Systematic Review of Irreversible Electroporation Role in Management of Locally Advanced Pancreatic Cancer

 , , , , , , and
, , , , , , and
Abstract
:1. Introduction
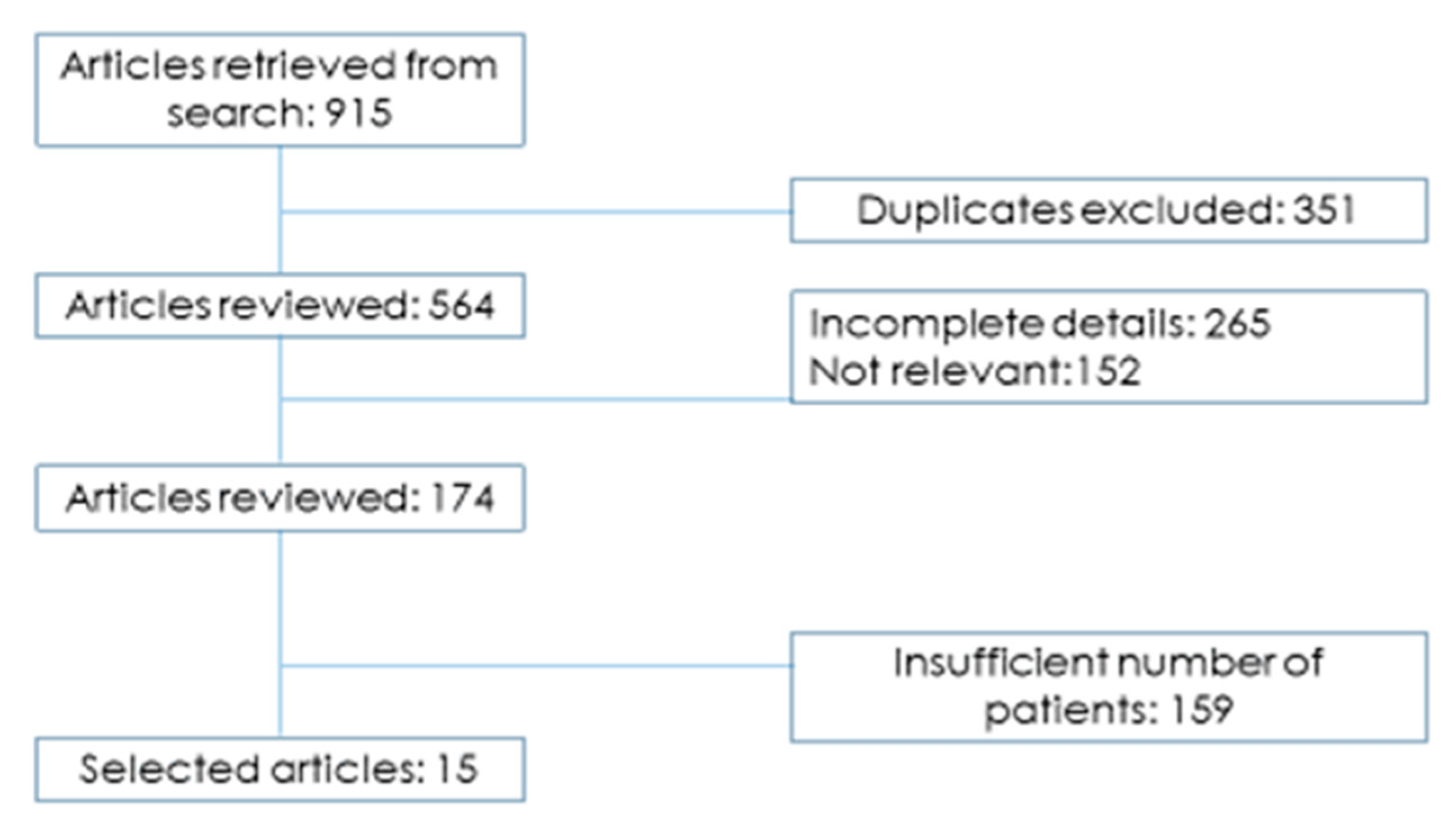
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Marsanic, P.; Mellano, A.; Sottile, A.; De Simone, M. Irreversible electroporation as treatment of locally advanced and as margin accentuation in borderline resectable pancreatic adenocarcinoma. Med. Biol. Eng. Comput. 2017. [Google Scholar] [CrossRef]
- He, J.; Page, J.; Weiss, M.; Wolfgang, C.; Herman, J.; Pawlik, T. Management of borderline and locally advanced pancreatic cancer: Where do we stand? World J. Gastroenterol. 2014, 20, 2255–2266. [Google Scholar] [CrossRef]
- Huguet, F.; Mukherjee, S.; Javie, M. Locally advanced pancreatic cancer: The role of definitive chemoradiotherapy. Clin. Oncol. 2014, 26, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Silvestris, N.; Longo, V.; Cellini, F.; Reni, M.; Bittoni, A.; Cataldo, I.; Partelli, S.; Falconi, M.; Scarpa, A.; Brunetti, O.; et al. Neoadjuvant multimodal treatment of pancreatic ductal adenocarcinoma. Crit. Rev. Oncol. Hematol. 2016, 98, 309–324. [Google Scholar] [CrossRef] [PubMed]
- Paiella, S.; De Pastena, M.; D’Onofrio, M.; Crinò, S.; Pan, T.; De Robertis, R.; Elio, G.; Martone, E.; Bassi, C.; Salvia, R. Palliative therapy in pancreatic cancer—Interventional treatment with radiofrequency ablation/irreversible electroporation. Transl. Gastroenterol. Hepatol. 2018, 3, 80. [Google Scholar] [CrossRef] [PubMed]
- Porcelli, L.; Quatrale, A.E.; Mantuano, P.; Leo, M.G.; Silvestris, N.; Rolland, J.F.; Carioggia, E.; Lioce, M.; Paradiso, A.; Azzariti, A. Optimize radiochemotherapy in pancreatic cancer: PARP inhibitors a new therapeutic opportunity. Mol. Oncol. 2013, 7, 308–322. [Google Scholar] [CrossRef] [PubMed]
- Moir, J.; White, S.A.; French, J.J.; Littler, P.; Manas, D.M. Systematic review of irreversible electroporation in the treatment of advanced pancreatic cancer. Eur. J. Surg. Oncol. 2014, 40, 1598–1604. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.; Ostapoff, K.; Kuvshinoff, B.; Hochwald, S. Ablative therapies for Locally Advanced Pancreatic Cancer. Pancreas 2018, 47, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Keane, M.; Bramis, K.; Pereira, S.; Fusai, G. Systematic review of novel ablative methods in locally advanced pancreatic cancer. World J. Gastroenterol. 2014, 20, 2267–2278. [Google Scholar] [CrossRef]
- Ierardi, A.M.; Lucchina, N.; Petrillo, M.; Floridi, C.; Piacentino, F.; Bacuzzi, A.; Fonio, P.; Fontana, F.; Fugazzola, C.; Brunese, L.; et al. Systematic review of minimally invasive ablation treatment for locally advanced pancreatic cancer. Radiol. Med. 2014, 119, 483–498. [Google Scholar] [CrossRef]
