Stereotactic Body Radiotherapy as a Salvage Therapy after Incomplete Radiofrequency Ablation for Hepatocellular Carcinoma: A Retrospective Propensity Score Matching Study

 , , , and
, , , and
Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Treatment-Related Outcomes
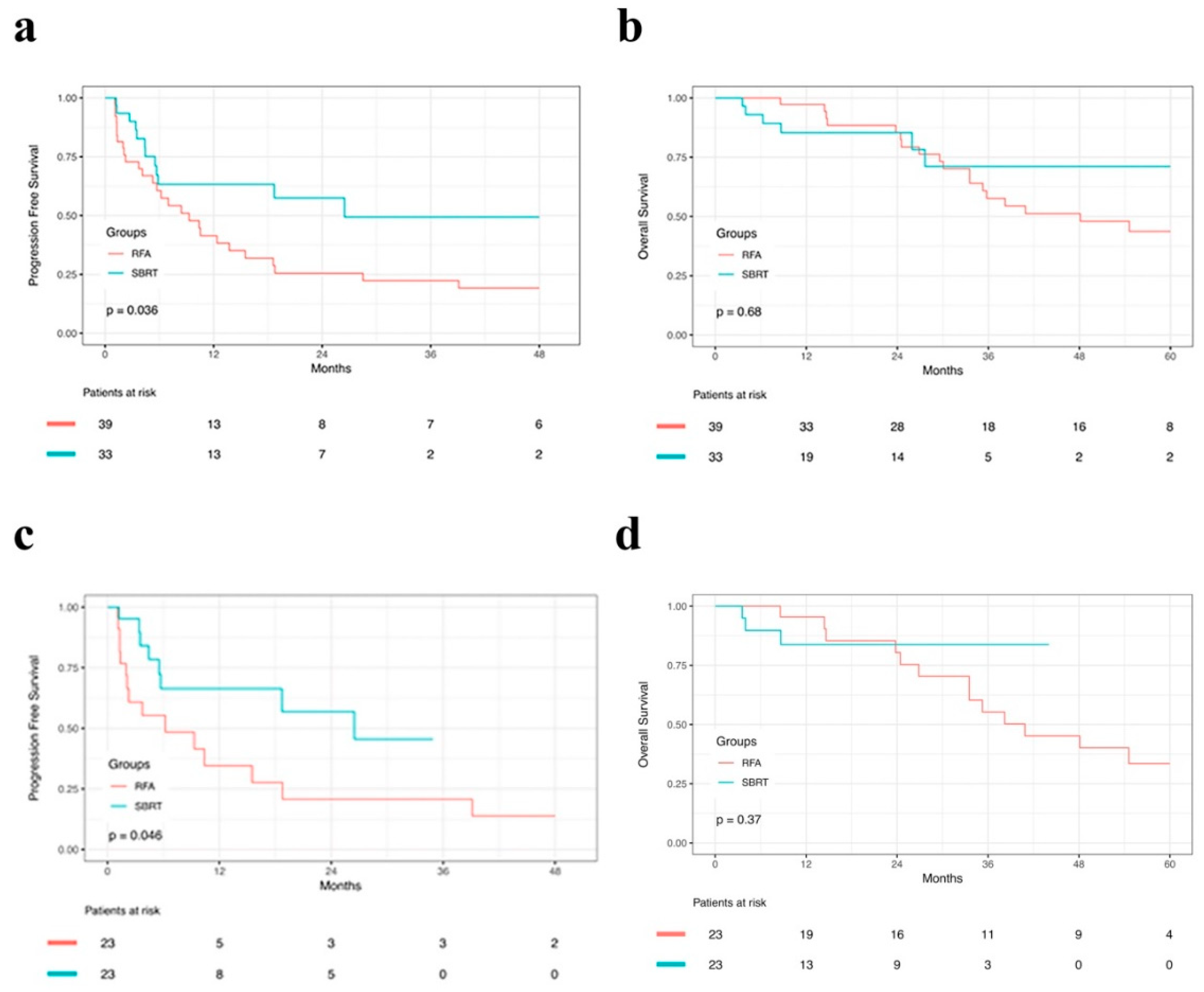
2.3. Progression-Free Survival before and after PSM
2.4. Overall Survival before and after PSM
2.5. Prognostic Factors
3. Discussion
4. Materials and Methods
4.1. Patient Selection
4.2. Protocol for RFA
4.3. Protocol for SBRT
4.4. Treatment Assessment and Follow-up
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Altekruse, S.F.; McGlynn, K.A.; Reichman, M.E. Hepatocellular carcinoma incidence, mortality, and survival trends in the United States from 1975 to 2005. J. Clin. Oncol. 2009, 27, 1485–1491. [Google Scholar] [CrossRef] [PubMed]
- Njei, B.; Rotman, Y.; Ditah, I.; Lim, J.K. Emerging trends in hepatocellular carcinoma incidence and mortality. Hepatology 2015, 61, 191–199. [Google Scholar] [CrossRef] [PubMed]
- He, W.; Zheng, Y.; Zou, R.; Shen, J.; Yang, J.; Qiu, J.; Tao, Q.; Liu, W.; Yang, Z.; Zhang, Y.; et al. Long- versus short-interval follow-up after resection of hepatocellular carcinoma: a retrospective cohort study. Cancer Commun. 2018, 38, 26. [Google Scholar] [CrossRef] [PubMed]
- Heimbach, J.K.; Kulik, L.M.; Finn, R.S.; Sirlin, C.B.; Abecassis, M.M.; Roberts, L.R.; Zhu, A.X.; Murad, M.H.; Marrero, J.A. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatology 2018, 67, 358–380. [Google Scholar] [CrossRef] [PubMed]
- Vogel, A.; Cervantes, A.; Chau, I.; Daniele, B.; Llovet, J.; Meyer, T.; Nault, J.-C.; Neumann, U.; Ricke, J.; Sangro, B.; et al. Hepatocellular carcinoma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann. Oncol. 2018, 29, iv238–iv255. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.-S.; Li, J.-Q.; Zheng, Y.; Guo, R.-P.; Liang, H.-H.; Zhang, Y.-Q.; Lin, X.-J.; Lau, W.Y. A prospective randomized trial comparing percutaneous local ablative therapy and partial hepatectomy for small hepatocellular carcinoma. Ann. Surg. 2006, 243, 321–328. [Google Scholar] [CrossRef] [PubMed]
- N’Kontchou, G.; Mahamoudi, A.; Aout, M.; Ganne-Carrie, N.; Grando, V.; Coderc, E.; Vicaut, E.; Trinchet, J.C.; Sellier, N.; Beaugrand, M.; et al. Radiofrequency ablation of hepatocellular carcinoma: long-term results and prognostic factors in 235 Western patients with cirrhosis. Hepatology 2009, 50, 1475–1483. [Google Scholar] [CrossRef]
