Metastatic Uveal Melanoma: Treatment Strategies and Survival—Results from the Dutch Melanoma Treatment Registry

 ,
,  ,
, 
 add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Results
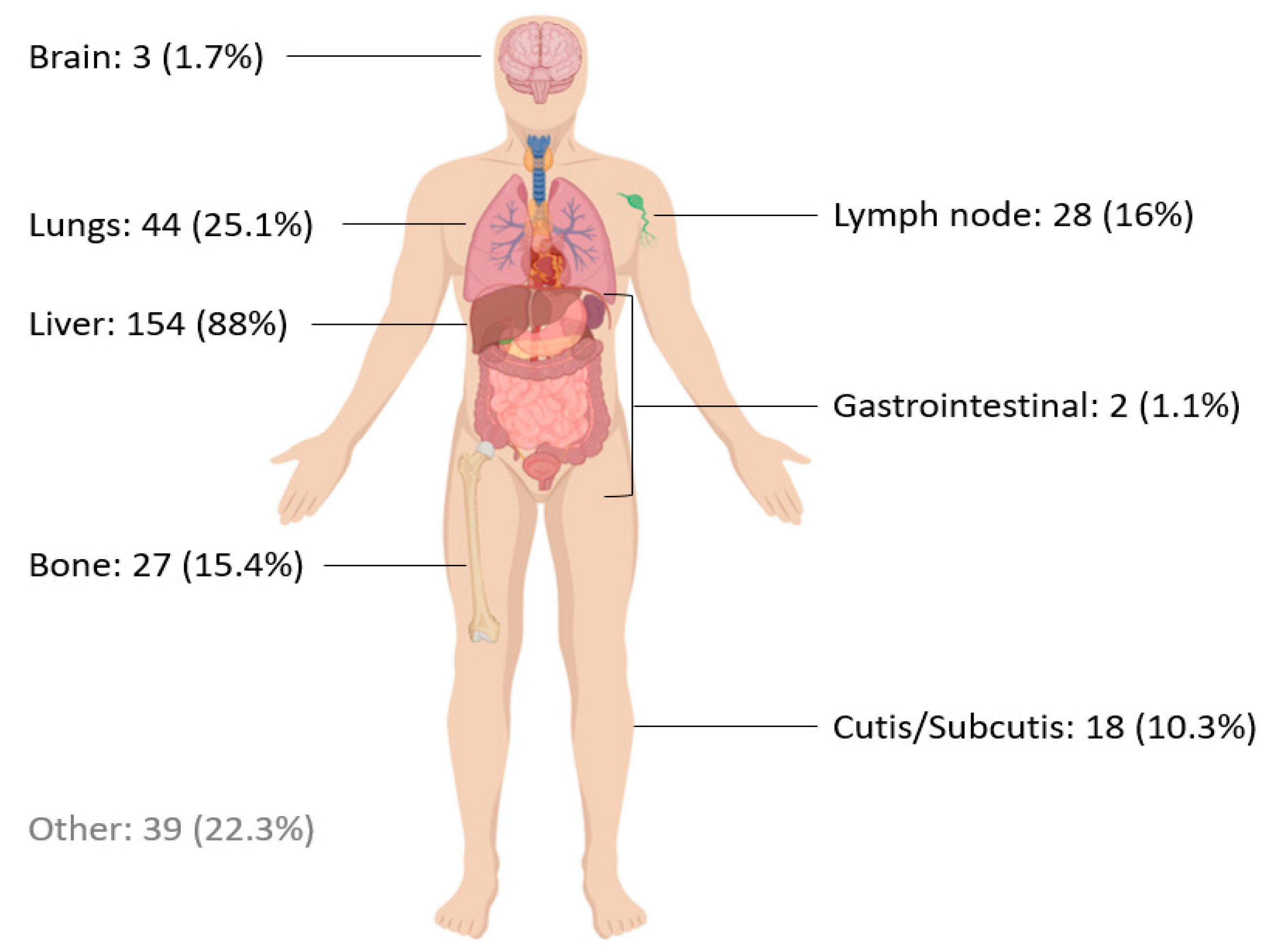
2.1. Patient Characteristics
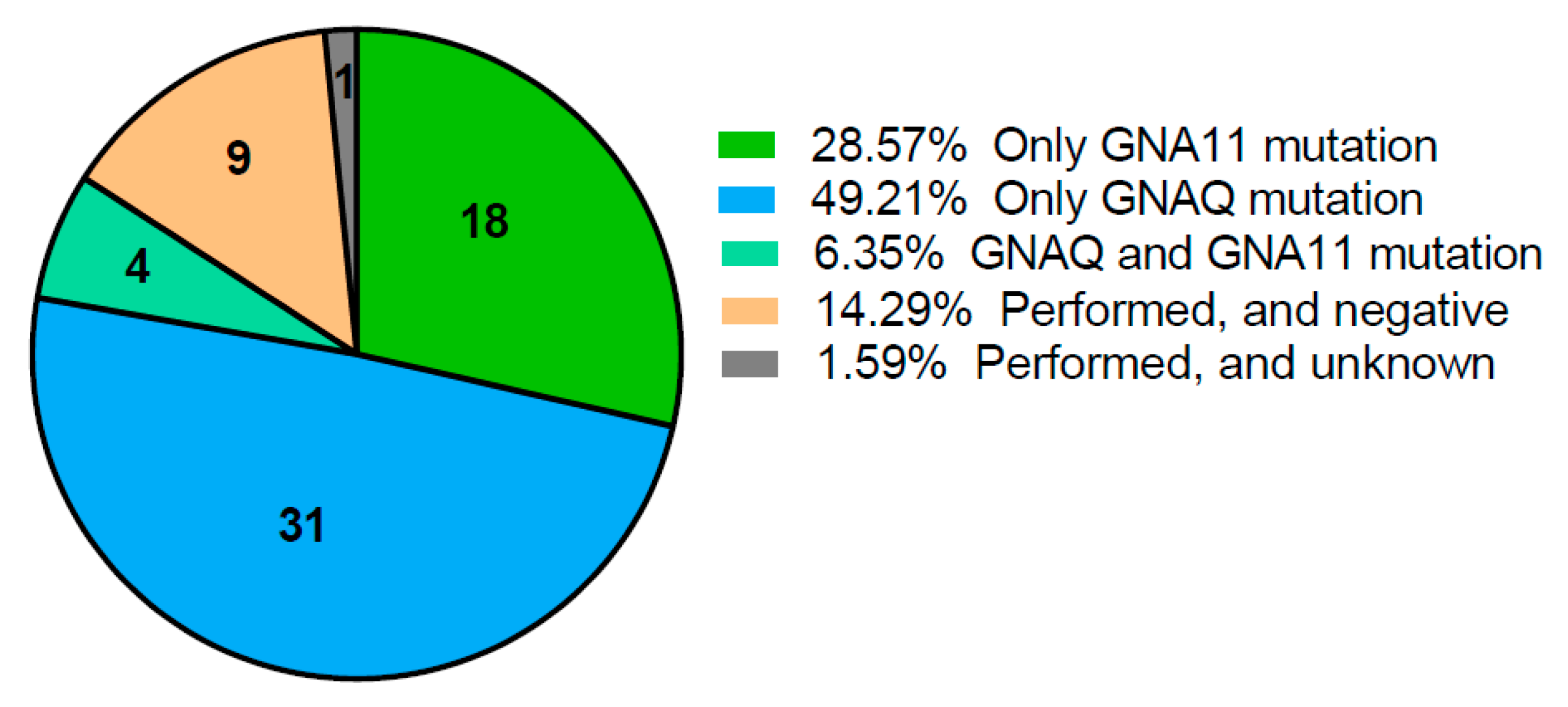
2.2. Mutation Analysis
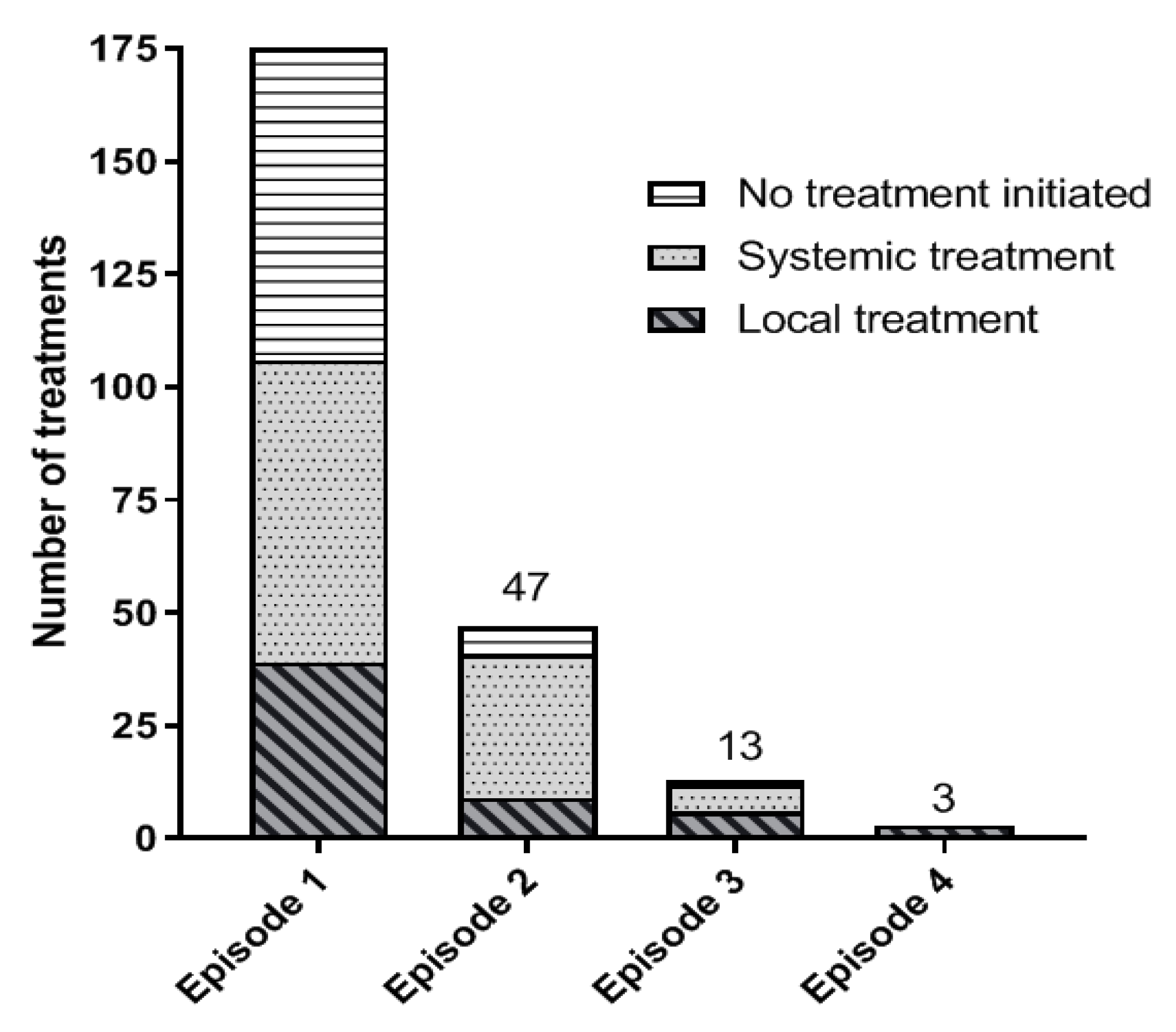
2.3. Treatment of Metastatic UM Patients
2.4. Survival
3. Discussion
4. Patients and Methods
4.1. Datasource
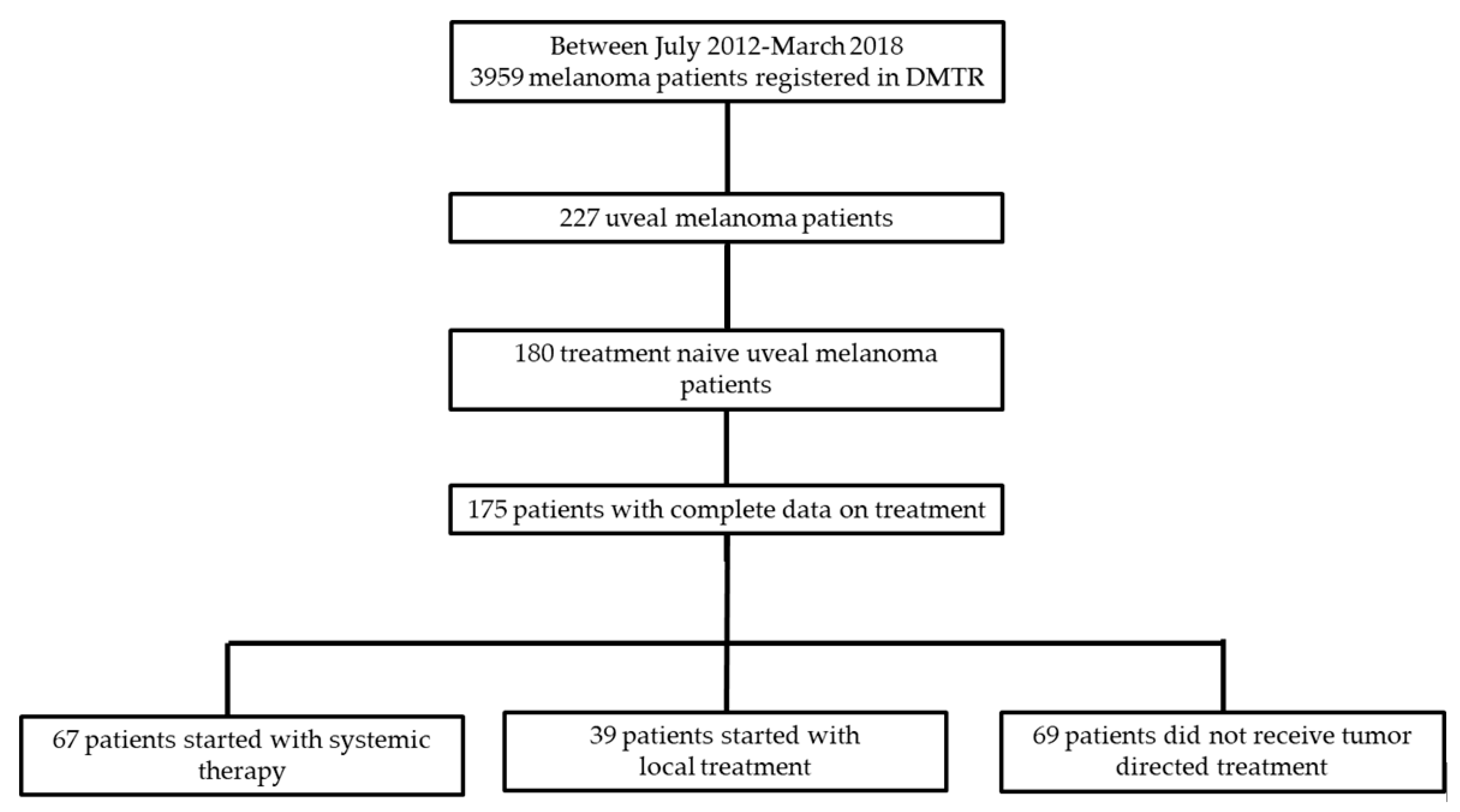
4.2. Patients
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bedikian, A.Y. Metastatic uveal melanoma therapy: Current options. Int. Ophthalmol. Clin. 2006, 46, 151–166. [Google Scholar] [CrossRef]
- Damato, B. Treatment of primary intraocular melanoma. Expert Rev. Anticancer Ther. 2006, 6, 493–506. [Google Scholar] [CrossRef]
