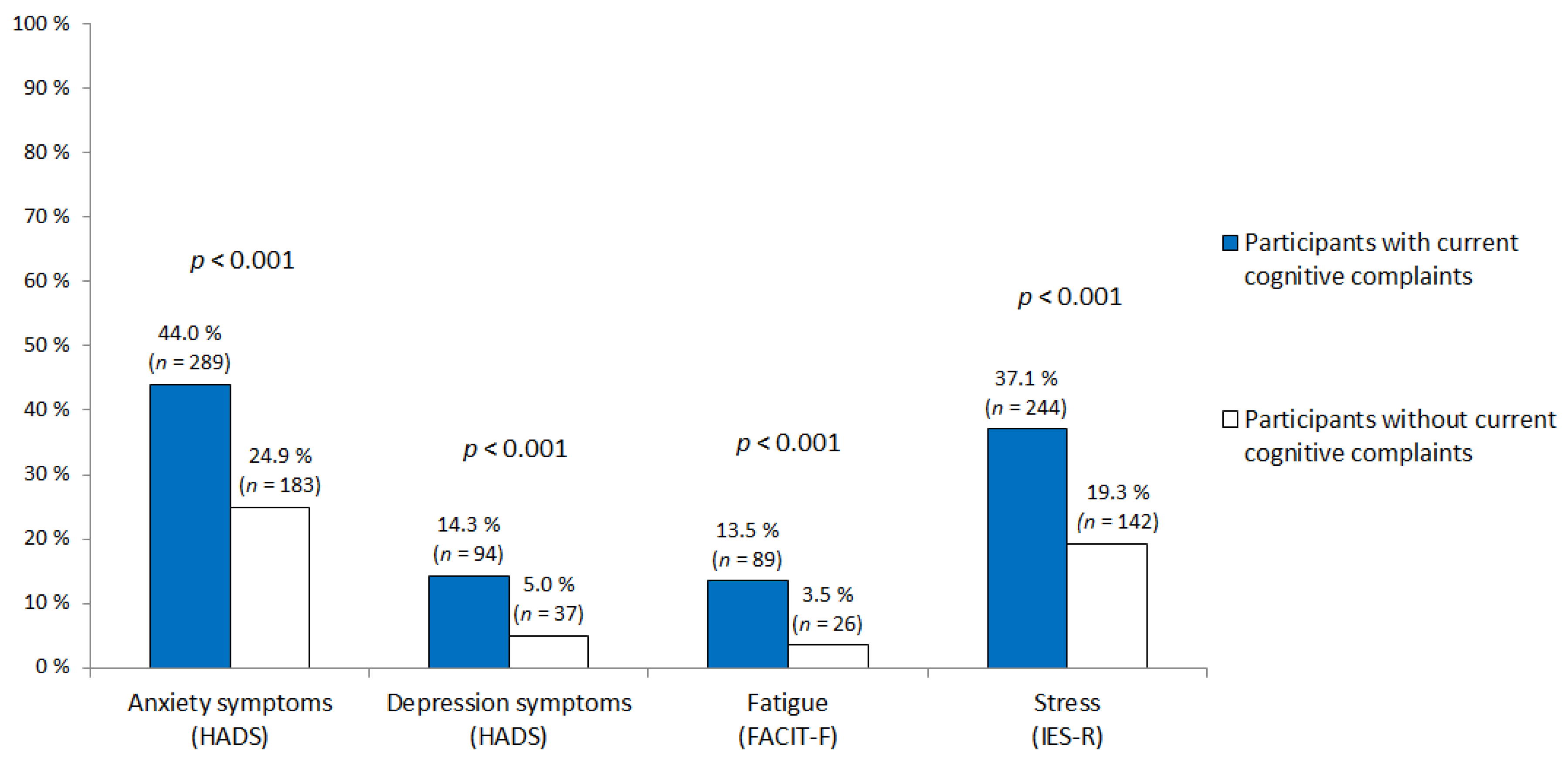
2.2.2. Current Cognitive Complaints
2.3. Multivariable Analyses
3. Discussion
4. Materials and Methods
4.1. Procedure
4.2. Participants
4.3. Assessment
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kim, H.; Jung, S.; Kim, H.; Abraham, I. Systematic review of longitudinal studies on chemotherapy-associated subjective cognitive impairment in cancer patients. Psycho-Oncology 2020, 29, 617–631. [Google Scholar] [CrossRef] [PubMed]
- Hutchinson, A.D.; Hosking, J.R.; Kichenadasse, G.; Mattiske, J.K.; Wilson, C. Objective and subjective cognitive impairment following chemotherapy for cancer: A systematic review. Cancer Treat. Rev. 2012, 38, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Von Ah, D.; Habermann, B.; Carpenter, J.S.; Schneider, B.L. Impact of perceived cognitive impairment in breast cancer survivors. Eur. J. Oncol. Nurs. 2013, 17, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Nieuwenhuijsen, K.; de Boer, A.; Spelten, E.; Sprangers, M.A.G.; Verbeek, J.H.A.M. The role of neuropsychological functioning in cancer survivors’ return to work one year after diagnosis. Psycho-Oncology 2009, 18, 589–597. [Google Scholar] [CrossRef]
- Myers, J.S.; Wick, J.A.; Klemp, J. Potential factors associated with perceived cognitive impairment in breast cancer survivors. Support. Care Cancer 2015, 23, 3219–3228. [Google Scholar] [CrossRef]
- Janelsins, M.C.; Kohli, S.; Mohile, S.G.; Usuki, K.; Ahles, T.A.; Morrow, G.R. An Update on Cancer- and Chemotherapy-Related Cognitive Dysfunction: Current Status. Semin. Oncol. 2011, 38, 431–438. [Google Scholar] [CrossRef]
- Vandenbossche, S.; Fery, P.; Razavi, D. Altérations cognitives et cancer du sein: Une revue critique de la littérature. Bull. Cancer 2009, 96, 239–248. [Google Scholar] [CrossRef]
- Ahles, T.A.; Root, J.C. Cognitive Effects of Cancer and Cancer Treatments. Annu. Rev. Clin. Psychol. 2018, 14, 425–451. [Google Scholar] [CrossRef]
- Janelsins, M.C.; Heckler, C.E.; Peppone, L.J.; Kamen, C.; Mustian, K.M.; Mohile, S.G.; Magnuson, A.; Kleckner, I.R.; Guido, J.J.; Young, K.L.; et al. Cognitive Complaints in Survivors of Breast Cancer After Chemotherapy Compared With Age-Matched Controls: An Analysis From a Nationwide, Multicenter, Prospective Longitudinal Study. JCO 2017, 35, 506–514. [Google Scholar] [CrossRef]
- Von Ah, D.; Tallman, E.F. Perceived Cognitive Function in Breast Cancer Survivors: Evaluating Relationships With Objective Cognitive Performance and Other Symptoms Using the Functional Assessment of Cancer Therapy—Cognitive Function Instrument. J. Pain Sympt. Manag. 2015, 49, 697–706. [Google Scholar] [CrossRef]