- Vogel, J.; van Veldhuisen, E.; Agnass, P.; Crezee, J.; Dijk, F.; Verheij, J.; van Gulik, T.M.; Meijerink, M.R.; Vroomen, L.G.; van Lienden, K.P.; et al. Time-dependent impact of irreversible electroporation on pancreas, liver, blood vessels and nerves: A systematic review of experimental studies. PLoS ONE 2016, 12, e0174018. [Google Scholar] [CrossRef] [PubMed]
- Belfiore, G.; Belfiore, M.P.; Reginelli, A.; Capasso, R.; Romano, F.; Ianniello, G.P.; Cappabianca, S.; Brunese, L. Cuncurrent chemotherapy alone versus irreversible electroporation followed by chemotherapy on survival patients with locally advanced pancreatic cancer. Med. Oncol. 2017, 34, 38. [Google Scholar] [CrossRef] [PubMed]
- Kluger, M.D.; Epelboym, J.; Schrope, B.A.; Mahendraraj, K.; Hecht, E.M.; Susman, J.; Weintraub, J.L.; Chabot, J.A. Single institution experience with Irreversible Electroporation for T4 Pancreatic Cancer: First 50 patients. Ann. Surg. Oncol. 2016, 23, 1736–1743. [Google Scholar] [CrossRef] [PubMed]
- Mansson, C.; Brahmstaedt, R.; Nilsson, A.; Nygren, P.; Karlson, B.M. Percutaneous irreversible electroporation for treatment of locally advanced pancreatic cancer following chemotherapy or radiochemotherapy. Eur. J. Surg. Oncol. 2016, 42, 1401–1406. [Google Scholar] [CrossRef]
- Lambert, L.; Horejs, J.; Krska, Z.; Hoskovec, D.; Petruzelka, L.; Krechler, T.; Kriz, P.; Briza, J. Treatment of locally advanced pancreatic cancer by percutaneous and intraoperative irreversible electroporation: General hospital cancer center experience. Neoplasma 2016, 63, 269–273. [Google Scholar] [CrossRef]
- Narayanan, G.; Hosein, P.J.; Beulaygue, I.C.; Froud, T.; Scheffer, H.J.; Venkat, S.R.; Echenique, A.M.; Hevert, E.C.; Livingstone, A.S.; Rocha-Lima, C.M.; et al. Percutaneous Image-Guided Irreversible Electroporation for the Treatment of Unresectable, Locally Advanced Pancreatic Adenocarcinoma. J. Vasc. Interv. Radiol. 2017, 28, 342–348. [Google Scholar] [CrossRef]
- Yan, L.; Chen, Y.L.; Su, M.; Liu, T.; Xu, K.; Liang, F.; Gu, W.Q.; Lu, S.C. A Single-institution Experience with Open Irreversible Electroporation for Locally Advanced Pancreatic Carcinoma. Chin. Med. J. 2016, 129, 2920–2925. [Google Scholar] [CrossRef]
- Leen, E.; Picard, J.; Stebbing, J.; Abel, M.; Dhillon, T.; Wasan, H. Percutaneous irreversible electroporation with systemic treatment for locally advanced pancreatic adenocarcinoma. J. Gastrointest. Oncol. 2018, 9, 275–281. [Google Scholar] [CrossRef]
- Zhang, Y.; Shi, J.; Zeng, J.; Alnagger, M.; Zhou, L.; Fang, G.; Long, X.A.; Pan, Z.; Li, Y.; Chen, J.; et al. Percutaneous Irreversible Electroporation for Ablation of Locally Advanced Pancreatic Cancer: Experience from a Chinese Institution. Pancreas 2017, 46, e12–e14. [Google Scholar] [CrossRef]
- Dunki-Jacobs, E.M.; Philips, P.; Martin, R.C. Evaluation of resistance as a measure of successful tumor ablation during irreversible electroporation of the pancreas. J. Am. Coll. Surg. 2014, 218, 179–187. [Google Scholar] [CrossRef]
