Extent of Resection, MGMT Promoter Methylation Status and Tumor Location Independently Predict Progression-Free Survival in Adult Sporadic Pilocytic Astrocytoma

 ,
,
Abstract
1. Introduction
2. Results
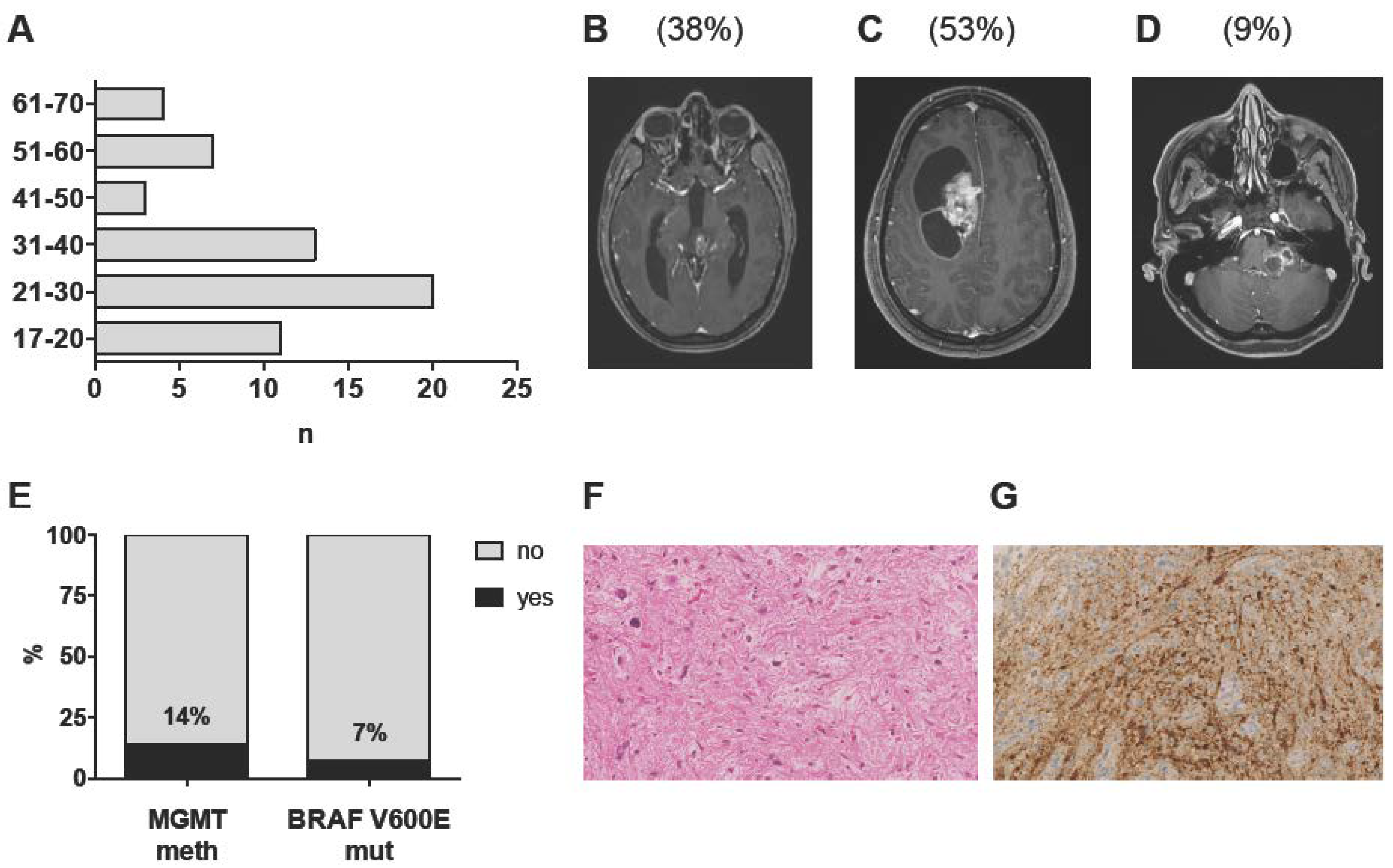
2.1. Patient Characteristics and Imaging Features
2.2. Histopathological and Molecular Analysis
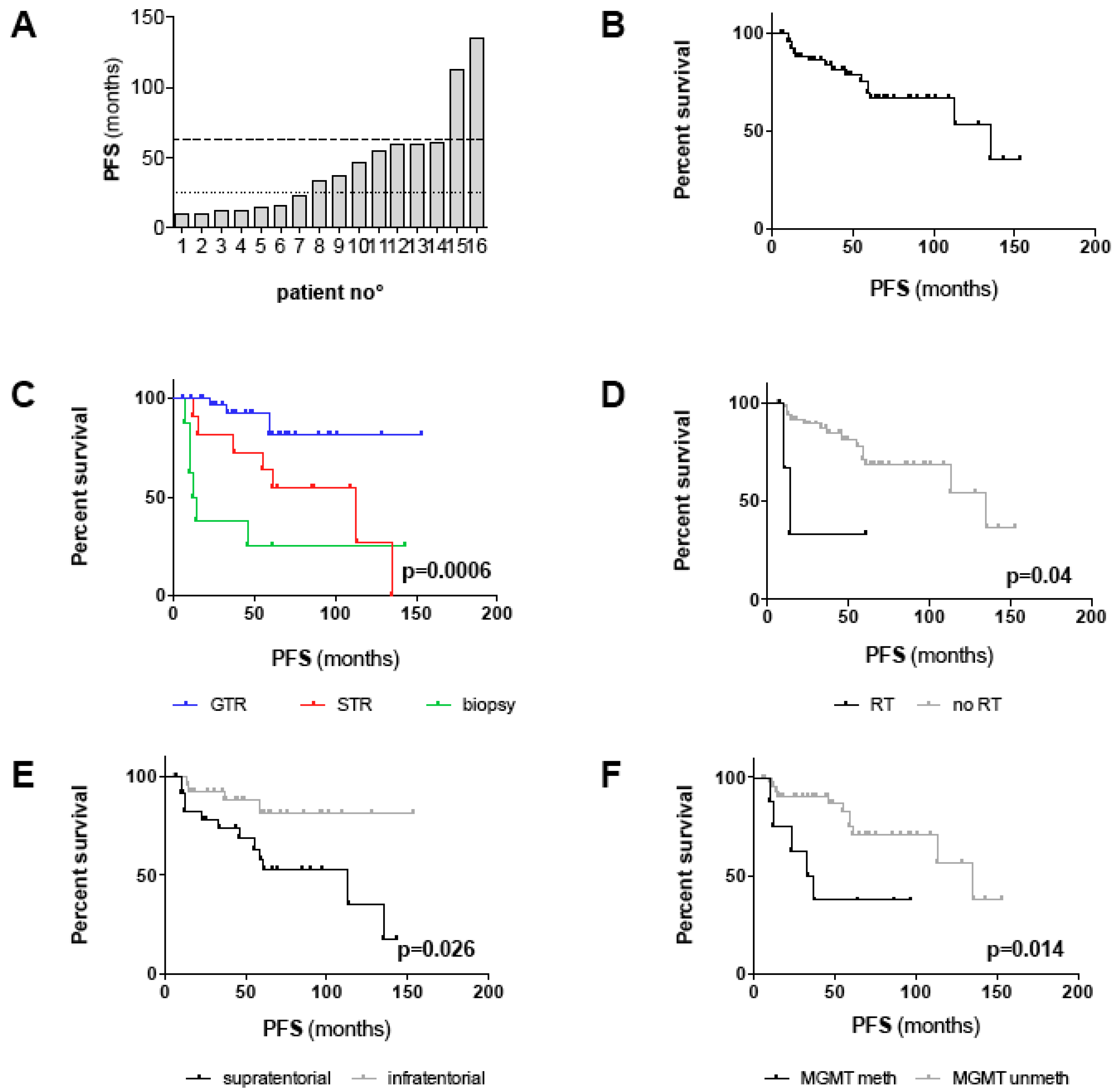
2.3. Clinical Outcome
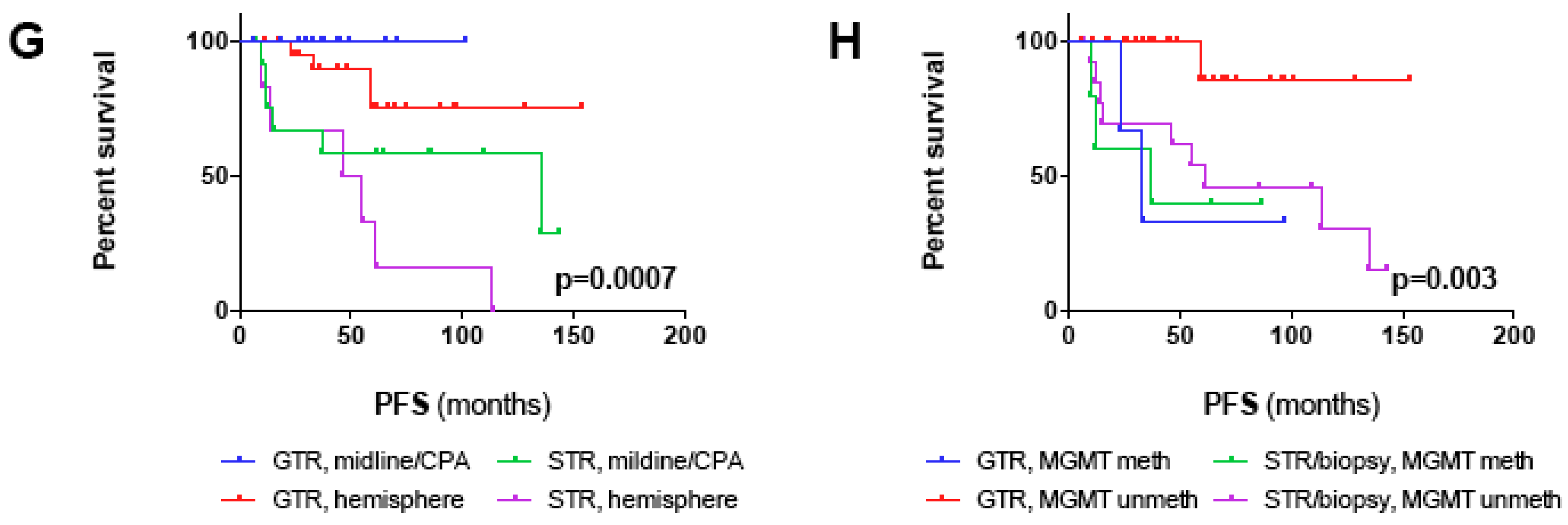
2.4. Prognostic Factors of Progression-free Survival
3. Discussion
4. Materials and Methods
4.1. Clinical Data
4.2. Histopathological and Molecular Analysis
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Ostrom, Q.T.; Gittleman, H.; Truitt, G.; Boscia, A.; Kruchko, C.; Barnholtz-Sloan, J.S. CBTRUS Statistical Report: Primary Brain and Other Central Nervous System Tumors Diagnosed in the United States in 2011–2015. Neuro Oncol. 2018, 20, iv1–iv86. [Google Scholar] [CrossRef] [PubMed]
- Burkhard, C.; Di Patre, P.-L.; Schüler, D.; Schüler, G.; Yaşargil, M.G.; Yonekawa, Y.; Lütolf, U.M.; Kleihues, P.; Ohgaki, H. A population-based study of the incidence and survival rates in patients with pilocytic astrocytoma. J. Neurosurg. 2003, 98, 1170–1174. [Google Scholar] [CrossRef] [PubMed]
- Georgakis, M.K.; Karalexi, M.A.; Kalogirou, E.I.; Ryzhov, A.; Zborovskaya, A.; Dimitrova, N.; Eser, S.; Antunes, L.; Sekerija, M.; Zagar, T.; et al. Incidence, time trends and survival patterns of childhood pilocytic astrocytomas in Southern-Eastern Europe and SEER, US. J. Neurooncol. 2017, 131, 163–175. [Google Scholar] [CrossRef] [PubMed]
- Dodgshun, A.J.; Maixner, W.J.; Hansford, J.R.; Sullivan, M.J. Low rates of recurrence and slow progression of pediatric pilocytic astrocytoma after gross-total resection: justification for reducing surveillance imaging. J. Neurosurg. Pediatr. 2016, 17, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Bond, K.M.; Hughes, J.D.; Porter, A.L.; Orina, J.; Fang, S.; Parney, I.F. Adult Pilocytic Astrocytoma: An Institutional Series and Systematic Literature Review for Extent of Resection and Recurrence. World Neurosurg. 