- Hermelink, K.; Bühner, M.; Sckopke, P.; Neufeld, F.; Kaste, J.; Voigt, V.; Münzel, K.; Wuerstlein, R.; Ditsch, N.; Hellerhoff, K.; et al. Chemotherapy and Post-traumatic Stress in the Causation of Cognitive Dysfunction in Breast Cancer Patients. JNCI J. Natl. Cancer Inst. 2017, 109. [Google Scholar] [CrossRef]
- Chapman, B.; Helmrath, S.; Derakshan, N. Perceived cognitive functioning and its influence on emotional vulnerability in breast cancer. Health Psychol. Open 2019, 6, 205510291987166. [Google Scholar] [CrossRef]
- Lange, M.; Licaj, I.; Clarisse, B.; Humbert, X.; Grellard, J.; Tron, L.; Joly, F. Cognitive complaints in cancer survivors and expectations for support: Results from a web–based survey. Cancer Med. 2019, 8, 2654–2663. [Google Scholar] [CrossRef] [PubMed]
- Joly, F.; Lange, M.; Rigal, O.; Correia, H.; Giffard, B.; Beaumont, J.L.; Clisant, S.; Wagner, L. French version of the Functional Assessment of Cancer Therapy–Cognitive Function (FACT-Cog) version 3. Support. Care Cancer 2012, 20, 3297–3305. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.E.; Beckjord, E.; Bovbjerg, D.H.; Low, C.A.; Posluszny, D.M.; Lowery, A.E.; Dew, M.A.; Nutt, S.; Arvey, S.R.; Rechis, R. Prevalence of perceived cognitive dysfunction in survivors of a wide range of cancers: Results from the 2010 LIVESTRONG survey. J. Cancer Surviv. 2016, 10, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Bray, V.J.; Dhillon, H.M.; Vardy, J.L. Systematic review of self-reported cognitive function in cancer patients following chemotherapy treatment. J. Cancer Surviv. 2018, 12, 537–559. [Google Scholar] [CrossRef]
- Wefel, J.S.; Lenzi, R.; Theriault, R.L.; Davis, R.N.; Meyers, C.A. The cognitive sequelae of standard-dose adjuvant chemotherapy in women with breast carcinoma: Results of a prospective, randomized, longitudinal trial. Cancer 2004, 100, 2292–2299. [Google Scholar] [CrossRef]
- Collins, B.; MacKenzie, J.; Tasca, G.A.; Scherling, C.; Smith, A. Cognitive effects of chemotherapy in breast cancer patients: A dose-response study: Cognitive effects of chemotherapy in breast cancer patients. Psycho-Oncology 2013, 22, 1517–1527. [Google Scholar] [CrossRef]
- Collins, B.; Mackenzie, J.; Stewart, A.; Bielajew, C.; Verma, S. Cognitive effects of chemotherapy in post-menopausal breast cancer patients 1 year after treatment. Psycho-Oncology 2009, 18, 134–143. [Google Scholar] [CrossRef]
- Biglia, N.; Bounous, V.E.; Malabaila, A.; Palmisano, D.; Torta, D.M.E.; D’Alonzo, M.; Sismondi, P.; Torta, R. Objective and self-reported cognitive dysfunction in breast cancer women treated with chemotherapy: A prospective study: Chemotherapy-induced cognitive dysfunction. Eur. J. Cancer Care 2012, 21, 485–492. [Google Scholar] [CrossRef]
