Effectiveness and Safety of OnabotulinumtoxinA in Adolescent Patients with Chronic Migraine

 , , and
, , and
Abstract
1. Introduction
2. Results
2.1. Case Series
2.1.1. Patient Characteristics
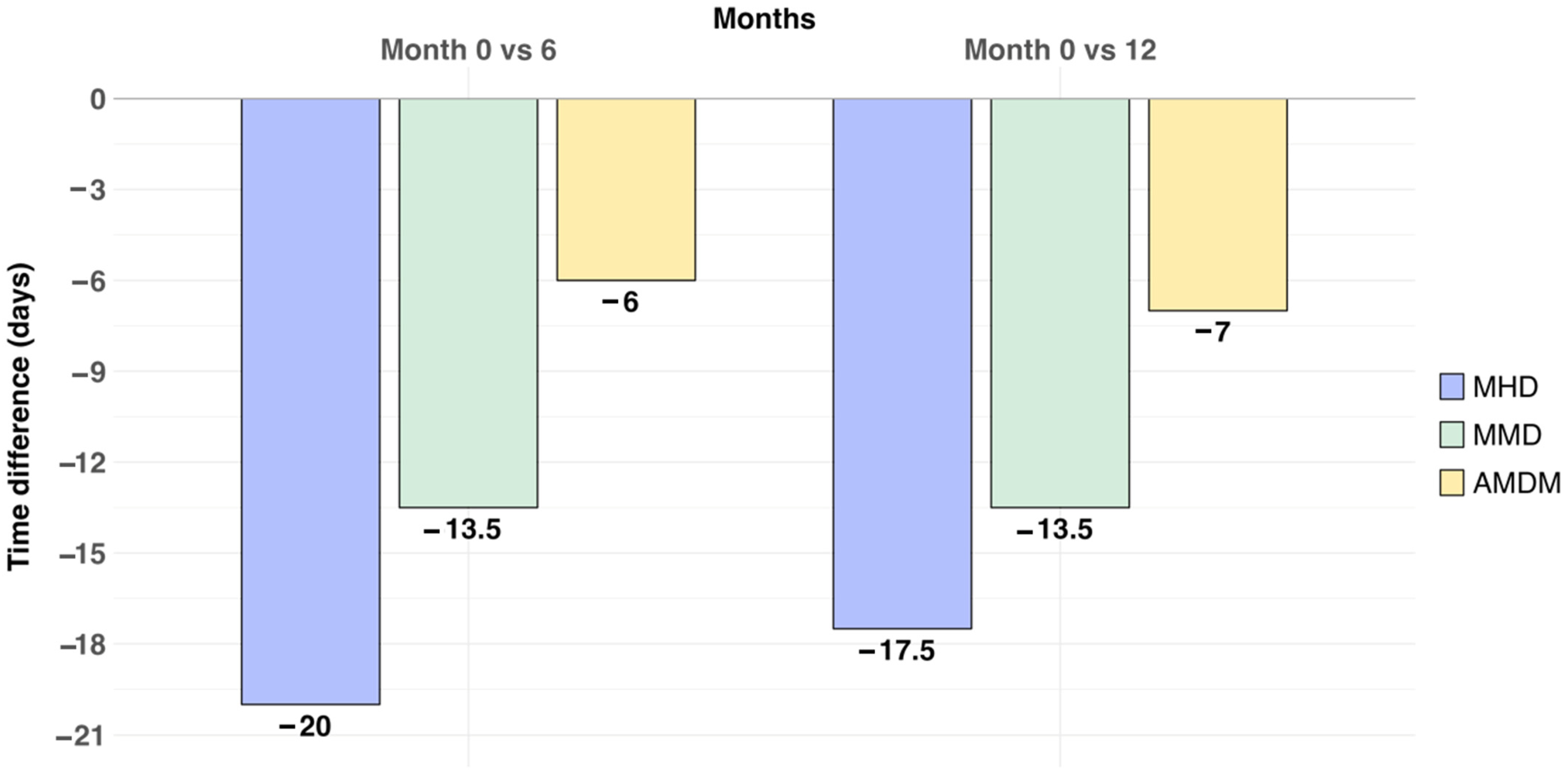
2.1.2. Effectiveness
2.1.3. Safety
2.2. Narrative Review
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Study Design, Population, and Outcomes
5.2. Statistical Analysis
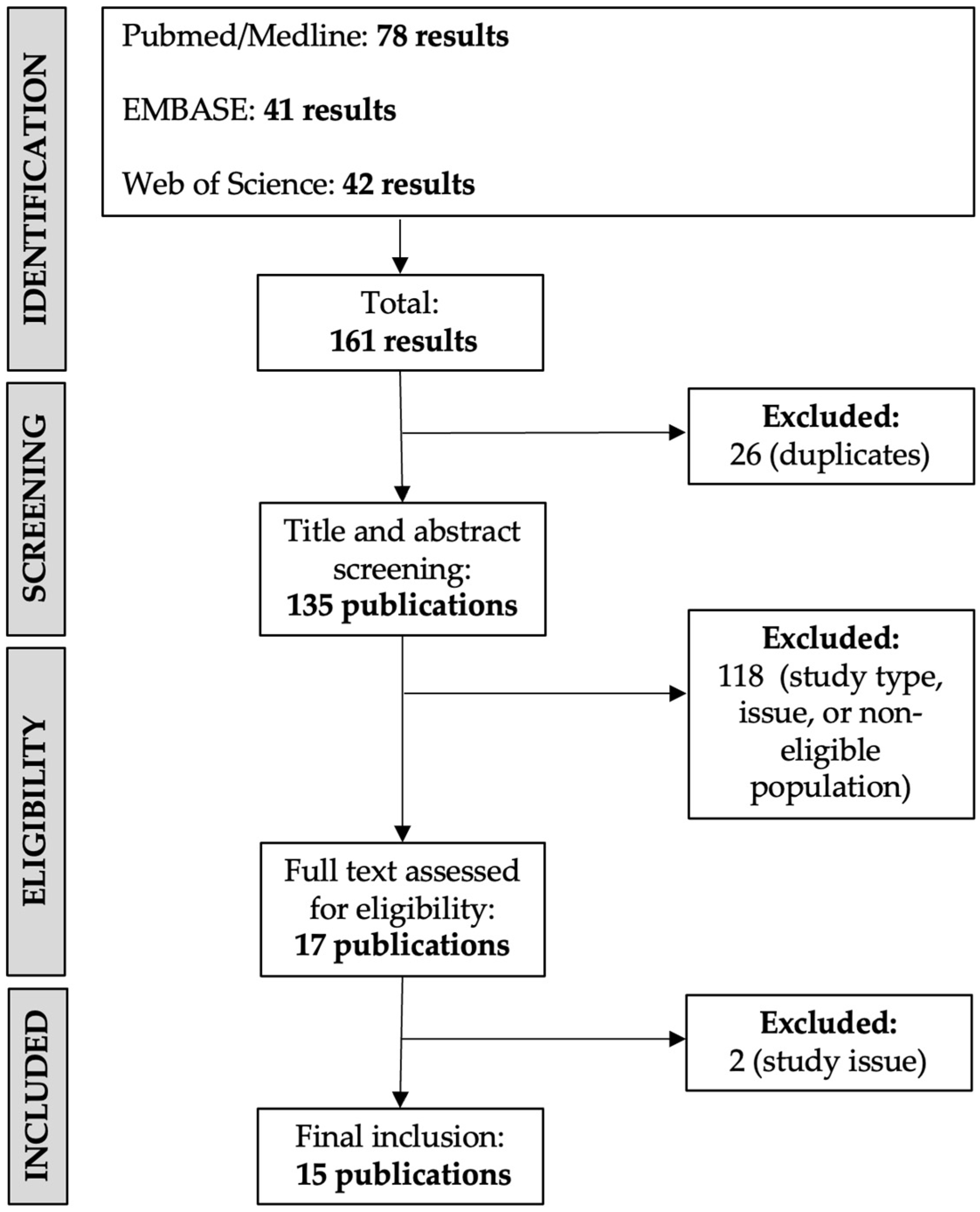
5.3. Narrative Review: Search Strategy and Study Selection
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AMDM | Acute medication days/month |
| BAI | Beck Anxiety Inventory Scale |
| BDI | Beck Depression Inventory |
| BTX-A | OnabotulinumtoxinA |
| CM | Chronic migraine |
| IQR | Interquartile range |
| ICHD-3 | International Classification of Headache Disorders |
| MHD | Monthly headache days |
| MMD | Monthly migraine days |
| RCT | Randomized clinical trial |
| PBO | Placebo |
| U | Unit |
References
- Onofri, A.; Pensato, U.; Rosignoli, C.; Wells-Gatnik, W.; Stanyer, E.; Ornello, R.; Chen, H.Z.; De Santis, F.; Torrente, A.; Mikulenka, P.; et al. European Headache Federation School of Advanced Studies (EHF-SAS). Primary headache epidemiology in children and adolescents: A systematic review and meta-analysis. J. Headache Pain. 2023, 24, 8. [Google Scholar] [CrossRef]
- Victor, T.W.; Hu, X.; Campbell, J.C.; Buse, D.C.; Lipton, R.B. Migraine prevalence by age and sex in the United States: A life-span study. Cephalalgia 2010, 30, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
- Alashqar, A.; Shuaibi, S.; Ahmed, S.F.; AlThufairi, H.; Owayed, S.; AlHamdan, F.; Alroughani, R.; Al-Hashel, J.Y. Impact of Puberty in Girls on Prevalence of Primary Headache Disorder Among Female Schoolchildren in Kuwait. Front. Neurol. 2020, 11, 594. [Google Scholar] [CrossRef] [PubMed]
- Torres-Ferus, M.; Vila-Sala, C.; Quintana, M.; Ajanovic, S.; Gallardo, V.J.; Gomez, J.B.; Alvarez-Sabin, J.; Macaya, A.; Pozo-Rosich, P. Headache, comorbidities and lifestyle in an adolescent population (The TEENs Study). Cephalalgia 2019, 39, 91–99. [Google Scholar] [CrossRef]
- Shimomura, H.; Tokunaga, S.; Taniguchi, N.; Inoue, K.; Okuda, M.; Kato, T.; Takeshima, Y. Emotional and behavioral problems in pediatric patients with migraine and tension-type headache. Brain Dev. 2021, 43, 826–832. [Google Scholar] [CrossRef]