- Tateishi, R.; Shiina, S.; Teratani, T.; Obi, S.; Sato, S.; Koike, Y.; Fujishima, T.; Yoshida, H.; Kawabe, T.; Omata, M. Percutaneous radiofrequency ablation for hepatocellular carcinoma. An analysis of 1000 cases. Cancer 2005, 103, 1201–1209. [Google Scholar] [CrossRef] [PubMed]
- Waki, K.; Aikata, H.; Katamura, Y.; Kawaoka, T.; Takaki, S.; Hiramatsu, A.; Takahashi, S.; Toyota, N.; Ito, K.; Chayama, K. Percutaneous radiofrequency ablation as first-line treatment for small hepatocellular carcinoma: results and prognostic factors on long-term follow up. J. Gastroenterol. Hepatol. 2010, 25, 597–604. [Google Scholar] [CrossRef] [PubMed]
- Granata, V.; Petrillo, M.; Fusco, R.; Setola, S.V.; de Lutio di Castelguidone, E.; Catalano, O.; Piccirillo, M.; Albino, V.; Izzo, F.; Petrillo, A. Surveillance of HCC Patients after Liver RFA: Role of MRI with Hepatospecific Contrast versus Three-Phase CT Scan-Experience of High Volume Oncologic Institute. Gastroenterol. Res. Pract. 2013, 2013, 469097. [Google Scholar] [CrossRef]
- Doyle, A.; Gorgen, A.; Muaddi, H.; Aravinthan, A.D.; Issachar, A.; Mironov, O.; Zhang, W.; Kachura, J.; Beecroft, R.; Cleary, S.P.; et al. Outcomes of Radiofrequency Ablation as First-Line Therapy for Hepatocellular Carcinoma less than 3 cm in Potentially Transplantable Patients. J. Hepatol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Rossi, S.; Ravetta, V.; Rosa, L.; Ghittoni, G.; Viera, F.T.; Garbagnati, F.; Silini, E.M.; Dionigi, P.; Calliada, F.; Quaretti, P.; et al. Repeated radiofrequency ablation for management of patients with cirrhosis with small hepatocellular carcinomas: a long-term cohort study. Hepatology 2011, 53, 136–147. [Google Scholar] [CrossRef] [PubMed]
- Yokoyama, K.; Anan, A.; Iwata, K.; Nishizawa, S.; Morihara, D.; Ueda, S.; Sakurai, K.; Iwashita, H.; Hirano, G.; Sakamoto, M.; et al. Limitation of repeated radiofrequency ablation in hepatocellular carcinoma: proposal of a three (times) x 3 (years) index. J. Gastroenterol. Hepatol. 2012, 27, 1044–1050. [Google Scholar] [CrossRef] [PubMed]
- Wahl, D.R.; Stenmark, M.H.; Tao, Y.; Pollom, E.L.; Caoili, E.M.; Lawrence, T.S.; Schipper, M.J.; Feng, M.; et al. Outcomes after stereotactic body radiotherapy or radiofrequency ablation for hepatocellular carcinoma. J. Clin. Oncol. 2016, 34, 452–459. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.; Suresh, K.; Schipper, M.J.; Bazzi, L.; Ben-Josef, E.; Matuszak, M.M.; Parikh, N.D.; Welling, T.H.; Normolle, D.; Ten Haken, R.K.; et al. Individualized Adaptive Stereotactic Body Radiotherapy for Liver Tumors in Patients at High Risk for Liver Damage: A Phase 2 Clinical Trial. JAMA Oncol. 2018, 4, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Rajyaguru, D.J.; Borgert, A.J.; Smith, A.L.; Thomes, R.M.; Conway, P.D.; Halfdanarson, T.R.; Truty, M.J.; Kurup, A.N.; Go, R.S. Radiofrequency Ablation Versus Stereotactic Body Radiotherapy for Localized Hepatocellular Carcinoma in Nonsurgically Managed Patients: Analysis of the National Cancer Database. J. Clin. Oncol. 2018, 36, 600–608. [Google Scholar] [CrossRef] [PubMed]
- Parikh, N.D.; Marshall, V.D.; Green, M.; Lawrence, T.S.; Razumilava, N.; Owen, D.; Singal, A.G.; Feng, M.; et al. Effectiveness and cost of radiofrequency ablation and stereotactic body radiotherapy for treatment of early-stage hepatocellular carcinoma: An analysis of SEER-medicare. J. Med. Imaging Radiat. Oncol. 2018, 62, 673–681. [Google Scholar] [CrossRef] [PubMed]
- Pollom, E.L.; Lee, K.; Durkee, B.Y.; Grade, M.; Mokhtari, D.A.; Wahl, D.R.; Feng, M.; Kothary, N.; Koong, A.C.; Owens, D.K.; et al. Cost-effectiveness of Stereotactic Body Radiation Therapy versus Radiofrequency Ablation for Hepatocellular Carcinoma: A Markov Modeling Study. Radiology 2017, 283, 460–468. [Google Scholar] [CrossRef]
- Song, K.D.; Lim, H.K.; Rhim, H.; Lee, M.W.; Kim, Y.; Lee, W.J.; Paik, Y.H.; Gwak, G.-Y.; Man Kim, J.; Kwon, C.H.D.; et al. Repeated Hepatic Resection versus Radiofrequency Ablation for Recurrent Hepatocellular Carcinoma after Hepatic Resection: A Propensity Score Matching Study. Radiology 2015, 000, 1–10. [Google Scholar] [CrossRef]
- Sapisochin, G.; Barry, A.; Doherty, M.; Fischer, S.; Goldaracena, N.; Rosales, R.; Russo, M.; Beecroft, R.; Ghanekar, A.; Bhat, M.; et al. Stereotactic body radiotherapy vs. TACE or RFA as a bridge to transplant in patients with hepatocellular carcinoma. An intention-to-treat analysis. J. Hepatol. 2017, 67, 92–99. [Google Scholar] [CrossRef]
- Moore, A.; Cohen-Naftaly, M.; Tobar, A.; Kundel, Y.; Benjaminov, O.; Braun, M.; Issachar, A.; Mor, E.; Sarfaty, M.; Bragilovski, D.; et al. Stereotactic body radiation therapy (SBRT) for definitive treatment and as a bridge to liver transplantation in early stage inoperable Hepatocellular carcinoma. Radiat. Oncol. 2017, 12, 163. [Google Scholar] [CrossRef] [PubMed]