- Dutch Cancer Registry. Available online: https://www.cijfersoverkanker.nl/ (accessed on 12 December 2018).
- Mallone, S.; De Vries, E.; Guzzo, M.; Midena, E.; Verne, J.; Coebergh, J.W.; Marcos-Gragera, R.; Ardanaz, E.; Martinez, R.; Chirlaque, M.D.; et al. Descriptive epidemiology of malignant mucosal and uveal melanomas and adnexal skin carcinomas in Europe. Eur. J. Cancer 2012, 48, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Spagnolo, F.; Caltabiano, G.; Queirolo, P. Uveal melanoma. Cancer Treat. Rev. 2012, 38, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Collaborative Ocular Melanoma Study Group. The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma: V. Twelve-year mortality rates and prognostic factors: COMS report No. 28. Arch. Ophthalmol. 2006, 124, 1684–1693. [Google Scholar] [CrossRef] [PubMed]
- Kujala, E.; Makitie, T.; Kivela, T. Very long-term prognosis of patients with malignant uveal melanoma. Investig. Ophthalmol. Vis. Sci. 2003, 44, 4651–4659. [Google Scholar] [CrossRef] [PubMed]
- Rietschel, P.; Panageas, K.S.; Hanlon, C.; Patel, A.; Abramson, D.H.; Chapman, P.B. Variates of survival in metastatic uveal melanoma. J. Clin. Oncol. 2005, 23, 8076–8080. [Google Scholar] [CrossRef]
- Augsburger, J.J.; Correa, Z.M.; Shaikh, A.H. Effectiveness of treatments for metastatic uveal melanoma. Am. J. Ophthalmol. 2009, 148, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Hughes, M.S.; Zager, J.; Faries, M.; Alexander, H.R.; Royal, R.E.; Wood, B.; Choi, J.; McCluskey, K.; Whitman, E.; Agarwala, S.; et al. Results of a Randomized Controlled Multicenter Phase III Trial of Percutaneous Hepatic Perfusion Compared with Best Available Care for Patients with Melanoma Liver Metastases. Ann. Surg. Oncol. 2016, 23, 1309–1319. [Google Scholar] [CrossRef]
