A Recurrent BRCA2 Mutation Explains the Majority of Hereditary Breast and Ovarian Cancer Syndrome Cases in Puerto Rico


 , ,
, ,  and
and
Abstract
1. Introduction
2. Results
2.1. Characteristics of the Study Population
2.2. BRCA1 Variants
2.3. BRCA2 Variants
2.4. Prediction of Functionality of Missense Variants of Uncertain Significance
2.5. BRCA Mutation Prevalence and Clinical Characteristics of the Carriers
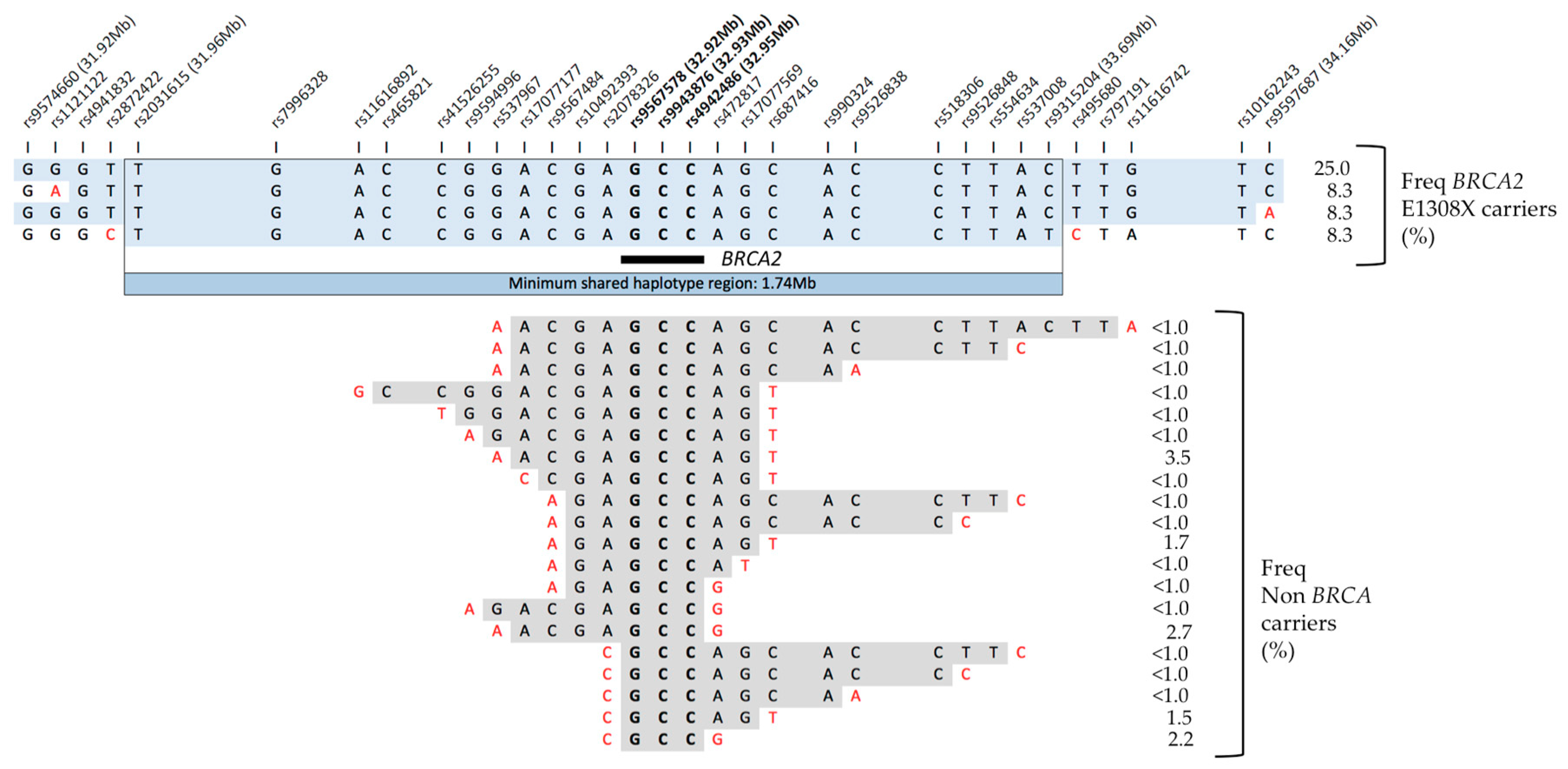
2.6. Genomic Context in BRCA2 E1308X Carriers
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Sample Preparation and BRCA1/2 Sequencing
4.3. Variant, Filtering and Annotation
4.4. Ancestry Analyses
4.5. Haplotype Analysis
4.6. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Miki, Y.; Swensen, J.; Shattuck-Eidens, D.; Futreal, P.A.; Harshman, K.; Tavtigian, S.; Liu, Q.; Cochran, C.; Bennett, L.M.; Ding, W.; et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 1994, 266, 66–71. [Google Scholar] [CrossRef] [PubMed]
- Wooster, R.; Bignell, G.; Lancaster, J.; Swift, S.; Seal, S.; Mangion, J.; Collins, N.; Gregory, S.; Gumbs, C.; Micklem, G.; et al. Identification of the breast cancer susceptibility gene BRCA2. Nature 1995, 378, 789–792. [Google Scholar] [CrossRef] [PubMed]
- Warner, E.; Plewes, D.B.; Hill, K.A.; Causer, P.A.; Zubovits, J.T.; Jong, R.A.; Cutrara, M.R.; DeBoer, G.; Yaffe, M.J.; Messner, S.J.; et al. Surveillance of BRCA1 and BRCA2 mutation carriers with magnetic resonance imaging, ultrasound, mammography, and clinical breast examination. JAMA 2004, 292, 1317–1325. [Google Scholar] [CrossRef] [PubMed]
- King, M.C.; Wieand, S.; Hale, K.; Lee, M.; Walsh, T.; Owens, K.; Tait, J.; Ford, L.; Dunn, B.K.; Costantino, J.; et al. Tamoxifen and breast cancer incidence among women with inherited mutations in BRCA1 and BRCA2: National Surgical Adjuvant Breast and Bowel Project (NSABP-P1) Breast Cancer Prevention Trial. JAMA 2001, 286, 2251–2256. [Google Scholar] [CrossRef] [PubMed]