- Martin, R.C., 2nd; McFarland, K.; Ellis, S.; Velanovich, V. Irreversible electroporation therapy in the management of locally advanced pancreatic adenocarcinoma. J. Am. Coll. Surg. 2012, 215, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.C., 2nd; McFarland, K.; Ellis, S.; Velanovich, V. Irreversible electroporation in locally advanced pancreatic cancer: Potential improved overall survival. Ann. Surg. Oncol. 2013, 20 (Suppl. 3), S443–S449. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.C., 2nd; Kwon, D.; Chalikonda, S.; Sellers, M.; Kotz, E.; Scoggins, C.; McMasters, K.M.; Watkins, K. Treatment of 200 locally advanced (stage III) pancreatic adenocarcinoma patients with irreversible electroporation: Safety and efficacy. Ann. Surg. 2015, 262, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Paiella, S.; Butturini, G.; Frigerio, I.; Salvia, R.; Armatura, G.; Bacchion, M.; Fontana, M.; Martone, E.; Bassi, C. Safety and feasibility of Irreversible Electroporation (IRE) in patients with locally advanced pancreatic cancer: Results of a prospective study. Dig. Surg. 2015, 32, 90–97. [Google Scholar] [CrossRef]
- Vogel, J.A.; Rombouts, S.J.; de Rooij, T.; van Delden, O.M.; Dijkgraaf, M.G.; van Gulik, T.M.; van Hooft, J.E.; van Laarhoven, H.W.; Martin, R.C.; Schoorlemmer, A.; et al. Induction Chemotherapy Followed by Resection or Irreversible Electroporation in Locally Advanced Pancreatic Cancer (IMPALA): A Prospective Cohort Study. Ann. Surg. Oncol. 2017, 24, 2734–2743. [Google Scholar] [CrossRef]
- Scheffer, H.J.; Vroomen, L.G.; de Jong, M.C.; Melenhorst, M.C.; Zonderhuis, B.M.; Daams, F.; Vogel, J.A.; Besselink, M.G.; van Kuijk, C.; Witvliet, J.; et al. Ablation of Locally Advanced Pancreatic Cancer with Percutaneous Irreversible Electroporation: Results of the Phase I/II PANFIRE Study. Radiology 2017, 282, 585–597. [Google Scholar] [CrossRef] [Green Version]
- Ansari, D.; Kristoffersson, S.; Andersson, R.; Bergenfeldt, M. The role of irreversible electroporation (IRE) for locally advanced pancreatic cancer: A sistematic review of safety and efficacy. Scand. J. Gastroenterol. 2017. [Google Scholar] [CrossRef]
- De Liguori Carino, N.; O’Reilly, D.; Siriwardena, A.; Valle, J.W.; Radhakrishna, G.; Pihlak, R.; McNamara, M.G. Irreversible electroporation in pancreatic ductal adenocarcinoma: Is there a role in conjunction with conventional treatment? Eur. J. Surg. Oncol. 2018. [Google Scholar] [CrossRef]
- Tasu, J.; Vesselle, G.; Herpe, G.; Richer, J.P.; Boucecbi, S.; Vélasco, S.; Carretier, M.; Debeane, B.; Tougeron, D. Irreversible electroporation for locally advanced pancreatic cancer. Diagn. Interv. Imaging 2016, 97, 1297–1304. [Google Scholar] [CrossRef]
