Snakebites in Cameroon: Tolerance of a Snake Antivenom (Inoserp™ PAN-AFRICA) in Africa in Real-Life Conditions


 , , ,
, , ,
Abstract
1. Introduction
2. Results
Tolerance
3. Discussion
4. Conclusions
5. Materials and Methods
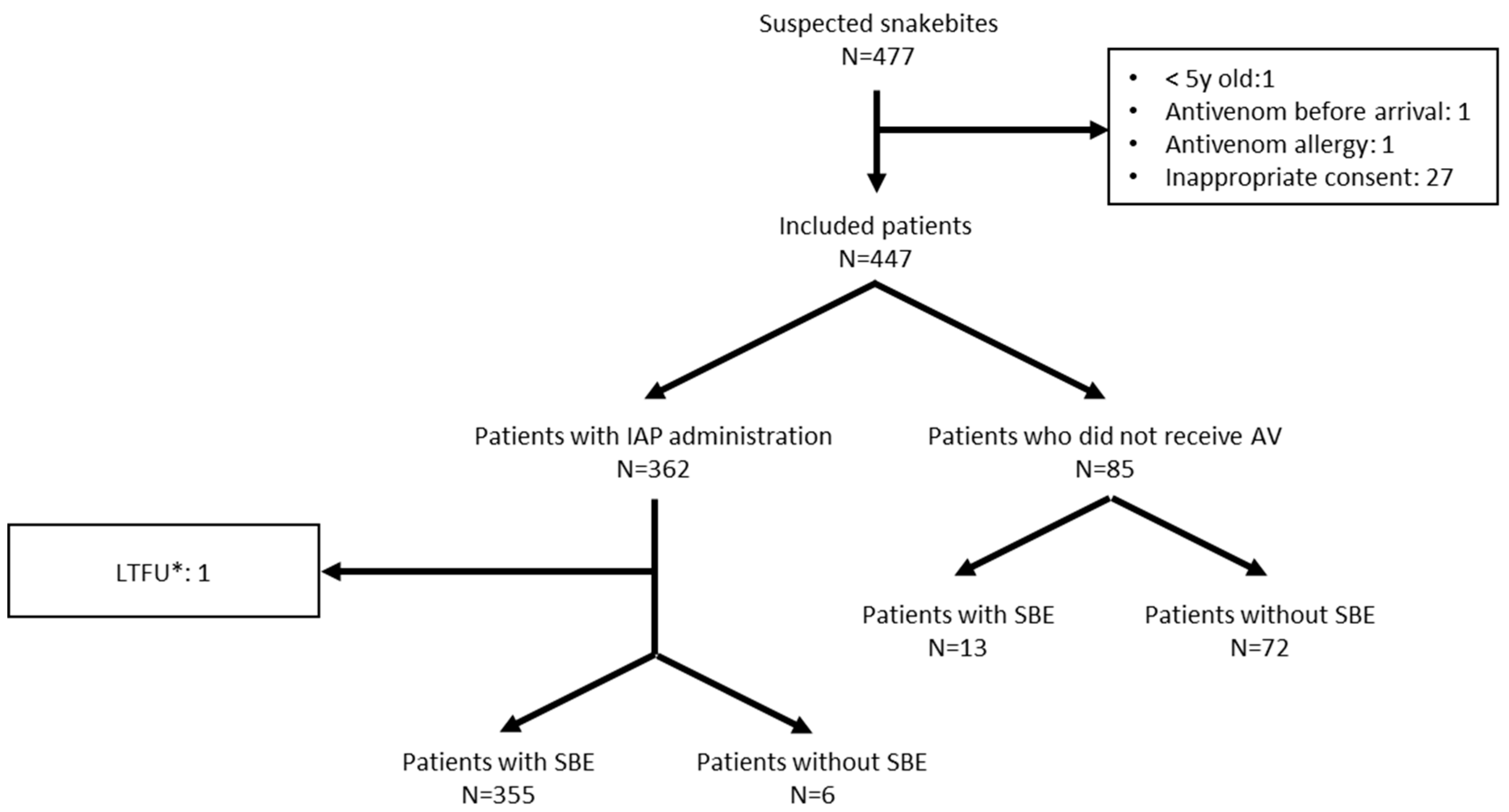
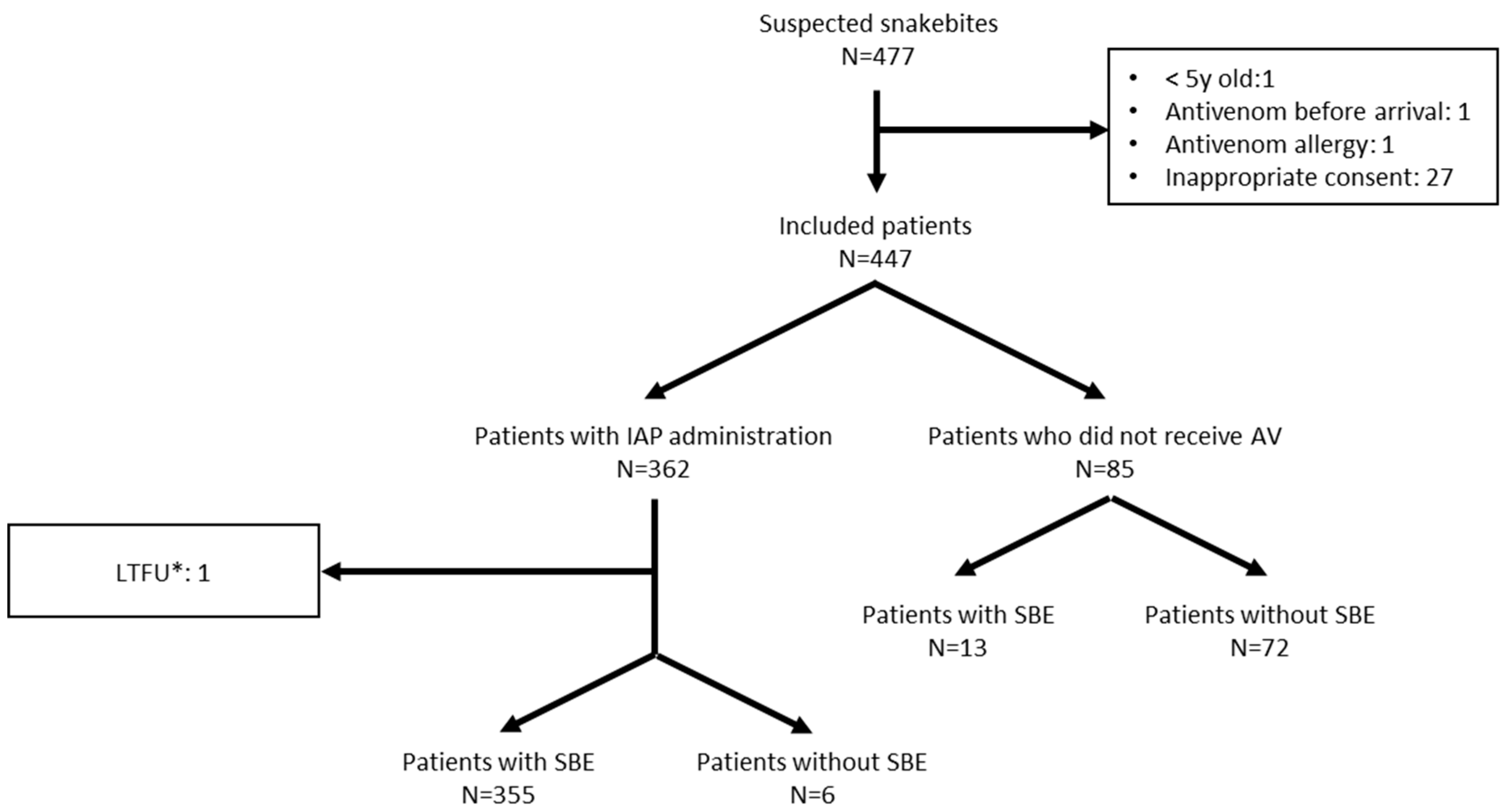
5.1. Population
5.2. Sample Size
5.3. Inoserp™ PAN-AFRICA
5.4. Assessment of Tolerance
- -
- Occurrence of any of the following symptoms: pruritus, urticaria, laryngeal edema, angioedema, bronchospasm, tachycardia/bradycardia, drop in blood pressure (systolic blood pressure < 70 mmHg for children aged five to ten years; <90 mmHg for patients older than ten), anaphylactic shock;
- -
- Onset of fever (axillary temperature ≥ 37.5 °C);
- -
- Digestive disorders (nausea, vomiting, diarrhea, abdominal cramps);
- -
- Agitation, severe headache, or confusion.