2018, 110, 276–283. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.; Chitnavis, B.P.; Al-Sarraj, S.; Connor, S.; Sharr, M.M.; Gullan, R.W. Pilocytic astrocytoma of the adult-clinical features, radiological features and management. Br. J. Neurosurg. 2004, 18, 613–616. [Google Scholar] [CrossRef] [PubMed]
- Brown, P.D.; Anderson, S.K.; Carrero, X.W.; O’Neill, B.P.; Giannini, C.; Galanis, E.; Shah, S.A.; Abrams, R.A.; Curran, W.J.; Buckner, J.C.; et al. Adult patients with supratentorial pilocytic astrocytoma: long-term follow-up of prospective multicenter clinical trial NCCTG-867251 (Alliance). Neuro Oncol. Pract. 2015, 2, 199–204. [Google Scholar] [CrossRef] [PubMed]
- Stüer, C.; Vilz, B.; Majores, M.; Becker, A.; Schramm, J.; Simon, M. Frequent recurrence and progression in pilocytic astrocytoma in adults. Cancer 2007, 110, 2799–2808. [Google Scholar] [CrossRef]
- Johnson, D.R.; Brown, P.D.; Galanis, E.; Hammack, J.E. Pilocytic astrocytoma survival in adults: analysis of the Surveillance, Epidemiology, and End Results Program of the National Cancer Institute. J. Neurooncol. 2012, 108, 187–193. [Google Scholar] [CrossRef]
- Lee, K.J.; Marchan, E.; Peterson, J.; Harrell, A.C.; Quinones-Hinojosa, A.; Brown, P.D.; Trifiletti, D.M. Management and Survival of Adult Patients with Pilocytic Astrocytoma in the National Cancer Database. World Neurosurg. 2018, 112, e881–e887. [Google Scholar] [CrossRef]
- Sadighi, Z.; Slopis, J. Pilocytic astrocytoma: a disease with evolving molecular heterogeneity. J. Child Neurol. 2013, 28, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Theeler, B.J.; Ellezam, B.; Sadighi, Z.S.; Mehta, V.; Tran, M.D.; Adesina, A.M.; Bruner, J.M.; Puduvalli, V.K. Adult pilocytic astrocytomas: clinical features and molecular analysis. Neuro Oncol. 2014, 16, 841–847. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.T.W.; Gronych, J.; Lichter, P.; Witt, O.; Pfister, S.M. MAPK pathway activation in pilocytic astrocytoma. Cell. Mol. Life Sci. 2012, 69, 1799–1811. [Google Scholar] [CrossRef] [PubMed]