- Vogel, V.G.; Costantino, J.P.; Wickerham, D.L.; Cronin, W.M.; Cecchini, R.S.; Atkins, J.N.; Bevers, T.B.; Fehrenbacher, L.; Pajon, E.R.; Wade, J.L., 3rd; et al. Update of the National Surgical Adjuvant Breast and Bowel Project Study of Tamoxifen and Raloxifene (STAR) P-2 Trial: Preventing breast cancer. Cancer Prev. Res. 2010, 3, 696–706. [Google Scholar] [CrossRef] [PubMed]
- Rebbeck, T.R.; Friebel, T.; Lynch, H.T.; Neuhausen, S.L.; van’t Veer, L.; Garber, J.E.; Evans, G.R.; Narod, S.A.; Isaacs, C.; Matloff, E.; et al. Bilateral prophylactic mastectomy reduces breast cancer risk in BRCA1 and BRCA2 mutation carriers: The PROSE Study Group. J. Clin. Oncol. 2004, 22, 1055–1062. [Google Scholar] [CrossRef] [PubMed]
- Domchek, S.M.; Friebel, T.M.; Singer, C.F.; Evans, D.G.; Lynch, H.T.; Isaacs, C.; Garber, J.E.; Neuhausen, S.L.; Matloff, E.; Eeles, R.; et al. Association of risk-reducing surgery in BRCA1 or BRCA2 mutation carriers with cancer risk and mortality. JAMA 2010, 304, 967–975. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.D.; Lerman, C.; Brogan, B.; Peshkin, B.N.; Halbert, C.H.; DeMarco, T.; Lawrence, W.; Main, D.; Finch, C.; Magnant, C.; et al. Impact of BRCA1/BRCA2 counseling and testing on newly diagnosed breast cancer patients. J. Clin. Oncol. 2004, 22, 1823–1829. [Google Scholar] [CrossRef] [PubMed]
- Weitzel, J.N.; McCaffrey, S.M.; Nedelcu, R.; MacDonald, D.J.; Blazer, K.R.; Cullinane, C.A. Effect of genetic cancer risk assessment on surgical decisions at breast cancer diagnosis. Arch. Surg. 2003, 138, 1323–1328. [Google Scholar] [CrossRef] [PubMed]
- Cortesi, L.; Razzaboni, E.; Toss, A.; De Matteis, E.; Marchi, I.; Medici, V.; Tazzioli, G.; Andreotti, A.; De Santis, G.; Pignatti, M.; et al. A rapid genetic counselling and testing in newly diagnosed breast cancer is associated with high rate of risk-reducing mastectomy in BRCA1/2-positive Italian women. Ann. Oncol. 2014, 25, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Galanter, J.M.; Fernandez-Lopez, J.C.; Gignoux, C.R.; Barnholtz-Sloan, J.; Fernandez-Rozadilla, C.; Via, M.; Hidalgo-Miranda, A.; Contreras, A.V.; Figueroa, L.U.; Raska, P.; et al. Development of a panel of genome-wide ancestry informative markers to study admixture throughout the Americas. PLoS Genet. 2012, 8, e1002554. [Google Scholar] [CrossRef] [PubMed]