- Hommer, R.; Lateef, T.; He, J.P.; Merikangas, K. Headache and mental disorders in a nationally representative sample of American youth. Eur. Child. Adolesc. Psychiatry 2022, 31, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Bektaş, Ö.; Uğur, C.; Gençtürk, Z.B.; Aysev, A.; Sireli, Ö.; Deda, G. Relationship of childhood headaches with preferences in leisure time activities, depression, anxiety and eating habits: A population-based, cross-sectional study. Cephalalgia 2015, 35, 527–537. [Google Scholar] [CrossRef]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Oskoui, M.; Pringsheim, T.; Billinghurst, L.; Potrebic, S.; Gersz, E.M.; Gloss, D.; Holler-Managan, Y.; Leininger, E.; Licking, N.; Mack, K.; et al. Practice guideline update summary: Pharmacologic treatment for pediatric migraine prevention: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology and the American Headache Society. Neurology 2019, 93, 500–509. [Google Scholar] [CrossRef]
- Antonaci, F.; Voiticovschi-Iosob, C.; Di Stefano, A.L.; Galli, F.; Ozge, A.; Balottin, U. The evolution of headache from childhood to adulthood: A review of the literature. J. Headache Pain. 2014, 15, 15. [Google Scholar] [CrossRef]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. PREEMPT 1 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; DeGryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F.; PREEMPT 2 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Lanteri-Minet, M.; Ducros, A.; Francois, C.; Olewinska, E.; Nikodem, M.; Dupont-Benjamin, L. Effectiveness of onabotulinumtoxinA (BOTOX®) for the preventive treatment of chronic migraine: A meta-analysis on 10 years of real-world data. Cephalalgia 2022, 42, 1543–1564. [Google Scholar] [CrossRef] [PubMed]
- Rothrock, J.F.; Adams, A.M.; Lipton, R.B.; Silberstein, S.D.; Jo, E.; Zhao, X.; Blumenfeld, A.M.; on behalf of the FORWARD Study investigative group. FORWARD Study: Evaluating the Comparative Effectiveness of Onabotulinumtoxina and Topiramate for Headache Prevention in Adults With Chronic Migraine. Headache 2019, 59, 1700–1713. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, A.M.; Stark, R.J.; Freeman, M.C.; Orejudos, A.; Manack Adams, A. Long-term study of the efficacy and safety of OnabotulinumtoxinA for the prevention of chronic migraine: COMPEL study. J. Headache Pain. 2018, 19, 13. [Google Scholar] [CrossRef] [PubMed]
- Winner, P.K.; Kabbouche, M.; Yonker, M.; Wangsadipura, V.; Lum, A.; Brin, M.F. A Randomized Trial to Evaluate OnabotulinumtoxinA for Prevention of Headaches in Adolescents With Chronic Migraine. Headache 2020, 60, 564–575. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Calderon, M.D.; Crain, N.; Pham, J.; Rinehart, J. Effectiveness of onabotulinumtoxinA (BOTOX) in pediatric patients experiencing migraines: A randomized, double-blinded, placebo-controlled crossover study in the pediatric pain population. Reg. Anesth. Pain. Med. 2021, 46, 41–48. [Google Scholar] [CrossRef]