- Horbinski, C.; Hamilton, R.L.; Nikiforov, Y.; Pollack, I.F. Association of molecular alterations, including BRAF, with biology and outcome in pilocytic astrocytomas. Acta Neuropathol. (Berl.) 2010, 119, 641–649. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.; Rodriguez, F.J.; Karajannis, M.A.; Williams, S.C.; Legault, G.; Zagzag, D.; Burger, P.C.; Allen, J.C.; Eberhart, C.G.; Bar, E.E. BRAF alterations in primary glial and glioneuronal neoplasms of the central nervous system with identification of 2 novel KIAA1549:BRAF fusion variants. J. Neuropathol. Exp. Neurol. 2012, 71, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Schindler, G.; Capper, D.; Meyer, J.; Janzarik, W.; Omran, H.; Herold-Mende, C.; Schmieder, K.; Wesseling, P.; Mawrin, C.; Hasselblatt, M.; et al. Analysis of BRAF V600E mutation in 1,320 nervous system tumors reveals high mutation frequencies in pleomorphic xanthoastrocytoma, ganglioglioma and extra-cerebellar pilocytic astrocytoma. Acta Neuropathol. (Berl.) 2011, 121, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Sippl, C.; Urbschat, S.; Kim, Y.J.; Senger, S.; Oertel, J.; Ketter, R. Promoter methylation of RB1, P15, P16, and MGMT and their impact on the clinical course of pilocytic astrocytomas. Oncol. Lett. 2018, 15, 1600–1606. [Google Scholar] [CrossRef] [PubMed]
- McAuley, E.; Brophy, H.; Hayden, J.; Pettorini, B.; Parks, C.; Avula, S.; Mallucci, C.; Pizer, B. The benefit of surveillance imaging for paediatric cerebellar pilocytic astrocytoma. Childs Nerv. Syst. ChNS Off. J. Int. Soc. Pediatr. Neurosurg. 2019, 35, 801–805. [Google Scholar] [CrossRef] [PubMed]
- Nelson, A.J.; Zakaria, R.; Jenkinson, M.D.; Brodbelt, A.R. Extent of resection predicts risk of progression in adult pilocytic astrocytoma. Br. J. Neurosurg. 2019, 33, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Korshunov, A.; Meyer, J.; Capper, D.; Christians, A.; Remke, M.; Witt, H.; Pfister, S.; von Deimling, A.; Hartmann, C. Combined molecular analysis of BRAF and IDH1 distinguishes pilocytic astrocytoma from diffuse astrocytoma. Acta Neuropathol. (Berl.) 2009, 118, 401–405. [Google Scholar] [CrossRef]