5.5. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
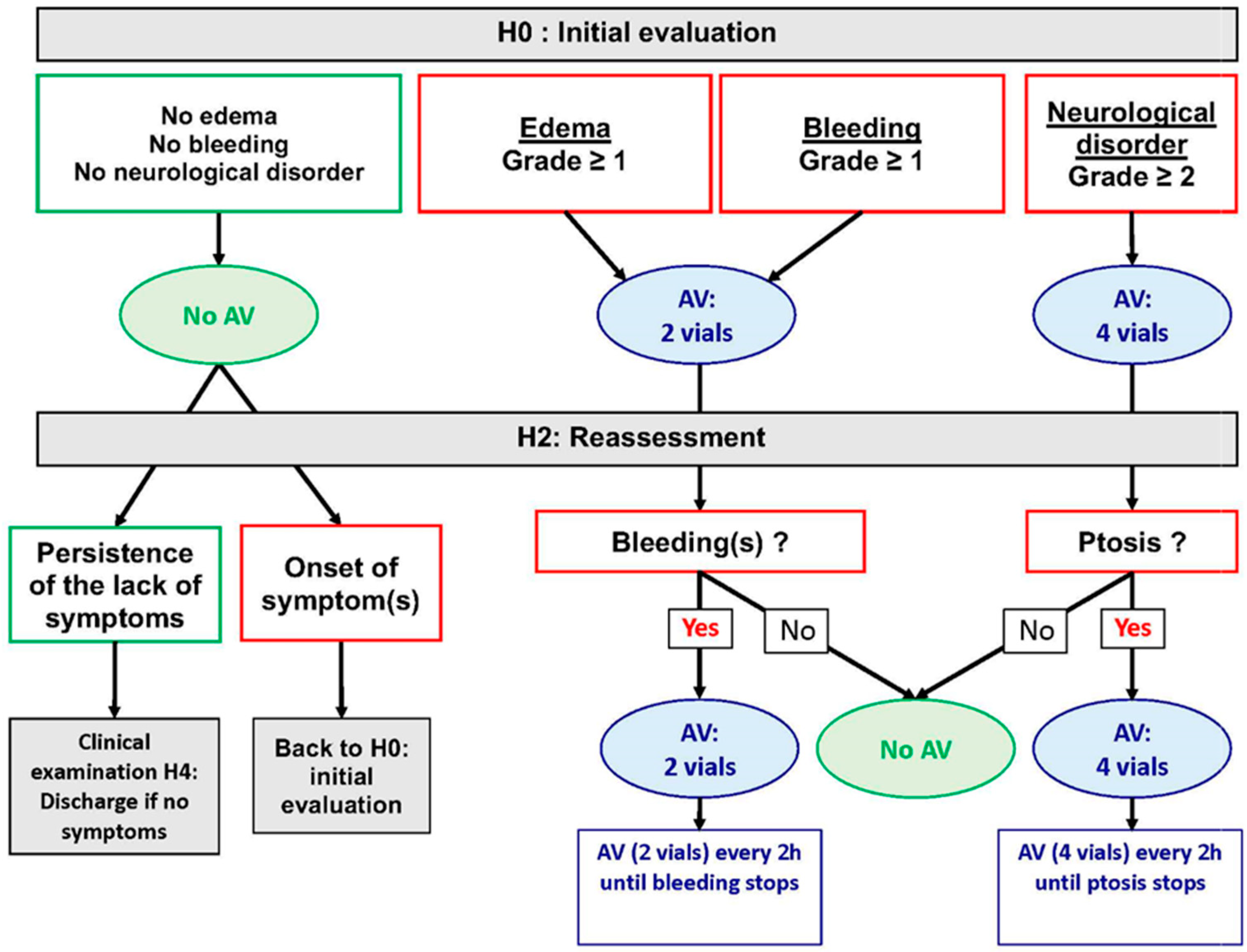
Appendix A. Management Algorithm Recommended by Cameroonian Ministry of Envenomation Patients
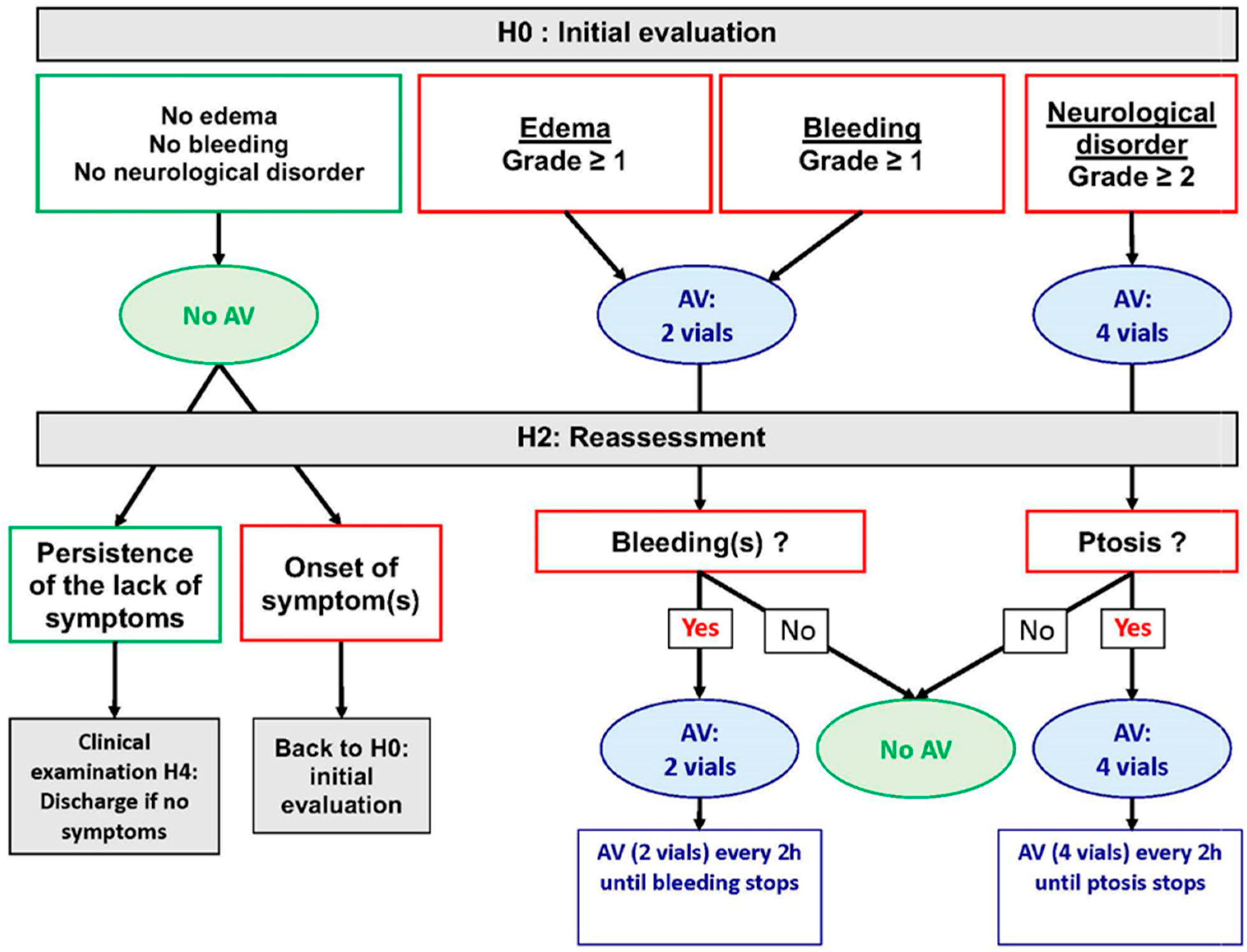
- 0.
- No edema.
- 1.
- Localized edema not exceeding the nearest joint.
- 2.
- Progressive edema not exceeding 2 contiguous joints.
- 3.
- Extensive edema not exceeding the root of the limb.
- 4.
- Edema extending beyond the root of the limb (hydrops).
- 0.
- No bleeding.
- 1.
- Persistent local bleeding at fang marks for more than one hour.
- 2.
- Bleeding from the gums, nose, scars, and recent wounds.
- 3.
- Ecchymosis, hematoma, purpura, phlyctens.
- 4.
- Internal hemorrhage (peritoneal, meningeal, metrorrhagia, hematemesis, etc.).
- 0.
- No neurological disorder.
- 1.
- Local anesthesia, tingling affecting the bitten limb.
- 2.
- Profuse sweat, saliva and vomiting, miosis.
- 3.
- Bilateral ptosis (±speech, vision, hearing and/or swallowing disorders).
- 4.
- Respiratory distress, impossibility to communicate.
Appendix B. List of Snakes for Which the IPA Is Effective (in Bold, Snake Species Present in Cameroon)
- -
- Echis ocellatus;
- -
- Echis leucogaster;
- -
- Echis pyramidum;
- -
- Bitis arietans;
- -
- Bitis rhinoceros;
- -
- Bitis nasicornis;
- -
- Bitis gabonica.
- -
- Dendroaspis polylepis;
- -
- Dendroaspis viridis;
- -
- Dendroaspis angusticeps;
- -
- Dendroaspis jamesoni;
- -
- Naja nigricollis;
- -
- Naja melanoleuca;
- -
- Naja haje;
- -
- Naja pallida;
- -
- Naja nubiae;
- -
- Naja katiensis;
- -
- Naja senegalensis.
Appendix C. Naranjo Algorithm

{kind=link}
{kind=link}
| Question | Yes | No | Don’t Know |
|---|---|---|---|
| 1. Are there previous conclusion reports on this reaction? | 1 | 0 | 0 |
| 2. Did the adverse event appear after the suspect drug was administered? | 2 | −1 | 0 |
| 3. Did the AR improve when the drug was discontinued or a specific antagonist was administered? | 1 | 0 | 0 |
| 4. Did the AR reappear when drug was readministered? | 2 | −1 | 0 |
| 5. Are there alternate causes [other than the drug] that could solely have caused the reaction? | −1 | 2 | 0 |
| 6. Did the reaction reappear when a placebo was given? | −1 | 1 | 0 |
| 7. Was the drug detected in the blood [or other fluids] in a concentration known to be toxic? | 1 | 0 | 0 |
| 8. Was the reaction more severe when the dose was increased or less severe when the dose was decreased? | 1 | 0 | 0 |
| 9. Did the patient have a similar reaction to the same or similar drugs in any previous exposure? | 1 | 0 | 0 |
| 10. Was the adverse event confirmed by objective evidence? | 1 | 0 | 0 |
| Score | Interpretation of Scores |
|---|---|