- Dutil, J.; Golubeva, V.A.; Pacheco-Torres, A.L.; Diaz-Zabala, H.J.; Matta, J.L.; Monteiro, A.N. The spectrum of BRCA1 and BRCA2 alleles in Latin America and the Caribbean: A clinical perspective. Breast Cancer Res. Treat. 2015, 154, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Dutil, J.; Colon-Colon, J.L.; Matta, J.L.; Sutphen, R.; Echenique, M. Identification of the prevalent BRCA1 and BRCA2 mutations in the female population of Puerto Rico. Cancer Genet. 2012, 205, 242–248. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Genetic/Familial High-Risk Assessment: Breast and Ovarian. Version 2. 2017. Available online: http://www.nccn.org/ (accessed on 10 August 2017).
- Landrum, M.J.; Lee, J.M.; Benson, M.; Brown, G.; Chao, C.; Chitipiralla, S.; Gu, B.; Hart, J.; Hoffman, D.; Hoover, J.; et al. ClinVar: Public archive of interpretations of clinically relevant variants. Nucleic Acids Res. 2016, 44, D862–D868. [Google Scholar] [CrossRef] [PubMed]
- Lek, M.; Karczewski, K.J.; Minikel, E.V.; Samocha, K.E.; Banks, E.; Fennell, T.; O’Donnell-Luria, A.H.; Ware, J.S.; Hill, A.J.; Cummings, B.B.; et al. Exome Aggregation Consortium. Analysis of protein-coding genetic variation in 60,706 humans. Nature 2016, 536, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Tavtigian, S.V.; Deffenbaugh, A.M.; Yin, L.; Judkins, T.; Scholl, T.; Samollow, P.B.; de Silva, D.; Zharkikh, A.; Thomas, A. Comprehensive statistical study of 452 BRCA1 missense substitutions with classification of eight recurrent substitutions as neutral. J. Med. Genet. 2006, 43, 295–305. [Google Scholar] [CrossRef] [PubMed]
- Huntsman Cancer Institute (HCI). Breast Cancer Genes Prior Probabilities. Available online: http://priors.hci.utah.edu/PRIORS/index.php/ (accessed on 20 June 2017).