- Wagner, L.I.; Gray, R.J.; Sparano, J.A.; Whelan, T.J.; Garcia, S.F.; Yanez, B.; Tevaarwerk, A.J.; Carlos, R.C.; Albain, K.S.; Olson, J.A.; et al. Patient-Reported Cognitive Impairment Among Women With Early Breast Cancer Randomly Assigned to Endocrine Therapy Alone Versus Chemoendocrine Therapy: Results From TAILORx. JCO 2020, 38, 1875–1886. [Google Scholar] [CrossRef] [PubMed]
- Castel, H.; Denouel, A.; Lange, M.; Tonon, M.-C.; Dubois, M.; Joly, F. Biomarkers Associated with Cognitive Impairment in Treated Cancer Patients: Potential Predisposition and Risk Factors. Front. Pharm. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Hermelink, K.; Voigt, V.; Kaste, J.; Neufeld, F.; Wuerstlein, R.; Buhner, M.; Munzel, K.; Rjosk-Dendorfer, D.; Grandl, S.; Braun, M.; et al. Elucidating Pretreatment Cognitive Impairment in Breast Cancer Patients: The Impact of Cancer-related Post-traumatic Stress. JNCI J. Natl. Cancer Inst. 2015, 107, djv099. [Google Scholar] [CrossRef] [PubMed]
- Earnheart, J.C.; Schweizer, C.; Crestani, F.; Iwasato, T.; Itohara, S.; Mohler, H.; Luscher, B. GABAergic Control of Adult Hippocampal Neurogenesis in Relation to Behavior Indicative of Trait Anxiety and Depression States. J. Neurosci. 2007, 27, 3845–3854. [Google Scholar] [CrossRef] [PubMed]
- Leng, Y.; McEvoy, C.T.; Allen, I.E.; Yaffe, K. Association of Sleep-Disordered Breathing With Cognitive Function and Risk of Cognitive Impairment: A Systematic Review and Meta-analysis. JAMA Neurol. 2017, 74, 1237. [Google Scholar] [CrossRef] [PubMed]
- Palesh, O.; Scheiber, C.; Kesler, S.; Mustian, K.; Koopman, C.; Schapira, L. Management of side effects during and post-treatment in breast cancer survivors. Breast J. 2018, 24, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Schagen, S.B.; Das, E.; Vermeulen, I. Information about chemotherapy-associated cognitive problems contributes to cognitive problems in cancer patients: Priming cognitive problems. Psycho-Oncology 2012, 21, 1132–1135. [Google Scholar] [CrossRef]
- Lange, M.; Hardy-Léger, I.; Licaj, I.; Pistilli, B.; Rigal, O.; Le Fel, J.; Lévy, C.; Capel, A.; Coutant, C.; Meyer, J.; et al. Cognitive impairment in breast cancer patients before surgery: Results from a CANTO cohort subgroup. Cancer Epidemiol. Biomark. Prev. 2020, 29, 1759–1766. [Google Scholar] [CrossRef]
- Ganz, P.A.; Petersen, L.; Castellon, S.A.; Bower, J.E.; Silverman, D.H.S.; Cole, S.W.; Irwin, M.R.; Belin, T.R. Cognitive Function After the Initiation of Adjuvant Endocrine Therapy in Early-Stage Breast Cancer: An Observational Cohort Study. JCO 2014, 32, 3559–3567. [Google Scholar] [CrossRef]