| Total Score ≥ 9 | Definite. The reaction (1) followed a reasonable temporal sequence after a drug or in which a toxic drug level had been established in body fluids or tissues, (2) followed a recognized response to the suspected drug, and (3) was confirmed by improvement on withdrawing the drug and reappeared on re-exposure. |
| Total Score 5–8 | Probable. The reaction (1) followed a reasonable temporal sequence after a drug, (2) followed a recognized response to the suspected drug, (3) was confirmed by withdrawal but not by exposure to the drug, and (4) could not be reasonably explained by the known characteristics of the patient’s clinical state. |
| Total Score 1–4 | Possible. The reaction (1) followed a temporal sequence after a drug, (2) possibly followed a recognized pattern to the suspected drug, and (3) could be explained by characteristics of the patient’s disease. |
| Total Score ≤ 0 | Doubtful. The reaction was likely related to factors other than a drug. |
References
- Williams, D.J.; Abul Faiz, M.; Abela-Ridder, B.; Ainsworth, S.; Bulfone, T.C.; Nickerson, A.D.; Habib, A.G.; Junghanss, T.; Fan, H.W.; Turner, M.; et al. Strategy for a globally coordinated response to a priority neglected tropical disease: Snakebite envenoming. PLoS Negl. Trop. Dis. 2019, 13, e0007059. [Google Scholar] [CrossRef] [PubMed]
- Chippaux, J.P. Estimate of the burden of snakebites in sub-Saharan Africa: A meta-analytic approach. Toxicon 2011, 57, 586–599. [Google Scholar] [CrossRef] [PubMed]
- Tchoffo, D.; Kamgno, J.; Kekeunou, S.; Yadufashije, C.; Djeunga, H.C.N.; Nkwescheu, A.S. High snakebite underreporting rate in the Centre Region of Cameroon: An observational study. BMC Public Health 2019, 19, 1040. [Google Scholar] [CrossRef] [PubMed]
- Chippaux, J.P.; Stock, R.P.; Massougbodji, A. Antivenom Safety and Tolerance for the Strategy of Snake Envenomation Management. In Snake Venom Toxinology; Gopalakrishnakone, P., Inagaki, H., Mukherjee, A.K., Rahmy, T.R., Vogel, C.W., Eds.; Springer: Dordrecht, The Netherlands, 2017; pp. 475–495. [Google Scholar] [CrossRef]
- Harrison, R.A.; Hargreaves, A.; Wagstaff, S.C.; Faragher, B.; Lalloo, D.G. Snake Envenoming: A Disease of Poverty. PLoS Negl. Trop. Dis. 2009, 3, e569. [Google Scholar] [CrossRef] [PubMed]
- Alcoba, G.; Chabloz, M.; Eyong, J.; Wanda, F.; Ochoa, C.; Comte, E.; Nkwescheu, A.; Chappuis, F. Snakebite epidemiology and health-seeking behavior in Akonolinga health district, Cameroon: Cross-sectional study. PLoS Negl. Trop. Dis. 2020, 14, e0008334. [Google Scholar] [CrossRef] [PubMed]
- Chuat, M.; Alcoba, G.; Eyong, J.; Wanda, F.; Comte, E.; Nkwescheu, A.; Chappuis, F.; Hudelson, P. Dealing with snakebite in rural Cameroon: A qualitative investigation among victims and traditional healers. Toxicon X 2021, 9–10, 100072. [Google Scholar] [CrossRef] [PubMed]
