Abstract
A microfluidic chip is a tiny reactor that can confine and flow a specific amount of fluid into channels of tens to thousands of microns as needed and can precisely control fluid flow, pressure, temperature, etc. Point-of-care testing (POCT) requires small equipment, has short testing cycles, and controls the process, allowing single or multiple laboratory facilities to simultaneously analyze biological samples and diagnose infectious diseases. In general, rapid detection and stage assessment of viral epidemics are essential to overcome pandemic situations and diagnose promptly. Therefore, combining microfluidic devices with POCT improves detection efficiency and convenience for viral disease SARS-CoV-2. At the same time, the POCT of microfluidic chips increases user accessibility, improves accuracy and sensitivity, shortens detection time, etc., which are beneficial in detecting SARS-CoV-2. This review shares recent advances in POCT-based testing for COVID-19 and how it is better suited to help diagnose in response to the ongoing pandemic.
1. Introduction
Although considerable methods have been constructed to detect infectious diseases, early-stage screening plays an important role in controlling the spread of viral infections and protecting it from creating a catastrophe. Viruses cause huge numbers of people to suffer from diseases, congenital disabilities, and even death, and they also have the potential to mutate rapidly and spread rapidly through different pathways. Currently, many discoveries are related to understanding various aspects of virology, and viruses remain a major cause of disease [1].
In the 21st century, the severe acute respiratory syndrome coronavirus (SARS-CoV) resulted in significant morbidity and mortality. The coronavirus disease 2019 (COVID-19) caused by the extreme acute SARS-CoV-2 virus was discovered in December 2019 and has spread rapidly around the world [1,2,3]. COVID-19 is the product of SARS-CoV-2 infecting host cells via the angiotensin-converting enzyme 2, which has a higher transmission potential than SARS [4]. World Health Organization has recognized the COVID-19 outbreak as a pandemic. Currently, the primary approach to controlling a pandemic situation is to achieve an accurate diagnosis of the virus to control and break the spread of the virus quickly [5,6]. Besides performing large-scale testing, focusing on isolating infected areas using POCT can provide treatment faster and more accurately, saving lives [7,8]. Rapid devices or biosensors for detecting viruses must be constructed to enable early detection and diagnosis. Generally, the principles of detection strategies for SARS-CoV-2 are usually divided into several categories depending on the biomarkers of analysis: antibodies and nucleic acids. Nucleic acid testing, including gene sequence and reverse transcription-polymerase chain reaction (RT-PCR), is sensitive and stable, and these tests are suitable for large diagnostic in laboratories. On the other hand, the antibodies detected in the blood are immunoglobulin G (IgG) and immunoglobulin M, which can be constructed for the sensitive detection of SARS-CoV-2 [9]. Notably, applying the above strategy RT-PCR for rapid detection in the field outside the laboratory setting is extremely difficult. Due to the rapid evolution of COVID-19 disease and the limited capacity of laboratory-based molecular assays, there is an urgent need for a rapid POCT strategy for the clinical diagnosis of COVID-19 outside the laboratory setting that can provide results within minutes for rapid decisions on patient management. Although many POCT methods are capable of detecting viruses, they use large amounts of reagents, are costly, and have multiple complex spiking sessions that lengthen the detection time and increase human error [10]. These inevitably add to the problems of reliability and sensitivity of the test results.
How do we address the challenges of POCT in SARS-CoV-2 sensitivity and rapidity detection? Microfluidic chips, also known as lab on a chip (LoC), have the characteristics of rapid detection, low cost, and are an ideal tool for simplifying complex small laboratories processes on a tiny device that can integrate sample handling, analysis and other processes and provide the necessary information from a small number of samples [11,12,13,14,15]. Decades of research into microelectronics and microelectromechanical-systems technology have opened up new avenues for developing microfluidic devices to detect viral infections [16,17,18]. Microfluidic chips can be used as a fast, accurate, and automated platform for detecting viral nucleic acids, the number of antibodies in the serum, etc. [1,4]. Combining microfluidic technology with POCT testing can therefore achieve goals that are not possible with conventional biomedical testing, making it easy to diagnose viruses in situ, even in remote locations.
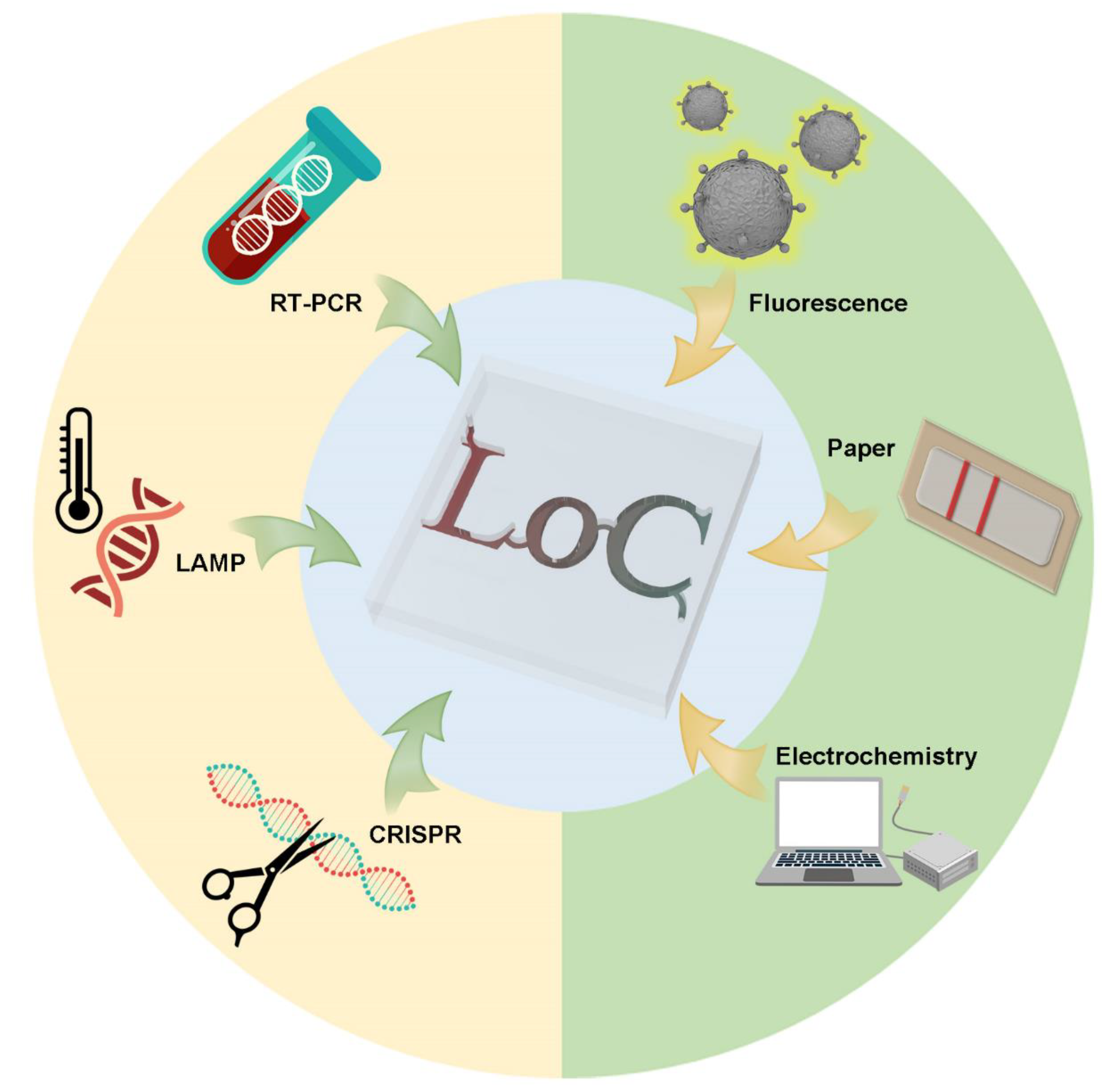
Building on the above, we review the existing POCT methods based on the microfluidic technique. We also review some under-development commercial POCT microfluidic methods, which use nucleic acid assays, immunoassays, biosensor assays and other assays for rapid standard diagnostics of COVID-19, shown in Figure 1.
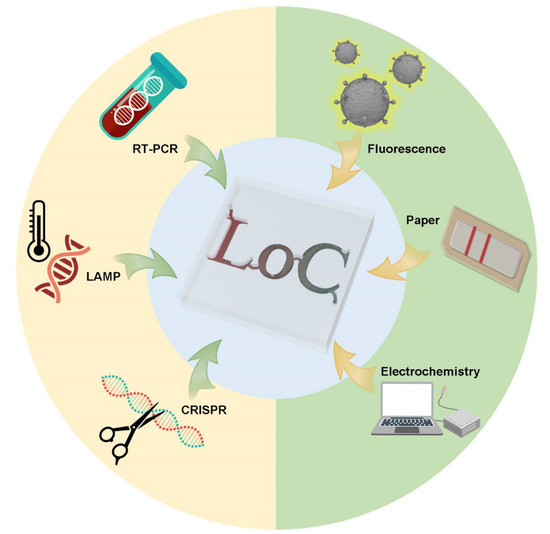
Figure 1.
Schematic view of POCT methods for microfluidic use to detect SARS-CoV-2.
2. Nucleic Acid Tests (NAT) Based on Microfluidics
NAT’s high sensitivity and specificity make it the first choice for SARS-CoV-2 detection, especially when COVID-19 antibodies are not yet mass-produced [19,20]. The primary process of nucleic acid detection includes sample collection, virus enrichment, amplification, and detection. However, nucleic acid detection requires multiple rounds of amplification and a long reaction time. Improper primer design and contamination can lead to false negatives and false positives. Microfluidics can control fluid more accurately, transfer heat faster and integrate multiple functions. Therefore, microfluidic technology can provide miniaturization and a high-efficiency solution for nucleic acid detection [21]. Nucleic acid methods based on microfluidics, such as RT-PCR, loop-mediated isothermal amplification (LAMP), and clustered regularly spaced short palindromic repeats (CRISPR), have been used in recent years to identify SARS-CoV-2. This section tells the story and narrates the most recent findings of scientific research teams and marketed POCT equipment.
2.1. RT-PCR Tests
RT-PCR combines RNA reverse transcription and complementary DNA (cDNA) PCR technologies. The basic steps for detecting SARS-CoV-2 by RT-PCR can be summarized as follows. Common sample collection forms are oropharyngeal, nasopharyngeal, or anal swabs [22]. The virus is filtered and purified from the sample. After extracting RNA, reverse transcriptase produces cDNA. The target fragment was amplified and synthesized by DNA polymerase using cDNA as a template. Currently, RT-PCR has become the gold standard for COVID-19 diagnosis [23].
Microfluidic chips’ channels have cross-sectional dimensions in micrometers and fluid volumes in microliters [24,25]. On the one hand, the smaller volume significantly reduces reagent consumption and greatly saves costs. High integration of different functions in a small space is also suitable for POCT development requirements [26]. On the other hand, the large surface–volume ratio allows diffusion and heat conduction to be efficient [27,28]. Microfluidics can improve detection accuracy and shorten detection time for RT-PCR using mass and heat transfer methods following basic hydrodynamic rules, which helps with the required repeated temperature changes.
Whole-genome sequencing is essential for virus recognition, PCR primer design, and vaccine development. Rapid sequencing could allow people to respond sooner and cause minor damage as the virus mutates. Li et al. reported an efficient whole-genome sequencing workflow based on microfluidic [29]. They integrated one-step RT-PCR amplification in the microfluidic system and precisely controlled µL fluid in microchannels and microchambers. In the integrated fluidic circuit chip, each sample and primer well contain only 5 µL and 10 µL mixtures, respectively. Although the smaller volume requires more efficient enrichment methods and more genomic copies due to the small amount of RNA in the sample, it effectively avoids tedious operations and cross-contamination between samples.
The extraction and purification of viral RNA is the key to accurate detection by RT-PCR. The participation of microfluidic devices can make this process smaller and faster. Turiello et al. developed an automatable rotationally driven microfluidic platform for enriching and purifying SARS-CoV-2 RNA [30]. The device uses nanotrap magnetic virus particles to isolate the virus for sample enrichment, which removes the complex matrix and avoids inhibiting RNA amplification and detection. The enzyme lysis mixture in the device lyses the virus capsids, releasing the pathogenic nucleic acid and realizing the purification process. Six samples can be preprocessed simultaneously in 15 min and used for RT-PCR. The effectiveness of the device is comparable to that of commercial kits. This automated sample preparation reduces operator involvement, effectively avoiding sample contamination and reducing the risk of infection.