- Takeda, A.; Sanuki, N.; Eriguchi, T.; Kobayashi, T.; Iwabutchi, S.; Matsunaga, K.; Mizuno, T.; Yashiro, K.; Nisimura, S.; Kunieda, E. Stereotactic ablative body radiotherapy for previously untreated solitary hepatocellular carcinoma. J. Gastroenterol. Hepatol. 2014, 29, 372–379. [Google Scholar] [CrossRef] [PubMed]
- Seo, Y.-S.; Kim, M.-S.; Yoo, H.-J.; Jang, W.I.; Paik, E.K.; Han, C.J.; Lee, B.-H. Radiofrequency ablation versus stereotactic body radiotherapy for small hepatocellular carcinoma: a Markov model-based analysis. Cancer Med. 2016, 5, 3094–3101. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, H.; Ji, Y.; Cho, B.; Kim, S.S.; Jung, J.; Kwak, J.; Park, J.-H.; Lee, S.-W.; Kim, J.H.; et al. Evaluation of Hepatic Toxicity after Repeated Stereotactic Body Radiation Therapy for Recurrent Hepatocellular Carcinoma using Deformable Image Registration. Sci. Rep. 2018, 8, 16224. [Google Scholar] [CrossRef] [PubMed]
- Bujold, A.; Massey, C.A.; Kim, J.J.; Brierley, J.; Cho, C.; Wong, R.K.S.; Dinniwell, R.E.; Kassam, Z.; Ringash, J.; Cummings, B.; et al. Sequential Phase I and II Trials of Stereotactic Body Radiotherapy for Locally Advanced Hepatocellular Carcinoma. J. Clin. Oncol. 2013, 31, 1631–1639. [Google Scholar] [CrossRef] [PubMed]
- Livraghi, T.; Meloni, F.; Di Stasi, M.; Rolle, E.; Solbiati, L.; Tinelli, C.; Rossi, S. Sustained complete response and complications rates after radiofrequency ablation of very early hepatocellular carcinoma in cirrhosis: Is resection still the treatment of choice? Hepatology 2008, 47, 82–89. [Google Scholar] [CrossRef] [PubMed]
- Groeschl, R.T.; Pilgrim, C.H.C.; Hanna, E.M.; Simo, K.A.; Swan, R.Z.; Sindram, D.; Martinie, J.B.; Iannitti, D.A.; Bloomston, M.; Schmidt, C.; et al. Microwave ablation for hepatic malignancies: a multiinstitutional analysis. Ann. Surg. 2014, 259, 1195–1200. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Battiston, C.; Perrone, S.; Pulvirenti, A.; Regalia, E.; Romito, R.; Sarli, D.; Schiavo, M.; Garbagnati, F.; Marchiano, A.; et al. Radiofrequency ablation of small hepatocellular carcinoma in cirrhotic patients awaiting liver transplantation: a prospective study. Ann. Surg. 2004, 240, 900–909. [Google Scholar] [CrossRef]
- Chang, W.-T.; Kao, W.-Y.; Chau, G.-Y.; Su, C.-W.; Lei, H.-J.; Wu, J.-C.; Hsia, C.-Y.; Lui, W.-Y.; King, K.-L.; Lee, S.-D. Hepatic resection can provide long-term survival of patients with non-early-stage hepatocellular carcinoma: extending the indication for resection? Surgery 2012, 152, 809–820. [Google Scholar] [CrossRef]
