Persistent Head and Neck Cancer Following First-Line Treatment


 ,
, 
Abstract
1. Introduction
2. Results
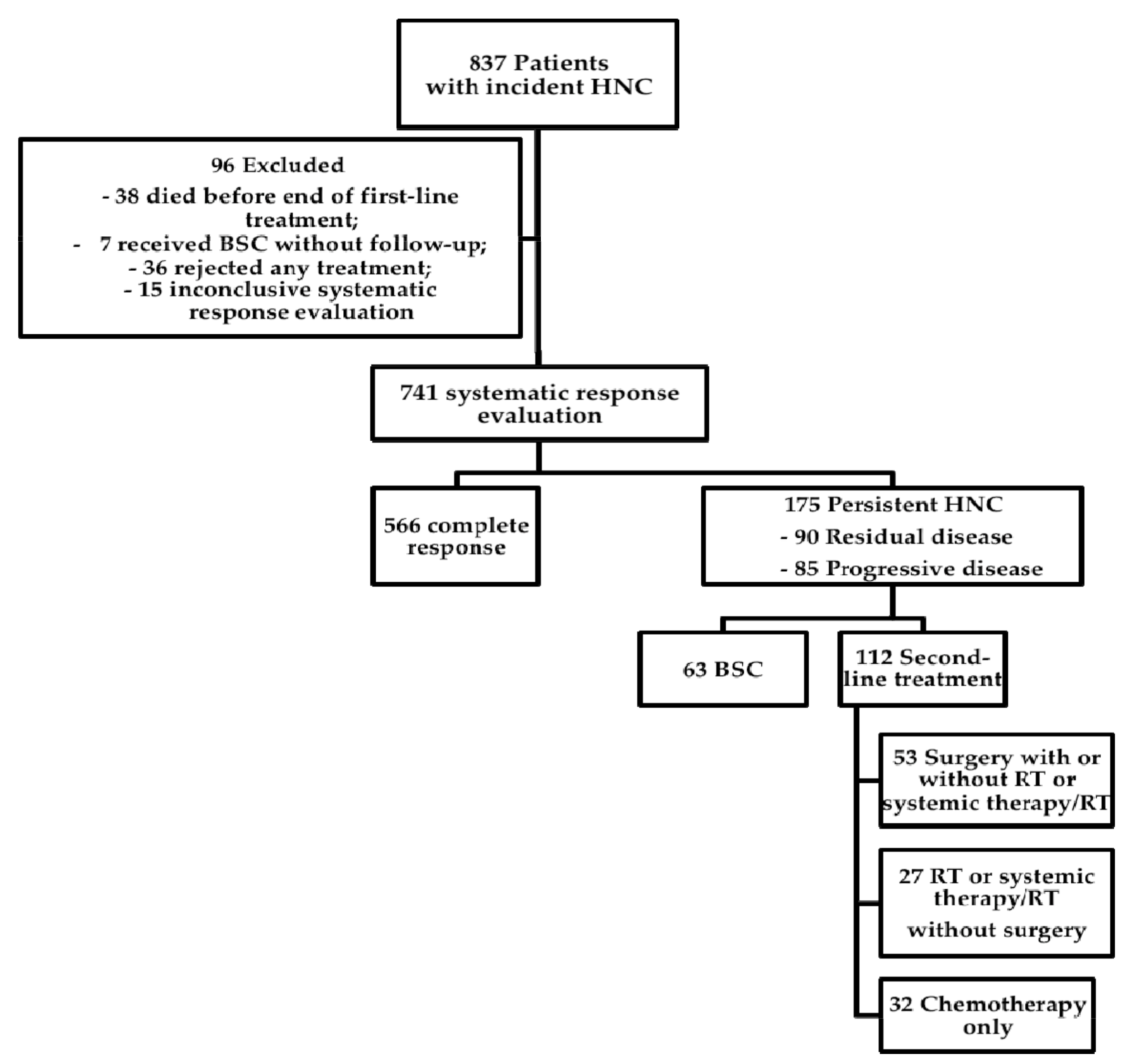
2.1. Tumor Registry Population, Exclusions, and Results of First-Line Treatment
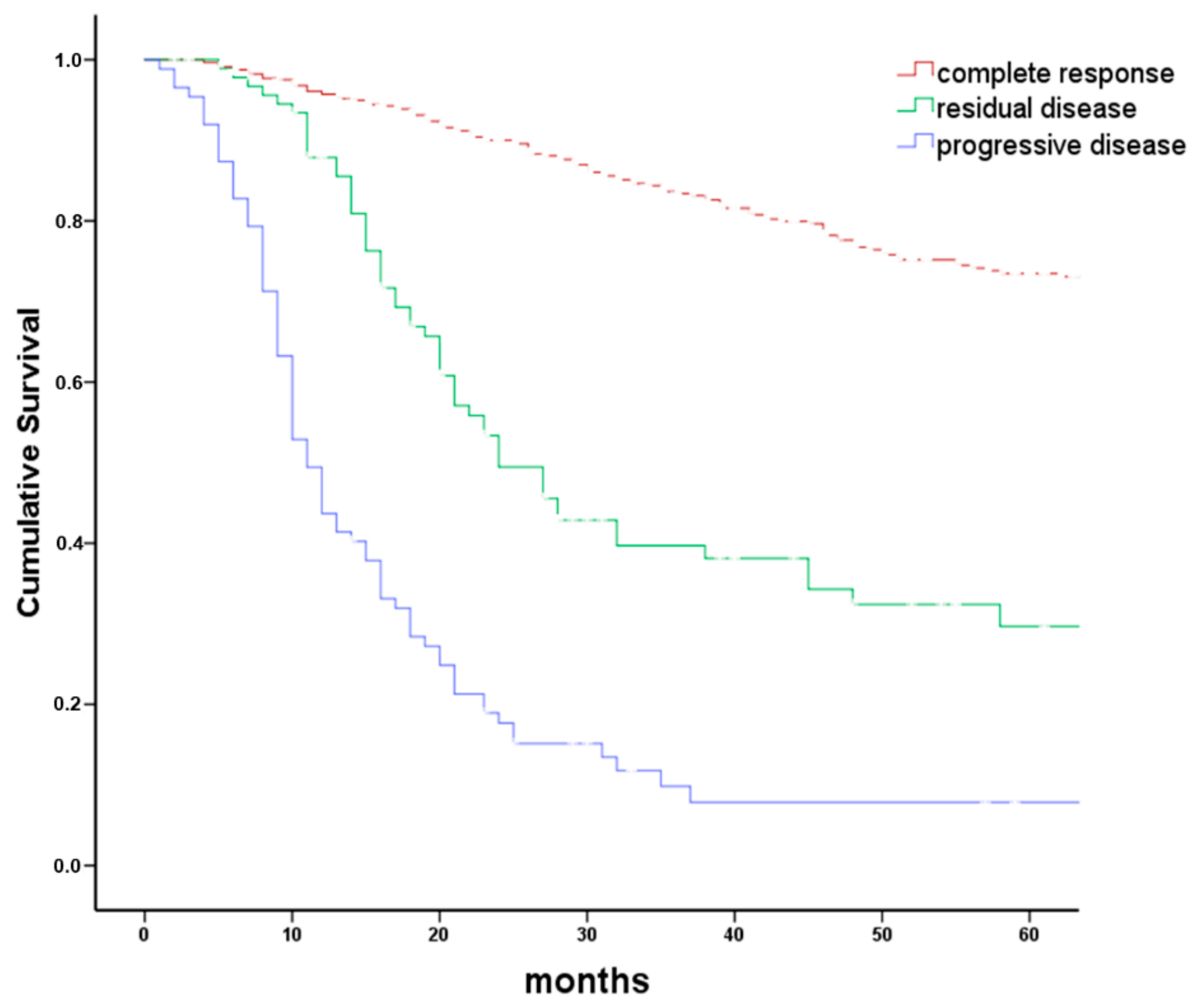
2.2. Characteristics of Patients with Persistent HNC
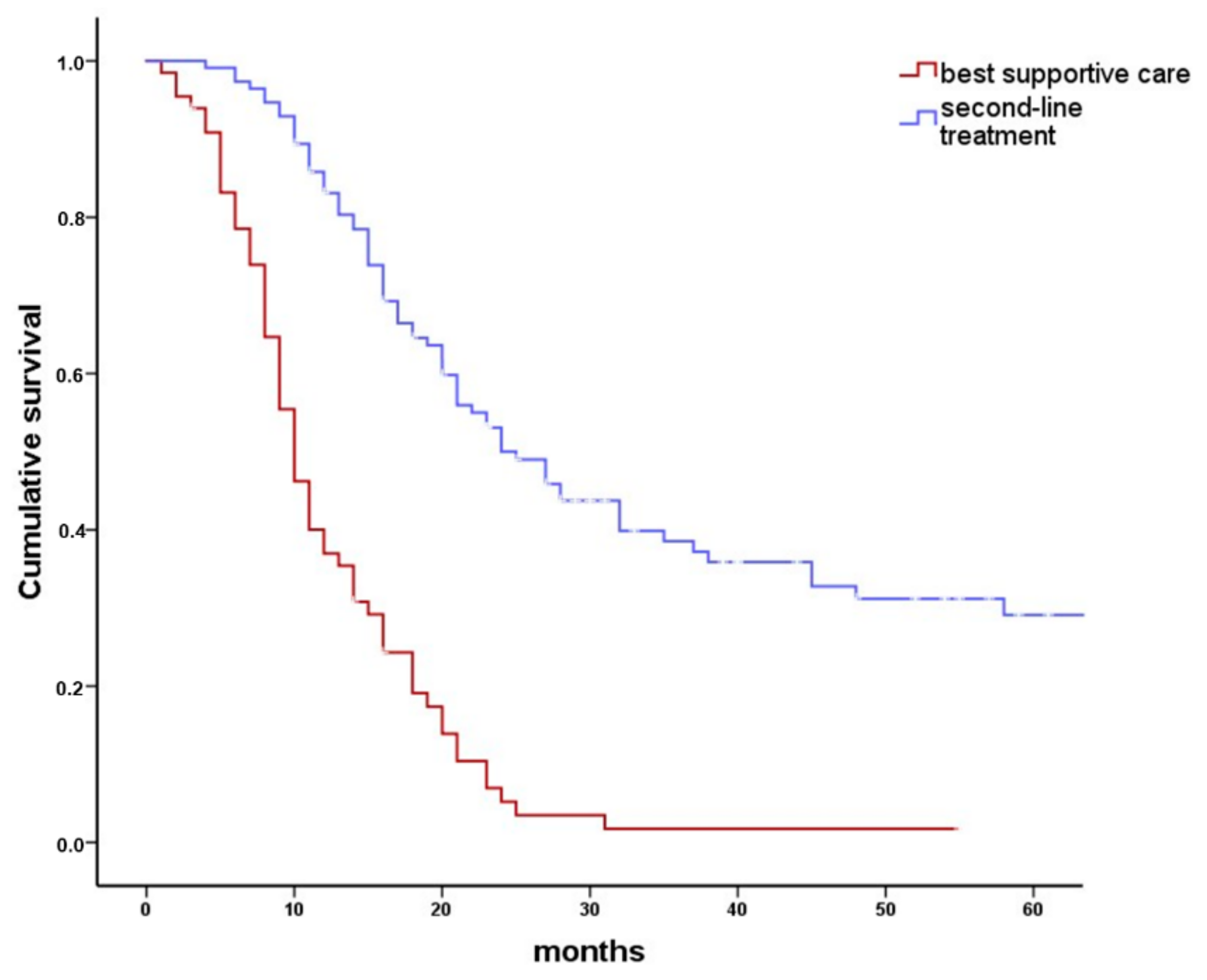
2.3. Best Supportive Care vs. Second-Line Treatment
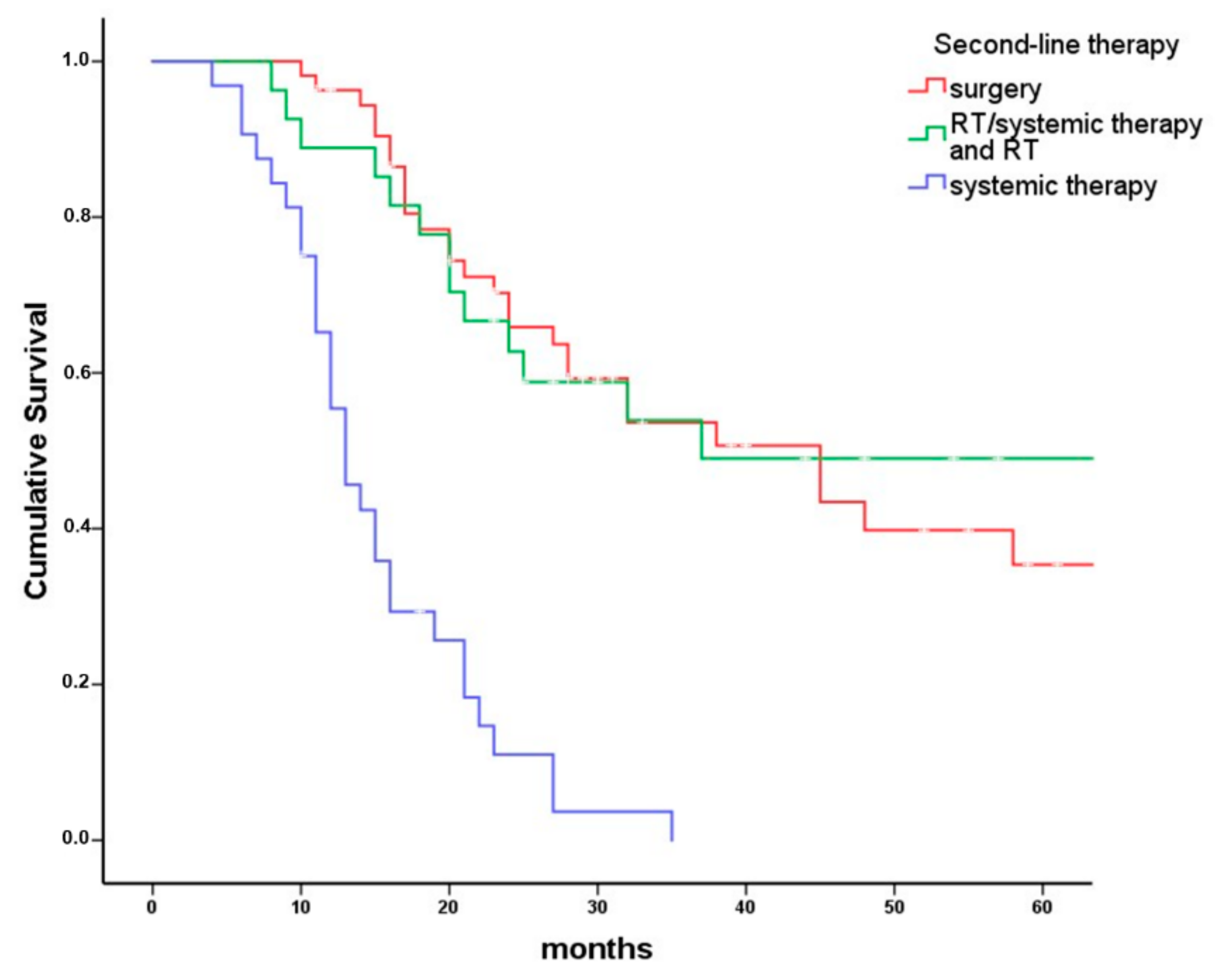
2.4. Second-Line Treatment Modalities
3. Discussion
3.1. Study Population
3.2. Second-Line Treatment vs. BSC
3.3. Second-Line Treatment
3.4. Influence of Second-Line Therapy Modality on Overall Survival
4. Materials and Methods
4.1. Clinical Tumor Registry
4.2. Outcome of First-Line Treatment
4.3. Inclusion and Exclusion
4.4. Extent of Persistent Disease and Second-Line Treatment Protocols
4.5. Data Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Adelstein, D.; Gillison, M.L.; Pfister, D.G.; Spencer, S.; Adkins, D.; Brizel, D.M.; Burtness, B.; Busse, P.M.; Caudell, J.J.; Cmelak, A.J.; et al. NCCN Guidelines Insights: Head and Neck Cancers, Version 2.2017. J. Natl. Compr. Canc. Netw. 2017, 15, 761–770. [Google Scholar] [CrossRef] [PubMed]
- Friedman, M.; Pearlman, A.W. Carcinoma of the Cervix: Radiation Salvage of Surgical Failures. Radiology 1965, 84, 801–811. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.C.; Shores, C.G.; Weissler, M.C. Salvage surgery after failed primary concomitant chemoradiation. Curr. Opin. Otolaryngol. Head Neck Surg. 2008, 16, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Lango, M.N.; Myers, J.N.; Garden, A.S. Controversies in surgical management of the node-positive neck after chemoradiation. Semin. Radiat. Oncol. 2009, 19, 24–28. [Google Scholar] [CrossRef] [PubMed]
