Evaluation and Validation of Plasma Proteins Using Two Different Protein Detection Methods for Early Detection of Colorectal Cancer

 , , ,
, , , 
Abstract
1. Introduction
2. Results
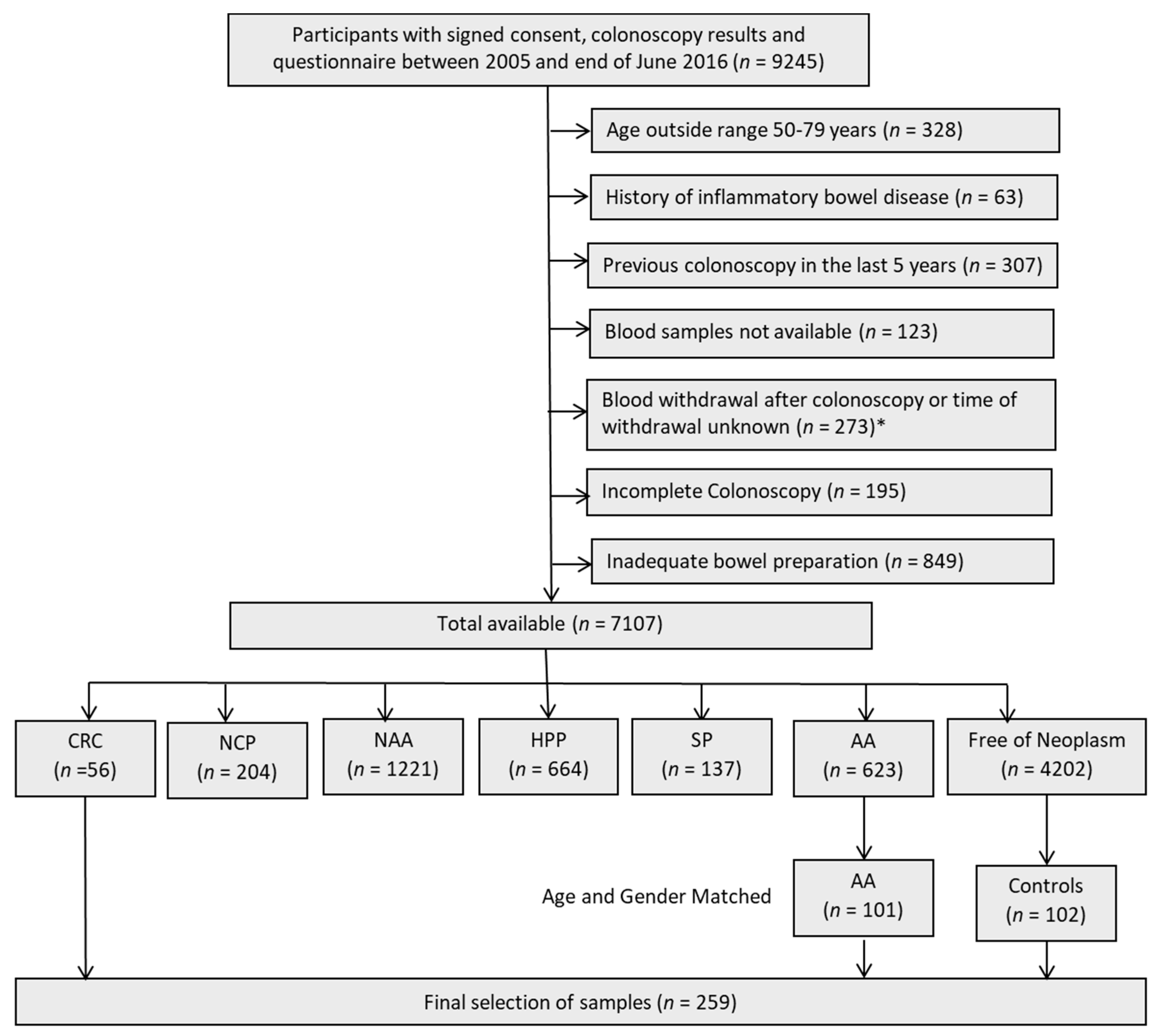
2.1. Characteristics of Study Population
2.2. Individual Markers
2.3. Correlation Analysis
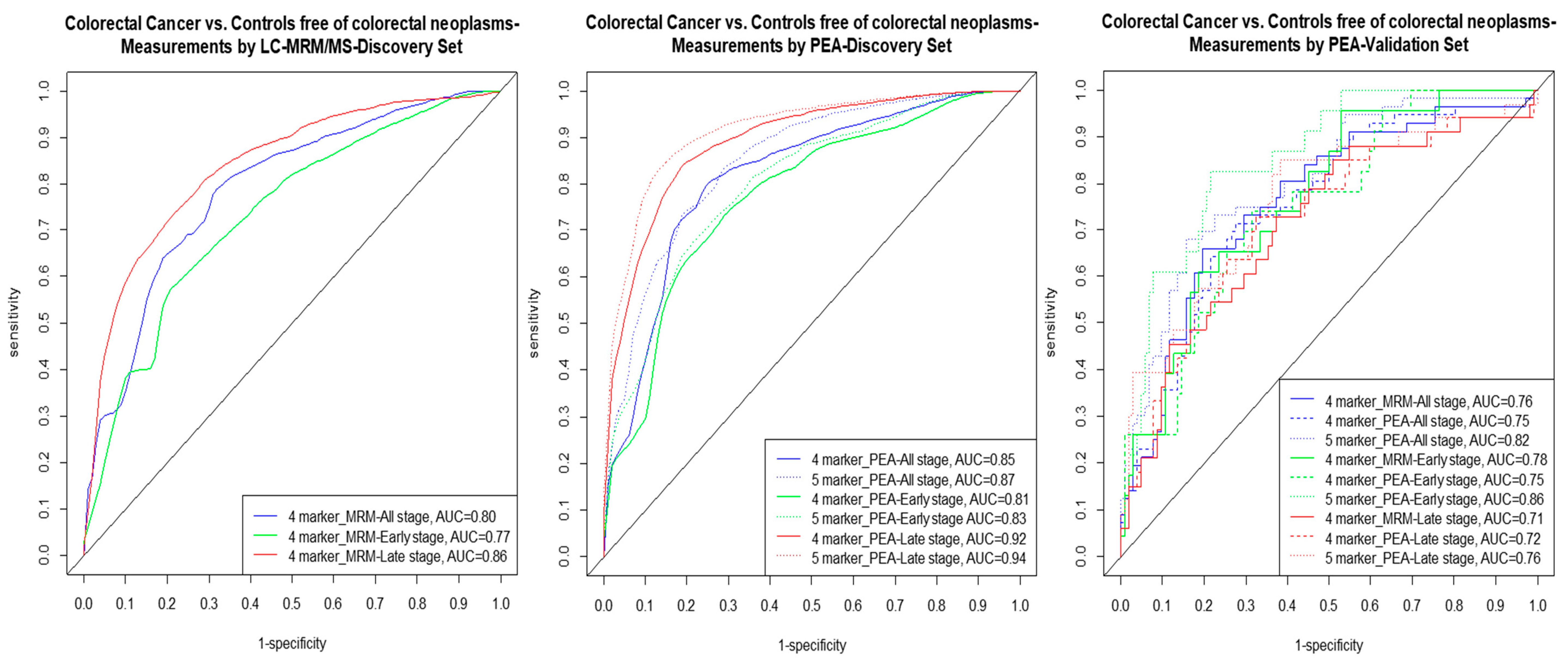
2.4. Multimarker Signatures
3. Discussion
4. Methods
4.1. Study Design
4.2. Study Population: Discovery Set
4.3. Study Population: Validation Set
4.4. Sample Collection and Storage
4.5. Laboratory Assays
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Stock, C.; Hoffmeister, M. Effect of screening sigmoidoscopy and screening colonoscopy on colorectal cancer incidence and mortality: Systematic review and meta-analysis of randomised controlled trials and observational studies. BMJ 2014, 348, g2467. [Google Scholar] [CrossRef] [PubMed]
- Zauber, A.G. The impact of screening on colorectal cancer mortality and incidence: Has it really made a difference? Dig. Dis. Sci. 2015, 60, 681–691. [Google Scholar] [CrossRef]
- Atkin, W.; Wooldrage, K.; Parkin, D.M.; Kralj-Hans, I.; MacRae, E.; Shah, U.; Duffy, S.; Cross, A.J. Long term effects of once-only flexible sigmoidoscopy screening after 17 years of follow-up: The uk flexible sigmoidoscopy screening randomised controlled trial. Lancet 2017, 389, 1299–1311. [Google Scholar] [CrossRef]
- Brenner, H.; Chen, C. The colorectal cancer epidemic: Challenges and opportunities for primary, secondary and tertiary prevention. Br. J. Cancer 2018, 119, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Klabunde, C.; Blom, J.; Bulliard, J.L.; Garcia, M.; Hagoel, L.; Mai, V.; Patnick, J.; Rozjabek, H.; Senore, C.; Tornberg, S. Participation rates for organized colorectal cancer screening programmes: An international comparison. J. Med. Screen. 2015, 22, 119–126. [Google Scholar] [CrossRef]
- Bretthauer, M.; Kaminski, M.F.; Løberg, M.; Zauber, A.G.; Regula, J.; Kuipers, E.J.; Påhlman, L.; Hernán, M.A.; McFadden, E.; Sunde, A.; et al. Population-based colonoscopy screening for colorectal cancer: A european randomized trial. JAMA Intern. Med. 2016, 176, 894–902. [Google Scholar] [CrossRef]
- Robertson, D.J.; Lee, J.K.; Boland, C.R.; Dominitz, J.A.; Giardiello, F.M.; Johnson, D.A.; Kaltenbach, T.; Lieberman, D.; Levin, T.R.; Rex, D.K. Recommendations on fecal immunochemical testing to screen for colorectal neoplasia: A consensus statement by the us multi-society task force on colorectal cancer. Gastroenterology 2017, 152, 1217–1237. [Google Scholar] [CrossRef]
