Geriatric Nutritional Risk Index Less Than 92 Is a Predictor for Late Postpancreatectomy Hemorrhage Following Pancreatoduodenectomy: A Retrospective Cohort Study

 , ,
, ,
Simple Summary
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics and Univariate Analysis for PPH risk Following PD
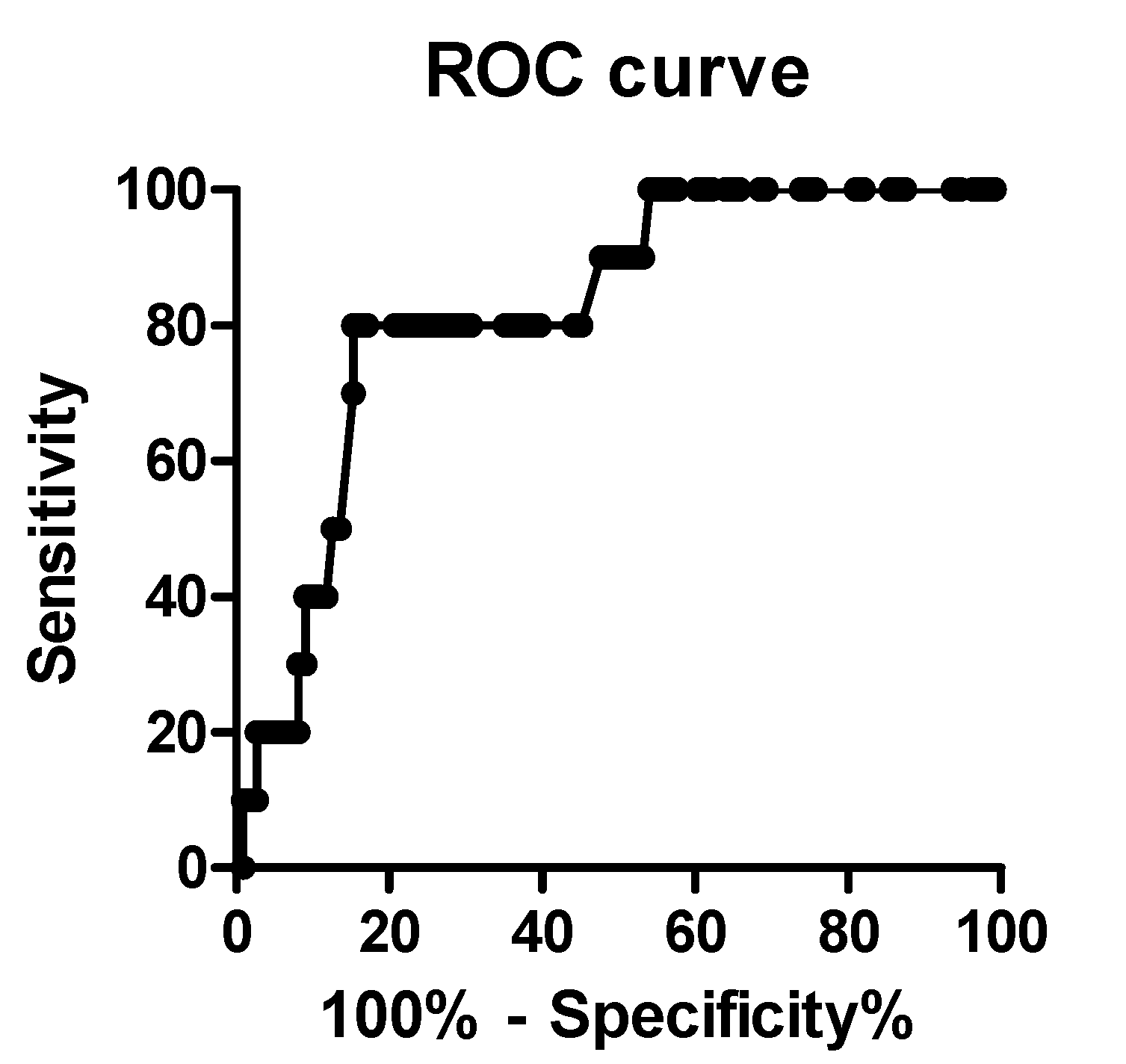
2.2. Receiver Operating Characteristic (ROC) Curve Analysis
2.3. Univariate Analysis of a GNRI < 92 for PPH
2.4. Multivariable with Logistic Regression Analyses
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Collection of Clinical and Laboratory Data
4.3. Definition of GNRI
4.4. Perioperative Management and Surgical Technique for PD
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Kimura, W.; Miyata, H.; Gotoh, M.; Hirai, I.; Kenjo, A.; Kitagawa, Y.; Shimada, M.; Baba, H.; Tomita, N.; Nakagoe, T.; et al. A pancreaticoduodenectomy risk model derived from 8575 cases from a national single-race population (Japanese) using a web-based data entry system: The 30-day and in-hospital mortality rates for pancreaticoduodenectomy. Ann. Surg. 2014, 259, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.S.; Zhou, Z.; Simons, J.P. A simple risk score to predict in-hospital mortality after pancreatic resection for cancer. Ann. Surg. Oncol. 2010, 17, 1802–1807. [Google Scholar] [CrossRef]
- Welsch, T.; Eisele, H.; Zschabitz, S.; Hinz, U.; Buchler, M.W.; Wente, M.N. Critical appraisal of the International Study Group of Pancreatic Surgery (ISGPS) consensus definition of postoperative hemorrhage after pancreatoduodenectomy. Langenbecks Arch. Surg. 2011, 396, 783–791. [Google Scholar] [CrossRef]
- Wente, M.N.; Veit, J.A.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, G.J.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; et al. Postpancreatectomy hemorrhage (PPH): An International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007, 142, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Darnis, B.; Lebeau, R.; Chopin-Laly, X.; Adham, M. Postpancreatectomy hemorrhage (PPH): Predictors and management from a prospective database. Langenbecks Arch. Surg. 2013, 398, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Stampfl, U.; Hackert, T.; Sommer, C.M.; Klauss, M.; Bellemann, N.; Siebert, S.; Werner, J.; Richeter, G.M.; Kauczor, H.U.; Radeleff, B. Superselective embolization for the management of postpancreatectomy hemorrhage: A single-center experience in 25 patients. J. Vasc. Interv. Radiol. 2012, 23, 504–510. [Google Scholar] [CrossRef]
- Limongelli, P.; Khorsandi, S.E.; Pai, M.; Jackson, J.E.; Tait, P.; Tierris, J.; Habib, N.A.; Williamson, R.C.; Jiao, L.R. Management of delayed postoperative hemorrhage after pancreaticoduodenectomy: A meta-analysis. Arch. Surg. 2008, 143, 1001–1007. [Google Scholar] [CrossRef]
- Garces, A.A.D.; Andrianello, S.; Maechegiani, G.; Piccolo, R.; Secchettin, E.; Paiella, S.; Malleo, G.; Salvia, R.; Bassi, C. Reappraisal of postpancreatectomy hemorrhage (PPH) classifications: Do we need to redefine Grade A and B? HPB (Oxford) 2018, 20, 702–707. [Google Scholar] [CrossRef]