- Vermorken, J.B.; Mesia, R.; Rivera, F.; Remenar, E.; Kawecki, A.; Rottey, S.; Erfan, J.; Zabolotnyy, D.; Kienzer, H.R.; Cupissol, D.; et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N. Engl. J. Med. 2008, 359, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Hui, D.; De La Cruz, M.; Mori, M.; Parsons, H.A.; Kwon, J.H.; Torres-Vigil, I.; Kim, S.H.; Dev, R.; Hutchins, R.; Liem, C.; et al. Concepts and definitions for “supportive care,” “best supportive care,” “palliative care,” and “hospice care” in the published literature, dictionaries, and textbooks. Support. Care Cancer 2013, 21, 659–685. [Google Scholar] [CrossRef] [PubMed]
- Zenga, J.; Gross, J.; Fowler, S.; Chen, J.; Vila, P.; Richmon, J.D.; Varvares, M.A.; Pipkorn, P. Salvage of recurrence after surgery and adjuvant therapy: A. systematic review. Am. J. Otolaryngol. 2018, 39, 223–227. [Google Scholar] [CrossRef] [PubMed]
- Moskovitz, J.; Moy, J.; Ferris, R.L. Immunotherapy for Head and Neck Squamous Cell Carcinoma. Curr. Oncol. Rep. 2018, 20, 22. [Google Scholar] [CrossRef] [PubMed]
- Colevas, A.D.; Yom, S.S.; Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Brizel, D.M.; Burtness, B.; Busse, P.M.; Caudell, J.J.; et al. NCCN Guidelines Insights: Head and Neck Cancers, Version 1.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.B.; Hoogstraten, B.; Staquet, M.; Winkler, A. Reporting results of cancer treatment. Cancer 1981, 47, 207–214. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Pagh, A.; Grau, C.; Overgaard, J. Failure pattern and salvage treatment after radical treatment of head and neck cancer. Acta. Oncol. 2016, 55, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Yovino, S.; Settle, K.; Taylor, R.; Wolf, J.; Kwok, Y.; Cullen, K.; Ord, R.; Zimrin, A.; Strome, S.; Suntharalingam, M. Patterns of failure among patients with squamous cell carcinoma of the head and neck who obtain a complete response to chemoradiotherapy. Head Neck 2010, 32, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Kostrzewa, J.P.; Lancaster, W.P.; Iseli, T.A.; Desmond, R.A.; Carroll, W.R.; Rosenthal, E.L. Outcomes of salvage surgery with free flap reconstruction for recurrent oral and oropharyngeal cancer. Laryngoscope 2010, 120, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Roosli, C.; Studer, G.; Stoeckli, S.J. Salvage