- Adzhubei, I.A.; Schmidt, S.; Peshkin, L.; Ramensky, V.E.; Gerasimova, A.; Bork, P.; Kondrashov, A.S.; Sunyaev, S.R. A method and server for predicting damaging missense mutations. Nat. Methods 2010, 7, 248–249. [Google Scholar] [CrossRef] [PubMed]
- Sim, N.L.; Kumar, P.; Hu, J.; Henikoff, S.; Schneider, G.; Ng, P.C. SIFT web server: Predicting effects of amino acid substitutions on proteins. Nucleic Acids Res. 2012, 40, W452–W457. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Sims, G.E.; Murphy, S.; Miller, J.R.; Chan, A.P. Predicting the functional effect of amino acid substitutions and indels. PLoS ONE 2012, 7, e46688. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.; Chan, A.P. PROVEAN web server: A tool to predict the functional effect of amino acid substitutions and indels. Bioinformatics 2015, 31, 2745–2747. [Google Scholar] [CrossRef] [PubMed]
- Via, M.; Gignoux, C.R.; Roth, L.A.; Fejerman, L.; Galanter, J.; Choudhry, S.; Toro-Labrador, G.; Viera-Vera, J.; Oleksyk, T.K.; Beckman, K.; et al. History shaped the geographic distribution of genomic admixture on the island of Puerto Rico. PLoS ONE 2011, 6, e16513. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Zabala, H.J.; Nieves-Colón, M.A.; Martínez-Cruzado, J.C. A Mainly Circum-Mediterranean Origin for West Eurasian and North African mtDNAs in Puerto Rico with Strong Contributions from the Canary Islands and West Africa. Hum. Biol. 2017, 89, 125–155. [Google Scholar] [CrossRef] [PubMed]
- Duran, M.; Esteban-Cardeñosa, E.; Velasco, E.; Infante, M.; Miner, C. Mutational analysis of BRCA2 in Spanish breast cancer patients from Castilla-Leon: Identification of four novel truncating mutations. Hum. Mutat. 2003, 21, 448. [Google Scholar] [CrossRef] [PubMed]
- Díez, O.; Osorio, A.; Durán, M.; Martinez-Ferrandis, J.I.; de la Hoya, M.; Salazar, R.; Vega, A.; Campos, B.; Rodríguez-López, R.; Velasco, E.; et al. Analysis of BRCA1 and BRCA2 genes in Spanish breast/ovarian cancer patients: A high proportion of mutations unique to Spain and evidence of founder effects. Hum. Mutat. 2003, 22, 301–312. [Google Scholar] [CrossRef] [PubMed]
- Dean, M.; Boland, J.; Yeager, M.; Im, K.M.; Garland, L.; Rodriguez-Herrera, M.; Perez, M.; Mitchell, J.; Roberson, D.; Jones, K.; et al. Addressing health disparities in Hispanic breast cancer: Accurate and inexpensive sequencing of BRCA1 and BRCA2. Gigascience 2015, 4, 50. [Google Scholar] [CrossRef] [PubMed]
- Vogel, K.J.; Atchley, D.P.; Erlichman, J.; Broglio, K.R.; Ready, K.J.; Valero, V.; Amos, C.I.; Hortobagyi, G.N.; Lu, K.H.; Arun, B. BRCA1 and BRCA2 genetic testing in Hispanic patients: Mutation prevalence and evaluation of the BRCAPRO risk assessment model. J. Clin. Oncol. 2007, 25, 4635–4661. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.J.; Reid, J.E.; Burbidge, L.A.; Pruss, D.; Deffenbaugh, A.M.; Frye, C.; Wenstrup, R.J.; Ward, B.E.; Scholl, T.A.; Noll, W.W. BRCA1 and BRCA2 mutations in women of different ethnicities undergoing testing for hereditary breast-ovarian cancer. Cancer 2009, 115, 2222–2233. [Google Scholar] [CrossRef] [PubMed]
- Frank, T.S.; Deffenbaugh, A.M.; Reid, J.E.; Hulick, M.; Ward, B.E.; Lingenfelter, B.; Gumpper, K.L.; Scholl, T.; Tavtigian, S.V.; Pruss, D.R.; et al. Clinical characteristics of individuals with germline mutations in BRCA1 and BRCA2: Analysis of 10,000 individuals. J. Clin. Oncol. 2002, 20, 1480–1490. [Google Scholar] [CrossRef] [PubMed]
- Solano, A.R.; Aceto, G.M.; Delettieres, D.; Veschi, S.; Neuman, M.I.; Alonso, E.; Chialina, S.; Chacón, R.D.; Renato, M.C.; Podestá, E.J. BRCA1 and BRCA2 analysis of Argentinean breast/ovarian cancer patients selected for age and family history highlights a role for novel mutations of putative south-American origin. SpringerPlus 2012, 1, 20. [Google Scholar] [CrossRef] [PubMed]