- Adler, A.; Geiger, S.; Keil, A.; Bias, H.; Schatz, P.; deVos, T.; Dhein, J.; Zimmermann, M.; Tauber, R.; Wiedenmann, B. Improving compliance to colorectal cancer screening using blood and stool based tests in patients refusing screening colonoscopy in germany. BMC Gastroenterol. 2014, 14, 183. [Google Scholar] [CrossRef]
- Ponomarenko, E.A.; Poverennaya, E.V.; Ilgisonis, E.V.; Pyatnitskiy, M.A.; Kopylov, A.T.; Zgoda, V.G.; Lisitsa, A.V.; Archakov, A.I. The size of the human proteome: The width and depth. Int. J. Anal. Chem. 2016, 2016, 7436849. [Google Scholar] [CrossRef]
- Kuzyk, M.A.; Smith, D.; Yang, J.; Cross, T.J.; Jackson, A.M.; Hardie, D.B.; Anderson, N.L.; Borchers, C.H. Multiple reaction monitoring-based, multiplexed, absolute quantitation of 45 proteins in human plasma. Mol. Cell. Proteomics 2009, 8, 1860–1877. [Google Scholar] [CrossRef] [PubMed]
- Domanski, D.; Percy, A.J.; Yang, J.; Chambers, A.G.; Hill, J.S.; Freue, G.V.; Borchers, C.H. Mrm-based multiplexed quantitation of 67 putative cardiovascular disease biomarkers in human plasma. Proteomics 2012, 12, 1222–1243. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Zucknick, M.; Werner, S.; Knebel, P.; Brenner, H. Head-to-head comparison and evaluation of 92 plasma protein biomarkers for early detection of colorectal cancer in a true screening setting. Clin. Cancer Res. 2015, 21, 3318–3326. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Qian, J.; Werner, S.; Cuk, K.; Knebel, P.; Brenner, H. Development and validation of a panel of five proteins as blood biomarkers for early detection of colorectal cancer. Clin. Epidemiol. 2017, 9, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, M.; Erben, V.; Schrotz-King, P.; Brenner, H. Cell line secretome and tumor tissue proteome markers for early detection of colorectal cancer: A systematic review. Cancers 2017, 9, 156. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, M.; Gies, A.; Werner, S.; Schrotz-King, P.; Brenner, H. Blood-based protein signatures for early detection of colorectal cancer: A systematic review. Clin. Transl. Gastroenterol. 2017, 8, e128. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.G.; Gerszten, R.E. Emerging affinity-based proteomic technologies for large-scale plasma profiling in cardiovascular disease. Circulation 2017, 135, 1651–1664. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Kim, J.W.; Jeon, S.Y.; Park, B.K.; Han, B.G. Proteomic analysis of the effect of storage temperature on human serum. Ann. Clin. Lab. Sci. 2010, 40, 61–70. [Google Scholar]