treatment for recurrent oropharyngeal squamous cell carcinoma. Head Neck 2010, 32, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.J.; Mehta, R.H.; Wenig, B.L.; Shaligram, C.; Portugal, L.G. Salvage treatment for recurrent squamous cell carcinoma of the oral cavity. Head Neck 2000, 22, 34–41. [Google Scholar] [CrossRef]
- Ho, A.S.; Kraus, D.H.; Ganly, I.; Lee, N.Y.; Shah, J.P.; Morris, L.G. Decision making in the management of recurrent head and neck cancer. Head Neck 2014, 36, 144–151. [Google Scholar] [CrossRef] [PubMed]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab for Recurrent Squamous-Cell Carcinoma of the Head and Neck. N. Engl. J. Med. 2016, 375, 1856–1867. [Google Scholar] [CrossRef] [PubMed]
- Goodwin, W.J., Jr. Salvage surgery for patients with recurrent squamous cell carcinoma of the upper aerodigestive tract: When do the ends justify the means? Laryngoscope 2000, 110, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Ricco, A.; Davis, J.; Rate, W.; Yang, J.; Perry, D.; Pablo, J.; D’Ambrosio, D.; Sharma, S.; Sundararaman, S.; Kolker, J.; et al. Lung metastases treated with stereotactic body radiotherapy: The RSSearch(R) patient Registry’s experience. Radiat. Oncol. 2017, 12, 35. [Google Scholar] [CrossRef] [PubMed]
- Janot, F.; de Raucourt, D.; Benhamou, E.; Ferron, C.; Dolivet, G.; Bensadoun, R.J.; Hamoir, M.; Géry, B.; Julieron, M.; Castaing, M.; et al. Randomized trial of postoperative reirradiation combined with chemotherapy after salvage surgery compared with salvage surgery alone in head and neck carcinoma. J. Clin. Oncol. 2008, 26, 5518–5523. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.; Chan, K.; Bekelman, J.E.; Zhung, J.; Mechalakos, J.; Narayana, A.; Wolden, S.; Venkatraman, E.S.; Pfister, D.; Kraus, D.; et al. Salvage re-irradiation for recurrent head and neck cancer. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.J.; Lee, S.H.; Baek, S.H.; Bae, W.J.; Chang, Y.J.; Rho, Y.S. Clinical outcome and prognostic factors after salvage surgery for isolated regional squamous cell carcinoma recurrences. Head Neck 2015, 37, 1612–1617. [Google Scholar] [CrossRef] [PubMed]