- Capper, D.; Preusser, M.; Habel, A.; Sahm, F.; Ackermann, U.; Schindler, G.; Pusch, S.; Mechtersheimer, G.; Zentgraf, H.; von Deimling, A. Assessment of BRAF V600E mutation status by immunohistochemistry with a mutation-specific monoclonal antibody. Acta Neuropathol. (Berl.) 2011, 122, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, C.; Walker, E.; Mohamed, N.; Zhang, C.; Jacob, K.; Shirinian, M.; Alon, N.; Kahn, D.; Fried, I.; Scheinemann, K.; et al. BRAF-KIAA1549 fusion predicts better clinical outcome in pediatric low-grade astrocytoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2011, 17, 4790–4798. [Google Scholar] [CrossRef] [PubMed]
- Esteller, M.; Herman, J.G. Generating mutations but providing chemosensitivity: the role of O6-methylguanine DNA methyltransferase in human cancer. Oncogene 2004, 23, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Esteller, M.; Hamilton, S.R.; Burger, P.C.; Baylin, S.B.; Herman, J.G. Inactivation of the DNA repair gene O6-methylguanine-DNA methyltransferase by promoter hypermethylation is a common event in primary human neoplasia. Cancer Res. 1999, 59, 793–797. [Google Scholar] [PubMed]
- Reinhardt, A.; Stichel, D.; Schrimpf, D.; Sahm, F.; Korshunov, A.; Reuss, D.E.; Koelsche, C.; Huang, K.; Wefers, A.K.; Hovestadt, V.; et al. Anaplastic astrocytoma with piloid features, a novel molecular class of IDH wildtype glioma with recurrent MAPK pathway, CDKN2A/B and ATRX alterations. Acta Neuropathol. (Berl.) 2018, 136, 273–291. [Google Scholar] [CrossRef] [PubMed]
- Esteller, M.; Garcia-Foncillas, J.; Andion, E.; Goodman, S.N.; Hidalgo, O.F.; Vanaclocha, V.; Baylin, S.B.; Herman, J.G. Inactivation of the DNA-repair gene MGMT and the clinical response of gliomas to alkylating agents. N. Engl. J. Med. 2000, 343, 1350–1354. [Google Scholar] [CrossRef] [PubMed]