- Potet, J.; Smith, J.; McIver, L. Reviewing evidence of the clinical effectiveness of commercially available antivenoms in sub-Saharan Africa identifies the need for a multi-centre, multi-antivenom clinical trial. PLoS Negl. Trop. Dis. 2019, 13, e0007551. [Google Scholar] [CrossRef] [PubMed]
- Chippaux, J.P.; Ntone, R.; Benhammou, D.; Madec, Y.; Noel, G.; Perilhou, A.; Karl, F.; Amta, P.; Sanchez, M.; Matchim, L.; et al. Real life condition evaluation of Inoserp PAN-AFRICA antivenom effectiveness in Cameroon. PLoS Negl. Trop. Dis. 2023, 17, e0011707. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, J.M.; Chippaux, J.P.; Jackson, K.; Ashe, S.; Tamou-Sambo, B.; Massougbodji, A.; Akpakpa, O.C.; Abo, B.N. Differential Diagnosis of an Unusual Snakebite Presentation in Benin: Dry Bite or Envenomation? J. Spec. Oper. Med. 2019, 19, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Mehta, S.R.; Sashindran, V.K. Clinical Features and Management of Snake Bite. Med. J. Armed Forces India 2002, 58, 247–249. [Google Scholar] [CrossRef] [PubMed]
- de Silva, H.A.; Ryan, N.M.; de Silva, H.J. Adverse reactions to snake antivenom, and their prevention and treatment. Br. J. Clin. Pharm. 2016, 81, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Naranjo, C.A.; Busto, U.; Sellers, E.M.; Sandor, P.; Ruiz, I.; Roberts, E.A.; Janecek, E.; Domecq, C.; Greenblatt, D.J. A method for estimating the probability of adverse drug reactions. Clin. Pharmacol. Ther. 1981, 30, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Shukla, A.K.; Jhaj, R.; Misra, S.; Ahmed, S.N.; Nanda, M.; Chaudhary, D. Agreement between WHO-UMC causality scale and the Naranjo algorithm for causality assessment of adverse drug reactions. J. Fam. Med. Prim. Care 2021, 10, 3303–3308. [Google Scholar] [CrossRef]
- LoVecchio, F.; Klemens, J.; Roundy, E.B.; Klemens, A. Serum sickness following administration of antivenin (Crotalidae) polyvalent in 181 cases of presumed rattlesnake envenomation. Wilderness Environ. Med. 2003, 14, 220–221. [Google Scholar] [CrossRef] [PubMed]
- Chippaux, J.P.; Balde, M.C.; Sessinou, E.; Yero Boiro, M.; Massougbodji, A. Evaluation of a new polyvalent antivenom against snakebite envenomation (Inoserp(R) Panafricain) in two different epidemiological settings: Northern Benin and Maritime Guinea. Med. Sante Trop. 2015, 25, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Lam, A.; Cabral, M.; Toure, A.; Ba, F.; Camara, B.; Kane, O.; Fall, M.; Diouf, A.; Chippaux, J.P. Evaluation of the efficacy and tolerance of Inoserp (R) Panafricain in Senegal. Toxicol. Anal. Clin. 2019, 31, 18–29. [Google Scholar] [CrossRef]
- Harris, P.A.; Taylor, R.; Minor, B.L.; Elliott, V.; Fernandez, M.; O’Neal, L.; McLeod, L.; Delacqua, G.; Delacqua, F.; Kirby, J.; et al. The REDCap consortium: Building an international community of software platform partners. J. Biomed. Inf. 2019, 95, 103208. [Google Scholar] [CrossRef] [PubMed]