- Underwood, E.A.; Jerzak, K.J.; Lebovic, G.; Rochon, P.A.; Elser, C.; Pritchard, K.I.; Tierney, M.C. Cognitive effects of adjuvant endocrine therapy in older women treated for early-stage breast cancer: A 1-year longitudinal study. Support. Care Cancer 2019, 27, 3035–3043. [Google Scholar] [CrossRef]
- Underwood, E.A.; Rochon, P.A.; Moineddin, R.; Lee, P.E.; Wu, W.; Pritchard, K.I.; Tierney, M.C. Cognitive sequelae of endocrine therapy in women treated for breast cancer: A meta-analysis. Breast Cancer Res. Treat. 2018, 168, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Galea, L.A.M.; Frick, K.M.; Hampson, E.; Sohrabji, F.; Choleris, E. Why estrogens matter for behavior and brain health. Neurosci. Biobehav. Rev. 2017, 76, 363–379. [Google Scholar] [CrossRef] [PubMed]
- Schilder, C.M.; Seynaeve, C.; Beex, L.V.; Boogerd, W.; Linn, S.C.; Gundy, C.M.; Huizenga, H.M.; Nortier, J.W.; van de Velde, C.J.; van Dam, F.S.; et al. Effects of Tamoxifen and Exemestane on Cognitive Functioning of Postmenopausal Patients With Breast Cancer: Results From the Neuropsychological Side Study of the Tamoxifen and Exemestane Adjuvant Multinational Trial. JCO 2010, 28, 1294–1300. [Google Scholar] [CrossRef] [PubMed]
- Boykoff, N.; Moieni, M.; Subramanian, S.K. Confronting chemobrain: An in-depth look at survivors’ reports of impact on work, social networks, and health care response. J. Cancer Surviv. 2009, 3, 223. [Google Scholar] [CrossRef]
- Von Ah, D.; Storey, S.; Crouch, A. Relationship between self-reported cognitive function and work-related outcomes in breast cancer survivors. J. Cancer Surviv. 2018, 12, 246–255. [Google Scholar] [CrossRef]
- Wagner, L.I.; Sweet, J.J.; Butt, Z.; Lai, J.S.; Cella, D. Measuring patient self-reported cognitive function: Development of the Functional Assessment of Cancer Therapy–Cognitive Function Instrument. J. Support Oncol. 2009, 7, W32–W39. [Google Scholar]
- Brunet, A.; St-Hilaire, A.; Jehel, L.; King, S. Validation of a French Version of the Impact of Event Scale-Revised. Can. J. Psych. 2003, 48, 56–61. [Google Scholar] [CrossRef]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the Impact of Event Scale—Revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef]
- Yellen, S.B.; Cella, D.F.; Webster, K.; Blendowski, C.; Kaplan, E. Measuring fatigue and other anemia-related symptoms with the Functional Assessment of Cancer Therapy (FACT) measurement system. J. Pain Symptom Manag. 1997, 13, 63–74. [Google Scholar] [CrossRef]