- Enroth, S.; Hallmans, G.; Grankvist, K.; Gyllensten, U. Effects of long-term storage time and original sampling month on biobank plasma protein concentrations. EBioMedicine 2016, 12, 309–314. [Google Scholar] [CrossRef] [PubMed]
- Shen, Q.; Bjorkesten, J.; Galli, J.; Ekman, D.; Broberg, J.; Nordberg, N.; Tillander, A.; Kamali-Moghaddam, M.; Tybring, G.; Landegren, U. Strong impact on plasma protein profiles by precentrifugation delay but not by repeated freeze-thaw cycles, as analyzed using multiplex proximity extension assays. Clin. Chem. Lab. Med. 2018, 56, 582–594. [Google Scholar] [CrossRef]
- Alnabulsi, A.; Murray, G.I. Proteomics for early detection of colorectal cancer: Recent updates. Expert Rev. Proteomics 2018, 15, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Surinova, S.; Choi, M.; Tao, S.; Schueffler, P.J.; Chang, C.-Y.; Clough, T.; Vyslouzil, K.; Khoylou, M.; Srovnal, J.; Liu, Y.; et al. Prediction of colorectal cancer diagnosis based oncirculating plasma proteins. EMBO Mol. Med. 2015, 7, 1166–1178. [Google Scholar] [CrossRef] [PubMed]
- Ciarloni, L.; Ehrensberger, S.H.; Imaizumi, N.; Monnier-Benoit, S.; Nichita, C.; Myung, S.J.; Kim, J.S.; Song, S.Y.; Kim, T.I.; van der Weg, B.; et al. Development and clinical validation of a blood test based on 29-gene expression for early detection of colorectal cancer. Clin. Cancer Res. 2016, 22, 4604–4611. [Google Scholar] [CrossRef] [PubMed]
- Barderas, R.; Mendes, M.; Torres, S.; Bartolome, R.A.; Lopez-Lucendo, M.; Villar-Vazquez, R.; Pelaez-Garcia, A.; Fuente, E.; Bonilla, F.; Casal, J.I. In-depth characterization of the secretome of colorectal cancer metastatic cells identifies key proteins in cell adhesion, migration, and invasion. Mol. Cell. Proteomics 2013, 12, 1602–1620. [Google Scholar] [CrossRef] [PubMed]
- Rodia, M.T.; Solmi, R.; Pasini, F.; Nardi, E.; Mattei, G.; Ugolini, G.; Ricciardiello, L.; Strippoli, P.; Miglio, R.; Lauriola, M. Lgals4, ceacam6, tspan8, and col1a2: Blood markers for colorectal cancer-validation in a cohort of subjects with positive fecal immunochemical test result. Clin. Colorectal Cancer 2018, 17, e217–e228. [Google Scholar] [CrossRef]