- Holsinger, F.C.; Funk, E.; Roberts, D.B.; Diaz, E.M., Jr. Conservation laryngeal surgery versus total laryngectomy for radiation failure in laryngeal cancer. Head Neck 2006, 28, 779–784. [Google Scholar] [CrossRef] [PubMed]
- Kim, A.J.; Suh, J.D.; Sercarz, J.A.; Abemayor, E.; Head, C.; Funk, G.; Blackwell, K.E. Salvage surgery with free flap reconstruction: Factors affecting outcome after treatment of recurrent head and neck squamous carcinoma. Laryngoscope 2007, 117, 1019–1023. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Kim, J.S.; Yi, J.S.; Lee, J.H.; Choi, S.H.; Nam, S.Y.; Cho, K.J.; Lee, S.W.; Kim, S.B.; Roh, J.L. Evaluation of 18F-FDG PET/CT and CT/MRI with histopathologic correlation in patients undergoing salvage surgery for head and neck squamous cell carcinoma. Ann. Surg. Oncol. 2011, 18, 2579–2584. [Google Scholar] [CrossRef] [PubMed]
- Mak, P.H.; Campbell, R.C.; Irwin, M.G. American Society of A. The ASA Physical Status Classification: Inter-observer consistency. Anaesth Intensive Care 2002, 30, 633–640. [Google Scholar] [PubMed]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C. TNM Classification of Malignant Tumours, 7th ed.; UICC: Oxford, UK, 2011; pp. 22–63. ISBN 978-1-4443-3241-4. [Google Scholar]
- Kofler, B.; Borena, W.; Manzl, C.; Dudas, J.; Wegscheider, A.S.; Jansen-Durr, P.; Schartinger, V.; Riechelmann, H. Sensitivity of tumor surface brushings to detect human papilloma virus DNA in head and neck cancer. Oral. Oncol. 2017, 67, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Reimers, N.; Kasper, H.U.; Weissenborn, S.J.; Stutzer, H.; Preuss, S.F.; Hoffmann, T.K.; Speel, E.J.; Dienes, H.P.; Pfister, H.J.; Guntinas-Lichius, O. Combined analysis of HPV-DNA, p16 and EGFR expression to predict prognosis in oropharyngeal cancer. Int. J. Cancer 2007, 120, 1731–1738. [Google Scholar] [CrossRef] [PubMed]