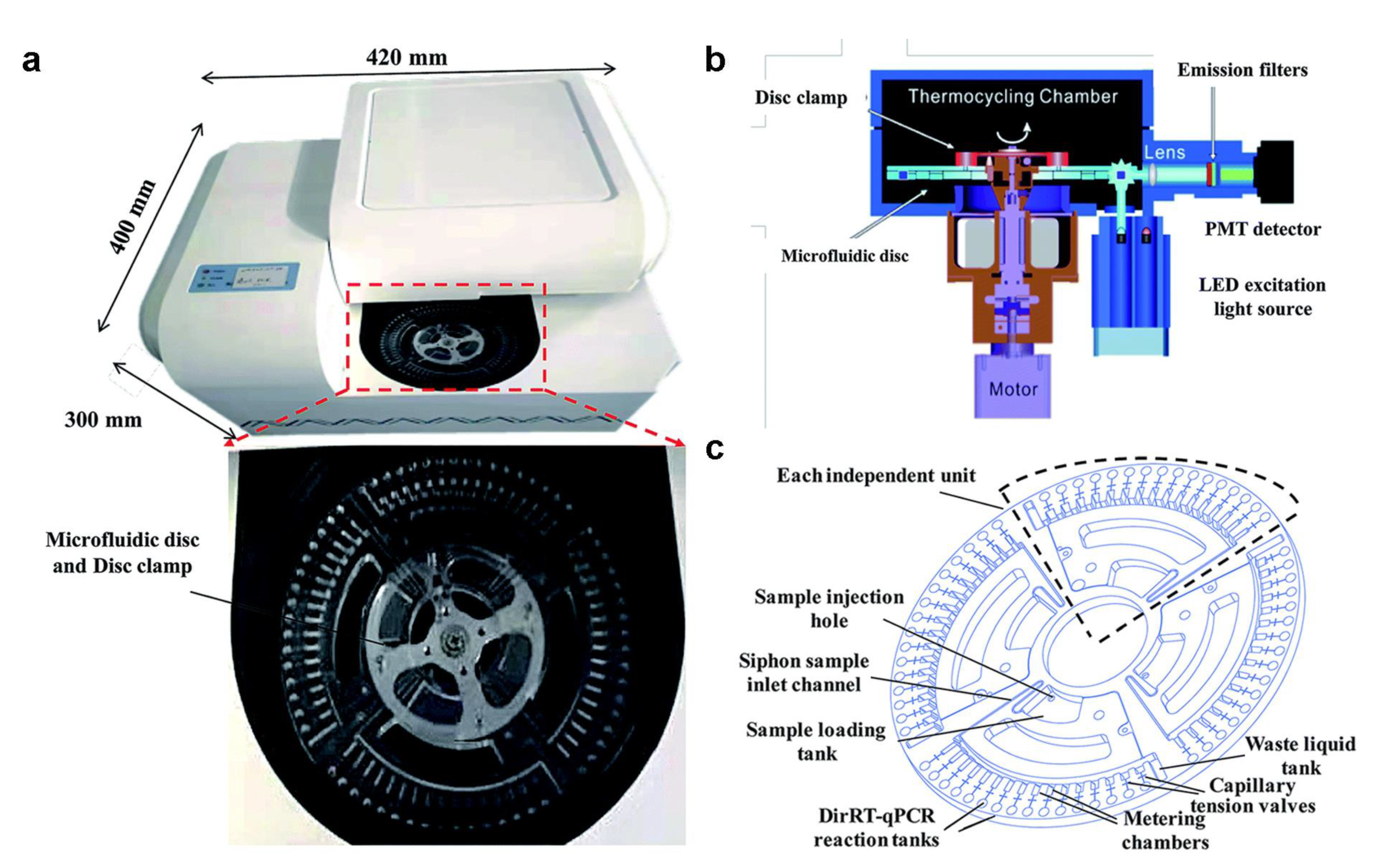
Microfluidic biochips and portable detection devices using RT-PCR technology provide strong support for the rapid and accurate detection of SARS-CoV-2. Centrifugal microfluidic chips are widely used in disease diagnosis [31,32]. They do not rely on expensive equipment and only use the centrifugal force generated by the rotation of the drive motor to drive the fluid. In addition, the centrifugal microfluidic chip enables highly integrated and automated multiple detections, improving functionality and practicality [33]. Figure 2 shows a direct RT-PCR method developed by Ji et al., based on a centrifugal microfluidic chip system [34]. In addition to the microfluidic chip and the drive motor, the system also contains an optical detection unit and a temperature control unit. The optical detection unit uses the LED Light Source as the excitation source, and a photomultiplier tube with emission filters to collect the fluorescence. This system can detect and classify SARS-CoV-2 and influenza A and B in 1.5 h without professional operators. The centrifugal microfluidic is commonly used for nucleic acid detection. It is simple to drive, does not need an external pump to control the fluid, and has almost no possibility of polluting the environment. In addition, the microfluidic chip has the advantage of realizing multiple target detection. Distinguishing COVID-19 and influenza, which have similar symptoms, could provide access to mass early screening and reduce medical pressure [35,36,37,38].

Figure 2.
(a) Photo of a portable centrifugal microfluidic device. (b) Schematic diagram of each component of the microfluidic device. (c) Schematic diagram of the structure and functional areas of the centrifugal microfluidic chip. (Reprinted/adapted with permission from Ref. [34]. Copyright 2020 Royal Society of Chemistry).
The disadvantages of RT-PCR cannot be ignored either. Due to the virus incubation period and differences in the amount of virus carried by individuals, upper respiratory tract sampling is often unable to obtain sufficient virus load samples the first time [39]. In addition, irregular operation of sampling personnel and contamination of samples may lead to inaccurate test results [40]. These problems limit the use of RT-PCR. We believe that the standardization and automation of the sampling process in microfluidic chips may improve this problem.
2.2. LAMP Tests
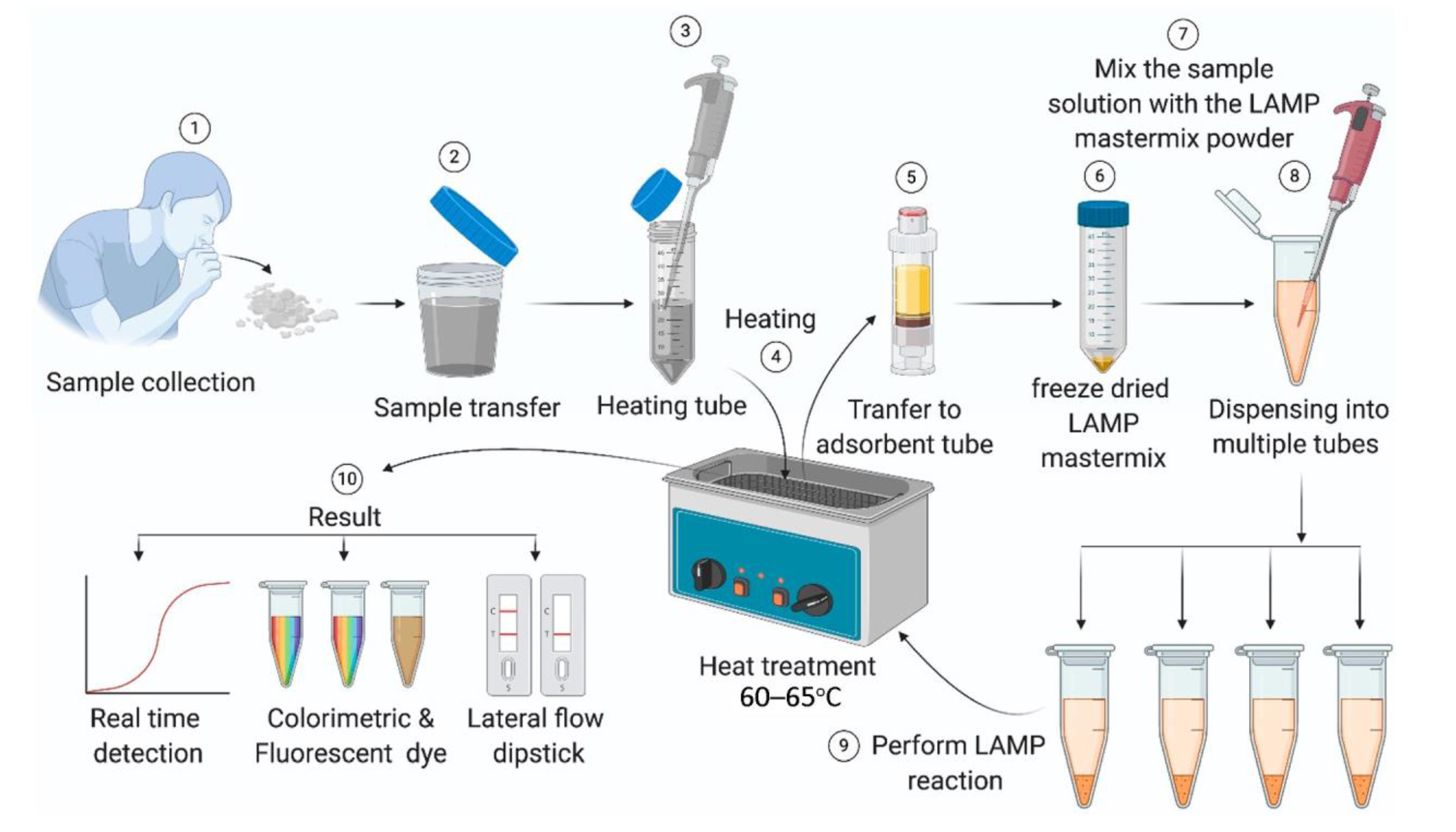
Isothermal amplification technology (IAT) can overcome the limitation of multiple thermal cycles of traditional PCR and carry out nucleic acid amplification under constant temperature. The development of IAT has greatly simplified PCR analysis steps, reduced detection time, and reduced operational difficulty [41,42,43,44]. LAMP is vital to IAT and can detect multiple targets simultaneously in a single reaction. Some studies have shown that LAMP is more sensitive and accurate than RT-PCR in detecting SARS-CoV-2. Figure 3 presents the reaction process of LAMP [45], which can be summarized as amplifying LAMP-specific primers and extracted viral nucleic acids at a constant temperature of 60–65 ℃. The results are usually produced in colorimetry or fluorescence and read out by naked eyes or a small device. LAMP does not rely on large instruments in the detection and reading process. It is suitable for self-screening in communities and families.

Figure 3.
Schematic diagram of the LAMP detection process [45].
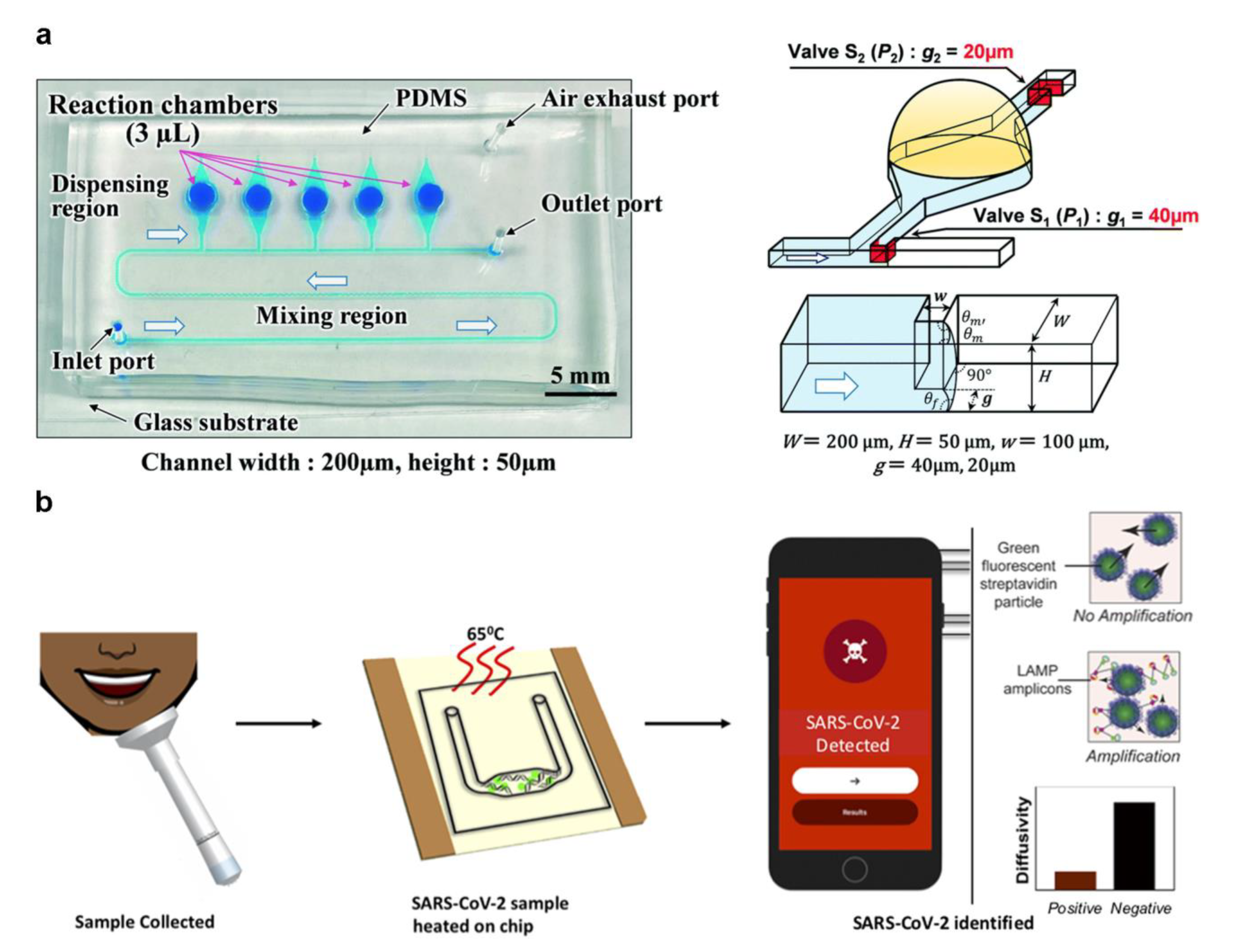
Natsuhara et al. designed a microfluidic chip with mixing and dispensing regions that can dispense continuous fluid (Figure 4a) [46]. In each chamber, infectious diseases such as COVID-19 and influenza can be analyzed by LAMP-based colorimetry. Changing the microchannel structure causes different cut-off pressures to achieve passive fluid dispensing. Lyu et al. developed a droplet array slip-chip that can be used for high-throughput detection of COVID-19 [47]. The fluid movement by sliding the chip is a simple step that avoids the precise bonding problems of traditional chips with high-precision microchannels. This design has tunability potential. This could allow the customizable design ability based on the modification of the size and density of the chamber while improving the detection efficiency. de Oliveira et al. reported a centrifuge microfluidic device manually controlled using a fidget spinner for LAMP-based SARS-CoV-2 detection [48]. The device is device-independent and portable, but the speed control is inaccurate, and improper operation may cause errors. The above works focus on designing a microfluidic chip structure to control the fluid, but there is a lack of a portable signal readout device.