- Papetti, L.; Frattale, I.; Ursitti, F.; Sforza, G.; Monte, G.; Ferilli, M.A.N.; Tarantino, S.; Proietti Checchi, M.; Valeriani, M. Real Life Data on OnabotulinumtoxinA for Treatment of Chronic Migraine in Pediatric Age. J. Clin. Med. 2023, 12, 1802. [Google Scholar] [CrossRef] [PubMed]
- Goenka, A.; Yu, S.G.; George, M.C.; Chikkannaiah, M.; MacDonald, S.; Stolfi, A.; Kumar, G. Is Botox Right for Me: When to Assess the Efficacy of the Botox Injection for Chronic Migraine in Pediatric Population. Neuropediatrics 2022, 53, 344–350. [Google Scholar] [CrossRef]
- Karian, V.; Morton, H.; Schefter, Z.J.; Smith, A.; Rogan, H.; Morse, B.; LeBel, A. OnabotulinumtoxinA for Pediatric Migraine. Pain. Manag. Nurs. 2023, 24, 610–616. [Google Scholar] [CrossRef]
- Schroeder, A.S.; Huss, K.; Blaschek, A.; Koerte, I.K.; Zeycan, B.; Roser, T.; Langhagen, T.; Schwerin, A.; Berweck, S.; Reilich, P.; et al. Ten-year follow-up in a case series of integrative botulinum toxin intervention in adolescents with chronic daily headache and associated muscle pain. Neuropediatrics 2012, 43, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Santana, L.; Liu, C. Experience of Botulinum Toxin A Injections for Chronic Migraine Headaches in a Pediatric Chronic Pain Clinic. J. Pediatr. Pharmacol. Ther. 2021, 26, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Calderon, M.D.; Wu WDer Grant, J.; Rinehart, J. Onabotulinumtoxin A (BOTOX®) for ProphylaCTIC Treatment of Pediatric Migraine: A Retrospective Longitudinal Analysis. J. Child. Neurol. 2018, 33, 580–586. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.S.; Bragin, I.; Rende, E.; Mejico, L.; Werner, K.E. Further Evidence that Onabotulinum Toxin is a Viable Treatment Option for Pediatric Chronic Migraine Patients. Cureus 2019, 11, e4343. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.Y.; Garza, I.; Dodick, D.W.; Robertson, C.E. The Effect of OnabotulinumtoxinA on Aura Frequency and Severity in Patients With Hemiplegic Migraine: Case Series of 11 Patients. Headache 2018, 58, 973–985. [Google Scholar] [CrossRef] [PubMed]
- Oliver, J.D.; Boesch, R.P.; Mack, K.J. Decreased Pulmonary Function During Botulinum Toxin A Therapy for Chronic Migraines in a 17-Year-Old Female. Headache 2018, 58, 1259–1261. [Google Scholar] [CrossRef] [PubMed]
- Goenka, A.; Yu, S.G.; Chikkannaiah, M.; George, M.C.; MacDonald, S.; Stolfi, A.; Kumar, G. Generalized Anxiety Disorder: A Predictor for Poor Responsiveness to Botulinum Toxin Type A Therapy for Pediatric Migraine. Pediatr. Neurol. 2022, 130, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, K.; Oas, K.H.; Mack, K.J.; Garza, I. Experience with botulinum toxin type A in medically intractable pediatric chronic daily headache. Pediatr. Neurol. 2010, 43, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Chan, V.W.; Mccabe, E.J.; Macgregor, D.L. Botox treatment for migraine and chronic daily headache in adolescents. J. Neurosci. Nurs. 2009, 41, 235–243. [Google Scholar] [CrossRef]