- Stinauer, M.A.; Kavanagh, B.D.; Schefter, T.E.; Gonzalez, R.; Flaig, T.; Lewis, K.; Robinson, W.; Chidel, M.; Glode, M.; Raben, D. Stereotactic body radiation therapy for melanoma and renal cell carcinoma: Impact of single fraction equivalent dose on local control. Radiat. Oncol. 2011, 6, 34. [Google Scholar] [CrossRef]
- Shashank, A.; Shehata, M.; Morris, D.L.; Thompson, J.F. Radiofrequency ablation in metastatic melanoma. J. Surg. Oncol. 2014, 109, 366–369. [Google Scholar] [CrossRef]
- Huppert, P.E.; Fierlbeck, G.; Pereira, P.; Schanz, S.; Duda, S.H.; Wietholtz, H.; Rozeik, C.; Claussen, C.D. Transarterial chemoembolization of liver metastases in patients with uveal melanoma. Eur. J. Radiol. 2010, 74, e38–e44. [Google Scholar] [CrossRef]
- Pawlik, T.M.; Zorzi, D.; Abdalla, E.K.; Clary, B.M.; Gershenwald, J.E.; Ross, M.I.; Aloia, T.A.; Curley, S.A.; Camacho, L.H.; Capussotti, L.; et al. Hepatic resection for metastatic melanoma: Distinct patterns of recurrence and prognosis for ocular versus cutaneous disease. Ann. Surg. Oncol. 2006, 13, 712–720. [Google Scholar] [CrossRef]
- De Leede, E.M.; Burgmans, M.C.; Kapiteijn, E.; Luyten, G.P.; Jager, M.J.; Tijl, F.G.; Hartgrink, H.H.; Grunhagen, D.J.; Rothbarth, J.; van de Velde, C.J.; et al. Isolated (hypoxic) hepatic perfusion with high-dose chemotherapy in patients with unresectable liver metastases of uveal melanoma: Results from two experienced centres. Melanoma Res. 2016, 26, 588–594. [Google Scholar] [CrossRef]
- Nathan, P.; Cohen, V.; Coupland, S.; Curtis, K.; Damato, B.; Evans, J.; Fenwick, S.; Kirkpatrick, L.; Li, O.; Marshall, E.; et al. Uveal Melanoma UK National Guidelines. Eur. J. Cancer 2015, 51, 2404–2412. [Google Scholar] [CrossRef]
- Melanoom, T. Available online: www.oncoline.nl/uveamelanoom (accessed on 12 December 2018).