Figure 4.
(a) A microfluidic chip structure of sequential fluid dispensing. (Reprinted/adapted with permission from Ref. [46]. Copyright 2021 Royal Society of Chemistry). (b) A microfluidic chip integrated LAMP and particle diffusometry. (Reprinted/adapted with permission from Ref. [49]. Copyright 2022 Elsevier).
Colorimetric and fluorescence methods are the most common readout method for LAMP detection results acquisition. The smartphone has become a reliable signal readout device for LAMP with enhanced image function and computing capability. Colbert et al. developed a SARS-CoV-2 detection technique by combining LAMP and particle diffusometry (Figure 4b) [49]. The samples containing fluorescent beads post-RT-LAMP can be imaged with the smartphone. There was a negative correlation between diffusion coefficient and virus content in the process of particle amplification. The virus can be detected in 35 min by using a smartphone to monitor the fluorescent signal. Lim et al. reported a highly integrated cartridge for SARS-CoV-2 detection and classification of different variants [50]. The device comprises an injection port, a micromixer, a detection area, a fluorescent excitation light source, and a pull-out chip placement area. The all-in-one portable device uses a smartphone to read signals and develops a unique program to analyze the detection signals and results, realizing complete analysis automation. The lack of reliance on specialized equipment allows LAMP-based microfluidic systems to provide POCT strategies for more ordinary people.
LAMP integration into the microfluidic system further reduces volume and operational requirements, making it a reliable way for people to accurately and rapidly self-diagnose COVID-19. However, LAMP requires the design of complex specific primers, which results in some diseases that cannot be detected by LAMP. In the face of rapidly mutating SARS-CoV-2, primer design will slow detection technology development [51]. Moreover, LAMP could not distinguish nonspecific amplification products caused by aerosol pollution, impurities in the sample base, enclosed environment destruction, and other factors. It may make highly sensitive LAMP produce false positives [52,53]. How to improve the system’s airtightness to avoid contamination of reagents is a problem that the designer needs to consider. For microfluidic systems, the injection process needs to be designed to be airtight and fluid-driven to avoid the entry of external impurities.
2.3. CRISPR-Associated Proteins System (Cas) Tests
CRISPR, dubbed “molecular scissors”, is a powerful gene-editing technology [54]. It originates from the bacteria’s acquired immune system, which cuts the DNA sequence of the invader with the intervention of CRISPR RNA (crRNA) and Cas enzymes [55]. CRISPR has two main classes. Class 1 interference complexes contain CRISPR-I, III, and IV, which employ a multieffector complex to cleave the target genome sequence using crRNA [56]. Class 2 is the system consisting of CRISPR-II, V, and VI, which uses a single multidomain Cas protein to interfere with the target region [57,58]. Cas12 and Cas13 in Class 2 are more suitable for SARS-CoV-2 detection among CRISPR-related proteins.
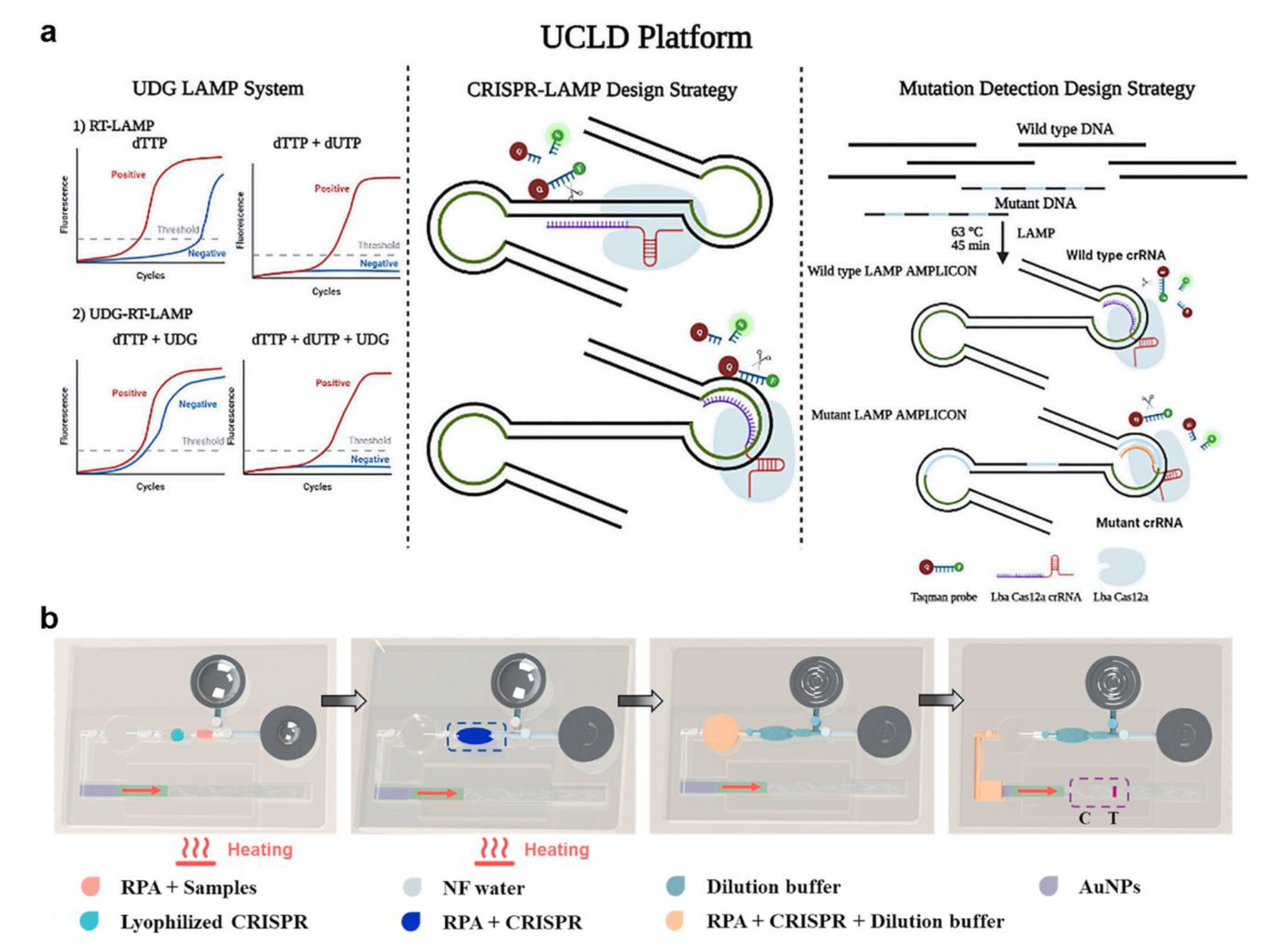
Zhang et al. constructed a CRISPR system combined with fluorophore-quencher DNA probes (Figure 5a) [59], which was a means of signal amplification and readout. Ramachandran et al. used isotachophoresis (ITP) to obtain an electric-field gradient on a microfluidic chip, combined with LAMP and CRISPR, to diagnose COVID-19 in 35 min [60]. In this system, Cas12 is combined with the guide DNA, the complex binds specifically to the target DNA, and the fluorophore-quencher DNA probes are cleaved. ITP optimizes DNA purification and speeds up the reaction in this process. CRISPR is greatly limited by the time-consuming nucleic acid amplification and the reliance on large instruments to read fluorescent signals. Silva et al. developed a catalase-mediated assay for detecting SARS-CoV-2 based on CRISPR [61]. Ribonucleoprotein complex was used to detect a SARS-CoV-2 reverse-transcribed DNA/RNA heteroduplex target. The bubble signal was produced by the transcleavage collateral activity of the Cas12a protein on a Catalase:ssDNA probe. The assay does not require nucleic acid amplification and can be read by smartphone photographing bubble signals. However, this analysis method can only be used for qualitative rather than quantitative detection. Some researchers have developed testing methods that are entirely independent of external devices. Li et al. reported a lateral flow microfluidic device using a hand-warmer pouch as a heat source (Figure 5b) [62]. They prestore the freeze-dried powder of the reagent in a reaction chamber. The user can push the liquid with fingers and read the results with the naked eye. The simple and device-independent operation will be the trend of SARS-CoV-2 detection technology.

Figure 5.
(a) Overview of the universally stable and precise CRISPR-LAMP detection platform. (Reprinted/adapted with permission from Ref. [59]. Copyright 2020 American Chemical Society). (b) A lateral flow microfluidic device that does not rely on external devices and has a hand-warmer pouch as its power source. (Reprinted/adapted with permission from Ref. [62]. Copyright 2022 Elsevier).
As an emerging technology, CRISPR-based detection takes less time and does not rely on complex equipment but is conducive to the quality of the equipment being used. In addition, in the face of the accelerated mutation rate of SARS-CoV-2, CRISPR can still perform highly sensitive detection for different mutation types. In addition, CRISPR can also detect results sensitively in samples with low viral loads [63,64]. However, the off-target effect of CRISPR can seriously affect the specificity of detection results, and the design complexity of crDNA also severely limits the development of this technology [65].
2.4. Commercial NAT Microfluidic Implementation
NAT for diagnosing COVID-19 has become a very reliable method for diagnosis [66]. Many commercial products used in Table 1 further classify these NAT devices. ID NOW™ COVID-19 from Abbott Diagnostics Scarborough Inc takes 15 min per test and targets the RNA-dependent RNA polymerase gene using an isothermal system. VitaPCR™ SARS-CoV-2 Gen2 Assay of Credo Diagnostics Biomedical Pte. Ltd. performs real-time PCR targeting N1, N2-Nucleocapsid Gene. Each test takes 20 min to finish. The device shows a positive (90.0%) and negative predictive value (99.0%) with high sensitivity (94.6%) and specificity (98.1%). The BioFire® Respiratory 2.1-EZ from BioFire Diagnostics, LLC can run simultaneous detection, which provides a wider range of diagnosis options for infectious diseases besides COVID-19. The nested multiplex PCR detection is advantageous, especially in dealing with different strains of COVID-19 at the same time. The Spike protein (S) gene and Membrane protein (M) gene are the targets for this device. 1copy COVID-19 qPCR Kit of 1 drop Inc focuses on RT PCR and targets. E gene is for beta coronavirus and the RdRp gene is for SARS-CoV-2. BIOSYNEX COVID-19 BSS gives an edge over only plasma or serum-dependent methods. Whole blood, serum, or plasma can all be used for detection. The kit also has a longer shelf time of 18 months. AQ-TOP COVID-9 Rapid Detection Kit PLUS of SEASUN BIOMATERIALS uses real-time Hyper RT-PCR, taking 30 min to produce results. The targets are SARS-CoV-2 Orf1ab and the human RNase P gene for this. Impressively, it has a claim to have no false positive due to its gene sequencing specific to the PNA probe. Novel Coronavirus (2019-nCoV) RT-PCR Detection Kit (Lyophilized) from Shanghai Chuangkun Bitech Inc. detects SARS-CoV-2 RNA using nasopharyngeal swabs, oropharyngeal swabs, sputum, and alveolar lavage fluid specimens. The kit targets the ORF1ab gene and N gene of SARS-CoV-2 with the real-time reverse transcription-polymerase chain reaction method.

Table 1.
Some commercialized POCT devices are based on NAT.
3. Microfluidics-Based POCT on Immunoassay
3.1. Fluorescence-Assisted Tests
Fluorescent elements to identify COVID-19 targeting the nanoparticles provides features such as large target surfaces, which contribute to the rapid identification of viral infections and play an important role in the COVID-19 detection system [76,77,78]. Nanoparticles can influence target elements [79,80] and amplification or sequencing steps [81,82], giving a better control with the overall detection methodology.