- Rodia, M.T.; Ugolini, G.; Mattei, G.; Montroni, I.; Zattoni, D.; Ghignone, F.; Veronese, G.; Marisi, G.; Lauriola, M.; Strippoli, P.; et al. Systematic large-scale meta-analysis identifies a panel of two mrnas as blood biomarkers for colorectal cancer detection. Oncotarget 2016, 7, 30295–30306. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.D.; Li, L.; Wang, Y.; Thoburn, C.; Afsari, B.; Danilova, L.; Douville, C.; Javed, A.A.; Wong, F.; Mattox, A.; et al. Detection and localization of surgically resectable cancers with a multi-analyte blood test. Science 2018, 359, 926–930. [Google Scholar] [CrossRef]
- Kohn, M.A.; Carpenter, C.R.; Newman, T.B. Understanding the direction of bias in studies of diagnostic test accuracy. Acad. Emerg. Med. 2013, 20, 1194–1206. [Google Scholar] [CrossRef]
- Whiting, P.; Rutjes, A.W.; Reitsma, J.B.; Glas, A.S.; Bossuyt, P.M.; Kleijnen, J. Sources of variation and bias in studies of diagnostic accuracy: A systematic review. Ann. Intern. Med. 2004, 140, 189–202. [Google Scholar] [CrossRef]
- Potter, N.T.; Hurban, P.; White, M.N.; Whitlock, K.D.; Lofton-Day, C.E.; Tetzner, R.; Koenig, T.; Quigley, N.B.; Weiss, G. Validation of a real-time pcr-based qualitative assay for the detection of methylated sept9 DNA in human plasma. Clin. Chem. 2014, 60, 1183–1191. [Google Scholar] [CrossRef]
- Church, T.R.; Wandell, M.; Lofton-Day, C.; Mongin, S.J.; Burger, M.; Payne, S.R.; Castaños-Vélez, E.; Blumenstein, B.A.; Rösch, T.; Osborn, N.; et al. Prospective evaluation of methylated sept9 in plasma for detection of asymptomatic colorectal cancer. Gut 2014, 63, 317–325. [Google Scholar] [CrossRef] [PubMed]
- Wild, N.; Andres, H.; Rollinger, W.; Krause, F.; Dilba, P.; Tacke, M.; Karl, J. A combination of serum markers for the early detection of colorectal cancer. Clin. Cancer Res. 2010, 16, 6111–6121. [Google Scholar] [CrossRef]
- Lumachi, F.; Marino, F.; Orlando, R.; Chiara, G.B.; Basso, S.M. Simultaneous multianalyte immunoassay measurement of five serum tumor markers in the detection of colorectal cancer. Anticancer Res. 2012, 32, 985–988. [Google Scholar] [PubMed]
- Werner, S.; Krause, F.; Rolny, V.; Strobl, M.; Morgenstern, D.; Datz, C.; Chen, H.; Brenner, H. Evaluation of a 5-marker blood test for colorectal cancer early detection in a colorectal cancer screening setting. Clin. Cancer Res. 2016, 22, 1725–1733. [Google Scholar] [CrossRef] [PubMed]