- Hegi, M.E.; Diserens, A.-C.; Gorlia, T.; Hamou, M.-F.; de Tribolet, N.; Weller, M.; Kros, J.M.; Hainfellner, J.A.; Mason, W.; Mariani, L.; et al. MGMT gene silencing and benefit from temozolomide in glioblastoma. N. Engl. J. Med. 2005, 352, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Wick, W.; Weller, M.; van den Bent, M.; Sanson, M.; Weiler, M.; von Deimling, A.; Plass, C.; Hegi, M.; Platten, M.; Reifenberger, G. MGMT testing--the challenges for biomarker-based glioma treatment. Nat. Rev. Neurol. 2014, 10, 372–385. [Google Scholar] [CrossRef]
- Ishkanian, A.; Laperriere, N.J.; Xu, W.; Millar, B.-A.; Payne, D.; Mason, W.; Sahgal, A. Upfront observation versus radiation for adult pilocytic astrocytoma. Cancer 2011, 117, 4070–4079. [Google Scholar] [CrossRef]
- Capper, D.; Jones, D.T.W.; Sill, M.; Hovestadt, V.; Schrimpf, D.; Sturm, D.; Koelsche, C.; Sahm, F.; Chavez, L.; Reuss, D.E.; et al. DNA methylation-based classification of central nervous system tumours. Nature 2018, 555, 469–474. [Google Scholar] [CrossRef]
- Karayan-Tapon, L.; Quillien, V.; Guilhot, J.; Wager, M.; Fromont, G.; Saikali, S.; Etcheverry, A.; Hamlat, A.; Loussouarn, D.; Campion, L.; et al. Prognostic value of O6-methylguanine-DNA methyltransferase status in glioblastoma patients, assessed by five different methods. J. Neurooncol. 2010, 97, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Quillien, V.; Lavenu, A.; Karayan-Tapon, L.; Carpentier, C.; Labussière, M.; Lesimple, T.; Chinot, O.; Wager, M.; Honnorat, J.; Saikali, S.; et al. Comparative assessment of 5 methods (methylation-specific polymerase chain reaction, MethyLight, pyrosequencing, methylation-sensitive high-resolution melting, and immunohistochemistry) to analyze O6-methylguanine-DNA-methyltranferase in a series of 100 glioblastoma patients. Cancer 2012, 118, 4201–4211. [Google Scholar] [PubMed]
- Bady, P.; Delorenzi, M.; Hegi, M.E. Sensitivity Analysis of the MGMT-STP27 Model and Impact of Genetic and Epigenetic Context to Predict the MGMT Methylation Status in Gliomas and Other Tumors. J. Mol. Diagn. JMD 2016, 18, 350–361. [Google Scholar] [CrossRef] [PubMed]