- Harris, P.A.; Taylor, R.; Thielke, R.; Payne, J.; Gonzalez, N.; Conde, J.G. Research electronic data capture (REDCap)-A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inf. 2009, 42, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Leon, G.; Vargas, M.; Segura, A.; Herrera, M.; Villalta, M.; Sanchez, A.; Solano, G.; Gomez, A.; Sanchez, M.; Estrada, R.; et al. Current technology for the industrial manufacture of snake antivenoms. Toxicon 2018, 151, 63–73. [Google Scholar] [CrossRef] [PubMed]
| Total (N = 447) | Envenomation with AV Injection (N = 356) | Envenomation without AV Injection (N = 13) | No Envenomation with AV Injection (N = 6) | No Envenomation without AV Injection (N = 72) | p Value * | |
|---|---|---|---|---|---|---|
| Male, N (%) | 228 (51.0) | 182 (51.1) | 8 (61.5) | 6 (100.0) | 32 (44.4) | 0.049 |
| Age (years) | 0.72 | |||||
| Median (IIQ) | 25 (14–40) | 26 (14–40) | 35 (12–49) | 30 (21–37) | 23 (13.5–35.5) | |
| Statistical range | 5–89 | 5–87 | 5–63 | 20–47 | 5–89 | |
| Age group (years) | 0.37 | |||||
| 5–11 | 71 (15.9) | 58(16.3) | 3 (23.1) | - | 10 (13.9) | |
| 12–19 | 93 (20.81) | 70 (19.7) | 2 (15.4) | - | 21 (29.2) | |
| >19 | 283 (63.3) | 228 (64.0) | 8 (61.5) | 6 (100.0) | 41 (56.9) | |
| Medical history | 0.44 | |||||
| No | 436 (97.5%) | |||||
| At least one | 11 (2.5%) | 11 (4.5%) | 0 | 0 | 0 | |
| Region | 0.43 | |||||
| Far North | 202 (45.2) | 161 (45.2) | 8 (61.5) | 1 (16.7) | 32 (44.4) | |
| North | 74 (16.6) | 60 (16.9) | 1 (7.7) | - | 13 (18.1) | |
| Adamawa | 46 (10.3) | 38 (10.7) | - | - | 8 (11.1) | |
| Midwest | 125 (28.0) | 97 (27.3) | 4 (30.8) | 5 (83.3) | 19 (26.4) | |
| Snake family ** | <0.001 | |||||
| Elapidae | 10 (2.2) | 9 (2.5) | - | - | 1 (1.4) | |
| Viperidae | 104 (23.3) | 95 (26.7) | 1 (7.7) | - | 8 (11.1) | |
| Lamprophiidae | 6 (1.3) | 3 (0.8) | - | 1 (16.7) | 2 (2.8) | |
| Colubridae | 19 (4.3) | 13 (3.7) | - | - | 6 (8.3) | |
| Nonvenomous | 11 (2.5) | 3 (0.8) | 1 (7.7) § | 1 (16.7) | 6 (8.3) | |
| Not identified | 297 (66.4) | 233 (65.5) | 11 (84.6) | 4 (66.7) | 49 (68.1) |
| Before Antivenom (N = 361) | After Antivenom Injection * (N = 361) | ≤2 h after Initial Antivenom Injection * | >2 h after Initial Antivenom Injection * | Patients without Antivenom (N = 85) | p ** | |
|---|---|---|---|---|---|---|
| Severe signs | ||||||
| Laryngeal edema | - | - | - | - | - | - |
| Angioedema | - | 1 (0.3) | 1 (0.3) | - | - | 0.99 |
| Bronchospasm | 1 (0.3) | 1 (0.3) | - | 1 (0.3) | - | 0.99 |
| Cough | 3 (0.8) | 1 (0.3) | - | 1 (0.3) | - | 0.99 |
| Anaphylactic shock | - | - | - | - | - | - |
| Cutaneous symptoms | ||||||
| Pruritus | 5 (1.4) | 8 (2.2) | 4 (1.1) | 4 (1.1) | 1 (1.2) | 0.99 |
| Urticaria | 1 (0.3) | 6 (1.7) | 5 (1.4) | 1 (0.3) | - | 0.60 |
| Localized erythema | 12 (3.3) | 2 (0.6) | - | 2 (0.6) | 2 (2.4) | 0.17 |
| Diffuse erythema | 1 (0.3) | 2 (0.6) | 1 (0.3) | 1 (0.3) | - | 0.99 |