- Shoushtari, A.N.; Carvajal, R.D. GNAQ and GNA11 mutations in uveal melanoma. Melanoma Res. 2014, 24, 525–534. [Google Scholar] [CrossRef]
- Harbour, J.W.; Onken, M.D.; Roberson, E.D.; Duan, S.; Cao, L.; Worley, L.A.; Council, M.L.; Matatall, K.A.; Helms, C.; Bowcock, A.M. Frequent mutation of BAP1 in metastasizing uveal melanomas. Science 2010, 330, 1410–1413. [Google Scholar] [CrossRef]
- Martin, M.; Masshofer, L.; Temming, P.; Rahmann, S.; Metz, C.; Bornfeld, N.; van de Nes, J.; Klein-Hitpass, L.; Hinnebusch, A.G.; Horsthemke, B.; et al. Exome sequencing identifies recurrent somatic mutations in EIF1AX and SF3B1 in uveal melanoma with disomy 3. Nat. Genet. 2013, 45, 933–936. [Google Scholar] [CrossRef]
- Yavuzyigitoglu, S.; Koopmans, A.E.; Verdijk, R.M.; Vaarwater, J.; Eussen, B.; van Bodegom, A.; Paridaens, D.; Kilic, E.; de Klein, A.; Rotterdam Ocular Melanoma Study Group. Uveal Melanomas with SF3B1 Mutations: A Distinct Subclass Associated with Late-Onset Metastases. Ophthalmology 2016, 123, 1118–1128. [Google Scholar] [CrossRef]
- Flaherty, L.E.; Unger, J.M.; Liu, P.Y.; Mertens, W.C.; Sondak, V.K. Metastatic melanoma from intraocular primary tumors: The Southwest Oncology Group experience in phase II advanced melanoma clinical trials. Am. J. Clin. Oncol. 1998, 21, 568–572. [Google Scholar] [CrossRef]
- Nathan, F.E.; Berd, D.; Sato, T.; Shield, J.A.; Shields, C.L.; De Potter, P.; Mastrangelo, M.J. BOLD+ interferon in the treatment of metastatic uveal melanoma: First report of active systemic therapy. J. Exp. Clin. Cancer Res. CR 1997, 16, 201–208. [Google Scholar]
- Kivela, T.; Suciu, S.; Hansson, J.; Kruit, W.H.; Vuoristo, M.S.; Kloke, O.; Gore, M.; Hahka-Kemppinen, M.; Parvinen, L.M.; Kumpulainen, E.; et al. Bleomycin, vincristine, lomustine and dacarbazine (BOLD) in combination with recombinant interferon alpha-2b for metastatic uveal melanoma. Eur. J. Cancer 2003, 39, 1115–1120. [Google Scholar] [CrossRef]
- Kelderman, S.; van der Kooij, M.K.; van den Eertwegh, A.J.; Soetekouw, P.M.; Jansen, R.L.; van den Brom, R.R.; Hospers, G.A.; Haanen, J.B.; Kapiteijn, E.; Blank, C.U. Ipilimumab in pretreated metastastic uveal melanoma patients. Results of the Dutch Working group on Immunotherapy of Oncology (WIN-O). Acta Oncol. 2013, 52, 1786–1788. [Google Scholar] [CrossRef]
- Zimmer, L.; Vaubel, J.; Mohr, P.; Hauschild, A.; Utikal, J.; Simon, J.; Garbe, C.; Herbst, R.; Enk, A.; Kampgen, E.; et al. Phase II DeCOG-study of ipilimumab in pretreated and treatment-naive patients with metastatic uveal melanoma. PLoS ONE 2015, 10, e0118564. [Google Scholar] [CrossRef]
- Maio, M.; Danielli, R.; Chiarion-Sileni, V.; Pigozzo, J.; Parmiani, G.; Ridolfi, R.; De Rosa, F.; Del Vecchio, M.; Di Guardo, L.; Queirolo, P.; et al. Efficacy and safety of ipilimumab in patients with pre-treated, uveal melanoma. Ann. Oncol. 2013, 24, 2911–2915. [Google Scholar] [CrossRef]
- Kottschade, L.A.; McWilliams, R.R.; Markovic, S.N.; Block, M.S.; Villasboas Bisneto, J.; Pham, A.Q.; Esplin, B.L.; Dronca, R.S. The use of pembrolizumab for the treatment of metastatic uveal melanoma. Melanoma Res. 2016, 26, 300–303. [Google Scholar] [CrossRef]
- Bender, C.; Enk, A.; Gutzmer, R.; Hassel, J.C. Anti-PD-1 antibodies in metastatic uveal melanoma: A treatment option? Cancer Med. 2017, 6, 1581–1586. [Google Scholar] [CrossRef]