- Blumenfeld, A.; Silberstein, S.D.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; Binder, W.J. Method of injection of onabotulinumtoxinA for chronic migraine: A safe, well-tolerated, and effective treatment paradigm based on the PREEMPT clinical program. Headache 2010, 50, 1406–1418. [Google Scholar] [CrossRef]
- Ashina, S.; Terwindt, G.M.; Steiner, T.J.; Lee, M.J.; Porreca, F.; Tassorelli, C.; Schwedt, T.J.; Jensen, R.H.; Diener, H.C.; Lipton, R.B. Medication overuse headache. Nat. Rev. Dis. Primers 2023, 9, 5. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018, 38, 1–211. [Google Scholar]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed]
- Bero, L.; Chartres, N.; Diong, J.; Fabbri, A.; Ghersi, D.; Lam, J.; Lau, A.; McDonald, S.; Mintzes, B.; Sutton, P.; et al. The risk of bias in observational studies of exposures (ROBINS-E) tool: Concerns arising from application to observational studies of exposures. Syst. Rev. 2018, 7, 242. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
| Baseline Characteristics | |
|---|---|
| Age, years, median [IQR] | 15 [14.75, 17] |
| Gender, female, n (%) | 14 (70%) |
| Migraine onset age, median [IQR] | 12 [8, 14] |
| Migraine diagnosis age, median [IQR] | 15 [14, 16] |
| Migraine age of chronification, median [IQR] | 14 [12.5–15.5] |
| Aura, n (%) | 1 (5%) |
| Hypertension, n (%) | 0 (0%) |
| Obesity, n (%) | 1 (5%) |
| Anxiety, n (%) | 2 (10%) |
| Depression, n (%) | 3 (15%) |
| Cardiovascular disease, n (%) | 0 (0%) |
| Neurovascular disease, n (%) | 0 (0%) |
| MHD, days/month, median [IQR] | 28 [20, 28] |
| MMD, days/month, median [IQR] | 18 [10, 28] |
| AMDM, days/month, median [IQR] | 10 [7.5, 21.25] |
| Failed preventive treatments, n (%) | 19 (95%) |
| Beta-blockers | 5 (25%) |
| Antidepressants | 15 (75%) |
| Neuromodulators | 5 (25%) |
| Calcium channel blockers | 9 (45%) |
| Angiotensin receptor blockers | 1 (5%) |
| Number of treatments failed, n (%) | |
| 1 class | 9 (45%) |
| 2 classes | 5 (25%) |
| 3 classes | 3 (15%) |
| 4 classes | 2 (10%) |
| Other ongoing treatments, n (%) | 4 (20%) |
| Beta-blockers | 1 (5%) |
| Antidepressants | 3 (15%) |
| Neuromodulators | 0 (0%) |
| Calcium channel blockers | 0 (0%) |
| Angiotensin receptor blockers | 0 (0%) |
| Ref | Type of Study | Study Participants | Primary Outcome | Result | Risk of Bias |
|---|---|---|---|---|---|