- Brenner, H.; Calderazzo, S.; Seufferlein, T.; Ludwig, L.; Dikopoulos, N.; Mangold, J.; Böck, W.; Stolz, T.; Eisenbach, T.; Block, T.; et al. Effect of a single aspirin dose prior to fecal immunochemical testing on test sensitivity for detecting advanced colorectal neoplasms: A randomized clinical trialeffect of single-dose aspirin prior to fit on colorectal cancer detectioneffect of single-dose aspirin prior to fit on colorectal cancer detection. JAMA 2019, 321, 1686–1692. [Google Scholar] [PubMed]
- Hundt, S.; Haug, U.; Brenner, H. Comparative evaluation of immunochemical fecal occult blood tests for colorectal adenoma detection. Ann. Intern. Med. 2009, 150, 162–169. [Google Scholar] [CrossRef]
- Brenner, H.; Tao, S.; Haug, U. Low-dose aspirin use and performance of immunochemical fecal occult blood tests. JAMA 2010, 304, 2513–2520. [Google Scholar] [CrossRef] [PubMed]
- Gies, A.; Cuk, K.; Schrotz-King, P.; Brenner, H. Direct comparison of diagnostic performance of 9 quantitative fecal immunochemical tests for colorectal cancer screening. Gastroenterology 2018, 154, 93–104. [Google Scholar] [CrossRef]
- Brenner, H.; Hoffmeister, M.; Arndt, V.; Stegmaier, C.; Altenhofen, L.; Haug, U. Protection from right- and left-sided colorectal neoplasms after colonoscopy: Population-based study. J. Natl. Cancer Inst. 2010, 102, 89–95. [Google Scholar] [CrossRef]
- Percy, A.J.; Chambers, A.G.; Parker, C.E.; Borchers, C.H. Absolute quantitation of proteins in human blood by multiplexed multiple reaction monitoring mass spectrometry. Methods Mol. Biol. 2013, 1000, 167–189. [Google Scholar]
- Assarsson, E.; Lundberg, M.; Holmquist, G.; Björkesten, J.; Bucht Thorsen, S.; Ekman, D.; Eriksson, A.; Rennel Dickens, E.; Ohlsson, S.; Edfeldt, G.; et al. Homogenous 96-plex pea immunoassay exhibiting high sensitivity, specificity, and excellent scalability. PLoS ONE 2014, 9, e95192. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Hochberg, Y. Controlling the false discovery rate—A practical and powerful approach to multiple testing. J. R. Stat. Soc. Ser. B-Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Efron, B.; Tibshirani, R. Improvements on cross-validation: The 632+ bootstrap method. J. Am. Stat. Assoc. 1997, 92, 548–560. [Google Scholar]
- The R Development Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2016. [Google Scholar]
- Gies, A.; Bhardwaj, M.; Stock, C.; Schrotz-King, P.; Brenner, H. Quantitative fecal immunochemical tests for colorectal cancer screening. Int. J. Cancer. 2018, 143, 234–244. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Group | Discovery Set | Validation Set | Participants of Screening Colonoscopy | ||||
|---|---|---|---|---|---|---|---|