- Capper, D.; Weissert, S.; Balss, J.; Habel, A.; Meyer, J.; Jäger, D.; Ackermann, U.; Tessmer, C.; Korshunov, A.; Zentgraf, H.; et al. Characterization of R132H mutation-specific IDH1 antibody binding in brain tumors. Brain Pathol. Zurich Switz. 2010, 20, 245–254. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All Patients | MGMT Meth | MGMT Unmeth | p-Value | |
|---|---|---|---|---|
| No. of Patients | 58 | 8 | 49 | |
| Demographic Data | ||||
| Age (years); median (range) | 30 (17–66) | 41 (20–66) | 30 (17–65) | 0.23 * |
| Sex (male:female) | 28:30 | 4:4 | 23:26 | 1.0° |
| Tumor Characteristics | ||||
| Supratentorial/Infratentorial | 27/31 | 5:3 | 21:28 | 0.45° |
| Midline/Hemisphere/CPA | 22/31/5 | 2:4:2 | 20:26:3 | 1.0° |
| Contrast Enhancement | 42 | 5 | 36 | 1.0° |
| Tumor Cysts | 35 | 5 | 29 | 1.0° |
| Molecular Data (available in n patients) | ||||
| MGMT Promoter Methylation | 8 (57) | 8 | 0 | |
| IDH1 Mutation | 0 (40) | 0 (6) | 0 (33) | |
| BRAF V600E Mutation | 2 (30) | 0 (4) | 2 (25) | |
| Secondary anaplastic | 1 (58) | 1 (8) | 0 (0) | |
| Treatment at 1st Diagnosis | ||||
| Surgery | 58 | 8 | 49 | |
| EOR: GTR/STR/Biopsy | 39/11/8 | 3/3/2 | 35/8/6 | 0.17 & |
| Adjuvant Radiotherapy | 4 | 1 | 3 | 0.46° |
| Adjuvant Chemotherapy (TMZ) | 1 | 0 | 1 | 1.0° |
| Others (Hyperthermia) | 1 | 0 | 1 | 1.0° |
| Treatment at 1st Recurrence | ||||
| Surgery | 9 | 3 | 6 | |
| EOR: GTR/STR/Biopsy/ND | 6/2/0/1 | 2/0/0/1 | 4/2/0/0 | |
| Adjuvant Radiotherapy | 2 | 1 | 1 | |
| Adjuvant Chemotherapy (TMZ) | 2 | 1 | 1 | |
| Outcome Data | ||||
| Progression/Recurrence | 16 | 5 | 11 | 0.03° |
| 2nd Progression/Recurrence | 6 | 2 | 4 | 1.0° |
| Death | 1 | 1 | 0 | 0.14° |
| PFS (months); median (range) | 135 (2–153) | 35 (10–97) | 135 (2–153) | 0.012 § |
| Follow-up (months); median (range) | 72 (3–259) | 72 (38–109) | 74 (3–259) | 0.27 § |
| Age | Sex | supra/infra | ML/Hem/CPA | CE | MGMT meth | EOR | RT | CHT | Recurrence | |
|---|---|---|---|---|---|---|---|---|---|---|
| Age | - | |||||||||
| Sex | 0.62 * | - | ||||||||
| supra/infra | 0.83 * | 0.43° | - | |||||||
| ML/Hem/CPA | 0.84 & | 0.60 $ | 0.043$ | - | ||||||
| CE | 0.93 * | 1.0° | 0.31° | 0.17°,a | - | |||||