| [16] | RCT of one dose of BTX-A (155 U or 74 U) versus PBO | N = 125 randomized patients with CM, 115/125 (92%) completed the study Age 15.1 (±1.5 years) Female 98/125 (78.4%) Follow-up: 3 months | Change in frequency of headache days from baseline at week 12 | All treatments reduced frequency with no significant differences between them: −6.3 (−8.5, −4.2) in BTX-A 155 U; −6.4 (−8.8, −4.0) in BTX-A 75 U; PBO −6.8 (−9.6, −4.1) in PBO; p ≥ 0.474. | Selection bias: low Performance bias: low Detection bias: low Attrition bias: low Reporting bias: low Overall risk of bias: low |
| [17] | 2-phase RCT (double-blind and open-label) of 155 U BTX-A (PREEMPT protocol) versus PBO | N = 15 patients with CM. 11/15 received three BTX-A treatmentsAge 15 (±1 year) Female 13/15 (87%) Follow-up: 6 weeks | To evaluate efficacy of BTX-A (reduction in frequency, intensity, duration, and disability) in patients with CM versus PBO. | Reduction in frequency (20 (7 to 17) vs. 28 (23 to 28); p = 0.038), intensity (5 (3 to 7) vs. 7 (5 to 9); p = 0.047) and disability (PedMIDAS 3 (2 to 4) vs. 4 (4 to 4); p = 0.047). No significant headache duration difference (10 (2 to 24) vs. 24 (4 to 24); p = 0.148). | Selection bias: unclear risk Performance bias: low Detection bias: low Attrition bias: low Reporting bias: low Overall risk of bias: low |
| [18] | Retrospective study of prospective case series of CM treated with BTX-A 155–195 U (PREEMPT protocol) | N = 46 CM patients (analysis performed on 43/46) Age 14.7 (±1.5 years) Female 37/46 (80.4%) Follow-up: 17.6 ± 13.7 months | Change in MHD from BL during 3 cycles of BTX-A | 68% had a significant reduction in the frequency of MHD within the 3 cycles, and 45% were responders (reduction ≥ 50% in MHD). | Due to confounding: high Measurement of the exposure: low In selection: high In post-exposure interventions: low Due to missing data: low In measurements of outcomes: low In selection of the reported result: low Overall risk of bias: high |
| [19] | Retrospective and prospective case series of CM treated with 155 U BTX-A (PREEMPT protocol) | N = 56 CM patients (analysis performed on 34/56) Age 17.5 (±2 years). 3/34 patients from 19–29 years Female 30/34 (88.2%) Follow-up: 9 months | To analyze the efficacy of BTX-A (reduction in headache frequency ≥ 50% and intensity) and reasons for discontinuation | 73% of responders (25/34 ≥ 50% reduction in frequency). A reduction in intensity with each additional BTX-A dose was observed (BL VAS 8.3 ± 0.8 vs. 4th dose 3.4 ± 1.4; p < 0.001). Discontinuation in 22/34 (11/22 moving out of the area, 3/22 minor side-effects and 8/22 non-response). | Due to confounding: high Measurement of the exposure: low In selection: high In post-exposure interventions: SC Due to missing data: SC In measurements of outcomes: low In selection of the reported result: low Overall risk of bias: high |