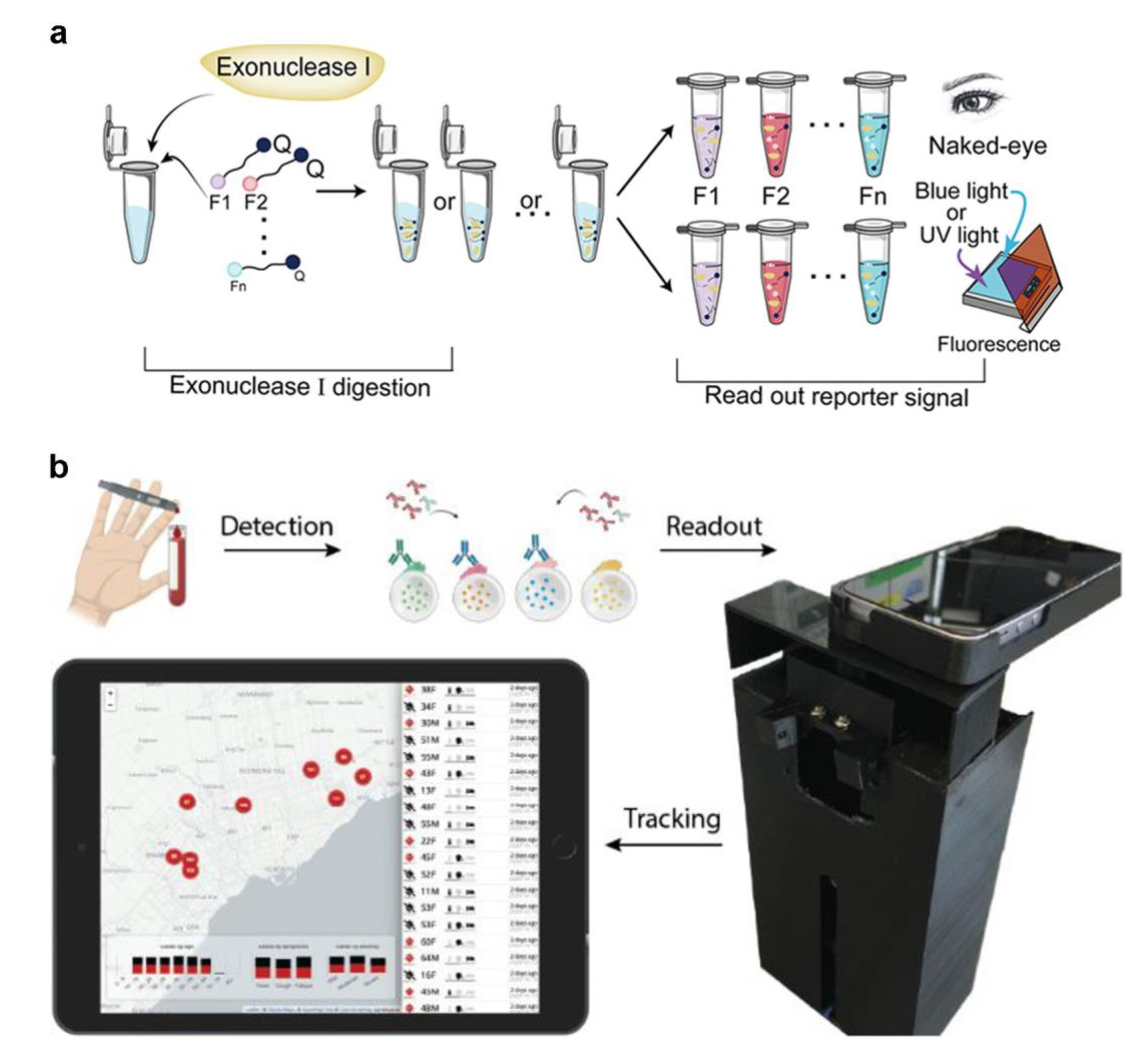
Due to the readability of fluorescence, it is the most prevalent signal-output nanoparticle. Fluorescence imaging has versatility and can be applied to various materials, including paper, polymers, and unstructured materials. [83,84,85]. It can also be used with smartphones or desktop scanners for automated analysis [79,86]. Virus avian influenza genomic DNA, for example, the development of a microfluidic system, was set up with a computer to amplify the target DNA, a bluish light-emitting diode, and a narrowband filter. The fluorescent signals provided by different dyes (EvaGreen, SYBR Green, and FAM fluorescent probe) can be recorded in real time using a smartphone. Ma et al. proposed another method for smartphone viral detection [87]. The group developed the process, which took 40 min to detect the H1N1 virus. Colorimetric methods that include modifying surfaces with chemical components may also be used to alert the consumer to the presence of viruses [88,89,90]. Their system used colorimetric LAMP with a passive microfluidic unit and an optical detector while regulating and analyzing the results using a smartphone. This makes developing POCT devices easier [72,76] and has accurate detection compatibility compared to the laboratory [79]. Xie et al. established a RApid VIsual CRISPR (RAVI-CRISPR) that can fabricate an instrument-less colorimetric POCT to detect SARS-CoV-2 [91]. In detail, exonuclease I cleavage (left) and subsequent inspection under blue or UV light or by the naked eye of colorimetric changes in the reaction solution (right) are used to determine ssDNA-FQ reporter activity (Figure 6a). In addition, a smartphone imaging platform loaded with software can diagnose SARS-CoV-2 at different sampling dates and infectious severity (Figure 6b) [92]. They fabricated a fluorescent-material (quantum dot) barcode device with about 3 times greater clinical sensitivity than lateral flow assays. In addition to this feature, the developed platform has the potential to realize antibody detection, immunity surveillance, and vaccination-induced seroconversion monitoring.
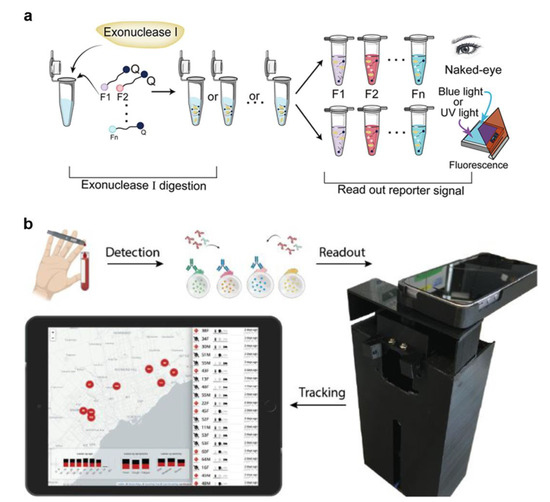
Figure 6.
(a) Screening and optimization of the ssDNA-FQ reporters for RAVI-CRISPR assays. (Reprinted/adapted with permission from Ref. [91]. Copyright 2022 American Chemical Society). (b) Schematic for the smartphone antibody detection workflow. (Reprinted/adapted with permission from Ref. [92]. Copyright 2021 American Chemical Society).
3.2. Paper-Based Tests
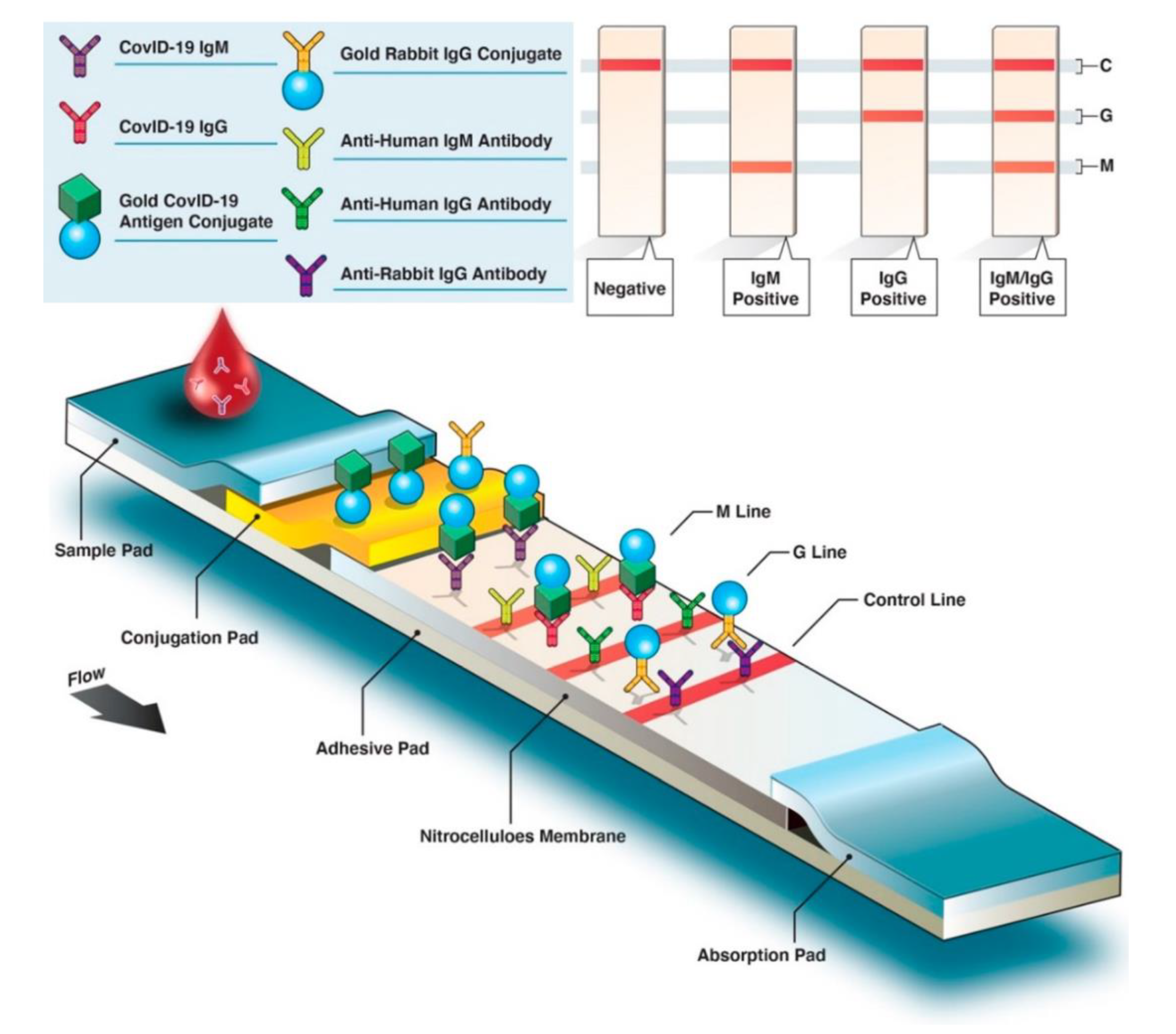
The advantage of the lateral flow assay (LFA) is that the color changes caused by the accumulation of gold nanoparticles can be read by naked eyes, providing a convenient way for large-scale screening of diseases [93,94,95,96]. With the development of nanotechnology, materials such as carbon nanoparticles and carbon nanotubes have significantly improved the sensitivity of LFA [97]. Researchers are also developing more sensitive technologies based on LFA that are not read by the naked eye [98]. Typically, patient antibodies (IgG, IgM, or IgA) produced against a specific SARS-CoV-2 antigen can be detected by LFA. Gold nanoparticle-labeled conjugated SARS-CoV-2-specific antigens bind with host antibodies. As antibody–antigen complexes migrate through the membrane, bound anti-SARS-CoV-2 IgM antibodies interact with anti-IgM secondary antibodies on the M line and anti-SARS-CoV-2 with anti-IgG on the G line. If the blood sample lacks SARS-CoV-2-specific antibodies, just the control (C) line will be visible (Figure 7). To create a commercial-grade LFA for detecting SARS-CoV-2 antigen, Benjamin D. Grant et al. employed publicly available reagents and a half-strip test procedure. The detection limit for recombinant antigen is 0.65 ng/mL [99]. Wen and Huang et al. optimized the pH, antigen concentration, and other parameters to ensure lateral flow immunoassay strip stability. The results for IgG and IgM antibodies against SARS-CoV-2 were both specific [97,100]. The specificities and sensitivities of IgM detection were 100% and 93.3%, respectively. Chen et al. used a fluorescent reporter lanthanide-doped polystyrene nanoparticles to detect anti-SARS-CoV-2 IgG in clinical samples [101]. The commercialization of the LFA approach for diagnosing COVID-19 has been widespread, and it can be implemented with simple equipment and low requirements for the detection environment. Additionally, it is capable of on-the-go inspection and has increased applications [102].
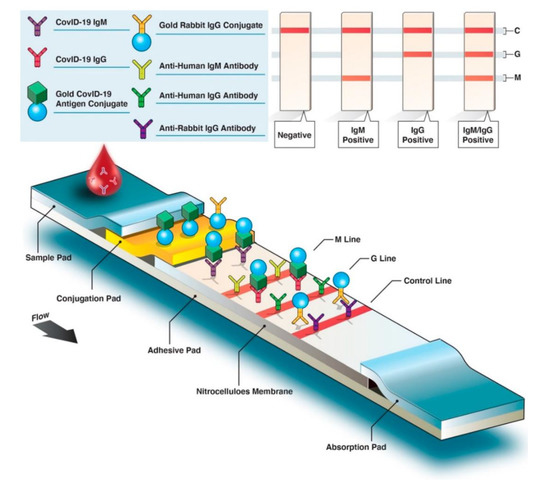
Figure 7.
Structure and flow diagram of colorimetric lateral flow immunoassay. (Reprinted/adapted with permission from Ref. [102]).
However, the lack of processing before testing can lead to some compounds skewing results and leading to false-positive results. To lower the number of false positives, improving the strip materials’ filtering capabilities is required by optimizing the strip materials’ processing, changing reagent compositions, and improving the anti-interference abilities. Yu et al. used an NLFA to detect three SARS-CoV-2 virus genes simultaneously: RdRp, ORF3a, and the N protein gene [103]. Before the NLFA method, amplification utilizing RT-PCR or another approach was required. NFLIAs have also been investigated for the detection of SARS-CoV-2. Several LFIAs have been developed to detect antibodies in the blood of COVID-19 patients due to the SARS-CoV-2 virus. Focusing on antibody detection may result in false-negative testing when the disease is in its early stages. This is because antibodies may be at undetectable levels in the days following infection [104,105]. During the COVID-19 epidemic, lateral flow technologies were created that are portable, fast-acting, low-cost, and simple to use. They are quickly becoming one of the best approaches for performing POC testing. This section has presented an overview of lateral flow assay testing improvements and how their sensitivity and specificity might be enhanced.
3.3. Electrochemical Biosensors
While electrochemical biosensors are tiny devices that are affordable and easy to shrink, they are particularly popular due to their simplicity and lower cost. In an electrochemical biosensor, real-time, specific, and accurate target monitoring generally relies on a tailored electrode, which acts as either the receptor or transducer depending on the need [106,107,108]. Potentiometric or amperometric signals, related to the presence of the analyte of interest, can be extracted from the sensing electrode’s information [109,110,111].