| MGMT meth | 0.23 * | 1.0° | 0.45° | 1.0°,a | 1.0° | - | ||||
| EOR | 0.99 & | 0.007§ | 0.037§ | 0.06 §,a | 0.18 § | 0.17 § | - | |||
| RT | 0.79 * | 1.0° | 0.33° | 1.0°,a | 1.0° | 0.46° | <0.0001 § | - | ||
| CHT | NC | 1.0° | 0.47° | 1.0°,a | 1.0° | 1.0° | 0.042§ | 1.0° | - | |
| Recurrence | 0.4 * | 0.24° | 0.019° | 0.56°,a | 0.67° | 0.032° | 0.0001§ | 0.3° | 0.28° | - |
| All Patients | MGMT Meth | MGMT Unmeth | p-Value | |
|---|---|---|---|---|
| Noumber of Patients | 54 | 8 | 45 | |
| Demographic Data | ||||
| Age (years); median (range) | 28.5 (17–66) | 41 (20–66) | 30 (17–65) | 0.21 * |
| Sex (male:female) | 27:27 | 4:4 | 22:23 | 1.0° |
| Tumor Characteristics | ||||
| Supratentorial/Infratentorial | 25/29 | 5:3 | 19:26 | 0.44° |
| Midline/Hemisphere/CPA | 22/28/4 | 2:4:2 | 20:23:2 | 1.0° |
| Contrast Enhancement | 38 | 5 | 32 | 1.0° |
| Tumor Cysts | 32 | 5 | 26 | 1.0° |
| Molecular Data (available in n patients) | ||||
| MGMT Promoter Methylation | 8 (53) | 8 | 0 | |
| IDH1 Mutation | 0 (36) | 0 (6) | 0 (29) | |
| BRAF V600E Mutation | 1 (26) | 0 (4) | 1 (21) | |
| Secondary anaplastic | 1 (54) | 1 (8) | 0 (0) | |
| Treatment at 1st Diagnosis | ||||
| Surgery | 54 | 8 | 45 | |
| EOR: GTR/STR/Biopsy | 35/11/8 | 3/3/2 | 31/8/6 | 0.23° |
| Adjuvant Radiotherapy | 3 | 1 | 3 | 0.49° |
| Adjuvant Chemotherapy (TMZ) | 1 | 0 | 1 | 1.0° |
| Others (Hyperthermia) | 1 | 0 | 1 | 1.0° |
| Treatment at 1st Recurrence | ||||
| Surgery | 9 | 3 | 6 | |
| EOR: GTR/STR/Biopsy/ND | 6/2/0/1 | 2/0/0/1 | 4/2/0/0 | |
| Adjuvant Radiotherapy | 2 | 1 | 1 | |
| Adjuvant Chemotherapy (TMZ) | 2 | 1 | 1 | |
| Outcome Data | ||||
| Progression/Recurrence | 16 | 5 | 11 | 0.045° |
| 2nd Progression/Recurrence | 6 | 2 | 4 | 1.0° |
| Death | 1 | 1 | 0 | 0.15° |
| PFS (months); median (range) | 135 (6–153) | 35 (10–97) | 135 (6–153) | 0.014§ |
| Follow-up (months); median (range) | 76.5 (12–259) | 72 (38–109) | 83 (12–259) | 0.16 § |
| Covariates of Progression-free Survival | Univariate | Multivariate | |
|---|---|---|---|
| p-Value | p-Value | HR (95% CI) | |