- Asari, S.; Matsumoto, I.; Toyama, H.; Yamaguchi, M.; Okada, T.; Shinzeki, M.; Goto, T.; Ajiki, T.; Fukumoto, T.; Ku, Y. Recommendation of treatment strategy for postpancreatectomy hemorrhage: Lessons from a single-center experience in 35 patients. Pancreatology 2016, 16, 454–463. [Google Scholar] [CrossRef] [PubMed]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric Nutritional Risk Index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef]
- Funamizu, N.; Nakabayashi, Y.; Iida, T.; Kurihara, K. Geriatric nutritional risk index predicts surgical site infection after pancreaticoduodenectomy. Mol. Clin. Oncol. 2018, 9, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Hackert, T.; Büchler, M.W.; Werner, J. Current state of surgical management of pancreatic cancer. Cancers (Basel) 2011, 3, 1253–1273. [Google Scholar] [CrossRef] [PubMed]
- Bachet, J.B.; Marechal, R.; Van Laethem, J.L. Treatment of pancreatic cancer: What can we really predict today? Cancers (Basel) 2011, 3, 675–699. [Google Scholar] [CrossRef] [PubMed]
- Hartwig, W.; Hackert, T.; Hinz, U.; Hassenpflug, M.; Strobel, O.; Buchler, M.W.; Werner, J. Multivisceral resection for pancreatic malignancies: Risk-analysis and long-term outcome. Ann. Surg. 2009, 250, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Abu, H.M.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef]
- Müssle, B.; Wierick, A.; Distler, M.; Weitz, J.; Welsch, T. Falciform ligament wrap for prevention of gastroduodenal artery bleed after pancreatoduodenectomy. J. Surg. Res. 2017, 207, 215–222. [Google Scholar]
- DeOliveira, M.L.; Winter, J.M.; Schafer, M. Assessment of complications after pancreatic surgery: A novel grading system applied to 633 patients undergoing pancreaticoduodenectomy. Ann. Surg. 2006, 244, 931–937. [Google Scholar] [CrossRef]
- Ricci, C.; Casadei, R.; Buscemi, S.; Minni, F. Late postpancreatectomy hemorrhage after pancreaticoduodenectomy: Is it possible to recognize risk factors? JOP. J. Pancreas 2012, 13, 193–198. [Google Scholar]
- Miura, F.; Asano, T.; Amano, H.; Yoshida, M.; Toyota, N.; Wada, K.; Kato, K.; Yamazaki, E.; Kadowaki, S.; Shibuya, M.; et al. Management of postoperative arterial hemorrhage after pancreato-biliary surgery according to the site of bleeding: Re-laparotomy or interventional radiology. J. Hepatobiliary Pancreat. Surg. 2009, 16, 56–63. [Google Scholar] [CrossRef]
- Wellner, U.F.; Kulemann, B.; Lapshyn, H.; Hoeppner, J.; Sick, O.; Makowiec, F.; Bausch, D.; Hopt, U.T.; Keck, T. Postpancreatectomy hemorrhage--incidence, treatment, and risk factors in over 1,000 pancreatic resections. J. Gastrointest. Surg. 2014, 18, 464–475. [Google Scholar] [CrossRef]
- Izumo, W.; Higuchi, R.; Yazawa, T.; Uemura, S.; Shiihara, M.; Yamamoto, M. Evaluation of preoperative risk factors for postpancreatectomy hemorrhage. Langenbecks Arch. Surg. 2019, 404, 967–974. [Google Scholar] [CrossRef] [PubMed]