- Jack, B.; Boland, A.; Dickson, R.; Stevenson, J.; McLeod, C. Best supportive care in lung cancer trials is inadequately described: A. systematic review. Eur. J. Cancer Care 2010, 19, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Sepulveda, C.; Marlin, A.; Yoshida, T.; Ullrich, A. Palliative Care: The World Health Organization’s global perspective. J. Pain Symptom Manag. 2002, 24, 91–96. [Google Scholar] [CrossRef]
- Kang, M.H.; Kang, J.H.; Song, H.N.; Jeong, B.K.; Chai, G.Y.; Kang, K.; Woo, S.H.; Park, J.J.; Kim, J.P. Concurrent Chemoradiation with Low-Dose Weekly Cisplatin in Locally Advanced Stage IV Head and Neck Squamous Cell Carcinoma. Cancer Res. Treat. 2015, 47, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Cohen, R.B.; Jones, C.U.; Sur, R.K.; Raben, D.; Baselga, J.; Spencer, S.A.; Zhu, J.; et al. Radiotherapy plus cetuximab for locoregionally advanced head and neck cancer: 5-year survival data from a phase 3 randomised trial, and relation between cetuximab-induced rash and survival. Lancet Oncol. 2010, 11, 21–28. [Google Scholar] [CrossRef]
- Budach, V.; Stromberger, C.; Poettgen, C.; Baumann, M.; Budach, W.; Grabenbauer, G.; Marnitz, S.; Olze, H.; Wernecke, K.D.; Ghadjar, P. Hyperfractionated accelerated radiation therapy (HART) of 70.6 Gy with concurrent 5-FU/Mitomycin C is superior to HART of 77.6 Gy alone in locally advanced head and neck cancer: Long-term results of the ARO 95-06 randomized phase III trial. Int. J. Radiat. Oncol. Biol. Phys. 2015, 91, 916–924. [Google Scholar] [CrossRef] [PubMed]
- Colevas, A.D. Chemotherapy options for patients with metastatic or recurrent squamous cell carcinoma of the head and neck. J. Clin. Oncol. 2006, 24, 2644–2652. [Google Scholar] [CrossRef] [PubMed]
- Schemper, M.; Smith, T.L. A note on quantifying follow-up in studies of failure time. Control Clin. Trials 1996, 17, 343–346. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value | Count | Percent |
|---|---|---|---|
| Sex | Male | 133 | 76% |
| Female | 42 | 24% | |
| Age at diagnosis | ≤50 | 25 | 14% |
| 51–60 | 51 | 29% | |
| 61–70 | 52 | 30% | |
| 71–80 | 30 | 17% | |