- Vaca-Paniagua, F.; Alvarez-Gomez, R.M.; Fragoso-Ontiveros, V.; Vidal-Millan, S.; Herrera, L.A.; Cantú, D.; Bargallo-Rocha, E.; Mohar, A.; López-Camarillo, C.; Pérez-Plasencia, C. Full-exon pyrosequencing screening of BRCA germline mutations in Mexican women with inherited breast and ovarian cancer. PLoS ONE 2012, 7, e37432. [Google Scholar] [CrossRef] [PubMed]
- Torres, D.; Rashid, M.U.; Gil, F.; Umana, A.; Ramelli, G.; Robledo, J.F.; Tawil, M.; Torregrosa, L.; Briceno, I.; Hamann, U. High proportion of BRCA1/2 founder mutations in Hispanic breast/ovarian cancer families from Colombia. Breast Cancer Res. Treat. 2007, 103, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.C.; Costa, M.M.; Borojevic, R.; Monteiro, A.N.; Vieira, R.; Koifman, S.; Koifman, R.J.; Li, S.; Royer, R.; Zhang, S.; et al. Prevalence of BRCA1 and BRCA2 mutations in breast cancer patients from Brazil. Breast Cancer Res. Treat. 2007, 103, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Peixoto, A.; Santos, C.; Pinheiro, M.; Pinto, P.; Soares, M.J.; Rocha, P.; Gusmão, L.; Amorim, A.; van der Hout, A.; Gerdes, A.M.; et al. International distribution and age estimation of the Portuguese BRCA2 c.156_157insAlu founder mutation. Breast Cancer Res. Treat. 2011, 127, 671–679. [Google Scholar] [CrossRef] [PubMed]
- Weitzel, J.N.; Clague, J.; Martir-Negron, A.; Ogaz, R.; Herzog, J.; Ricker, C.; Jungbluth, C.; Cina, C.; Duncan, P.; Unzeitig, G.; et al. Prevalence and type of BRCA mutations in Hispanics undergoing genetic cancer risk assessment in the southwestern United States: A report from the Clinical Cancer Genetics Community Research Network. J. Clin. Oncol. 2013, 31, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Hart, S.N.; Hoskin, T.; Shimelis, H.; Moore, R.M.; Feng, B.; Thomas, A.; Lindor, N.M.; Polley, E.C.; Goldgar, D.E.; Iversen, E.; et al. Comprehensive annotation of BRCA1 and BRCA2 missense variants by functionally validated sequence-based computational prediction models. Genet. Med. 2018. [Google Scholar] [CrossRef] [PubMed]
- Lindor, N.M.; Goldgar, D.E.; Tavtigian, S.V.; Plon, S.E.; Couch, F.J. BRCA1/2 sequence variants of uncertain significance: A primer for providers to assist in discussions and in medical management. Oncologist 2013, 18, 518–524. [Google Scholar] [CrossRef] [PubMed]
- U.S. Preventive Task Force. Risk Assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: Recommendation statement. Am. Fam. Phys. 2015, 91. Available online: https://www.aafp.org/afp/2015/0115/od1.html/ (accessed on 8 August 2018).
- Dutil, J.; Godoy, L.; Rivera-Lugo, R.; Arroyo, N.; Albino, E.; Negrón, L.; Monteiro, A.N.; Matta, J.L.; Echenique, M. No Evidence for the pathogenicity of the BRCA2 c.6937 + 594T>G deep intronic variant: A case-control analysis. Genet. Test. Mol. Biomark. 2018, 22, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.; Casadei, S.; Lee, M.K.; Pennil, C.C.; Nord, A.S.; Thornton, A.M.; Roeb, W.; Agnew, K.J.; Stray, S.M.; Wickramanayake, A.; et al. Mutations in 12 genes for inherited ovarian, fallopian tube, and peritoneal carcinoma identified by massively parallel sequencing. Proc. Natl. Acad. Sci. USA 2011, 108, 18032–18037. [Google Scholar] [CrossRef] [PubMed]
- Easton, D.F.; Pharoah, P.D.P.; Antoniou, A.C.; Tischkowitz, M.; Tavtigian, S.V.; Nathanson, K.L.; Devilee, P.; Meindl, A.; Couch, F.J.; Southey, M.; et al. Gene-panel sequencing and the prediction of breast cancer risk. N. Engl. J. Med. 2015, 372, 2243–2257. [Google Scholar] [CrossRef] [PubMed]
- Wacholder, S.; Hartge, P.; Prentice, R.; Garcia-Closas, M.; Feigelson, H.S.; Diver, W.R.; Thun, M.J.; Cox, D.G.; Hankinson, S.E.; Kraft, P.; et al. Performance of common genetic variants in breast-cancer risk models. N. Engl. J. Med. 2010, 362, 986–993. [Google Scholar] [CrossRef] [PubMed]
- Dutil, J.; Teer, J.K.; Golubeva, V.; Yoder, S.; Tong, W.L.; Arroyo, N.; Echenique, M.; Matta, J.L.; Monterio, A.N. Germline vaiants in cancer genes in high-risk non-BRCA patients from Puerto Rico. In preparation.