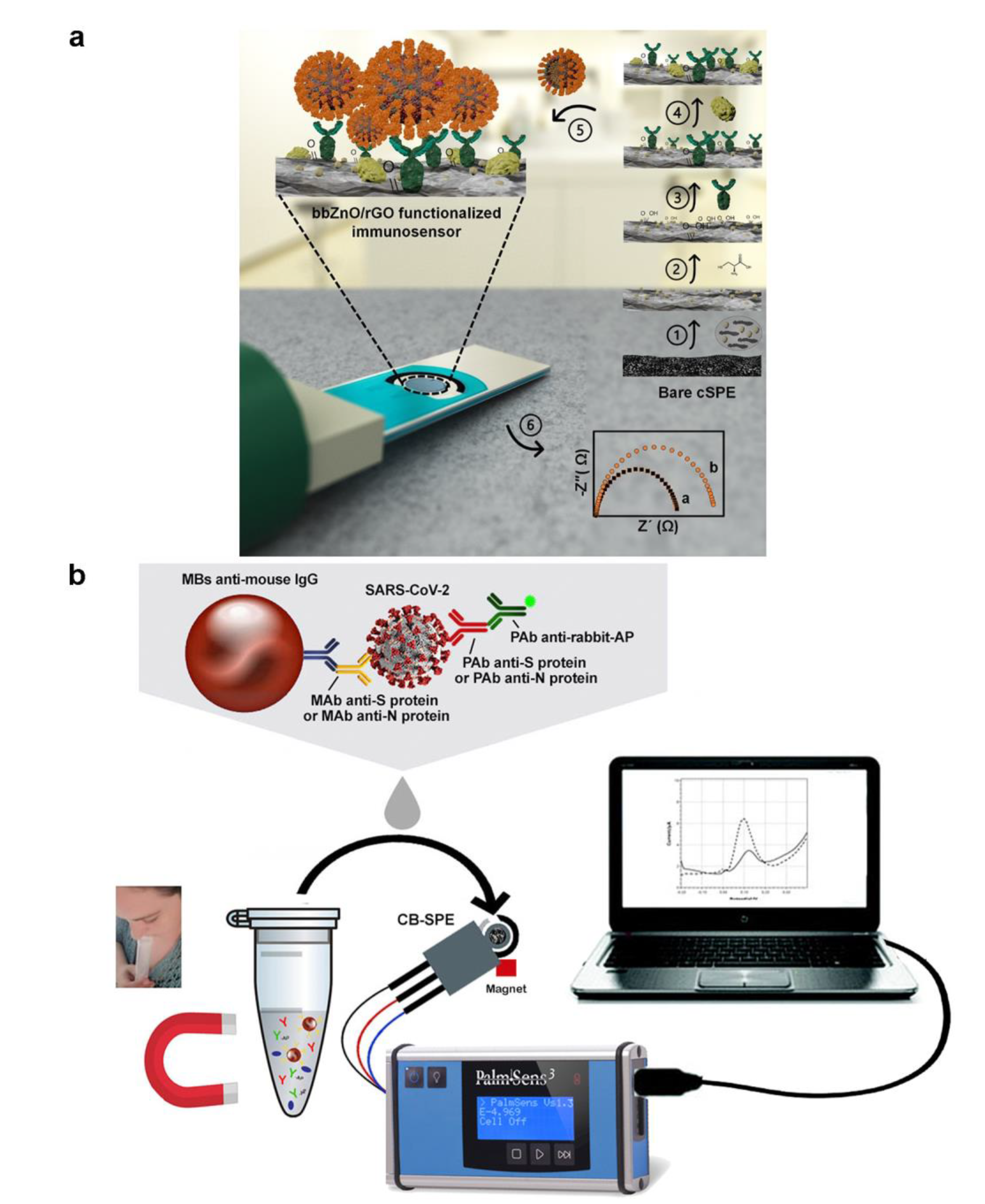
A portable electrochemical analysis device, combining surface immobilization with smartphone software, can acquire data rapidly and potentially be a smart POCT tool to help decrease the need for cumbersome gear [112]. The ability to identify viruses is even further enhanced by the ongoing research exploring various electrochemical solutions and, perhaps, cuts the cost and amount of time necessary to operate. Sanati-Nezhad et al. developed an electrochemical immuno-biosensing for the detection of SARS-CoV-2 nucleocapsid protein antigens by bbZnO/rGO nanocomposite coated on carbon screen-printed electrodes, which can improve the adsorbing of antibodies (Figure 8a) [113]. The fabricated device was then linked to the readout system, generating the resulting electrochemical signals in the presence of the COVID-19. The electrochemical immuno-biosensor could yield acceptable sensitivity and LOD, which was profoundly significant in early COVID-19 diagnosis. Ali et al. constructed a three-dimensional reduced-graphene-oxide electrode and connected it with a microfluidic device as an electrochemical sensor by introducing improved 3D-printing technology [114]. To allow for the detection of antibodies specific to SARS-CoV-2, viral antigens were attached to 3D electrodes, resulting in a detection limit of 2.8 × 10−15 M. Fabiani et al. created a miniaturized electrochemical sensor for the detection of SARS-CoV-2 using magnetic beads with a carbon black-based electrode (Figure 8b) [115]. Magnetic beads can increase preconcentration and minimize washing while retaining sensitivity and reliability. The external magnetic field can also help remove seasonal H1N1 influenza virus interference detection.
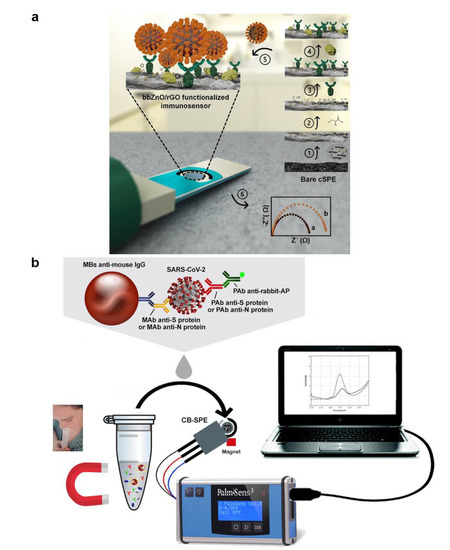
Figure 8.
(a) Graphical illustration of the step-by-step immuno-biosensor preparation. (Reprinted/adapted with permission from Ref. [113]. Copyright 2020 American Chemical Society). (b) Schematic diagram of electrochemical biosensor detection of a saliva sample. (Reprinted/adapted with permission from Ref. [115]. Copyright 2020 Elsevier).
Two recent studies have used paper’s low-cost, mobile, and disposable features as an electrochemical sensor substrate. To detect SARS-CoV-2 antibodies in about thirty minutes, Yakoh et al. designed an electrochemical apparatus that prints electrode patterns on paper [116]. The paper-based sensor has great potential as a POCT platform because of its unique, inexpensive, portable, and disposable qualities. The paper-based electrochemical substrate was utilized to attach the sensing probes, which were employed to develop a device that could detect nucleic acids [117]. Sensing materials, such as gold nanoparticles, are precisely designed to maximize the sensor’s sensitivity and output signals within five minutes. It is additionally able to provide a quantitative range for the detection of SARS-CoV-2 targets, from 585.4 copies/μL to 5.854 × 107 copies/μL, with a sensitivity of 231 copies/μL, which allows for the tracking of the infection progression in suspected cases. Data transmission to end-user devices is another crucial electrochemical-sensing component. Zhao et al. demonstrated that a smartphone’s electrochemical sensor could detect SARS-CoV-2 RNA, relieving the need for large-scale equipment and lab processes [118]. Portable testing may be possible if this “plug-and-play” setup is available to clients. A new study further integrated the electrochemical platform with a wireless module to help develop graphene electrodes that allow ultrarapid COVID-19 identification [119]. ‘SARS-CoV-2 RapidPlex′ can detect SARS-CoV infection while being inexpensive and highly sensitive, providing information on the three important components of COVID-19 disease (viral infection, immunological response, and disease severity) with the potential to be conducted at home.
3.4. Commercial Microfluidics Immunoassay Products
Many commercialized POCT devices are available based on immunoassay technology (Table 2) [120]. A. Menarini Diagnostics, Italy, developed immunoassay-based ANTIGEN RAPID TEST CASSETTE SARS-CoV-2 (SWAB). This takes a nasopharyngeal swab and uses nucleocapside protein. The overall process takes about 15 min. AAZ-LMB, France, uses the ELISA in their COV-QUANTO with plasma sampling. Nevertheless, this takes a long time. The process can take up to 210 min to finish. Panbio COVID-19 Ag Rapid Test by Abbott Rapid Diagnostics, Switzerland, uses the near-POC method, which takes 15 min to perform the rapid test from a nasal swab or nasopharyngeal swab. The accuracy this device claims to have 100% accuracy. Similarly, AccuBioTech Co., Ltd., China, launched ACCU-TELL® SARS-CoV-2 Neutralizing Antibody Cassette with near POC, which takes 10 min to finish detection from whole blood. Another POC device, Flowflex SARS-CoV-2 Antigen Rapid Test from Acon Biotech (Hangzhou) Co., Ltd., China, uses nucleocapsid protein as a detection principle. However, detection accuracy varies with the sampling, with 98.7% for the nasopharyngeal swab and 98.8% for the nasal swab. Actim Oy, Finland, uses immunochromatography in their Actim SARS-CoV-2 device to detect SARS-CoV-2 taking 15 min from sampling to result. InfectCheck®-COVID-19 IgG/IgM Test of Affimedix, Inc., United States and 2019-nCoV Antigen Device (Anterior Nasal Swab) AMS UK (NI) Ltd., United Kingdom uses similar technology, immunochromatography, but differs in sampling. Both the devices have good accuracy, with 99.8% and 98.1%, respectively.
Table 2.
Some Commercialized POCT devices based on immunoassay.
4. Conclusions and Perspectives
This review briefly discusses why microfluidic can be used as a POCT strategy for detecting SARS-CoV-2. Microfluidic technology can integrate complex analytical processes in small volumes, enabling sampling, mixing, separation, enrichment, washing, temperature control, and other operations. It can provide a rapid, accurate, and automated platform for SARS-CoV-2 detection at a low cost. Researchers have integrated typical NAT applications into microfluidic chips, including PT-PCR, LAMP, and CRISPR. In addition, highly sensitive analysis methods represented by fluorescence-assisted tests, paper-based tests, and electrochemical biosensors have also been widely used. False negatives may result from samples with low viral loads, which may also be caused by external environmental contamination and nonspecific reactions. While sensitivity and specificity have improved, occasional errors can delay prevention and treatment. Although the performance of these devices has been impressive, there is still a long way to go from leading-edge results in the laboratory. The operational requirements of commercial equipment make test results less reliable, and the product is not affordable for most people. We believe that as testing needs continue to increase, more exemplary methods can be introduced to the market.
As COVID-19 spreads and mutates, rapid, accurate testing in communities and households is critical. We believe that future detection methods can be improved in the following aspects. First, the development of standardized and automated sampling procedures to avoid detection errors caused by incorrect sampling and to reduce the burden on human resources. Second, it is necessary to reduce the difficulty of the operation and the detection time, which requires the complete coordination of processes such as reagent preparation, instrumentation, test procedures, and signal analysis. A simple-enough preparation process is fundamental to meeting the testing needs of developing regions. The premise of the large-scale popularization of technology is how to enable ordinary people to self-test rapidly. The third is the accuracy of the test results. Many tests are not designed to produce false negatives for samples with low viral loads and may also be caused by external environmental contamination and nonspecific reactions. While sensitivity and specificity have improved, occasional errors can delay prevention and treatment.
Author Contributions
B.Y. designed the structure; B.Y. provided funding; B.Y., X.W. and A.S.M.M.F.S. drafted the manuscript; X.W., edited figures; X.W. and A.S.M.M.F.S., collected the references; B.Y., A.S.M.M.F.S. and X.L. revised the manuscript; X.L. revised the figures. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Natural Science Foundation of China [grant number 52075138]; the Natural Science Foundation of Jiangsu Province [grant number BK20190872]; the Natural Science Foundation of the Jiangsu Higher Education Institutions of China [grant number 22KJB150050]; the Jiangsu Agricultural Science and Technology Innovation Fund [grant number CX(21)3162]; the Postgraduate Research & Practice Innovation Program of Jiangsu Province [grant number KYCX22_3479] and the Doctoral Scientific Research Foundation of Zhengzhou University of Light Industry [grant number 2021BSJJ001].
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviation
Point-of-care testing (POCT); severe acute respiratory syndrome coronavirus (SARS-CoV); coronavirus disease 2019 (COVID-19); reverse transcription-polymerase chain reaction (RT-PCR); immunoglobulin G (IgG); lab on a chip (LoC); loop-mediated isothermal amplification (LAMP); clustered regularly spaced short palindromic repeats (CRISPR); complementary DNA (cDNA); isothermal amplification technology (IAT); CRISPR-associated proteins system (Cas); CRISPR RNA (crRNA); isotachophoresis (ITP); RApid VIsual CRISPR (RAVI-CRISPR); lateral flow assay (LFA).