| >80 | 17 | 10% | |
| ASA I/II vs. ASA III/IV | ASA I/II | 40 | 37% |
| ASA III/IV | 68 | 63% | |
| Common tumor sites | Lip/oral cavity | 32 | 18% |
| Oropharynx | 53 | 30% | |
| Hypopharynx | 23 | 13% | |
| Larynx | 34 | 19% | |
| Other | 33 | 19% | |
| Clinical stage | Stage 1 | 9 | 5% |
| Stage 2 | 12 | 7% | |
| Stage 3 | 18 | 10% | |
| Stage 4a | 105 | 60% | |
| Stage 4b | 18 | 10% | |
| Stage 4c | 13 | 7% | |
| p16-IHC | Negative | 90 | 80% |
| Positive | 22 | 20% | |
| First-line treatment | Surgery only | 23 | 13% |
| Surgery and postoperative radiotherapy | 15 | 9% | |
| Surgery and systemic therapy/radiotherapy | 20 | 11% | |
| Systemic therapy/radiotherapy | 73 | 42% | |
| Chemotherapy | 11 | 6% | |
| Radiotherapy | 26 | 15% | |
| Radioimmunotherapy | 7 | 4% | |
| First-line treatment adherence | Treated as planned | 140 | 80% |
| Discontinued | 19 | 11% | |
| Treatment modified | 16 | 9% |
| RD/PD | Site of Persistence | Total | ||||
|---|---|---|---|---|---|---|
| Primary Site | Primary Site and Neck | Neck Only | Distant Only | Distant and Primary Site and/or Neck | ||
| Residual disease | 44 | 10 | 28 | 3 | 5 | 90 |
| Progression | 30 | 5 | 4 | 20 | 26 | 85 |
| Total | 74 | 15 | 32 | 23 | 31 | 175 |
| Variable | Value | Second-line | BSC | Total | p-Value |
|---|---|---|---|---|---|
| Age at diagnosis | ≤50 | 20 (80%) | 5 (20%) | 25 | 0.001 |
| 51–60 | 38 (75%) | 13 (25%) | 51 | ||
| 61–70 | 33 (63%) | 19 (37%) | 52 | ||
| 71–80 | 17 (57%) | 13 (43%) | 30 | ||
| >80 | 4 (24%) | 13 (76%) | 17 | ||
| ASA I/II vs. ASA III/IV | ASA I/II | 34 (85%) | 6 (15%) | 40 | 0.004 |
| ASA III/IV | 40 (59%) | 28 (41%) | 68 | ||
| p16-IHC | Negative | 58 (64%) | 32 (36%) | 90 | 0.047 |
| Positive | 19 (86%) | 3 (14%) | 22 | ||
| First-line treatment | Surgery only | 19 (83%) | 4 (17%) | 23 | <0.001 |
| Surgery and PORT | 8 (53%) | 7 (47%) | 15 | ||
| Surgery and systemic therapy/RT | 13 (65%) | 7 (35%) | 20 | ||
| Systemic therapy/RT | 56 (77%) | 17 (23%) | 73 | ||
| Systemic therapy | 5 (45%) | 6 (55%) | 11 | ||