- Matta, J.; Echenique, M.; Negron, E.; Morales, L.; Vargas, W.; Gaetan, F.S.; Lizardi, E.R.; Torres, A.; Rosado, J.O.; Bolaños, G.; et al. The association of DNA Repair with breast cancer risk in women. A comparative observational study. BMC Cancer 2012, 12, 490. [Google Scholar] [CrossRef] [PubMed]
- Thorvaldsdóttir, H.; Robinson, J.T.; Mesirov, J.P. Integrative Genomics Viewer (IGV): High-performance genomics data visualization and exploration. Brief. Bioinform. 2013, 14, 178–192. [Google Scholar] [CrossRef] [PubMed]
- Fejerman, L.; John, E.M.; Huntsman, S.; Beckman, K.; Choudhry, S.; Perez-Stable, E.; Burchard, E.G.; Ziv, E. Genetic ancestry and risk of breast cancer among U.S. Latinas. Cancer Res. 2008, 68, 9723–9728. [Google Scholar] [CrossRef] [PubMed]
- Alexander, D.H.; Novembre, J.; Lange, K. Fast model-based estimation of ancestry in unrelated individuals. Genome Res. 2009, 19, 1655–1664. [Google Scholar] [CrossRef] [PubMed]
- Delaneau, O.; Coulonges, C.; Zagury, J.-F. Shape-IT: New rapid and accurate algorithm for haplotype inference. BMC Bioinformat. 2008, 9, 540. [Google Scholar] [CrossRef] [PubMed]
- Maples, B.K.; Gravel, S.; Kenny, E.E.; Bustamante, C.D. RFMix: A discriminative modeling approach for rapid and robust local-ancestry inference. Am. J. Hum. Genet. 2013, 93, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Stephens, M.; Smith, N.J.; Donnelly, P. A new statistical method for haplotype reconstruction from population data. Am. J. Hum. Genet. 2001, 68, 978–989. [Google Scholar] [CrossRef] [PubMed]
- R Studio Team. RStudio: Integrated Development for R; RStudio, Inc.: Boston, MA, USA; Available online: http://www.rstudio.com/ (accessed on 10 August 2017).