| iDa (Clinical) CRC | ASTER (Mostly Screening) Controls | BLITZ Matched Set (Screening) | BLITZ (Screening) | ||||
| CRC | AA | Controls | AA | Controls | |||
| Total | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) |
| 96 | 94 | 56 | 101 | 102 | 623 | 4202 | |
| Age in years | |||||||
| 50–59 | 22 (23) | 25 (27) | 10 (18) | 22 (21) | 21 (21) | 237 (38) | 1916 (46) |
| 60–69 | 41 (43) | 44 (46) | 28 (50) | 49 (49) | 50 (49) | 247 (40) | 1614 (38) |
| 70–79 | 33 (34) | 25 (27) | 18 (32) | 30 (30) | 31 (30) | 139 (22) | 672 (16) |
| Mean | 64.8 | 64.1 | 66.0 | 65.5 | 65.4 | 63.3 | 61.9 |
| Median | 65.0 | 66.0 | 65.0 | 65.0 | 65.5 | 62.0 | 60.0 |
| SD | 7.0 | 7.4 | 5.8 | 6.6 | 6.9 | 5.9 | 6.5 |
| Gender distribution | |||||||
| Male | 59 (61) | 55 (59) | 36 (64) | 65 (64) | 66 (65) | 393 (63) | 1808 (43) |
| Female | 37 (39) | 39 (41) | 20 (36) | 36 (36) | 36 (35) | 230 (37) | 2394 (57) |
| Stage distribution | |||||||
| Stage I | 17 (18) | - | 17 (30) | - | - | - | - |
| Stage II | 31 (32) | - | 6 (11) | - | - | - | - |
| Stage III | 22 (23) | - | 26 (46) | - | - | - | - |
| Stage IV | 26 (27) | - | (13) | - | - | - | - |
| Early stage (I/II) | 48 (50) | - | 23 (41) | - | - | - | - |
| Late stage (III/IV) | 48 (50) | - | 33 (59) | - | - | - | - |
| Protein Biomarkers | Discovery Set (LC/MRM-MS Measurements) | Discovery Set (PEA Measurements) | Validation Set (PEA Measurements) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p-val | p-valadj | AUC (95% CI) | AUCBS (95% CI) | Se% at 90% Sp | p-val | p-valadj | AUC (95% CI) | AUCBS (95% CI) | Se% at 90% Sp | p-val | p-valadj | AUC (95% CI) | AUCBS (95% CI) | Se% at 90% Sp | |
| CDH5 | 0.35 | 0.38 | 0.54 (0.46–0.62) | 0.48 (0.36–0.61) | 8 | 0.20 | 0.25 | 0.55 (0.47–0.64) | 0.50 (0.36–0.64) | 10 | <0.05 | <0.05 | 0.62 (0.54–0.71) | 0.59 (0.50–0.73) | 12 |
| Gal 3 | 0.51 | 0.51 | 0.53 (0.45–0.61) | 0.47 (0.36–0.59) | 7 | 0.84 | 0.84 | 0.51 (0.43–0.59) | 0.46 (0.37–0.55) | 7 | 0.13 | 0.16 | 0.57 (0.48–0.67) | 0.51 (0.33–0.67) | 11 |
| IGFBP2 | <0.05 | <0.05 | 0.61 (0.53–0.69) | 0.58 (0.50–0.71) | 24 | <0.05 | <0.05 | 0.61 (0.53–0.69) | 0.58 (0.50–0.72) | 21 | 0.43 | 0.46 | 0.54 (0.44–0.63) | 0.48 (0.34–0.62) | 10 |
| MASP1 | <0.001 | <0.001 | 0.68 (0.61–0.76) | 0.67 (0.58–0.78) | 27 | <0.001 | <0.001 | 0.65 (0.57–0.72) | 0.63 (0.53–0.75) | 20 | 0.08 | 0.11 | 0.58 (0.49–0.68) | 0.53 (0.37–0.68) | 13 |