| Radiotherapy | 8 (31%) | 18 (69%) | 26 | ||
| Radioimmunotherapy | 3 (43%) | 4 (57%) | 7 | ||
| First-line treatment discontinuation | No | 100 (71%) | 40 (29%) | 140 | <0.001 |
| Discontinued | 4 (21%) | 15 (79%) | 19 | ||
| Treatment modified | 8 (50%) | 8 (50%) | 16 | ||
| RD/PD | Residual disease | 72 (80%) | 18 (20%) | 90 | <0.001 |
| Progression | 40 (47%) | 45 (53%) | 85 | ||
| Sites of persistence | Primary site | 39 (53%) | 35 (47%) | 74 | 0.002 |
| Primary site and neck | 12 (80%) | 3 (20%) | 15 | ||
| Neck only | 28 (88%) | 4 (13%) | 32 | ||
| Distant only | 17 (74%) | 6 (26%) | 23 | ||
| Distant and primary site and/or neck | 16 (52%) | 15 (48%) | 31 |
| Surgical Treatment (2) | RT/RCHT/RIT Without Surgery | Chemotherapy Only | Total (3) | |
|---|---|---|---|---|
| With CR | 41 | 14 | 1 | 56 |
| No CR | 12 | 11 | 20 | 43 |
| Death before end of treatment (1) | 0 | 2 | 10 | 12 |
| Total | 53 | 27 | 32 | 112 |
| Patient Factors | Regression Coefficient B | Wald | df | Sig. | Adjusted OR | 95% Confident Interval for OR | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | |||||||
| extent of persistence | extent of persistence | 1.26 | 4 | 0.87 | ||||
| local | 0.38 | 0.35 | 1 | 0.55 | 1.46 | 0.42 | 5.13 | |
| locoregional | −0.16 | 0.06 | 1 | 0.81 | 0.86 | 0.25 | 2.96 | |
| regional | −0.02 | 0.00 | 1 | 0.99 | 0.99 | 0.23 | 4.27 | |
| distant | 0.153 | 0.06 | 1 | 0.80 | 1.17 | 0.36 | 3.82 | |
| locoregional and distant * | 0.00 | 1.00 | ||||||
| residual vs. progressive disease | residual disease | 0.16 | 0.15 | 1 | 0.7 | 1.18 | 0.51 | 2.68 |
| progressive disease * | 0.00 | 1.00 | ||||||
| UICC stage | UICC Stage | 2.61 | 3 | 0.46 | ||||
| I | −1.01 | 0.85 | 1 | 0.36 | 0.37 | 0.043 | 3.12 | |
| II | −0.91 | 1.12 | 1 | 0.29 | 0.40 | 0.08 | 2.17 | |
| III | −1.08 | 1.98 | 1 | 0.16 | 0.34 | 0.08 | 1.53 | |
| IV * | 0.00 | 1.00 | ||||||
| initial tumor site | tumor site | 2.66 | 4 | 0.62 | ||||
| lips/oral cavity | −0.19 | 0.06 | 1 | 0.82 | 0.82 | 0.16 | 4.33 | |
| oropharynx | −0.53 | 0.57 | 1 | 0.45 | 0.59 | 0.15 | 2.33 | |