{kind=link}
| Gene/Exon | AA | HGVS | No | dbSNP | ExAC Frequencies 3 | |||
|---|---|---|---|---|---|---|---|---|
| Change | Positions 1 | obs. 2 | Overall | Eur | Afr | Lat | ||
| BRCA1 | ||||||||
| Exon 6 | Stop 75 | c.213-11T>G (g.41256984A>C) | * | rs80358061 | 8.3 × 10−6 | 1.5 × 10−5 | 0 | 0 |
| Exon 20 | Stop 1829 | c.5263_5264insC (g.41209082_41209083insG) | * | rs80357906 | 1.6 × 10−4 | 2.8 × 10−4 | 0 | 0 |
| BRCA2 | ||||||||
| Exon 10 | Stop 599 | c.1794_1798delATTTT (g.32907409_32907413delATCTT) | 1 | NA | NA | NA | NA | NA |
| Exon 11 | E1308X | c.3922G>T (g.32912414G>T) | 8 | rs80358638 | NA | NA | NA | NA |
| Gene/Exon | AA | HGVS | No | dbSNP | ExAC Frequencies 3 | |||
|---|---|---|---|---|---|---|---|---|
| Change | Positions 1 | obs. 2 | Overall | Eur | Afr | Lat | ||
| BRCA1 | ||||||||
| Exon 11 | I571T | c.1712C>T (g.41245836A>G) | 3 | rs80357159 | 1.7 × 10−5 | 0 | 0 | 1.7 × 10−4 |
| Exon 11 | F1231L | c.3691T>C (g.41243857A>G) | 1 | rs41293451 | 3.3 × 10−5 | 0 | 3.8 × 10−4 | 0 |
| Exon 11 | I1275V | c.3823A>G (g.41243725T>C) | 1 | rs80357280 | 1.1 × 10−4 | 7.5 × 10−5 | 0 | 7.8 × 10−4 |
| Exon 13 | H1421R | c.4262A>G (g.41234516T>C) | 1 | rs80357079 | NA | NA | NA | NA |
| Exon 13 | H1421Y | c.4261C>T (g.41234517G>A) | 1 | rs80357013 | 1.6 × 10−5 | 0 | 9.6 × 10−5 | 8.6 × 10−5 |
| Exon 14 | E1470D | c.4410A>T (g.41228579T>A) | 4 | rs80357075 | 2.5 × 10−5 | 0 | 0 | 2.6 × 10−4 |
| BRCA2 | ||||||||
| Exon 10 | I283V | c.847A>G (g.32906462A>G) | 1 | rs80359097 | NA | NA | NA | NA |
| Exon 10 | I488V | c.1462A>G (g.32907077A>G) | 1 | NA | NA | NA | NA | NA |
| Exon 10 | Y600H | c.1798T>C (g.32907413T>C) | 1 | rs75419644 | 4.9 × 10−4 | 0 | 5.8 × 10−3 | 1.7 × 10−4 |
| Exon 11 | K1058R | c.3173A>G (g.32911665A>G) | 1 | rs431825302 | 1.7 × 10−5 | 0 | 0 | 1.7 × 10−4 |
| Exon 11 | D1923A | C.5768A>C (g.32914260A>C) | 1 | rs45491005 | 2.8 × 10−4 | 0 | 3.2 × 10−3 | 8.6 × 10−5 |
| Exon 11 | Q2159E | c.6475C>G (g.32914967C>G) | 2 | NA | NA | NA | NA | NA |
| Exon 22 | K2950N | c.8850G>T (g.32953549G>T) | 1 | rs28897754 | 6.8 × 10−4 | 8.1 × 10−4 | 9.8 × 10−5 | 1.8 × 10−3 |
| Exon 27 | P3292L | c.9875C>T (g.32972525C>T) | 1 | rs56121817 | 7.4 × 10−5 | 4.5 × 10−5 | 0 | 8.7 × 10−5 |
| Gene/Variant | ClinVar 1 | Align GVGD 2 | HCI Probability Pathogenicity | Polyphen 2 | SIFT 3 | Provean 4 | |
|---|---|---|---|---|---|---|---|
| Protein | de novo Donor Site | ||||||
| BRCA1 | |||||||
| I571T | VUS | C0 | Weak/Null | Weak/Null | Benign | Tolerated | Neutral |
| F1231L | Conflicting | C0 | Weak/Null | Weak/Null | Possibly damaging | Damaging | Neutral |
| I1275V | Conflicting | C0 | Weak/Null | Increased | Benign | Tolerated | Neutral |
| H1421R | Conflicting | C15 | Weak/Null | Weak/Null | Possibly damaging | Damaging | Neutral |
| H1421Y | VUS | C0 | Weak/Null | Weak/Null | Benign | Tolerated | Neutral |
| E1470D | Conflicting | C0 | Weak/Null | Weak/Null | Benign | Damaging | Neutral |
| BRCA2 | |||||||
| I283V | Conflicting | C0 | Weak/Null | Weak/Null | Benign | Tolerated | Neutral |
| I488V | VUS | C0 | Weak/Null | Weak/Null | Benign | Tolerated | Neutral |
| Y600H | Conflicting | C0 | Weak/Null | Weak/Null | Benign | Tolerated | Neutral |