References
- Kim, D.; Lee, J.Y.; Yang, J.S.; Kim, J.W.; Kim, V.N.; Chang, H. The Architecture of SARS-CoV-2 Transcriptome. Cell 2020, 181, 914–921. [Google Scholar] [CrossRef]
- Guo, Y.R.; Cao, Q.D.; Hong, Z.S.; Tan, Y.Y.; Chen, S.D.; Jin, H.J.; Tan, K.S.; Wang, D.Y.; Yan, Y. The origin, transmission and clinical therapies on coronavirus disease 2019 (COVID-19) outbreak—An update on the status. Military Med. Res. 2020, 7, 11. [Google Scholar] [CrossRef] [Green Version]
- Jin, Y.H.; Cai, L.; Cheng, Z.S.; Cheng, H.; Deng, T.; Fan, Y.P.; Fang, C.; Huang, D.; Huang, L.Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [Green Version]
- Zheng, Y.Y.; Ma, Y.T.; Zhang, J.Y.; Xie, X. COVID-19 and the cardiovascular system. Nat. Rev. Cardiol. 2020, 17, 259–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Augustin, M.N.; Mbeva, J.B.K. Knowledge, attitudes, and behaviors of healthcare professionals at the start of an Ebola virus epidemic. Infect. Dis. Now 2021, 51, 50–54. [Google Scholar] [CrossRef]
- Sarkar, S. Breaking the chain: Governmental frugal innovation in Kerala to combat the COVID-19 pandemic. Gov. Inf. Q. 2021, 38, 101549. [Google Scholar] [CrossRef]
- Eames, K.T.D.; Keeling, M.J. Contact tracing and disease control. Proc. R. Soc. B-Biol. Sci. 2003, 270, 2565–2571. [Google Scholar] [CrossRef] [Green Version]
- Song, Q.; Sun, X.D.; Dai, Z.Y.; Gao, Y.B.; Gong, X.Q.; Zhou, B.P.; Wu, J.B.; Wen, W.J. Point-of-care testing detection methods for COVID-19. Lab Chip 2021, 21, 1634–1660. [Google Scholar] [CrossRef] [PubMed]
- Mou, L.; Zhang, Y.Y.; Feng, Y.; Hong, H.H.; Xia, Y.; Jiang, X.Y. Multiplexed Lab-on-a-Chip Bioassays for Testing Antibodies against SARS-CoV-2 and Its Variants in Multiple Individuals. Anal. Chem. 2022, 94, 2510–2516. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, Y.; Tang, H.; Zong, N.; Jiang, X.Y. Microfluidics for Biomedical Analysis. Small Methods 2020, 4, 1900451. [Google Scholar] [CrossRef]
- Yang, L.; Yamamoto, T. Quantification of Virus Particles Using Nanopore-Based Resistive-Pulse Sensing Techniques. Front. Microbiol. 2016, 7, 1500. [Google Scholar] [CrossRef] [Green Version]
- Zhu, H.L.; Fohlerova, Z.; Pekarek, J.; Basova, E.; Neuzil, P. Recent advances in lab-on-a-chip technologies for viral diagnosis. Biosens. Bioelectron. 2020, 153, 112041. [Google Scholar] [CrossRef] [PubMed]
- Yin, B.F.; Wan, X.H.; Yang, M.Z.; Qian, C.C.; Sohan, A. Wave-shaped microfluidic chip assisted point-of-care testing for accurate and rapid diagnosis of infections. Mil. Med. Res. 2022, 9, 8. [Google Scholar] [CrossRef]
- Yin, B.F.; Qian, C.C.; Wan, X.H.; Sohan, A.; Lin, X.D. Tape integrated self-designed microfluidic chip for point-of-care immunoassays simultaneous detection of disease biomarkers with tunable detection range. Biosens. Bioelectron. 2022, 212, 114429. [Google Scholar] [CrossRef]
- Yin, B.F.; Wan, X.H.; Qian, C.C.; Sohan, A.; Zhou, T.; Yue, W.K. Enzyme Method-Based Microfluidic Chip for the Rapid Detection of Copper Ions. Micromachines 2021, 12, 1380. [Google Scholar] [CrossRef]
- Peeri, N.C.; Shrestha, N.; Rahman, M.S.; Zaki, R.; Tan, Z.Q.; Bibi, S.; Baghbanzadeh, M.; Aghamohammadi, N.; Zhang, W.Y.; Haque, U. The SARS, MERS and novel coronavirus (COVID-19) epidemics, the newest and biggest global health threats: What lessons have we learned? Int. J. Epidemiol. 2020, 49, 717–726. [Google Scholar] [CrossRef] [Green Version]
- Prakash, S.; Pinti, M.; Bhushan, B. Theory, fabrication and applications of microfluidic and nanofluidic biosensors. Philos. Trans. R. Soc. A-Math. Phys. Eng. Sci. 2012, 370, 2269–2303. [Google Scholar] [CrossRef] [PubMed]
- Mazzu-Nascimento, T.; Donofrio, F.C.; Bianchi, B.C.; Travensolo, R.D.; Souza, J.B.; Moraes, D.A.; Morbioli, G.G.; Segato, T.P.; Varanda, L.C.; Carrilho, E. Paper-Based Microfluidics Immunoassay for Detection of Canine Distemper Virus. Braz. Arch. Biol. Technol. 2017, 60, e17160317. [Google Scholar] [CrossRef]
- Lu, S.M.; Lin, S.; Zhang, H.R.; Liang, L.G.; Shen, S. Methods of Respiratory Virus Detection: Advances towards Point-of-Care for Early Intervention. Micromachines 2021, 12, 697. [Google Scholar] [CrossRef]
- Zhang, S.Y.; Su, X.S.; Wang, J.; Chen, M.Y.; Li, C.Y.; Li, T.D.; Ge, S.X.; Xia, N.S. Nucleic Acid Testing for Coronavirus Disease 2019: Demand, Research Progression, and Perspective. Crit. Rev. Anal. Chem. 2022, 52, 413–424. [Google Scholar] [CrossRef]
- Su, W.T.; Gao, X.H.; Jiang, L.; Qin, J.H. Microfluidic platform towards point-of-care diagnostics in infectious diseases. J. Chromatogr. A 2015, 1377, 13–26. [Google Scholar] [CrossRef]
- Huang, C.L.; Wang, Y.M.; Li, X.W.; Ren, L.L.; Zhao, J.P.; Hu, Y.; Zhang, L.; Fan, G.H.; Xu, J.Y.; Gu, X.Y.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Gupta, N.; Augustine, S.; Narayan, T.; O’Riordan, A.; Das, A.; Kumar, D.; Luong, J.H.T.; Malhotra, B.D. Point-of-Care PCR Assays for COVID-19 Detection. Biosensors 2021, 11, 141. [Google Scholar] [CrossRef] [PubMed]
- Yin, B.F.; Qian, C.C.; Wang, S.B.; Wan, X.H.; Zhou, T. A Microfluidic Chip-Based MRS Immunosensor for Biomarker Detection via Enzyme-Mediated Nanoparticle Assembly. Front. Chem. 2021, 9, 688442. [Google Scholar] [CrossRef]
- Yin, B.F.; Wan, X.H.; Qian, C.C.; Sohan, A.; Wang, S.B.; Zhou, T. Point-of-Care Testing for Multiple Cardiac Markers Based on a Snail-Shaped Microfluidic Chip. Front. Chem. 2021, 9, 741058. [Google Scholar] [CrossRef]
- Yin, B.F.; Yue, W.K.; Sohan, A.; Zhou, T.; Qian, C.C.; Wan, X.H. Micromixer with Fine-Tuned Mathematical Spiral Structures. ACS Omega 2021, 6, 30779–30789. [Google Scholar] [CrossRef] [PubMed]
- Dong, X.B.; Liu, L.Y.; Tu, Y.P.; Zhang, J.; Miao, G.J.; Zhang, L.L.; Ge, S.X.; Xia, N.S.; Yu, D.L.; Qiu, X.B. Rapid PCR powered by microfluidics: A quick review under the background of COVID-19 pandemic. Trac-Trends Anal. Chem. 2021, 143, 116377. [Google Scholar] [CrossRef]
- Basiri, A.; Heidari, A.; Nadi, M.F.; Fallahy, M.T.P.; Nezamabadi, S.S.; Sedighi, M.; Saghazadeh, A.; Rezaei, N. Microfluidic devices for detection of RNA viruses. Rev. Med. Virol. 2021, 31, e2154. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Chung, H.K.; Pireku, P.K.; Beitzel, B.F.; Sanborn, M.A.; Tang, C.Y.; Hammer, R.D.; Ritter, D.; Wan, X.F.; Berry, I.M.; et al. Rapid High-Throughput Whole-Genome Sequencing of SARS-CoV-2 by Using One-Step Reverse Transcription-PCR Amplification with an Integrated Microfluidic System and Next-Generation Sequencing. J. Clin. Microbiol. 2021, 59, e02784-20. [Google Scholar] [CrossRef]
- Turiello, R.; Dignan, L.M.; Thompson, B.; Poulter, M.; Hickey, J.; Chapman, J.; Landers, J.P. Centrifugal Microfluidic Method for Enrichment and Enzymatic Extraction of Severe Acute Respiratory Syndrome Coronavirus 2 RNA. Anal. Chem. 2022, 94, 3287–3295. [Google Scholar] [CrossRef]
- Malic, L.; Brassard, D.; Da Fonte, D.; Nassif, C.; Mounier, M.; Ponton, A.; Geissler, M.; Shiu, M.; Morton, K.J.; Veres, T. Automated sample-to-answer centrifugal microfluidic system for rapid molecular diagnostics of SARS-CoV-2. Lab Chip 2022, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Zong, N.; Ye, F.; Mei, Y.; Qu, J.; Jiang, X. Dual-CRISPR/Cas12a-Assisted RT-RAA for Ultrasensitive SARS-CoV-2 Detection on Automated Centrifugal Microfluidics. Anal. Chem. 2022, 94, 9603–9609. [Google Scholar] [CrossRef] [PubMed]
- Miyazaki, C.M.; Carthy, E.; Kinahan, D.J. Biosensing on the Centrifugal Microfluidic Lab-on-a-Disc Platform. Processes 2020, 8, 1360. [Google Scholar] [CrossRef]
- Ji, M.H.; Xia, Y.; Loo, J.F.C.; Li, L.; Ho, H.P.; He, J.N.; Gu, D.Y. Automated multiplex nucleic acid tests for rapid detection of SARS-CoV-2, influenza A and B infection with direct reverse-transcription quantitative PCR (dirRT-qPCR) assay in a centrifugal microfluidic platform. RSC Adv. 2020, 10, 34088–34098. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.; Chu, C.H.; Sarioglu, A.F. Point-of-Care Toolkit for Multiplex Molecular Diagnosis of SARS-CoV-2 and Influenza A and B Viruses. ACS Sens. 2021, 6, 3204–3213. [Google Scholar] [CrossRef] [PubMed]
- Jiang, C.; Yao, X.G.; Zhao, Y.L.; Wu, J.M.; Huang, P.; Pan, C.H.; Liu, S.W.; Pan, C.G. Comparative review of respiratory diseases caused by coronaviruses and influenza A viruses during epidemic season. Microbes Infect. 2020, 22, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Solomon, D.A.; Sherman, A.C.; Kanjilal, S. Influenza in the COVID-19 Era. JAMA-J. Am. Med. Assoc. 2020, 324, 1342–1343. [Google Scholar] [CrossRef]
- Choreno-Parra, J.A.; Jimenez-Alvarez, L.A.; Cruz-Lagunas, A.; Rodriguez-Reyna, T.S.; Ramirez-Martinez, G.; Sandoval-Vega, M.; Hernandez-Garcia, D.L.; Choreno-Parra, E.M.; Balderas-Martinez, Y.I.; Martinez-Sanchez, M.E.; et al. Clinical and Immunological Factors That Distinguish COVID-19 From Pandemic Influenza A(H1N1). Front. Immunol. 2021, 12, 593595. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Long, L.Y.; Zhang, D.T.; Yan, T.T.; Cui, S.J.; Yang, P.; Wang, Q.Y.; Ren, S.M. Potential False-Negative Nucleic Acid Testing Results for Severe Acute Respiratory Syndrome Coronavirus 2 from Thermal Inactivation of Samples with Low Viral Loads. Clin. Chem. 2020, 66, 794–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Y.Y.; Pei, F.Y.; Ji, M.Y.; Wang, L.; Zhao, H.L.; Li, H.J.; Yang, W.H.; Wang, Q.X.; Zhao, Q.Q.; Wang, Y.S. Sensitivity evaluation of 2019 novel coronavirus (SARS-CoV-2) RT-PCR detection kits and strategy to reduce false negative. PLoS ONE 2020, 15, e0241469. [Google Scholar] [CrossRef] [PubMed]