| hypopharynx | 0.10 | 0.02 | 1 | 0.90 | 1.10 | 0.23 | 5.26 | |
| larynx | −0.22 | 0.07 | 1 | 0.79 | 1.24 | 0.25 | 6.2 | |
| Other * | 0.00 | 1.00 | ||||||
| second-line treatment modality | 9.57 | 2 | 0.01 | |||||
| surgery | −1.75 | 9.43 | 1 | 0.002 | 0.17 | 0.06 | 0.53 | |
| RT/RCHT | −1.13 | 3.24 | 1 | 0.07 | 0.32 | 0.09 | 1.11 | |
| CHT * | 0.00 | 1.00 | ||||||
| age | age | 5.23 | 4 | 0.26 | ||||
| ≤50 | −2.27 | 2.82 | 1 | 0.09 | 0.10 | 0.01 | 1.47 | |
| 51–60 | −2.78 | 4.55 | 1 | 0.03 | 0.06 | 0.05 | 0.80 | |
| 61–70 | −2.38 | 3.26 | 1 | 0.07 | 0.09 | 0.01 | 1.23 | |
| 71–80 | −2.54 | 3.31 | 1 | 0.07 | 0.08 | 0.01 | 1.22 | |
| >80 * | 0.00 | 1.00 | ||||||
| ASA score | I/II | −0.9 | 5.88 | 1 | 0.02 | 0.4 | 0.20 | 0.84 |
| III/IV * | 0.00 | 1.00 | ||||||
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Steinbichler, T.B.; Lichtenecker, M.; Anegg, M.; Dejaco, D.; Kofler, B.; Schartinger, V.H.; Kasseroler, M.-T.; Forthuber, B.; Posch, A.; Riechelmann, H. Persistent Head and Neck Cancer Following First-Line Treatment. Cancers 2018, 10, 421. https://doi.org/10.3390/cancers10110421
Steinbichler TB, Lichtenecker M, Anegg M, Dejaco D, Kofler B, Schartinger VH, Kasseroler M-T, Forthuber B, Posch A, Riechelmann H. Persistent Head and Neck Cancer Following First-Line Treatment. Cancers. 2018; 10(11):421. https://doi.org/10.3390/cancers10110421
Chicago/Turabian StyleSteinbichler, Teresa Bernadette, Madeleine Lichtenecker, Maria Anegg, Daniel Dejaco, Barbara Kofler, Volker Hans Schartinger, Maria-Therese Kasseroler, Britta Forthuber, Andrea Posch, and Herbert Riechelmann. 2018. "Persistent Head and Neck Cancer Following First-Line Treatment" Cancers 10, no. 11: 421. https://doi.org/10.3390/cancers10110421
APA StyleSteinbichler, T. B., Lichtenecker, M., Anegg, M., Dejaco, D., Kofler, B., Schartinger, V. H., Kasseroler, M.-T., Forthuber, B., Posch, A., & Riechelmann, H. (2018). Persistent Head and Neck Cancer Following First-Line Treatment. Cancers, 10(11), 421. https://doi.org/10.3390/cancers10110421