- Greenberg, A.; Hsu, J.; Bawazeer, M.; Marshall, J.; Friedrich, J.O.; Nathens, A.; Coburn, N.; May, G.R.; Pearsall, E.; McLeod, R.S. Clinical practice guidelines: Management for acute pancreatitis. Can. J. Surg. 2016, 59, 128. [Google Scholar] [CrossRef]
- He, C.; Wang, J.; Sun, S.; Zhang, Y.; Lin, X.; Lao, X.; Cui, B.; Li, S. Irreversible electroporation versus radiotherapy after induction chemotherapy on survival in patients with locally advanced pancreatic cancer: A propensity score analysis. BMC Cancer 2019, 19, 394. [Google Scholar] [CrossRef] [PubMed]
- Huang, K.W.; Yang, P.C.; Pua, U.; Kim, M.D.; Li, S.P.; Qiu, Y.D.; Song, T.Q.; Liang, P.C. The efficacy of combination of induction chemotherapy and irreversible electroporation ablation for patients with locally advanced pancreatic adenocarcinoma. J. Surg. Oncol. 2018, 118, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Bhutiani, N.; Agle, S.; Li, Y.; Li, S.; Martin, R.C., 2nd. Irreversible electroporation enhances delivery of gemcitabine to pancreatic adenocarcinoma. J. Surg. Oncol. 2016, 114, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Choné, L.; Francois, E.; Artru, P.; Biagi, J.J. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [PubMed]
- Gnoni, A.; Licchetta, A.; Scarpa, A.; Azzariti, A.; Brunetti, A.E.; Simone, G.; Nardulli, P.; Santini, D.; Aieta, M.; Delcuratolo, S. Carcinogenesis of pancreatic adenocarcinoma: Precursor lesions. Int. J. Mol. Sci. 2013, 14, 19731–19762. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Ablative Techniques | Target Patients | Ablation Technique | QoL Improvement | Complications |
|---|---|---|---|---|
| HIFU | LAPC Metastatic | Extracorporeal | Pain relief, Opioid intake, Better survival | Pancreatic fistula, gastric ulcers, pseudocyst formation, hematologic disorders |
| RFA | LAPC | Percutaneous Intraoperative | Pain relief | Heat damage, Hemorragies, acute pancreatitis, pancreatic fistula, biliary or duodenal burn, vein thrombosis |
| IRE | LAPC | Percutaneous Intraoperative | Pain relief, Opioid intake, Better survival | Pancreatic fistula, mild pancreatitits, vessel thrombosis, pseudoaneurysm |
| Cryoablation | LAPC Metastatic | Percutaneous Intraoperative | Mild pain relief | Severe pancreatitis, bleeding, pancreatic fistula, delayed gastric emptying |
| Microwave | LAPC | Percutaneous Intraoperative | Few reports | Mild pancreatitis, pancreatic fistula, minor bleeding |
| References | Pts (n) | Age | T Size (cm) | Prior RT (n) | Prior Cht (n) | Technique | Complication Rate (%) | Median OS (mo) | Mortality (%) |
|---|---|---|---|---|---|---|---|---|---|
| Belfiore [12] | 29 | 68.5 | 4.5 | NA | NA | Percut | 0 | 14 (d) | NA |
| Kluger [13] | 50 | 68.2 | 3.2 | Open | 24.5 | 12 (t) | 6 | ||
| Dunkl-Jacobs [20] | 65 | NA | NA | 37 | 43 | Percut/Open | 20 | NA | NA |
| Mansson [14] | 24 | 65 | 3.5 | 10 | 22 | Percut | 45.8 | 17.9 (d) | 4 |
| Lambert [15] | 21 | 68.2 | 3.9 | NA | 5 | Percut/Open | 23.8 | 10 (t) | 0 |