| K1058R | Conflicting | C0 | Weak/Null | Weak/Null | Benign | Tolerated | Neutral |
| D1923A | Conflicting | C0 | Weak/Null | Weak/Null | Benign | Damaging | Deleterious |
| Q2159E | Conflicting | C0 | Weak/Null | Weak/Null | Benign | Tolerated | Neutral |
| K2950N | Conflicting | C35 | Moderate | Weak/Null | Probably damaging | Damaging | Neutral |
| P3292L | Conflicting | C0 | Weak/Null | Weak/Null | Probably damaging | Damaging | Deleterious |
| Gene/Variant Patient Identification | NCCN 1 | Age dx | Tumor Type | Tumor Size (cm) | Lymph Nodes | Receptors | Family History of Cancers |
|---|---|---|---|---|---|---|---|
| BRCA2 c.1794_1798del5 | |||||||
| UPR1024 | NA | 52 | NA | 2.0 | negative | PR−, HER2- | Sister, breast (dx NA) |
| BRCA2 E1308X | |||||||
| PRI1154 | yes | 55 | ductal, in situ | NA | negative | ER+, PR+ | Maternal uncle, breast (dx 60 yrs) |
| PRI1304 | yes | 33 | NA | NA | NA | NA | Sister, breast (dx 46); sister, breast (dx 47); father, liver (dx 77) |
| PRI1657 | yes | 24 | ductal, invasive | NA | NA | ER+, PR+, HER2- | Paternal grand-parent, gastric (dx 83) |
| PRI1699 | yes | 50 | ductal, in situ | 1.5 | NA | ER+, PR+ | Mother, ovarian (dx 69); paternal uncle, breast (dx 62) |
| PRI1713 | yes | 38 | lobular, invasive | 1.5 | negative | ER+, PR+ | Maternal aunt, breast (dx 40) |
| PRI1936 | yes | 46 | ductal, in situ | NA | NA | ER+, PR+, HER2- | Father, pancreas (dx 50); paternal aunt, breast (dx 60); maternal uncle, breast (dx 54); maternal grand-mother, breast (dx 75) |
| PRI1949 | NA | 53 | ductal, in situ | 0.1 | NA | ER+, PR+, HER2+ | Father, prostate (dx 70); brother, prostate (dx 47), sister, thyroid (dx 58) |
| UPR1043 | yes | 40 | NA | 2.1 | negative | ER+, PR+, HER2+ | Sister, breast (dx NA) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz-Zabala, H.J.; Ortiz, A.P.; Garland, L.; Jones, K.; Perez, C.M.; Mora, E.; Arroyo, N.; Oleksyk, T.K.; Echenique, M.; Matta, J.L.; et al. A Recurrent BRCA2 Mutation Explains the Majority of Hereditary Breast and Ovarian Cancer Syndrome Cases in Puerto Rico. Cancers 2018, 10, 419. https://doi.org/10.3390/cancers10110419
Diaz-Zabala HJ, Ortiz AP, Garland L, Jones K, Perez CM, Mora E, Arroyo N, Oleksyk TK, Echenique M, Matta JL, et al. A Recurrent BRCA2 Mutation Explains the Majority of Hereditary Breast and Ovarian Cancer Syndrome Cases in Puerto Rico. Cancers. 2018; 10(11):419. https://doi.org/10.3390/cancers10110419
Chicago/Turabian StyleDiaz-Zabala, Hector J., Ana P. Ortiz, Lisa Garland, Kristine Jones, Cynthia M. Perez, Edna Mora, Nelly Arroyo, Taras K. Oleksyk, Miguel Echenique, Jaime L. Matta, and et al. 2018. "A Recurrent BRCA2 Mutation Explains the Majority of Hereditary Breast and Ovarian Cancer Syndrome Cases in Puerto Rico" Cancers 10, no. 11: 419. https://doi.org/10.3390/cancers10110419
APA StyleDiaz-Zabala, H. J., Ortiz, A. P., Garland, L., Jones, K., Perez, C. M., Mora, E., Arroyo, N., Oleksyk, T. K., Echenique, M., Matta, J. L., Dean, M., & Dutil, J. (2018). A Recurrent BRCA2 Mutation Explains the Majority of Hereditary Breast and Ovarian Cancer Syndrome Cases in Puerto Rico. Cancers, 10(11), 419. https://doi.org/10.3390/cancers10110419