| MMP9 | 0.24 | 0.33 | 0.55 (0.47–0.63) | 0.50 (0.37–0.62) | 10 | 0.32 | 0.36 | 0.55 (0.38–0.54) | 0.50 (0.38–0.62) | 10 | 0.05 | 0.08 | 0.59 (0.50–0.69) | 0.55 (0.46–0.71) | 16 |
| MPO | 0.06 | 0.11 | 0.58 (0.50–0.66) | 0.47 (0.36–0.59) | 8 | <0.005 | <0.005 | 0.63 (0.55–0.71) | 0.60 (0.52–0.73) | 17 | 0.53 | 0.53 | 0.53 (0.44–0.62) | 0.46 (0.35–0.57) | 6 |
| OPN | <0.001 | <0.001 | 0.64 (0.57–0.72) | 0.62 (0.54–0.75) | 26 | <0.001 | <0.001 | 0.75 (0.68–0.82) | 0.73 (0.65–0.84) | 35 | <0.05 | <0.05 | 0.62 (0.53–0.71) | 0.59 (0.49–0.73) | 18 |
| PON3 | <0.001 | <0.001 | 0.73 (0.66–0.80) | 0.72 (0.63–0.82) | 32 | <0.001 | <0.001 | 0.75 (0.68–0.82) | 0.74 (0.66–0.84) | 43 | 0.05 | 0.08 | 0.59 (0.51–0.68) | 0.54 (0.37–0.69) | 11 |
| PRTN3 | 0.13 | 0.21 | 0.56 (0.48–0.64) | 0.51 (0.36–0.65) | 10 | <0.001 | <0.001 | 0.64 (0.56–0.72) | 0.61 (0.54–0.74) | 18 | 0.06 | 0.09 | 0.59 (0.50–0.68) | 0.49 (0.31–0.65) | 5 |
| SPARC | 0.30 | 0.37 | 0.54 (0.46–0.63) | 0.49 (0.37–0.61) | 10 | 0.33 | 0.36 | 0.54 (0.46–0.62) | 0.49 (0.36–0.62) | 9 | 0.41 | 0.46 | 0.54 (0.45–0.63) | 0.48 (0.36–0.61) | 5 |
| TR | <0.001 | <0.001 | 0.67 (0.60–0.75) | 0.66 (0.57–0.77) | 35 | <0.001 | <0.001 | 0.70 (0.63–0.77) | 0.69 (0.60–0.79) | 36 | <0.001 | <0.001 | 0.74 (0.66–0.82) | 0.72 (0.64–0.85) | 33 |
| AREG | - | - | - | - | - | <0.001 | <0.001 | 0.79 (0.73–0.86) | 0.78 (0.70–0.87) | 54 | <0.001 | <0.001 | 0.72 (0.64–0.80) | 0.70 (0.61–0.83) | 35 |
| Protein Biomarkers Discovered in the Signatures | Discovery Set (LC/MRM-MS Measurements) | Discovery Set (PEA Measurements) | Validation Set (PEA Measurements) as in Screening Population | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| AUCBS | AUC | Se % at 80% Sp | Se % at 90% Sp | AUCBS | AUC | Se % at 80% Sp | Se % at 90% Sp | Weighted AUC (95% CI) | Se % at 80% Sp | Se % at 90% Sp | |
| All stages CRC | |||||||||||
| MASP1 + OPN + PON3 + TR # | 0.80 | 0.80 | 65 | 35 | - | - | - | - | 0.76 (0.67–0.85) | 46 | 36 |
| - | - | - | - | 0.84 | 0.85 | 73 | 42 | 0.75 (0.65–0.84) | 46 | 36 | |
| AREG + MASP1 + OPN+ PON3 + TR § | - | - | - | - | 0.87 | 0.87 | 74 | 57 | 0.82 (0.74–0.89) | 71 | 50 |
| Early stages CRC | |||||||||||
| MASP1 + OPN + PON3 + TR # | 0.75 | 0.77 | 56 | 38 | - | - | - | - | 0.78 (0.66–0.88) | 43 | 30 |
| - | - | - | - | 0.79 | 0.81 | 64 | 30 | 0.75 (0.63–0.86) | 52 | 35 | |
| AREG + MASP1 + OPN + PON3 + TR § | - | - | - | - | 0.81 | 0.83 | 69 | 42 | 0.86 (0.77–0.92) | 83 | 43 |
| Late stages CRC | |||||||||||
| MASP1 + OPN+ PON3 + TR # | 0.84 | 0.86 | 72 | 59 | - | - | - | - | 0.71 (0.59–0.83) | 48 | 21 |