| Martin [21] | 27 | 61 | 3.0 | Percut/Open | 33 | 17.9 (d) | 4 | ||
| Martin [22] | 54 | 61 | 3.2 | Open/VLS | 59.2 | 20.2 (d) | 2 | ||
| Martin [23] | 200 | 62 | 2.8 | 77 | 130 | Open | 37 | 24.9 (d) | 2 |
| Paiella [24] | 10 | 66 | 3 | 4 | 10 | Open | 10 | 15.3 (d) | 0 |
| Vogel [25] | 15 | NA | NA | 0 | 9 | Open | 53 | 16 (d) | 13 |
| Narayanan [16] | 50 | 62.5 | 3.2 | 30 | 50 | Percut | 20 | 27 (d) | 6 |
| Yan [17] | 25 | 58 | 4.2 | 3 | 1 | Open | 36 | NA | 4 |
| Leen [18] | 75 | 63.4 | NA | 4 | 75 | Percut | 25 | 27 (t) | 0 |
| Zhang [19] | 21 | NA | 3.5 | NA | NA | Percut | nr | NA | NA |
| Scheffer [26] | 25 | 61 | 4 | 0 | 13 | Percut | 40 | 17 (d) | 0 |
| Trial ID | Title | Phase | Number of Patients | Countries |
|---|---|---|---|---|
| NCT02791503 | CROSSFIRE Trial: Cross atlantic randomized controlled trial comparing outcome in survival after systemic plus focal therapy for inoperable pancreatic carcinoma: RT vs. IRE | 2–3 | 138 | The Netherlands |
| NCT03080974 | Immunotherapy and Irreversible Electroporation in the treatment of advanced pancreatic adenocarcinoma | 2 | 10 | USA |
| NCT02718859 | Study of the combined therapy of IRE and Natural Killer Cells for advanced pancreatic cancer | 1–2 | 60 | China |
| NCT02041936 | Evaluation of the short and intermediate term outcomes of ablation of locally advanced unresectable pancreatic cancer using the Nanoknife IRE System—A prospective study | NA | 12 | USA |
| NCT03257150 | IRE for locally advanced pancreatic ductal adenocarcinoma (LEAP TRIAL): A phase I/II prospective trial | 1–2 | 47 | Canada |
| NCT03105921 | IRE (Nanoknife) for the Treatment of Pancreatic Adenocarcinoma | NA | 20 | France |
| NCT02674100 | AHPBA Pancreatic Irreversible electroporation (IRE) registry for pancreatic cancer | NA | 500 | USA, Japan, Taiwan, UK |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lafranceschina, S.; Brunetti, O.; Delvecchio, A.; Conticchio, M.; Ammendola, M.; Currò, G.; Piardi, T.; de’Angelis, N.; Silvestris, N.; Memeo, R. Systematic Review of Irreversible Electroporation Role in Management of Locally Advanced Pancreatic Cancer. Cancers 2019, 11, 1718. https://doi.org/10.3390/cancers11111718
Lafranceschina S, Brunetti O, Delvecchio A, Conticchio M, Ammendola M, Currò G, Piardi T, de’Angelis N, Silvestris N, Memeo R. Systematic Review of Irreversible Electroporation Role in Management of Locally Advanced Pancreatic Cancer. Cancers. 2019; 11(11):1718. https://doi.org/10.3390/cancers11111718
Chicago/Turabian StyleLafranceschina, Stefano, Oronzo Brunetti, Antonella Delvecchio, Maria Conticchio, Michele Ammendola, Giuseppe Currò, Tullio Piardi, Nicola de’Angelis, Nicola Silvestris, and Riccardo Memeo. 2019. "Systematic Review of Irreversible Electroporation Role in Management of Locally Advanced Pancreatic Cancer" Cancers 11, no. 11: 1718. https://doi.org/10.3390/cancers11111718