- Algazi, A.P.; Tsai, K.K.; Shoushtari, A.N.; Munhoz, R.R.; Eroglu, Z.; Piulats, J.M.; Ott, P.A.; Johnson, D.B.; Hwang, J.; Daud, A.I.; et al. Clinical outcomes in metastatic uveal melanoma treated with PD-1 and PD-L1 antibodies. Cancer 2016, 122, 3344–3353. [Google Scholar] [CrossRef]
- Heppt, M.V.; Heinzerling, L.; Kahler, K.C.; Forschner, A.; Kirchberger, M.C.; Loquai, C.; Meissner, M.; Meier, F.; Terheyden, P.; Schell, B.; et al. Prognostic factors and outcomes in metastatic uveal melanoma treated with programmed cell death-1 or combined PD-1/cytotoxic T-lymphocyte antigen-4 inhibition. Eur. J. Cancer 2017, 82, 56–65. [Google Scholar] [CrossRef]
- van der Kooij, M.K.; Joosse, A.; Speetjens, F.M.; Hospers, G.A.; Bisschop, C.; de Groot, J.W.; Koornstra, R.; Blank, C.U.; Kapiteijn, E. Anti-PD1 treatment in metastatic uveal melanoma in the Netherlands. Acta Oncol. 2017, 56, 101–103. [Google Scholar] [CrossRef]
- Carvajal, R.D.; Sosman, J.A.; Quevedo, J.F.; Milhem, M.M.; Joshua, A.M.; Kudchadkar, R.R.; Linette, G.P.; Gajewski, T.F.; Lutzky, J.; Lawson, D.H.; et al. Effect of selumetinib vs chemotherapy on progression-free survival in uveal melanoma: A randomized clinical trial. JAMA 2014, 311, 2397–2405. [Google Scholar] [CrossRef]
- Carvajal, R.D.; Piperno-Neumann, S.; Kapiteijn, E.; Chapman, P.B.; Frank, S.; Joshua, A.M.; Piulats, J.M.; Wolter, P.; Cocquyt, V.; Chmielowski, B.; et al. Selumetinib in Combination With Dacarbazine in Patients With Metastatic Uveal Melanoma: A Phase III, Multicenter, Randomized Trial (SUMIT). J. Clin. Oncol. 2018, 36, 1232–1239. [Google Scholar] [CrossRef]
- Van Raamsdonk, C.D.; Griewank, K.G.; Crosby, M.B.; Garrido, M.C.; Vemula, S.; Wiesner, T.; Obenauf, A.C.; Wackernagel, W.; Green, G.; Bouvier, N.; et al. Mutations in GNA11 in uveal melanoma. N. Engl. J. Med. 2010, 363, 2191–2199. [Google Scholar] [CrossRef]
- Jochems, A.; Schouwenburg, M.G.; Leeneman, B.; Franken, M.G.; van den Eertwegh, A.J.; Haanen, J.B.; Gelderblom, H.; Uyl-de Groot, C.A.; Aarts, M.J.; van den Berkmortel, F.W.; et al. Dutch Melanoma Treatment Registry: Quality assurance in the care of patients with metastatic melanoma in the Netherlands. Eur. J. Cancer 2017, 72, 156–165. [Google Scholar] [CrossRef]
- Pelster, M.; Gruschkus, S.K.; Basset, R.; Gombus, D.S.; Shephard, M.; Posada, L.; Glover, M.; Diab, A.; Hwu, P.; Patel, S.P. Phase II study of ipilimumab and nivolumab (ipi/nivo) in metastatic uveal melanoma (UM). J. Clin. Oncol. 2019, 37, 9522. [Google Scholar] [CrossRef]
- Diener-West, M.; Reynolds, S.M.; Agugliaro, D.J.; Caldwell, R.; Cumming, K.; Earle, J.D.; Hawkins, B.S.; Hayman, J.A.; Jaiyesimi, I.; Jampol, L.M.; et al. Development of metastatic disease after enrollment in the COMS trials for treatment of choroidal melanoma: Collaborative Ocular Melanoma Study Group Report No. 26. Arch. Ophthalmol. 2005, 123, 1639–1643. [Google Scholar] [CrossRef]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control. Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | All Patients (n = 175) | Systemic Therapy (n = 67) | Local Therapy (n = 39) | Best Supportive Care (n = 69) | p-Value |
|---|---|---|---|---|---|
| Age | 0.001 | ||||
| Median, years (range) | 65 (29–89) | 61 (29–80) | 61 (41–80) | 69 (45–89) | |
| <65 years (%) | 86 (49.1) | 39 (58.2) | 25 (64.1) | 22 (31.9) | |