| Respiratory disorders | ||||||
| Dyspnea | 24 (6.6) | 3 (0.8) | 1 (0.3) | 2 (0.6) | 3 (3.5) | 0.09 |
| Stridor | 1 (0.3) | - | - | - | - | - |
| Cyanosis | 1 (0.3) | - | - | - | - | - |
| Hypoxemia | - | - | - | - | - | - |
| Digestive disorders | ||||||
| Nausea | 26 (7.2) | 8 (2.2) | 4 (1.1) | 4 (1.1) | 1 (1.2) | 0.99 |
| Vomiting | 34 (9.4) | 8 (2.2) | 5 (1.4) | 3 (0.8) | 1 (1.2) | 0.99 |
| Diarrhea | 9 (2.5) | 3 (0.8) | - | 3 (0.8) | 1 (1.2) | 0.57 |
| Abdominal pain | 7 (1.9) | 7 (1.9) | 3 (0.8) | 4 (1.1) | - | 0.36 |
| Other symptoms | ||||||
| Fever | 66 (18.3) | 86 (23.8) | 35 (9.7) | 51 (14.1) | 21 (24.7) | 0.86 |
| Blood pressure drop | 22 (6.1) | 19 (5.3) | 10 (2.8) | 9 (2.5) | 3 (3.5) | 0.78 |
| Tachycardia | 109 (30.2) | 40 (11.1) | 18 (5.0) | 22 (6.1) | 22 (25.9) | <0.001 |
| Bradycardia | 12 (3.3) | 34 (9.4) | 10 (2.8) | 24 (6.6) | 2 (2.4) | 0.031 |
| Myalgia | 129 (35.7) | 43 (11.9) | 27 (7.5) | 16 (4.4) | 10 (11.8) | 0.97 |
| Malaise | 10 (2.8) | 1 (0.3) | - | 1 (0.3) | - | 0.99 |
| Agitation | 21 (5.8) | 2 (0.6) | 1 (0.3) | 1 (0.3) | - | 0.99 |
| Headache | 14 (3.9) | 8 (2.2) | 4 (1.1) | 3 (0.8) | 1 (1.2) | 0.99 |
| Frisson | 6 (1.9) | 4 (1.1) | 3 (0.8) | 1 (0.3) | 1 (1.2) | 0.99 |
| Number of Patients with AE * after AV † Injection (n = 361) | Unlikely n (%) | Possible n (%) | Probable n (%) | Definite n (%) | |
|---|---|---|---|---|---|
| Laryngeal edema | - | ||||
| Angioedema | 1 (0.3) | 1 (0.3) | |||
| Bronchospasm | 1 (0.3) | 1 (0.3) | |||
| Cough | 1 (0.3) | 1 (0.3) | |||
| Anaphylactic shock | - | ||||
| Pruritus | 8 (2.2) | 1 (0.3) | 6 (1.7) | 1 (0.3) | |
| Urticaria | 6 (1.7) | 4 (1.1) | 2 (0.6) | ||
| Localized erythema | 2 (0.6) | 2 (0.6) | |||
| Diffuse erythema | 2 (0.6) | 2 (0.6) | |||
| Dyspnea | 3 (0.8) | 1 (0.3) | 2 (0.6) | ||
| Stridor | - | ||||
| Cyanosis | - | ||||
| Hypoxemia | - | ||||
| Nausea | 8 (2.2) | 4 (1.1) | 4 (1.1) | ||
| Vomiting | 8 (2.2) | 3 (0.8) | 5 (1.4) | ||
| Diarrhea | 3 (0.8) | 3 (0.8) | |||
| Abdominal pain | 7 (1.9) | 4 (1.1) | 3 (0.8) | ||
| Fever | 86 (23.8) | 51 (14.1) | 35 (9.7) | ||
| Blood pressure drop | 19 (5.3) | 9 (2.5) | 10 (2.8) | ||
| Tachycardia | 40 (11.1) | 22 (6.1) | 18 (5.0) | ||
| Bradycardia | 34 (9.4) | 24 (6.6) | 10 (2.8) | ||
| Myalgia | 43 (11.9) | 16 (4.4) | 27 (7.5) | ||
| Malaise | 1 (0.3) | 1 (0.3) | |||
| Agitation | 2 (0.6) | 1 (0.3) | 1 (0.3) | ||
| Headache | 7 (1.9) | 3 (0.8) | 4 (1.1) | ||
| Frisson | 4 (1.1) | 1 (0.3) | 3 (0.8) |
| ID | Snake | Event | Place of Death | Age | Time between Bite and Hospital Presentation | Time between Bite and Death | IPA Dose | Link with IPA (Score *) | Cause of Death According to Scientific Committee |
|---|---|---|---|---|---|---|---|---|---|
| 1 | Elapidae | Death | Hospital | 6 | 1 h 30 | 2 h | 0 vial | No (NA **) | Respiratory failure |