| [20] | Retrospective chart review on patients with CM with ≥ 2 BTX-A administrations (doses not specified) | N = 32 patients with CM Age 16.09 (±1 year) Female 30/32 (93.8%) Follow-up: not clearly specified | Comparison of headache frequency, intensity and duration across BL, first and second BTX-A Inj | Reduction in frequency (mean reduction of 6.5 days between BL and Inj1 (p < 0.01); 7 days between BL and Inj2 (p <0.01)) and intensity (BL 6.8 ± 1.51; Inj1 6.17 ± 2.12; Inj2 5.52 ± 6.2; p = 0.003). No significant reduction in duration. | Due to confounding: high Measurement of the exposure: high In selection: high In post-exposure interventions: low Due to missing data: SC In measurements of outcomes: low In selection of the reported result: SC Overall risk of bias: high |
| [21] | Retrospective case series of patients with CDH with “StiBo” approach +. Mean total BTX-A dose 32.7 U (20–90 U). | N = 5 patients (1 lost follow-up) Age 13 (±2.4 years) Female 4/5 (80%) Follow-up: 17 months | Long-term evaluation (10 year) of StiBo project regarding headache | Reduction in headache frequency from 20 (15–30) to 5 (0–15) and headache intensity (VAS) from 6.6 (6–8) to 2.4 (0–5). | Due to confounding: high Measurement of the exposure: low In selection: high In post-exposure interventions: SC Due to missing data: high In measurements of outcomes: high In selection of the reported: SC Overall risk of bias: high |
| [22] | Retrospective case series of patients with CM. Mean BTX 173.23 ± 35.03 U (PREEMPT protocol) | N = 65 patients with CM. Age 15 (11–18 years) Female % not known. Follow-up: 6 weeks | To analyze tolerability, side effects and pain scores (VAS) of BTX-A | 2/65 patients presented mild side effects (1/2 not related to BTX-A). Significant reduction in pain score with an average pain score decrease of 5.2 ± 2.2 on VAS. | Due to confounding: high Measurement of the exposure: low In selection: high In post-exposure interventions: low Due to missing data: high In measurements of outcomes: SC In selection of the reported result: lowOverall risk of bias: high |
| [23] | Retrospective chart review of refractory CM treated with BTX-A 155–215 U (PREEMPT protocol) | N= 10 patients with refractory migraine ‡ Age 15.1 (±2.95 years) Female 7/10 (70%)Follow up: 2.5 years. | Decrease in frequency (MHD), duration and intensity of migraine episodes with BTX-A compared to pretreatment | Reduction in frequency (15 (8 to 29) vs. 4 (2 to 10); p < 0.0001), intensity (6 (4 to 8) vs. 4 (2 to 5); p = 0.0063) and duration in hours (8 (0 to 24) vs. 0.8 (0.3 to 7); p = 0.025). | Due to confounding: high Measurement of the exposure: low In selection: high In post-exposure interventions: low Due to missing data: high In measurements of outcomes: low In selection of the reported result: SC Overall risk of bias: high |