- Forner, A.; Llovet, J.M.; Bruix, J. Hepatocellular carcinoma. Lancet 2012, 379, 1245–1255. [Google Scholar] [CrossRef]
- KANG, J.; NIE, Q.; DU, R.; ZHANG, L.; ZHANG, J.; LI, Q.; LI, J.; QI, W. Stereotactic body radiotherapy combined with transarterial chemoembolization for hepatocellular carcinoma with portal vein tumor thrombosis. Mol. Clin. Oncol. 2014, 2, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Lencioni, R.; Llovet, J.M. Modified RECIST (mRECIST) Assessment for Hepatocellular Carcinoma. Semin. Liver Dis. 2010, 30, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.-W.; Zhang, Y.-J.; Chen, M.-S.; Xu, L.; Liang, H.-H.; Lin, X.-J.; Guo, R.-P.; Zhang, Y.-Q.; Lau, W.Y. Radiofrequency ablation with or without transcatheter arterial chemoembolization in the treatment of hepatocellular carcinoma: a prospective randomized trial. J. Clin. Oncol. 2013, 31, 426–432. [Google Scholar] [CrossRef] [PubMed]
- National Institute of Health Common Terminology Criteria for Adverse Events (CTCAE). Available online: https://ctep.cancer.gov/protocolDevelopment/electronic_applications/ctc.htm (accessed on 5 January 2018).
- Yanaga, K. Central bisectionectomy (bisegmentectomy) of the liver (with video). J. Hepatobiliary. Pancreat. Sci. 2012, 19, 44–47. [Google Scholar] [CrossRef] [PubMed]
- Ripatti, S.; Palmgren, J. Estimation of multivariate frailty models using penalized partial likelihood. Biometrics 2000, 56, 1016–1022. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Before PSM | After PSM | |||||
|---|---|---|---|---|---|---|---|
| RFA Group (n = 39) | SBRT Group (n = 33) | P Value | RFA Group (n = 23) | SBRT Group (n = 23) | P Value | ||
| Sex, M/F | 33/6 | 32/1 | 0.137 | 20/3 | 22/1 | 0.601 | |
| Age, years | 56.00 (49.00–64.50) | 60.00 (47.00–66.00) | 0.670 | 56.00 (48.00–65.50) | 59.00 (42.50–65.50) | 0.958 | |
| Cirrhosis, Y/N | 22/17 | 15/18 | 0.490 | 11/12 | 10/13 | 1.000 | |
| B virus hepatitis, Y/N | 33/6 | 25/8 | 0.517 | 21/2 | 19/4 | 0.662 | |
| Child-Pugh score, n | A5 | 37 | 27 | 0.059 | 22 | 18 | 0.189 |
| A6 | 1 | 6 | 1 | 5 | |||
| B7 | 1 | 0 | 0 | 0 | |||
| White blood cell, *109/L | 5.00 (4.25–6.23) | 5.19 (4.79–6.60) | 0.367 | 5.40 (4.70–6.60) | 5.19 (4.80–7.08) | 0.630 | |
| Platelet, *109/L | 107.00 (93.00–155.00) | 137.00 (113.00–192.00) | 0.038 | 153.00 (116.00–176.00) | 129.00 (100.00–188.00) | 0.957 | |
| Alanine aminotransferase, U/L | 33.40 (21.90–46.90) | 28.50 (22.70–38.60) | 0.239 | 33.40 (20.00–43.40) | 28.50 (23.00–39.70) | 0.377 | |