- Funamizu, N.; Nakabayashi, Y.; Kurihara, K. Lower geriatric nutritional risk index predicts postoperative pancreatic fistula in patients with distal pancreatectomy. Mol. Clin. Oncol. 2020, 12, 134–137. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, M.; Okazaki, M.; Tsuchiya, K.; Kawaguchi, H.; Nitta, K. Geriatric Nutritional Risk Index Is a Simple Predictor of Mortality in Chronic Hemodialysis Patients. Blood Purify 2015, 39, 281–287. [Google Scholar] [CrossRef] [PubMed]
- Kaneko, H.; Suzuki, S.; Goto, M.; Yuzawa, Y.; Arita, T.; Yagi, N.; Murata, N.; Kato, Y.; Kano, H.; Matsuno, S.; et al. Geriatric nutritional risk index in hospitalized heart failure patients. Int. J. Cardiol. 2015, 181, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Naumann, P.; Eberlein, J.; Farnia, B.; Hackert, T.; Debus, J.; Combs, S.E. Continued weight loss and sarcopenia predict poor outcomes in locally advanced pancreatic cancer treated with chemoradiation. Cancers (Basel) 2019, 11, 709. [Google Scholar] [CrossRef] [PubMed]
- Ichikawa, K.; Mizuno, S.; Hayasaki, A.; Kishiwada, M.; Fujii, T.; Iizawa, Y.; Kato, H.; Tanemura, A.; Murata, Y.; Azumi, Y.; et al. Prognostic Nutritional Index After Chemoradiotherapy Was the Strongest Prognostic Predictor Among Biological and Conditional Factors in Localized Pancreatic Ductal Adenocarcinoma Patients. Cancers (Basel) 2019, 11, 514. [Google Scholar] [CrossRef]
- Wang, Y.; Wang, L.; Fang, M.; Li, L.; Song, T.; Zhan, W.; Xu, H. Prognostic Value of the Geriatric Nutritional Risk Index in Patients Exceeding 70 Years Old with Esophageal Squamous Cell Carcinoma. Nutr. Cancer 2019, 8, 1–7. [Google Scholar] [CrossRef]
- Kushiyama, S.; Sakurai, K.; Kubo, N.; Tamamori, Y.; Nishii, T.; Tachimori, A.; Inoue, T.; Maeda, K. The Preoperative Geriatric Nutritional Risk Index Predicts Postoperative Complications in Elderly Patients with Gastric Cancer Undergoing Gastrectomy. In Vivo 2018, 32, 1667–1672. [Google Scholar] [CrossRef]
- Iguchi, T.; Sugimachi, K.; Mano, Y.; Motomura, T.; Sugiyama, M.; Ota, M.; Ikebe, M.; Esaki, T.; Yoshizumi, T.; Morita, M.; et al. Prognostic Impact of Geriatric Nutritional Risk Index in Patients With Synchronous Colorectal Liver Metastasis. Anticancer Res. 2020, 40, 4165–4171. [Google Scholar] [CrossRef]
- Hirahara, N.; Matsubara, T.; Fujii, Y.; Kaji, S.; Hyakudomi, R.; Yamamoto, T.; Uchida, Y.; Miyazaki, Y.; Ishitobi, K.; Kawabata, Y.; et al. Preoperative geriatric nutritional risk index is a useful prognostic indicator in elderly patients with gastric cancer. Oncotarget 2020, 11, 2345–2356. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | PPH Group | Non-PPH Group | p-Value |
|---|---|---|---|
| (n = 10) | (n = 111) | ||
| Gender | |||
| Male vs Female | 10 vs. 0 | 69 vs. 42 | p = 0.01 |
| Age (years) | 76.1 ± 2.0 | 70.8 ± 1.1 | p = 0.15 |
| Body mass index | 22.7 ± 0.7 | 22.1 ± 0.3 | p = 0.55 |