| [24] | Retrospective cohort of adolescents with CM treated with BTX-A 155 U–185 U (PREEMPT protocol) | N = 30 patients with CM Age 16.5 (±1.83 years) Female 24/30 (80%) Follow-up: 12–24 months | To analyze response in terms of intensity and frequency of BTX-A in children with CM | Significant reduction in headache intensity (VAS 7.47 ± 1.89 to 4.34 ± 3.02; p < 0.001) and frequency (24.4 ± 7.49 to 14.8 ± 12.52 MHD; p < 0.001). | Due to confounding: high Measurement of the exposure: low In selection: high In post-exposure interventions: low Due to missing data: low In measurements of outcomes: SC In selection of the reported: low Overall risk of bias: high |
| [25] | Retrospective case series of 11 patients with CM. Pediatric patient treated with BTX-A 155–200 U standard fixed-site protocol | N = 1/11 pediatric patient 16-year-old female with CM Follow-up: 1 year | Description of effectiveness of BTX-A in a patient with CM | Reduction in severe migraine headaches preceded by visual and motor aura (severe headaches reduced to 8 days per month, and severe motor aura from 3/week to 1/3 months). | Due to confounding: NI Measurement of the exposure: low In selection: high In post-exposure interventions: low Due to missing data: high In measurements of outcomes: high In selection of the reported result: low Overall risk of bias: high |
| [26] | Case report patient with CM; 150 U BTX-A | N = 1 patient 15 years old female with CM Follow-up: 24 months | Description of progressively decreasing pulmonary function during BTX-A administration | FVC from 109% to 55% over 24 months; Pulmonary function recovered immediately after discontinuation of BTX-A therapy. | Due to confounding: NI Measurement of the exposure: lLow In selection: H high In post-exposure interventions: lLow Due to missing data: hHigh In measurements of outcomes: Hhigh In selection of the reported result: SC Overall risk of bias: hHigh |
| [27] | Retrospective and prospective case series of CM treated with 155 U BTX-A (PREEMPT protocol) | N = 56 CM patients (analysis performed on 34/56). Age 17.5 (±2 years) Female 30/34 (88.2%) Follow-up: 9 months Same cohort (23) but different primary endpoint. | To evaluate the effectiveness of BTX-A and the impact of comorbidity (anxiety) on its response | GAD-7 score greater than 15 was significantly higher in non-responders (67%) vs. responders (42%); p = 0.040. | Due to confounding: high Measurement of the exposure: low In selection: high In post-exposure interventions: SC Due to missing data: SC In measurements of outcomes: low In selection of the reported result: low Overall risk of bias: high |