| Aspartate aminotransferase, U/L | 32.70 (27.60–42.10) | 28.40 (23.60–37.30) | 0.553 | 32.70 (24.40–35.40) | 28.40 (24.00–39.20) | 0.633 | |
| Alpha fetoprotein, ng/mL | 67.50 (5.34–982.00) | 185.00 (4.86–840.20) | 0.810 | 136.00 (10.00–1870.00) | 218.00 (5.02–840.00) | 0.878 | |
| Tumor Size, cm | 2.10 (1.70–3.55) | 4.10 (3.40–5.20) | <0.001 | 3.50 (2.35–4.00) | 3.70 (3.00–4.80) | 0.257 | |
| Location, peripheral/central | 16/23 | 11/22 | 0.669 | 2/21 | 9/14 | 1.000 | |
| HCC adjacent to main vessel, Y/N | 17/16 | 28/5 | 0.001 | 12/11 | 19/4 | 0.059 | |
| HCC abutting the capsule, Y/N | 18/21 | 8/25 | 0.092 | 11/12 | 7/16 | 0.365 | |
| Follow–up time, months | 35.30 (21.20–54.70) | 16.30 (6.27–29.10) | <0.001 | 33.50 (19.20–50.80) | 13.60 (4.13–29.10) | 0.002 | |
| Variable | RFA Group (n = 39) | SBRT Group (n = 33) | P Value | |
|---|---|---|---|---|
| Post-treatment hospitalization, days | 3.00 (2.50–4.50) | - | - | |
| Short-term treatment-related toxicities #, n | ||||
| Pain | 7 | 3 | 0.459 | |
| Fever | 9 | 4 | 0.370 | |
| Gastrointestinal disorders | 2 | 7 | 0.089 | |
| Hematological toxicity | 0 | 2 | 0.401 | |
| Liver toxicities | 0 | 2 | 0.401 | |
| Skin toxicities | 0 | 1 | 0.933 | |
| Response according to mRECIST *, n | 1.000 | |||
| Complete response | 38 | 33 | ||
| Incomplete response | 1 | 0 | ||
| Disease progression, n | 28 | 12 | 0.005 | |
| Local disease progression, n | 23 | 6 | 0.002 | |
| Variable | Progression-Free Survival | Overall Survival | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Patient Number | Observed | UVA | MVA | Patient Number | Observed | UVA | MVA | |||
| Age, years | ≥60 | 31 | 17 | 0.500 | - | 31 | 11 | 0.600 | - | |
| <60 | 41 | 22 | 41 | 13 | ||||||
| Gender | Male | 65 | 33 | 0.020 | 0.390 | 65 | 20 | 0.300 | - | |
| Female | 7 | 6 | 7 | 4 | ||||||
| Location | Peripheral | 27 | 14 | 0.500 | - | 27 | 6 | 0.030 | 0.039 | |
| Central | 45 | 25 | 45 | 18 | ||||||
| Tumor size | >3 cm | 42 | 20 | 0.800 | - | 42 | 13 | 0.400 | - | |
| ≤3 cm | 30 | 19 | 30 | 11 | ||||||
| B virus hepatitis | Y | 58 | 33 | 0.400 | - | 58 | 19 | 0.900 | - | |
| N | 14 | 6 | 14 | 5 | ||||||
| HCC adjacent to or invading main vessel | Y | 45 | 22 | 0.700 | - | 45 | 11 | 0.200 | - | |
| N | 27 | 17 | 27 | 13 | ||||||
| HCC abutting the capsule | Y | 26 | 15 | 1.000 | - | 26 | 11 | 0.200 | - | |
| N | 46 | 24 | 46 | 13 | ||||||
| White blood cell, *10e9/L | ≥9.5 | 2 | 2 | 0.700 | - | 2 | 1 | 0.600 | - | |