- Kang, T.J.; Lu, J.M.; Yu, T.; Long, Y.; Liu, G.Z. Advances in nucleic acid amplification techniques (NAATs): COVID-19 point-of-care diagnostics as an example. Biosens. Bioelectron. 2022, 206, 114109. [Google Scholar] [CrossRef] [PubMed]
- Panpradist, N.; Kline, E.C.; Atkinson, R.G.; Roller, M.; Wang, Q.; Hull, I.T.; Kotnik, J.H.; Oreskovic, A.K.; Bennett, C.; Leon, D.; et al. Harmony COVID-19: A ready-to-use kit, low-cost detector, and smartphone app for point-of-care SARS-CoV-2 RNA detection. Sci. Adv. 2021, 7, eabj1281. [Google Scholar] [CrossRef] [PubMed]
- Park, G.S.; Ku, K.; Baek, S.H.; Kim, S.J.; Kim, S.I.; Kim, B.T.; Maeng, J.S. Development of Reverse Transcription Loop-Mediated Isothermal Amplification Assays Targeting Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2). J. Mol. Diagn. 2020, 22, 729–735. [Google Scholar] [CrossRef]
- Jiang, M.H.; Pan, W.H.; Arasthfer, A.; Fang, W.J.; Ling, L.Y.; Fang, H.; Daneshnia, F.; Yu, J.; Liao, W.Q.; Pei, H.; et al. Development and Validation of a Rapid, Single-Step Reverse Transcriptase Loop-Mediated Isothermal Amplification (RT-LAMP) System Potentially to Be Used for Reliable and High-Throughput Screening of COVID-19. Front. Cell. Infect. Microbiol. 2020, 10, 331. [Google Scholar] [CrossRef] [PubMed]
- Augustine, R.; Hasan, A.; Das, S.; Ahmed, R.; Mori, Y.; Notomi, T.; Kevadiya, B.D.; Thakor, A.S. Loop-Mediated Isothermal Amplification (LAMP): A Rapid, Sensitive, Specific, and Cost-Effective Point-of-Care Test for Coronaviruses in the Context of COVID-19 Pandemic. Biology 2020, 9, 182. [Google Scholar] [CrossRef] [PubMed]
- Natsuhara, D.; Saito, R.; Aonuma, H.; Sakurai, T.; Okamoto, S.; Nagai, M.; Kanuka, H.; Shibata, T. A method of sequential liquid dispensing for the multiplexed genetic diagnosis of viral infections in a microfluidic device. Lab Chip 2021, 21, 4779–4790. [Google Scholar] [CrossRef]
- Lyu, W.Y.; Zhang, J.J.; Yu, Y.; Xu, L.; Shen, F. Slip formation of a high-density droplet array for nucleic acid quantification by digital LAMP with a random-access system. Lab Chip 2021, 21, 3086–3093. [Google Scholar] [CrossRef]
- De Oliveira, K.G.; Estrela, P.F.N.; Mendes, G.D.; dos Santos, C.A.; Silveira-Lacerda, E.D.; Duarte, G.R.M. Rapid molecular diagnostics of COVID-19 by RT-LAMP in a centrifugal polystyrene-toner based microdevice with end-point visual detection. Analyst 2021, 146, 11. [Google Scholar] [CrossRef]
- Colbert, A.J.J.; Lee, D.H.; Clayton, K.N.; Wereley, S.T.; Linnes, J.C.; Kinzer-Ursem, T.L. PD-LAMP smartphone detection of SARS-CoV-2 on chip. Anal. Chim. Acta 2022, 1203, 339702. [Google Scholar] [CrossRef]
- Lim, J.; Stavins, R.; Kindratenko, V.; Baek, J.; Wang, L.Y.; White, K.; Kumar, J.; Valera, E.; King, W.P.; Bashir, R. Microfluidic point-of-care device for detection of early strains and B.1.1.7 variant of SARS-CoV-2 virus. Lab Chip 2022, 22, 1297–1309. [Google Scholar] [CrossRef]
- Nzelu, C.O.; Kato, H.; Peters, N.C. Loop-mediated isothermal amplification (LAMP): An advanced molecular point-of-care technique for the detection of Leishmania infection. PLoS Neglect. Trop. Dis. 2019, 13, e0007698. [Google Scholar] [CrossRef] [Green Version]
- Chaouch, M. Loop-mediated isothermal amplification (LAMP): An effective molecular point-of-care technique for the rapid diagnosis of coronavirus SARS-CoV-2. Rev. Med. Virol. 2021, 31, e2215. [Google Scholar] [CrossRef]
- Anahtar, M.N.; McGrath, G.E.G.; Rabe, B.A.; Tanner, N.A.; White, B.A.; Lennerz, J.K.M.; Branda, J.A.; Cepko, C.L.; Rosenberg, E.S. Clinical Assessment and Validation of a Rapid and Sensitive SARS-CoV-2 Test Using Reverse Transcription Loop-Mediated Isothermal Amplification Without the Need for RNA Extraction. Open Forum Infect. Dis. 2021, 8, ofaa631. [Google Scholar] [CrossRef]
- Barrangou, R.; Fremaux, C.; Deveau, H.; Richards, M.; Boyaval, P.; Moineau, S.; Romero, D.A.; Horvath, P. CRISPR provides acquired resistance against viruses in prokaryotes. Science 2007, 315, 1709–1712. [Google Scholar] [CrossRef] [PubMed]
- Moreno, A.M.; Mali, P. Therapeutic genome engineering via CRISPR-Cas systems. Wiley Interdiscip. Rev.-Syst. Biol. 2017, 9, e1380. [Google Scholar] [CrossRef]
- Koonin, E.V.; Makarova, K.S.; Zhang, F. Diversity, classification and evolution of CRISPR-Cas systems. Curr. Opin. Microbiol. 2017, 37, 67–78. [Google Scholar] [CrossRef] [PubMed]
- O’Connell, M.R. Molecular Mechanisms of RNA Targeting by Cas13-containing Type VI CRISPR-Cas Systems. J. Mol. Biol. 2019, 431, 66–87. [Google Scholar] [CrossRef]
- Makarova, K.S.; Wolf, Y.I.; Alkhnbashi, O.S.; Costa, F.; Shah, S.A.; Saunders, S.J.; Barrangou, R.; Brouns, S.J.J.; Charpentier, E.; Haft, D.H.; et al. An updated evolutionary classification of CRISPR-Cas systems. Nat. Rev. Microbiol. 2015, 13, 722–736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Zhao, W.; Zhao, W.; Si, Y.Y.; Chen, N.Z.; Chen, X.; Zhang, X.L.; Fan, L.Y.; Sui, G.D. Universally Stable and Precise CRISPR-LAMP Detection Platform for Precise Multiple Respiratory Tract Virus Diagnosis Including Mutant SARS-CoV-2 Spike N501Y. Anal. Chem. 2021, 93, 16184–16193. [Google Scholar] [CrossRef]
- Ramachandran, A.; Huyke, D.A.; Sharma, E.; Sahoo, M.K.; Huang, C.H.; Banaei, N.; Pinsky, B.A.; Santiago, J.G. Electric field-driven microfluidics for rapid CRISPR-based diagnostics and its application to detection of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2020, 117, 29518–29525. [Google Scholar] [CrossRef]
- Silva, F.S.R.; Erdogmus, E.; Shokr, A.; Kandula, H.; Thirumalaraju, P.; Kanakasabapathy, M.K.; Hardie, J.M.; Pacheco, L.G.C.; Li, J.Z.; Kuritzkes, D.R.; et al. SARS-CoV-2 RNA Detection by a Cellphone-Based Amplification-Free System with CRISPR/CAS-Dependent Enzymatic (CASCADE) Assay. Adv. Mater. Technol. 2021, 6, 2100602. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Ding, X.; Yin, K.; Avery, L.; Ballesteros, E.; Liu, C. Instrument-free, CRISPR-based diagnostics of SARS-CoV-2 using self-contained microfluidic system. Biosens. Bioelectron. 2022, 199, 113865. [Google Scholar] [CrossRef] [PubMed]
- Rahimi, H.; Salehiabar, M.; Barsbay, M.; Ghaffarlou, M.; Kavetskyy, T.; Sharafi, A.; Davaran, S.; Chauhan, S.C.; Danafar, H.; Kaboli, S.; et al. CRISPR Systems for COVID-19 Diagnosis. ACS Sens. 2021, 6, 1430–1445. [Google Scholar] [CrossRef] [PubMed]
- Suea-Ngam, A.; Bezinge, L.; Mateescu, B.; Howes, P.D.; deMello, A.J.; Richards, D.A. Enzyme-Assisted Nucleic Acid Detection for Infectious Disease Diagnostics: Moving toward the Point-of-Care. ACS Sens. 2020, 5, 2701–2723. [Google Scholar] [CrossRef] [PubMed]
- Habimana, J.D.; Huang, R.Q.; Muhoza, B.; Kalisa, Y.N.; Han, X.B.; Deng, W.Y.; Li, Z.Y. Mechanistic insights of CRISPR/Cas nucleases for programmable targeting and early-stage diagnosis: A review. Biosens. Bioelectron. 2022, 203, 114033. [Google Scholar] [CrossRef]
- Spindiag Declares CE-Conformity for Two New Rhonda PCR Rapid Tests for Use at the Point of Care (POC)—Spindiag. Available online: https://www.spindiag.de/ce-conformity-for-two-new-rhonda-pcr-rapid-tests/ (accessed on 15 July 2022).
- ID NOW COVID-19 Testing|Abbott U.S. Available online: https://www.abbott.com/IDNOW.html (accessed on 5 June 2022).
- Credo Diagnostics Biomedical VitaPCR SARS-CoV-2 Assay Garners CE Mark. Credo Diagnostics Biomedical Pte. Ltd. Available online: https://www.credodxbiomed.com/en/news/100-credo-diagnostics-biomedical-vitapcr-sars-cov-2-assay-garners-ce-mark (accessed on 5 June 2022).
- POC Respiratory Panel Test|Respiratory EZ Panel|BioFire Diagnostics. Available online: https://www.biofiredx.com/products/the-filmarray-panels/filmarray-respiratory-panel-ez (accessed on 5 June 2022).
- 1copy COVID-19 qPCR Multi Kit—Instructions for Use. Available online: https://www.fda.gov/media/137935/download (accessed on 5 June 2022).
- TEST COVID-19—Biosynex. Available online: https://www.biosynex.com/en/pharmacie-para-test-covid-19/ (accessed on 5 June 2022).
- Foaming Test—Covid-19 Screening Test Kit|PharmaNona. Available online: https://foamingtest.com/en (accessed on 5 June 2022).
- AQ-TOP COVID-19 Rapid Detection Kit PLUS—Instructions for Use. Available online: https://www.fda.gov/media/142800/download (accessed on 5 June 2022).
- COVID-19 Mutation Multiplex RT-PCR Detection Kit (Lyophilized). Available online: https://www.chkbiotech.com/covid-19-mutation-multiplex-rt-pcr-detection-kit-lyophilized-product/ (accessed on 5 June 2022).
- Zyobio_INSERTO.pdf. Available online: www.bvs.hn/COVID-19/Plataforma/Zyobio_INSERTO.pdf (accessed on 5 June 2022).