| Age; median (high vs. low) | 0.41 | n.s. | |
| Sex (male vs. female) | 0.39 | n.s. | |
| Supratentorial vs. Infratentorial | 0.026 | n.s. | |
| Midline vs. Hemisphere vs. CPA | 0.85 | ||
| - Midline (Ref.) vs. Hemisphere | 0.02 | 0.21 (0.06–0.78) | |
| - CPA (Ref.) vs. Hemisphere | 0.038 | 0.08 (0.01–0.87) | |
| Contrast-Enhancement | 0.3 | n.s. | |
| MGMT Promoter unmethylated | 0.014 | 0.009 | 0.18 (0.05–0.64) |
| GTR vs. STR vs. biopsy | 0.0006 | ||
| - GTR vs. STR | 0.02 | ||
| - GTR vs. biopsy | <0.0001 | ||
| - STR vs. biopsy | 0.25 | ||
| - GTR (Ref.) vs. STR/biopsy | <0.001 | 0.1 (0.03–0.37) | |
| Radiotherapy | 0.04 | n.s. | |
| Chemotherapy | 0.11 | n.s. | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jungk, C.; Reinhardt, A.; Warta, R.; Capper, D.; von Deimling, A.; Herold-Mende, C.; Unterberg, A. Extent of Resection, MGMT Promoter Methylation Status and Tumor Location Independently Predict Progression-Free Survival in Adult Sporadic Pilocytic Astrocytoma. Cancers 2019, 11, 1072. https://doi.org/10.3390/cancers11081072
Jungk C, Reinhardt A, Warta R, Capper D, von Deimling A, Herold-Mende C, Unterberg A. Extent of Resection, MGMT Promoter Methylation Status and Tumor Location Independently Predict Progression-Free Survival in Adult Sporadic Pilocytic Astrocytoma. Cancers. 2019; 11(8):1072. https://doi.org/10.3390/cancers11081072
Chicago/Turabian StyleJungk, Christine, Annekathrin Reinhardt, Rolf Warta, David Capper, Andreas von Deimling, Christel Herold-Mende, and Andreas Unterberg. 2019. "Extent of Resection, MGMT Promoter Methylation Status and Tumor Location Independently Predict Progression-Free Survival in Adult Sporadic Pilocytic Astrocytoma" Cancers 11, no. 8: 1072. https://doi.org/10.3390/cancers11081072
APA StyleJungk, C., Reinhardt, A., Warta, R., Capper, D., von Deimling, A., Herold-Mende, C., & Unterberg, A. (2019). Extent of Resection, MGMT Promoter Methylation Status and Tumor Location Independently Predict Progression-Free Survival in Adult Sporadic Pilocytic Astrocytoma. Cancers, 11(8), 1072. https://doi.org/10.3390/cancers11081072