| - | - | - | - | 0.90 | 0.92 | 85 | 67 | 0.72 (0.59–0.83) | 55 | 33 | |
| AREG + MASP1 + OPN+ PON3 + TR § | - | - | - | - | 0.92 | 0.94 | 88 | 78 | 0.76 (0.64–0.86) | 58 | 45 |
| AA | |||||||||||
| MASP1 + OPN+ PON3 + TR # | - | - | - | - | - | - | - | - | 0.58 (0.48–0.68) | 28 | 19 |
| - | - | - | - | - | - | - | - | 0.59 (0.49–0.68) | 32 | 21 | |
| AREG + MASP1 + OPN + PON3 + TR § | - | - | - | - | - | - | - | - | 0.60 (0.51–0.69) | 36 | 23 |
| Biomarkers | Name | Uniprot ID | Molecular Function | Biological Process |
|---|---|---|---|---|
| AREG | amphiregulin | P15514 | cytokine, growth factor | Cell–cell signaling, cell proliferation |
| MASP1 | mannan-binding lectin serine protease 1 | P48740 | hydrolase, protease, serine protease | Complement activation lectin pathway, Immunity, Innate immunity |
| OPN/SPP1 | osteopontin | P10451 | cytokine | Biomineralization, Cell adhesion |
| PON3 | serum paraoxonase lactonase 3 | Q15166 | hydrolase | Calcium, Metal-binding |
| TR/TFRC | transferrin receptor protein 1 | P02786 | host cell receptor for virus entry, receptor | Endocytosis, Host–virus interaction |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bhardwaj, M.; Gies, A.; Weigl, K.; Tikk, K.; Benner, A.; Schrotz-King, P.; Borchers, C.H.; Brenner, H. Evaluation and Validation of Plasma Proteins Using Two Different Protein Detection Methods for Early Detection of Colorectal Cancer. Cancers 2019, 11, 1426. https://doi.org/10.3390/cancers11101426
Bhardwaj M, Gies A, Weigl K, Tikk K, Benner A, Schrotz-King P, Borchers CH, Brenner H. Evaluation and Validation of Plasma Proteins Using Two Different Protein Detection Methods for Early Detection of Colorectal Cancer. Cancers. 2019; 11(10):1426. https://doi.org/10.3390/cancers11101426
Chicago/Turabian StyleBhardwaj, Megha, Anton Gies, Korbinian Weigl, Kaja Tikk, Axel Benner, Petra Schrotz-King, Christoph H. Borchers, and Hermann Brenner. 2019. "Evaluation and Validation of Plasma Proteins Using Two Different Protein Detection Methods for Early Detection of Colorectal Cancer" Cancers 11, no. 10: 1426. https://doi.org/10.3390/cancers11101426
APA StyleBhardwaj, M., Gies, A., Weigl, K., Tikk, K., Benner, A., Schrotz-King, P., Borchers, C. H., & Brenner, H. (2019). Evaluation and Validation of Plasma Proteins Using Two Different Protein Detection Methods for Early Detection of Colorectal Cancer. Cancers, 11(10), 1426. https://doi.org/10.3390/cancers11101426