| 2 | Questionable snake | Death | Hospital | 24 | 5 h | 22 h30 | 6 vials | No (−3) | Digestive hemorrhage or plant poisoning |
| 3 | Echis romani § | Death | Hospital | 12 | 1 or 2 h | 6/7 h | 4 vials | No (−3) | Hemorrhagic syndrome + malaria + insufficient antivenom dose |
| 4 | Echis romani & | Death | Hospital | 20 | 158 h | 165 h | 4 vials | No (−3) | Severe anemia + brain hemorrhage |
| 5 | Echis romani § | Death | Home † | 45 | 3 h | 168 h | 6 vials | No (−3) | Anemia + malaria |
| 6 | Echis romani & | Death | Home † | 41 | 7 h | 120 h | 4 vials | No (−3) | Anemia |
| 7 | Naja nigricollis § | Death | Home † | 80 | 4 h | 500 h | 2 vials | No (−2) | Heart failure unrelated to envenomation + envenomation |
| 8 | Echis romani & | Death | Hospital | 42 | 24 h | 117 h | 4 vials | No (−3) | Cardiovascular collapse |
| 9 | Naja haje § | Death | Hospital | 8 | 17.4 h | 49.6 h | 4 vials | No (−3) | Sepsis, inhalation of vomiting, intoxication from traditional treatment, or pulmonary embolism |
| 10 | Echis romani § | In utero fetal death | Hospital | 30 | 22.9 h | 38.5 h | 2 vials | No (−2) | Fetal hypotrophy prior to snakebite + hemorrhage |
| 11 | Echis romani § | Death | Hospital | 25 | 1.7 h | 114.3 h | 10 vials | No (−3) | Acute renal failure + obstetric hemorrhage due to envenomation |
| 12 | Echis romani § | Death | Hospital | 8 | 62.5 h | 63.5 h | 2 vials | No (−2) | Brain hemorrhage |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benhammou, D.; Chippaux, J.-P.; Ntone, R.; Madec, Y.; Amta, P.; Noel, G.; Karl, F.N.; Perilhou, A.; Matchim, L.; Sanchez, M.; et al. Snakebites in Cameroon: Tolerance of a Snake Antivenom (Inoserp™ PAN-AFRICA) in Africa in Real-Life Conditions. Toxins 2024, 16, 165. https://doi.org/10.3390/toxins16040165
Benhammou D, Chippaux J-P, Ntone R, Madec Y, Amta P, Noel G, Karl FN, Perilhou A, Matchim L, Sanchez M, et al. Snakebites in Cameroon: Tolerance of a Snake Antivenom (Inoserp™ PAN-AFRICA) in Africa in Real-Life Conditions. Toxins. 2024; 16(4):165. https://doi.org/10.3390/toxins16040165
Chicago/Turabian StyleBenhammou, David, Jean-Philippe Chippaux, Rodrigue Ntone, Yoann Madec, Pierre Amta, Gaëlle Noel, Fai Njuwa Karl, Anaïs Perilhou, Lucrece Matchim, Marie Sanchez, and et al. 2024. "Snakebites in Cameroon: Tolerance of a Snake Antivenom (Inoserp™ PAN-AFRICA) in Africa in Real-Life Conditions" Toxins 16, no. 4: 165. https://doi.org/10.3390/toxins16040165
APA StyleBenhammou, D., Chippaux, J.-P., Ntone, R., Madec, Y., Amta, P., Noel, G., Karl, F. N., Perilhou, A., Matchim, L., Sanchez, M., Ndifon, M., Clauteaux, P., Eteki, L., Boum, Y., II, Nkwescheu, A. S., & Taieb, F. (2024). Snakebites in Cameroon: Tolerance of a Snake Antivenom (Inoserp™ PAN-AFRICA) in Africa in Real-Life Conditions. Toxins, 16(4), 165. https://doi.org/10.3390/toxins16040165