- Montesinos, I.; Gruson, D.; Kabamba, B.; Dahma, H.; Van den Wijngaert, S.; Reza, S.; Carbone, V.; Vandenberg, O.; Gulbis, B.; Wolff, F.; et al. Evaluation of two automated and three rapid lateral flow immunoassays for the detection of anti-SARS-CoV-2 antibodies. J. Clin. Virol. 2020, 128, 104413. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.H.; Kim, M.W.; Park, C.Y.; Choi, C.-S.; Kailasa, S.K.; Park, J.P.; Park, T.J. Development of a rapid and sensitive electrochemical biosensor for detection of human norovirus via novel specific binding peptides. Biosens. Bioelectron. 2019, 123, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Lu, P.H.; Ma, Y.D.; Fu, C.Y.; Lee, G.B. A structure-free digital microfluidic platform for detection of influenza a virus by using magnetic beads and electromagnetic forces. Lab Chip 2020, 20, 789–797. [Google Scholar] [CrossRef]
- Shi, B.; Li, Y.M.; Wu, D.; Wu, W.M. A handheld continuous-flow real-time fluorescence qPCR system with a PVC microreactor. Analyst 2020, 145, 2767–2773. [Google Scholar] [CrossRef] [PubMed]
- Richards, G.A.; Baker, T.; Amin, P.; Council World Federation, Societies. Ebola virus disease: Report from the task force on tropical diseases by the World Federation of Societies of Intensive and Critical Care Medicine. J. Crit. Care 2018, 43, 352–355. [Google Scholar] [CrossRef]
- Shen, K.M.; Sabbavarapu, N.M.; Fu, C.Y.; Jan, J.T.; Wang, J.R.; Hung, S.C.; Lee, G.B. An integrated microfluidic system for rapid detection and multiple subtyping of influenza A viruses by using glycan-coated magnetic beads and RT-PCR. Lab Chip 2019, 19, 1277–1286. [Google Scholar] [CrossRef] [PubMed]
- Black, J.A.; Hamilton, E.; Hueros, R.A.R.; Parks, J.W.; Hawkins, A.R.; Schmidt, H. Enhanced Detection of Single Viruses On-Chip via Hydrodynamic Focusing. IEEE J. Sel. Top. Quantum Electron. 2019, 25, 7201206. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Kang, M.; Park, E.; Chung, D.R.; Kim, J.; Hwang, E.S. A Simple and Multiplex Loop-Mediated Isothermal Amplification (LAMP) Assay for Rapid Detection of SARS-CoV. BioChip J. 2019, 13, 341–351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tourlousse, D.M.; Ahmad, F.; Stedtfeld, R.D.; Seyrig, G.; Tiedje, J.M.; Hashsham, S.A. A polymer microfluidic chip for quantitative detection of multiple water- and foodborne pathogens using real-time fluorogenic loop-mediated isothermal amplification. Biomed. Microdevices 2012, 14, 769–778. [Google Scholar] [CrossRef]
- Iswardy, E.; Tsai, T.C.; Cheng, I.F.; Ho, T.C.; Perng, G.C.; Chang, H.C. A bead-based immunofluorescence-assay on a microfluidic dielectrophoresis platform for rapid dengue virus detection. Biosens. Bioelectron. 2017, 95, 174–180. [Google Scholar] [CrossRef]
- Lee, S.H.; Baek, Y.H.; Kim, Y.H.; Choi, Y.K.; Song, M.S.; Ahn, J.Y. One-Pot Reverse Transcriptional Loop-Mediated Isothermal Amplification (RT-LAMP) for Detecting MERS-CoV. Front. Microbiol. 2017, 7, 2166. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.D.; Li, K.H.; Chen, Y.H.; Lee, Y.M.; Chou, S.T.; Lai, Y.Y.; Huang, P.C.; Ma, H.P.; Lee, G.B. A sample-to-answer, portable platform for rapid detection of pathogens with a smartphone interface. Lab Chip 2019, 19, 3804–3814. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Aggarwal, K.; Vinitha, T.U.; Nguyen, T.; Han, J.; Ahn, C.H. A new microchannel capillary flow assay (MCFA) platform with lyophilized chemiluminescence reagents for a smartphone-based POCT detecting malaria. Microsyst. Nanoeng. 2020, 6, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mauk, M.; Song, J.Z.; Bau, H.H.; Gross, R.; Bushman, F.D.; Collman, R.G.; Liu, C.C. Miniaturized devices for point of care molecular detection of HIV. Lab Chip 2017, 17, 382–394. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.C.; Wang, K.; Xu, H.; Yan, W.Q.; Jin, Q.H.; Cui, D.X. Detection platforms for point-of-care testing based on colorimetric, luminescent and magnetic assays: A review. Talanta 2019, 202, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.S.; Tao, D.G.; Fu, Y.H.; Xu, B.R.; Tang, Y.; Steinaa, L.; Hemmink, J.D.; Pan, W.Y.; Huang, X.; Nie, X.W.; et al. Rapid Visual CRISPR Assay: A Naked-Eye Colorimetric Detection Method for Nucleic Acids Based on CRISPR/Cas12a and a Convolutional Neural Network. ACS Synth. Biol. 2022, 11, 383–396. [Google Scholar] [CrossRef]
- Zhang, Y.W.; Malekjahani, A.; Udugama, B.N.; Kadhiresan, P.; Chen, H.M.; Osborne, M.; Franz, M.; Kucera, M.; Plenderleith, S.; Yip, L.; et al. Surveilling and Tracking COVID-19 Patients Using a Portable Quantum Dot Smartphone Device. Nano Lett. 2021, 21, 5209–5216. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.L.; Jiang, H.; Li, X.Q.; Lv, X.F. Recent advances in sensitivity enhancement for lateral flow assay. Microchim. Acta 2021, 188, 379. [Google Scholar] [CrossRef]
- Hristov, D.; Rijal, H.; Gomez-Marquez, J.; Hamad-Schifferli, K. Developing a Paper-Based Antigen Assay to Differentiate between Coronaviruses and SARS-CoV-2 Spike Variants. Anal. Chem. 2021, 93, 7825–7832. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.F.; Kacherovsky, N.; Panpradist, N.; Wan, R.; Liang, J.; Zhang, B.; Salipante, S.J.; Lutz, B.R.; Pun, S.H. Aptamer Sandwich Lateral Flow Assay (AptaFlow) for Antibody-Free SARS-CoV-2 Detection. Anal. Chem. 2022, 94, 7278–7285. [Google Scholar] [CrossRef]
- Boehringer, H.R.; O’Farrell, B.J. Lateral Flow Assays in Infectious Disease Diagnosis. Clin. Chem. 2021, 68, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wen, T.; Shi, F.J.; Zeng, X.Y.; Jiao, Y.J. Rapid Detection of IgM Antibodies against the SARS-CoV-2 Virus via Colloidal Gold Nanoparticle-Based Lateral-Flow Assay. ACS Omega 2020, 5, 12550–12556. [Google Scholar] [CrossRef]
- Chen, R.; Ren, C.P.; Liu, M.; Ge, X.P.; Qu, M.S.; Zhou, X.B.; Liang, M.F.; Liu, Y.; Li, F.Y. Early Detection of SARS-CoV-2 Seroconversion in Humans with Aggregation-Induced Near-Infrared Emission Nanoparticle-Labeled Lateral Flow Immunoassay. ACS Nano 2021, 15, 8996–9004. [Google Scholar] [CrossRef]
- Grant, B.D.; Anderson, C.E.; Williford, J.R.; Alonzo, L.F.; Glukhova, V.A.; Boyle, D.S.; Weigl, B.H.; Nichols, K.P. SARS-CoV-2 Coronavirus Nucleocapsid Antigen-Detecting Half-Strip Lateral Flow Assay Toward the Development of Point of Care Tests Using Commercially Available Reagents. Anal. Chem. 2020, 92, 11305–11309. [Google Scholar] [CrossRef]
- Wen, T.; Huang, C.; Shi, F.J.; Zeng, X.Y.; Lu, T.; Ding, S.N.; Jiao, Y.J. Development of a lateral flow immunoassay strip for rapid detection of IgG antibody against SARS-CoV-2 virus. Analyst 2020, 145, 5345–5352. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.H.; Zhang, Z.G.; Zhai, X.M.; Li, Y.Y.; Lin, L.; Zhao, H.; Bian, L.; Li, P.; Yu, L.; Wu, Y.S.; et al. Rapid and Sensitive Detection of anti-SARS-CoV-2 IgG, Using Lanthanide-Doped Nanoparticles-Based Lateral Flow Immunoassay. Anal. Chem. 2020, 92, 7226–7231. [Google Scholar] [CrossRef] [PubMed]
- Ghaffari, A.; Meurant, R.; Ardakani, A. COVID-19 Serological Tests: How Well Do They Actually Perform? Diagnostics 2020, 10, 453. [Google Scholar] [CrossRef] [PubMed]
- Yu, S.; Nimse, S.B.; Kim, J.; Song, K.S.; Kim, T. Development of a Lateral Flow Strip Membrane Assay for Rapid and Sensitive Detection of the SARS-CoV-2. Anal. Chem. 2020, 92, 14139–14144. [Google Scholar] [CrossRef]
- Zhu, X.; Wang, X.X.; Han, L.M.; Chen, T.; Wang, L.C.; Li, H.; Li, S.; He, L.F.; Fu, X.Y.; Chen, S.J.; et al. Multiplex reverse transcription loop-mediated isothermal amplification combined with nanoparticle-based lateral flow biosensor for the diagnosis of COVID-19. Biosens. Bioelectron. 2020, 166, 112437. [Google Scholar] [CrossRef]
- Wang, D.M.; He, S.G.; Wang, X.H.; Yan, Y.Q.; Liu, J.Z.; Wu, S.M.; Liu, S.G.; Lei, Y.; Chen, M.; Li, L.; et al. Rapid lateral flow immunoassay for the fluorescence detection of SARS-CoV-2 RNA. Nat. Biomed. Eng 2020, 4, 1150–1158. [Google Scholar] [CrossRef] [PubMed]
- Shaffaf, T.; Forouhi, S.; Ghafar-Zadeh, E. Towards Fully Integrated Portable Sensing Devices for COVID-19 and Future Global Hazards: Recent Advances, Challenges, and Prospects. Micromachines 2021, 12, 915. [Google Scholar] [CrossRef]
- Drobysh, M.; Ramanaviciene, A.; Viter, R.; Ramanavicius, A. Affinity Sensors for the Diagnosis of COVID-19. Micromachines 2021, 12, 390. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, A.K.; Dhau, J.S.; Gohel, H.; Mishra, Y.K.; Kateb, B.; Kim, N.Y.; Goswami, D.Y. Electrochemical SARS-CoV-2 Sensing at Point-of-Care and Artificial Intelligence for Intelligent COVID-19 Management. ACS Appl. Bio Mater. 2020, 3, 7306–7325. [Google Scholar] [CrossRef]
- De Eguilaz, M.R.; Cumba, L.R.; Forster, R.J. Electrochemical detection of viruses and antibodies: A mini review. Electrochem. Commun. 2020, 116, 106762. [Google Scholar] [CrossRef]
- Thiyagarajan, N.; Chang, J.L.; Senthilkumar, K.; Zen, J.M. Disposable electrochemical sensors: A mini review. Electrochem. Commun. 2014, 38, 86–90. [Google Scholar] [CrossRef]
- Beduk, T.; Beduk, D.; de Oliveira, J.I.; Zihnioglu, F.; Cicek, C.; Sertoz, R.; Arda, B.; Goksel, T.; Turhan, K.; Salama, K.N.; et al. Rapid Point-of-Care COVID-19 Diagnosis with a Gold-Nanoarchitecture-Assisted Laser-Scribed Graphene Biosensor. Anal. Chem. 2021, 93, 8585–8594. [Google Scholar] [CrossRef] [PubMed]
- Li, J.R.; Lillehoj, P.B. Microfluidic Magneto Immunosensor for Rapid, High Sensitivity Measurements of SARS-CoV-2 Nucleocapsid Protein in Serum. ACS Sens. 2021, 6, 1270–1278. [Google Scholar] [CrossRef] [PubMed]
- Haghayegh, F.; Salahandish, R.; Hassani, M.; Sanati-Nezhad, A. Highly Stable Buffer-Based Zinc Oxide/Reduced Graphene Oxide Nanosurface Chemistry for Rapid Immunosensing of SARS-CoV-2 Antigens. ACS Appl. Mater. Interfaces 2022, 14, 10844–10855. [Google Scholar] [CrossRef] [PubMed]
- Ali, M.A.; Hu, C.S.; Jahan, S.; Yuan, B.; Saleh, M.S.; Ju, E.G.; Gao, S.J.; Panat, R. Sensing of COVID-19 Antibodies in Seconds via Aerosol Jet Nanoprinted Reduced-Graphene-Oxide-Coated 3D Electrodes. Adv. Mater. 2021, 33, 2006647. [Google Scholar] [CrossRef] [PubMed]
- Fabiani, L.; Saroglia, M.; Galata, G.; De Santis, R.; Fillo, S.; Luca, V.; Faggioni, G.; D’Amore, N.; Regalbuto, E.; Salvatori, P.; et al. Magnetic beads combined with carbon black -based screen-printed electrodes for COVID-19: A reliable and miniaturized electrochemical immunosensor for SARS-CoV-2 detection in saliva. Biosens. Bioelectron. 2021, 171, 112686. [Google Scholar] [CrossRef]
- Yakoh, A.; Pimpitak, U.; Rengpipat, S.; Hirankarn, N.; Chailapakul, O.; Chaiyo, S. Paper-based electrochemical biosensor for diagnosing COVID-19: Detection of SARS-CoV-2 antibodies and antigen. Biosens. Bioelectron. 2021, 176, 112912. [Google Scholar] [CrossRef] [PubMed]
- Alafeef, M.; Dighe, K.; Moitra, P.; Pan, D. Rapid, Ultrasensitive, and Quantitative Detection of SARS-CoV-2 Using Antisense Oligonucleotides Directed Electrochemical Biosensor Chip. ACS Nano 2020, 14, 17028–17045. [Google Scholar] [CrossRef] [PubMed]
- Zhao, H.; Liu, F.; Xie, W.; Zhou, T.C.; OuYang, J.; Jin, L.; Li, H.; Zhao, C.Y.; Zhang, L.; Wei, J.; et al. Ultrasensitive supersandwich-type electrochemical sensor for SARS-CoV-2 from the infected COVID-19 patients using a smartphone. Sens. Actuator B-Chem. 2021, 327, 128899. [Google Scholar] [CrossRef]
- Torrente-Rodriguez, R.M.; Lukas, H.; Tu, J.B.; Min, J.H.; Yang, Y.R.; Xu, C.H.; Rossiter, H.B.; Gao, W. SARS-CoV-2 RapidPlex: A Graphene-Based Multiplexed Telemedicine Platform for Rapid and Low-Cost COVID-19 Diagnosis and Monitoring. Matter 2020, 3, 19. [Google Scholar] [CrossRef]
- Products Catalog—Biosurfit. Available online: https://www.biosurfit.com/en/products/spinit-covid-antibody/ (accessed on 15 July 2022).
- Schnurra, C.; Reiners, N.; Biemann, R.; Kaiser, T.; Trawinski, H.; Jassoy, C. Comparison of the diagnostic sensitivity of SARS-CoV-2 nucleoprotein and glycoprotein-based antibody tests. J. Clin. Virol. 2020, 129, 104544. [Google Scholar] [CrossRef]
- Antigen test ELISA—AAZ|COVID-19 AAZ. Available online: https://www.covid19aaz.com/en/antigen-test-elisa (accessed on 8 June 2022).
- Gremmels, H.; Winkel, B.M.F.; Schuurman, R.; Rosingh, A.; Rigter, N.A.M.; Rodriguez, O.; Ubijaan, J.; Wensing, A.M.J.; Bonten, M.J.M.; Hofstra, L.M. Real-life validation of the Panbio (TM) COVID-19 antigen rapid test (Abbott) in community-dwelling subjects with symptoms of potential SARS-CoV-2 infection. EClinicalMedicine 2021, 31, 100677. [Google Scholar] [CrossRef] [PubMed]
- SARS-CoV-2 Neutralizing Antibody, Coronavirus, COVID-19, Vaccine, SARS, Rapid Test. Available online: https://www.accubiotech.com/product-accu-tell-lt;sup-gt;-lt;-sup-gt;-sars-cov-2-neutralizing-antibody-rapid-test-cassette.html (accessed on 8 June 2022).
- Actim® SARS-CoV-2—Actim. Available online: https://www.actimtest.com/actim-sars-cov-2/ (accessed on 8 June 2022).
- TestNOW-COVID-19-e-Brochure-NEW. Available online: https://affimedix.com/wp-content/uploads/2021/10/TestNOW-COVID-19-e-Brochure-NEW.pdf (accessed on 30 May 2022).
- 2019-nCoV Antigen Device (Anterior Nasal Swab). Available online: www.amslabs.co.uk (accessed on 17 March 2022).
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).