| ASA classification | |||
| 1 or 2 | 8 (80.0%) | 97 (87.4%) | p = 0.51 |
| 3 | 2 (20.0%) | 14 (12.6%) | |
| Pancreatic or periampullary | 8 (80.0%) | 91 (82.0%) | p = 0.88 |
| adenocarcinoma (%) | |||
| Smoking habit (%) | 2 (20.0%) | 8 (7.2%) | p = 0.19 |
| Alcohol intake (%) | 0 (0.0%) | 3 (2.7%) | p = 0.60 |
| Diabetes mellitus (%) | 1 (10.0%) | 36 (32.4%) | p = 0.14 |
| Neoadjuvant chemotherapy (%) | 0 (0.0%) | 9 (8.1%) | p = 0.35 |
| Preoperative biliary drainage (%) | 6 (60.0%) | 35 (31.5%) | p = 0.09 |
| Preoperative albumin (g/L) | 3.3 ± 0.1 | 3.9 ± 0.1 | p < 0.001 |
| Robotic/open PD | 2/8 | 16/95 | p = 0.63 |
| GNRI | 89.2 ± 1.9 | 98.3 ± 0.8 | p = 0.001 |
| 92< | 8 | 19 | p < 0.001 |
| 92≥ | 2 | 92 | |
| Time taken for the operation (min) | 578.1 ± 42.2 | 497.2 ± 15.1 | p = 0.13 |
| Estimated blood loss (ml) | 712.7 ± 103.5 | 656.2 ± 63.3 | p = 0.69 |
| Blood transfusion (%) | 2 (20.0%) | 25 (22.5%) | p = 0.85 |
| Portal vein resection (%) | 0 (0.0%) | 6 (5.4%) | p = 0.45 |
| Bile leakage (%) | 2 (20.0%) | 5 (4.5%) | p = 0.09 |
| Postoperative pancreatic fistula (%) | 7 (70.0%) | 27 (24.3%) | p = 0.005 |
| Grade B or C (%) | |||
| Rate of intraabdominal infection (%) | 6 (60.0%) | 24 (22.5%) | p = 0.02 |
| Postoperative hospital stays (day) | 49.0 ± 8.2 | 22.9 ± 5.5 | p < 0.001 |
| Variables | Odds Ratio | 95% Confidence Interval | p-Value |
|---|---|---|---|
| Gender | 0.001 | Not available | p = 0.97 |
| Intra-abdominal abscess | 0.58 | 0.01–0.46 | p = 0.65 |
| POPF | 4.11 | 0.44–38.29 | p = 0.21 |
| GNRI < 92 | 0.07 | 0.01–0.46 | p = 0.006 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Funamizu, N.; Omura, K.; Takada, Y.; Ozaki, T.; Mishima, K.; Igarashi, K.; Wakabayashi, G. Geriatric Nutritional Risk Index Less Than 92 Is a Predictor for Late Postpancreatectomy Hemorrhage Following Pancreatoduodenectomy: A Retrospective Cohort Study. Cancers 2020, 12, 2779. https://doi.org/10.3390/cancers12102779
Funamizu N, Omura K, Takada Y, Ozaki T, Mishima K, Igarashi K, Wakabayashi G. Geriatric Nutritional Risk Index Less Than 92 Is a Predictor for Late Postpancreatectomy Hemorrhage Following Pancreatoduodenectomy: A Retrospective Cohort Study. Cancers. 2020; 12(10):2779. https://doi.org/10.3390/cancers12102779
Chicago/Turabian StyleFunamizu, Naotake, Kenji Omura, Yasutsugu Takada, Takahiro Ozaki, Kohei Mishima, Kazuharu Igarashi, and Go Wakabayashi. 2020. "Geriatric Nutritional Risk Index Less Than 92 Is a Predictor for Late Postpancreatectomy Hemorrhage Following Pancreatoduodenectomy: A Retrospective Cohort Study" Cancers 12, no. 10: 2779. https://doi.org/10.3390/cancers12102779
APA StyleFunamizu, N., Omura, K., Takada, Y., Ozaki, T., Mishima, K., Igarashi, K., & Wakabayashi, G. (2020). Geriatric Nutritional Risk Index Less Than 92 Is a Predictor for Late Postpancreatectomy Hemorrhage Following Pancreatoduodenectomy: A Retrospective Cohort Study. Cancers, 12(10), 2779. https://doi.org/10.3390/cancers12102779