| >65 years (%) | 89 (50.9) | 28 (41.8) | 14 (35.9) | 47 (68.1) | |
| Gender (%) | 0.98 | ||||
| Male | 88 (50.3) | 34 (50.7) | 20 (51.3) | 34 (49.3) | |
| Female | 87 (49.7) | 33 (49.3) | 19 (48.7) | 35 (50.7) | |
| WHO performance score (%) | 0.000 | ||||
| 0 | 106 (60.6) | 55 (82.1) | 21 (53.8) | 30 (60.6) | |
| 1 | 25 (14.3) | 7 (10.4) | 3 (7.7) | 15 (21.7) | |
| 2 | 11 (6.3) | 2 (3) | 1 (2.6) | 8 (11.6) | |
| 3 | 3 (1.7) | 0 | 0 | 3 (4.3) | |
| 4 | 1 (0.6) | 0 | 0 | 1 (1.4) | |
| Unknown | 29 (16.6) | 3 (4,5) | 14 (35,9) | 12 (17.4) | |
| Median time from diagnosis primary tumor to stage IV | 0.02 * | ||||
| months (range) | 38 (0–477) | 43 (0–296) | 29 (0–477) | 42 (0–361) | |
| Brain metastases (%) | 0.75 | ||||
| No | 169 (96.6) | 64 (95.5) | 39 (100) | 66 (95.7) | |
| Yes | 3 (1.7) | 2 (3) | 0 | 1 (1.4) | |
| Unknown | 3 (1.7) | 1 (1.5) | 0 | 2 (2.9) | |
| Liver metastases (%) | 0.10 | ||||
| No | 20 (11.4) | 11 (16.4) | 1 (2.6) | 8 (11.6) | |
| Yes | 154 (88) | 56 (83.6) | 38 (97.4) | 60 (87) | |
| Unknown | 1 (0.6) | 0 | 0 | 1 (1.4) | |
| Metastatic sites (%) | 0.002 | ||||
| <3 metastatic sites | 134 (76.6) | 44 (65.7) | 39 (100) | 52 (75.4) | |
| >3 metastatic sites | 31 (17.7) | 18 (26.9) | 0 | 13 (18.8) | |
| Unknown | 10 (5.7) | 5 (7.5) | 0 | 4 (5.8) | |
| LDH (%) | 0.000 | ||||
| Not elevated | 81 (46.3) | 37 (55.2) | 26 (66.7) | 18 (26.1) | |
| Elevated (250–500) | 34 (19.4) | 12 (17.9) | 9 (23.1) | 13 (18.8) | |
| Elevated (>500) | 51 (29.1) | 17 (25.4) | 1 (2.6) | 33 (47.8) | |
| Unknown | 9 (5.1) | 1 (1.5) | 3 (7.7) | 5 (7.2) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jochems, A.; van der Kooij, M.K.; Fiocco, M.; Schouwenburg, M.G.; Aarts, M.J.; van Akkooi, A.C.; van den Berkmortel, F.W.P.J.; Blank, C.U.; van den Eertwegh, A.J.M.; Franken, M.G.; et al. Metastatic Uveal Melanoma: Treatment Strategies and Survival—Results from the Dutch Melanoma Treatment Registry. Cancers 2019, 11, 1007. https://doi.org/10.3390/cancers11071007
Jochems A, van der Kooij MK, Fiocco M, Schouwenburg MG, Aarts MJ, van Akkooi AC, van den Berkmortel FWPJ, Blank CU, van den Eertwegh AJM, Franken MG, et al. Metastatic Uveal Melanoma: Treatment Strategies and Survival—Results from the Dutch Melanoma Treatment Registry. Cancers. 2019; 11(7):1007. https://doi.org/10.3390/cancers11071007
Chicago/Turabian StyleJochems, Anouk, Monique K. van der Kooij, Marta Fiocco, Maartje G. Schouwenburg, Maureen J. Aarts, Alexander C. van Akkooi, Franchette W.P.J. van den Berkmortel, Christian U. Blank, Alfonsus J.M. van den Eertwegh, Margreet G. Franken, and et al. 2019. "Metastatic Uveal Melanoma: Treatment Strategies and Survival—Results from the Dutch Melanoma Treatment Registry" Cancers 11, no. 7: 1007. https://doi.org/10.3390/cancers11071007
APA StyleJochems, A., van der Kooij, M. K., Fiocco, M., Schouwenburg, M. G., Aarts, M. J., van Akkooi, A. C., van den Berkmortel, F. W. P. J., Blank, C. U., van den Eertwegh, A. J. M., Franken, M. G., de Groot, J. B., Haanen, J. B. A. G., Hospers, G. A. P., Koornstra, R. H., Kruit, W. H. J., Louwman, M., Piersma, D., van Rijn, R. S., Suijkerbuijk, K. P. M., ... Kapiteijn, E. (2019). Metastatic Uveal Melanoma: Treatment Strategies and Survival—Results from the Dutch Melanoma Treatment Registry. Cancers, 11(7), 1007. https://doi.org/10.3390/cancers11071007