| [28] | Retrospective case series of CDH treated with BTX-A 100 U fixed Inj sites | N = 10 patients (5 with CM). Age 15.5 (SD not available). Female 7/10 (70%). Follow-up: not clearly specified | Description of tolerability and effectiveness of BTX-A in intractable pediatric patients with CDH | No serious AE, 3/10 minor events. 4/10 (40%) clinically meaningful reliefs of headache symptoms. 3/5 (60%) patients with CM were responders in terms of intensity (3/3 40–50% reduction) and/or frequency (2/3; 40–50% reduction); p not available | Due to confounding: high Measurement of the exposure: low In selection: high In post-exposure interventions: low Due to missing data: high In measurements of outcomes: high In selection of the reported result: SC Overall risk of bias: high |
| [29] | Qualitative review of patients with CM treated with 100 U BTX following a combination of fixed-site and follow-the-pain pattern (9–63 Inj sites) | N = 12 patients with CM (analysis performed on 6/10 with long-term BTX-A) Age 14.8–18.1 years Female 6/6 (100%) Follow-up: 3–29 months | Decrease in headache frequency, pain intensity and/or duration of headache. Evaluation of headache in QoL | 6/6 had a reduction in migraine frequency days (variable) and 3/6 a decrease in intensity. 25% improvement in the total scores of MSQOL (although comparison scores prior to starting BTX and at 3 months failed to reach significance). | Due to confounding: high Measurement of the exposure: SC In selection: high In post-exposure interventions: SC Due to missing data: high In measurements of outcomes: high In selection of the reported result: SC Overall risk of bias: high |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Dabó, L.; Caronna, E.; Mas-de-les-Valls, R.; Gallardo, V.J.; Alpuente, A.; Torres-Ferrus, M.; Pozo-Rosich, P. Effectiveness and Safety of OnabotulinumtoxinA in Adolescent Patients with Chronic Migraine. Toxins 2024, 16, 221. https://doi.org/10.3390/toxins16050221
Gómez-Dabó L, Caronna E, Mas-de-les-Valls R, Gallardo VJ, Alpuente A, Torres-Ferrus M, Pozo-Rosich P. Effectiveness and Safety of OnabotulinumtoxinA in Adolescent Patients with Chronic Migraine. Toxins. 2024; 16(5):221. https://doi.org/10.3390/toxins16050221
Chicago/Turabian StyleGómez-Dabó, Laura, Edoardo Caronna, Rut Mas-de-les-Valls, Víctor J. Gallardo, Alicia Alpuente, Marta Torres-Ferrus, and Patricia Pozo-Rosich. 2024. "Effectiveness and Safety of OnabotulinumtoxinA in Adolescent Patients with Chronic Migraine" Toxins 16, no. 5: 221. https://doi.org/10.3390/toxins16050221
APA StyleGómez-Dabó, L., Caronna, E., Mas-de-les-Valls, R., Gallardo, V. J., Alpuente, A., Torres-Ferrus, M., & Pozo-Rosich, P. (2024). Effectiveness and Safety of OnabotulinumtoxinA in Adolescent Patients with Chronic Migraine. Toxins, 16(5), 221. https://doi.org/10.3390/toxins16050221