- Cleeland, C.; Wang, X. Measuring and understanding fatigue. Oncology 1999, 13, 91–97. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Razavi, D.; Delvaux, N.; Farvacques, C.; Robaye, E. Screening for Adjustment Disorders and Major Depressive Disorders in Cancer In-Patients. Br. J. Psychiatry 1990, 156, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.-S.; Wagner, L.I.; Jacobsen, P.B.; Cella, D. Self-reported cognitive concerns and abilities: Two sides of one coin?: Cognitive concerns versus cognitive abilities. Psycho-Oncology 2014, 23, 1133–1141. [Google Scholar] [CrossRef] [PubMed]
- Lange, M.; Heutte, N.; Morel, N.; Eustache, F.; Joly, F.; Giffard, B. Cognitive complaints in cancer: The French version of the Functional Assessment of Cancer Therapy–Cognitive Function (FACT-Cog), normative data from a healthy population. Neuropsychol. Rehabil. 2016, 26, 392–409. [Google Scholar] [CrossRef]
- Hidalgo, B.; Goodman, M. Multivariate or Multivariable Regression? Am. J. Public Health 2013, 103, 39–40. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| N (%) | All Sample | Participants with Current Cognitive Complaints (n = 657) | Participants without Current Cognitive Complaints (n = 736) | p |
|---|---|---|---|---|
| Age in years | ||||
| 21–44 | 322 (23.1%) | 226 (34.4%) | 96 (13.0%) | <0.001 |
| 45–64 | 940 (67.5%) | 413 (62.9%) | 527 (71.6%) | |
| ≥65 | 131 (9.4%) | 18 (2.7%) | 113 (15.4%) | |
| Education level | ||||
| Low | 44 (3.2%) | 17 (2.6%) | 27 (3.7%) | 0.284 |
| Middle | 373 (26.8%) | 168 (25.6%) | 205 (27.8%) | |
| High | 976 (70.0%) | 472 (71.8%) | 504 (68.5%) | |
| Employment | ||||
| Full-time or part-time | 787 (56.5%) | 384 (58.5%) | 403 (54.8%) | <0.001 |
| Sick leave | 148 (10.6%) | 100 (15.2%) | 48 (6.5%) | |
| Student, retired | 249 (17.9%) | 58 (8.8%) | 191 (25.9%) | |
| Unemployed | 64 (4.6%) | 39 (5.9%) | 25 (3.4%) | |
| Other | 145 (10.4%) | 76 (11.6%) | 69 (9.4%) | |
| Married/partnered | ||||
| No | 364 (26.1%) | 159 (24.2%) | 205 (27.9%) | 0.121 |
| Yes | 1029 (73.9%) | 498 (75.8%) | 531 (72.1%) | |
| Cancer without metastasis | ||||
| Yes | 1236 (88.7%) | 575 (87.5%) | 661 (89.8%) | 0.177 |
| No | 157 (11.3%) | 82 (12.5%) | 75 (10.2%) | |
| Post-cancer curative treatment time | ||||
| ≤1 year | 373 (26.8%) | 210 (32.0%) | 163 (22.1%) | <0.001 |
| 1–3 years | 336 (24.1%) | 167 (25.4%) | 169 (23.0%) | |
| ≥3 years | 684 (49.1%) | 280 (42.6%) | 404 (54.9%) | |
| BMI | ||||
| Insufficient | 51 (3.7%) | 30 (4.6%) | 21 (2.9%) | 0.037 |
| Normal | 802 (57.6%) | 377 (57.4%) | 425 (57.7%) | |
| Overweight | 377 (27.0%) | 162 (24.6%) | 215 (29.2%) | |
| Obesity | 163 (11.7%) | 88 (13.4%) | 75 (10.2%) | |
| Frequency of psychotropic treatments | ||||
| Never | 914 (65.6%) | 389 (59.2%) | 525 (71.3%) | <0.001 |
| <1/month | 169 (12.1%) | 91 (13.8%) | 78 (10.6%) | |
| >1/month and <1/week | 77 (5.5%) | 38 (5.8%) | 39 (5.3%) | |
| >1/week | 233 (16.8%) | 139 (21.2%) | 94 (12.8%) | |