| <9.5 | 70 | 37 | 70 | 23 | ||||||
| Platelet, *10e9/L | ≥100 | 51 | 23 | 0.050 | 0.555 | 51 | 19 | 0.700 | - | |
| <100 | 21 | 16 | 21 | 5 | ||||||
| Hemoglobin, g/L | ≥130 | 52 | 52 | 0.040 | 0.290 | 52 | 15 | 0.200 | - | |
| <130 | 20 | 20 | 20 | 9 | ||||||
| Alanine aminotransferase, U/L | ≥40 | 22 | 15 | 0.300 | - | 22 | 8 | 0.700 | - | |
| <40 | 50 | 24 | 50 | 16 | ||||||
| Aspartate aminotransferase, U/L | ≥45 | 13 | 7 | 0.800 | - | 13 | 6 | 0.600 | - | |
| <45 | 59 | 32 | 59 | 18 | ||||||
| Albumin, g/L | ≥35 | 68 | 36 | 0.200 | - | 68 | 23 | 0.800 | - | |
| <35 | 4 | 3 | 4 | 1 | ||||||
| Total bilirubin, umol/dL | >34.2 | 4 | 3 | 0.300 | - | 4 | 2 | 0.200 | - | |
| ≤34.2 | 68 | 36 | 68 | 22 | ||||||
| Alpha fetoprotein, ng/L | ≥200 | 31 | 18 | 0.400 | - | 31 | 9 | 0.900 | - | |
| <200 | 41 | 21 | 41 | 15 | ||||||
| Treatment allocation | RFA | 39 | 27 | 0.040 | 0.133 | 39 | 18 | 0.700 | 0.464 | |
| SBRT | 33 | 12 | 33 | 6 | ||||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pan, Y.-X.; Xi, M.; Fu, Y.-Z.; Hu, D.-D.; Wang, J.-C.; Liu, S.-L.; Chen, J.-B.; Xu, L.; Zhou, Z.-G.; Liu, M.-Z.; et al. Stereotactic Body Radiotherapy as a Salvage Therapy after Incomplete Radiofrequency Ablation for Hepatocellular Carcinoma: A Retrospective Propensity Score Matching Study. Cancers 2019, 11, 1116. https://doi.org/10.3390/cancers11081116
Pan Y-X, Xi M, Fu Y-Z, Hu D-D, Wang J-C, Liu S-L, Chen J-B, Xu L, Zhou Z-G, Liu M-Z, et al. Stereotactic Body Radiotherapy as a Salvage Therapy after Incomplete Radiofrequency Ablation for Hepatocellular Carcinoma: A Retrospective Propensity Score Matching Study. Cancers. 2019; 11(8):1116. https://doi.org/10.3390/cancers11081116
Chicago/Turabian StylePan, Yang-Xun, Mian Xi, Yi-Zhen Fu, Dan-Dan Hu, Jun-Cheng Wang, Shi-Liang Liu, Jin-Bin Chen, Li Xu, Zhong-Guo Zhou, Meng-Zhong Liu, and et al. 2019. "Stereotactic Body Radiotherapy as a Salvage Therapy after Incomplete Radiofrequency Ablation for Hepatocellular Carcinoma: A Retrospective Propensity Score Matching Study" Cancers 11, no. 8: 1116. https://doi.org/10.3390/cancers11081116
APA StylePan, Y.-X., Xi, M., Fu, Y.-Z., Hu, D.-D., Wang, J.-C., Liu, S.-L., Chen, J.-B., Xu, L., Zhou, Z.-G., Liu, M.-Z., Chen, M.-S., Zhao, L., & Zhang, Y.-J. (2019). Stereotactic Body Radiotherapy as a Salvage Therapy after Incomplete Radiofrequency Ablation for Hepatocellular Carcinoma: A Retrospective Propensity Score Matching Study. Cancers, 11(8), 1116. https://doi.org/10.3390/cancers11081116