| Self-reported sleep difficulties | ||||
| Never | 95 (6.8%) | 34 (5.2%) | 61 (8.3%) | <0.001 |
| Sometimes | 481 (34.5%) | 197 (30.0%) | 284 (38.6%) | |
| Often | 817 (58.7%) | 426 (64.8%) | 391 (53.1%) | |
| Physical activity | ||||
| None or < once a week | 446 (32.0%) | 203 (30.9%) | 243 (33.0%) | 0.431 |
| Once a week | 255 (18.3%) | 116 (17.7%) | 139 (18.9%) | |
| Twice a week | 362 (26.0%) | 184 (28.0%) | 178 (24.2%) | |
| ≥3 times a week | 330 (23.7%) | 154 (23.4%) | 176 (23.9%) | |
| History of neurological disease | ||||
| No | 1316 (94.5%) | 625 (95.1%) | 691 (93.9%) | 0.311 |
| Yes | 77 (5.5%) | 32 (4.9%) | 45 (6.1%) | |
| Pre-existing knowledge 1 | ||||
| No | 842 (60.5%) | 359 (54.6%) | 483 (65.6%) | <0.001 |
| Yes | 551 (39.5%) | 298 (45.4%) | 253 (34.4%) |
| Questionnaires | Median | Mean | SD | |
|---|---|---|---|---|
| Cognitive complaints (FACT-Cog) | PCI (0–72) | 50 | 48.1 | 15.6 |
| PCA (0–28) | 15 | 15.6 | 5.6 | |
| Oth (0–16) | 16 | 14.4 | 2.6 | |
| QoL (0–16) | 8 | 8.8 | 4.7 | |
| HADS | Depression (0–21) | 5 | 5.4 | 3.5 |
| Anxiety (0–21) | 8 | 8.9 | 4.0 | |
| Post-traumatic stress symptoms (IES-R) (0–88) | 21 | 23.2 | 16.0 | |
| Fatigue (FACIT-F) (0–52) | 19 | 19.5 | 11.8 | |
| Multivariable | 1 = Chemotherapy | 2 = IES-R | 3 = Endocrine Therapy | |||
|---|---|---|---|---|---|---|
| Mean (SD) | OR | 95% CI | OR | 95% CI | OR | 95% CI |
| Chemotherapy | ||||||
| No | 1.00 | Reference | 1.00 | Reference | ||
| Yes | 2.26 | 1.67–3.05 | 2.28 | 1.68–3.08 | ||
| Post-cancer curative treatment time in years | ||||||
| ≤1 | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference |
| 1–3 | 0.98 | 0.70–1.37 | 1.00 | 0.71–1.41 | 1.05 | 0.75–1.46 |
| ≥3 | 0.79 | 0.59–1.08 | 0.83 | 0.61–1.12 | 0.89 | 0.66–1.22 |
| Cancer without metastasis | ||||||
| Yes | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference |
| No | 1.04 | 0.72–1.50 | 1.04 | 0.72–1.51 | 1.23 | 0.86–1.77 |
| Age in years | ||||||
| 21–44 | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference |
| 45–64 | 0.37 | 0.28–0.51 | 0.37 | 0.27–0.50 | 0.33 | 0.24–0.44 |
| ≥65 | 0.14 | 0.07–0.27 | 0.15 | 0.07–0.30 | 0.11 | 0.05–0.21 |
| Employment | ||||||
| Full-time or part-time | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference |
| Sick leave | 1.64 | 1.08–2.49 | 1.57 | 1.03–2.52 | 1.67 | 1.11–2.52 |
| Student/retired | 0.69 | 0.45–1.04 | 0.67 | 0.44–1.03 | 0.70 | 0.46–1.05 |
| Unemployed | 1.62 | 0.93–2.84 | 1.43 | 0.81–2.52 | 1.69 | 0.97–2.94 |
| Other | 1.24 | 0.84–1.82 | 1.18 | 0.80–1.75 | 1.25 | 0.86–1.83 |
| Education level | ||||||
| Low | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference |
| Middle | 1.02 | 0.50–2.07 | 1.02 | 0.50–2.10 | 1.05 | 0.52–2.13 |
| High | 1.11 | 0.55–2.23 | 1.13 | 0.56–2.28 | 1.13 | 0.57–2.25 |
| Self-reported sleep difficulties | ||||||
| Never | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference |
| Sometimes | 1.51 | 0.91–2.49 | 1.41 | 0.85–2.33 | 1.51 | 0.92–2.49 |
| Often | 2.41 | 1.47–3.95 | 2.08 | 1.26–3.42 | 2.34 | 1.43–3.84 |
| Frequency of psychotropic treatments | ||||||
| Never | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference |
| <1/month | 1.56 | 1.08–2.26 | 1.51 | 1.04–2.19 | 1.52 | 1.06–2.18 |
| >1/month and <1/week | 1.23 | 0.73–2.07 | 1.04 | 0.61–1.77 | 1.16 | 0.70–1.93 |
| >1/week | 1.70 | 1.23–2.36 | 1.60 | 1.15–2.23 | 1.69 | 1.23–2.34 |
| Physical activity | ||||||
| None or <once a week | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference |
| Once a week | 0.92 | 0.66–1.30 | 0.92 | 0.65–1.29 | 0.92 | 0.66–1.30 |
| Twice a week | 1.30 | 0.95–1.76 | 1.28 | 0.94–1.74 | 1.31 | 0.96–1.77 |
| ≥3 times a week | 1.08 | 0.78–1.48 | 1.11 | 0.80–1.53 | 1.10 | 0.80–1.51 |
| Pre-existing knowledge 1 | ||||||
| Yes | 1.00 | Reference | 1.00 | Reference | 1.00 | Reference |
| No | 1.23 | 0.96–1.56 | 1.25 | 0.98–1.59 | 1.35 | 1.07–1.71 |
| Stress symptoms (IES-R) | ||||||
| No | 1.00 | Reference | ||||
| Yes | 2.05 | 1.57–2.69 | ||||
| Endocrine therapy | ||||||
| Never | 1 | Reference | ||||
| Former | 0.96 | 0.67–1.39 | ||||
| Current | 1.11 | 0.84–1.47 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boscher, C.; Joly, F.; Clarisse, B.; Humbert, X.; Grellard, J.-M.; Binarelli, G.; Tron, L.; Licaj, I.; Lange, M. Perceived Cognitive Impairment in Breast Cancer Survivors and Its Relationships with Psychological Factors. Cancers 2020, 12, 3000. https://doi.org/10.3390/cancers12103000
Boscher C, Joly F, Clarisse B, Humbert X, Grellard J-M, Binarelli G, Tron L, Licaj I, Lange M. Perceived Cognitive Impairment in Breast Cancer Survivors and Its Relationships with Psychological Factors. Cancers. 2020; 12(10):3000. https://doi.org/10.3390/cancers12103000
Chicago/Turabian StyleBoscher, Clémence, Florence Joly, Bénédicte Clarisse, Xavier Humbert, Jean-Michel Grellard, Giulia Binarelli, Laure Tron, Idlir Licaj, and Marie Lange. 2020. "Perceived Cognitive Impairment in Breast Cancer Survivors and Its Relationships with Psychological Factors" Cancers 12, no. 10: 3000. https://doi.org/10.3390/cancers12103000
APA StyleBoscher, C., Joly, F., Clarisse, B., Humbert, X., Grellard, J.-M., Binarelli, G., Tron, L., Licaj, I., & Lange, M. (2020). Perceived Cognitive Impairment in Breast Cancer Survivors and Its Relationships with Psychological Factors. Cancers, 12(10), 3000. https://doi.org/10.3390/cancers12103000