Can Botulinum Toxin-A Contribute to Reconstructing the Physiological Homeostasis of the Masticatory Complex in Short-Faced Patients during Occlusal Therapy? A Prospective Pilot Study

Abstract
1. Introduction
2. Patients and Methods
2.1. Subjects
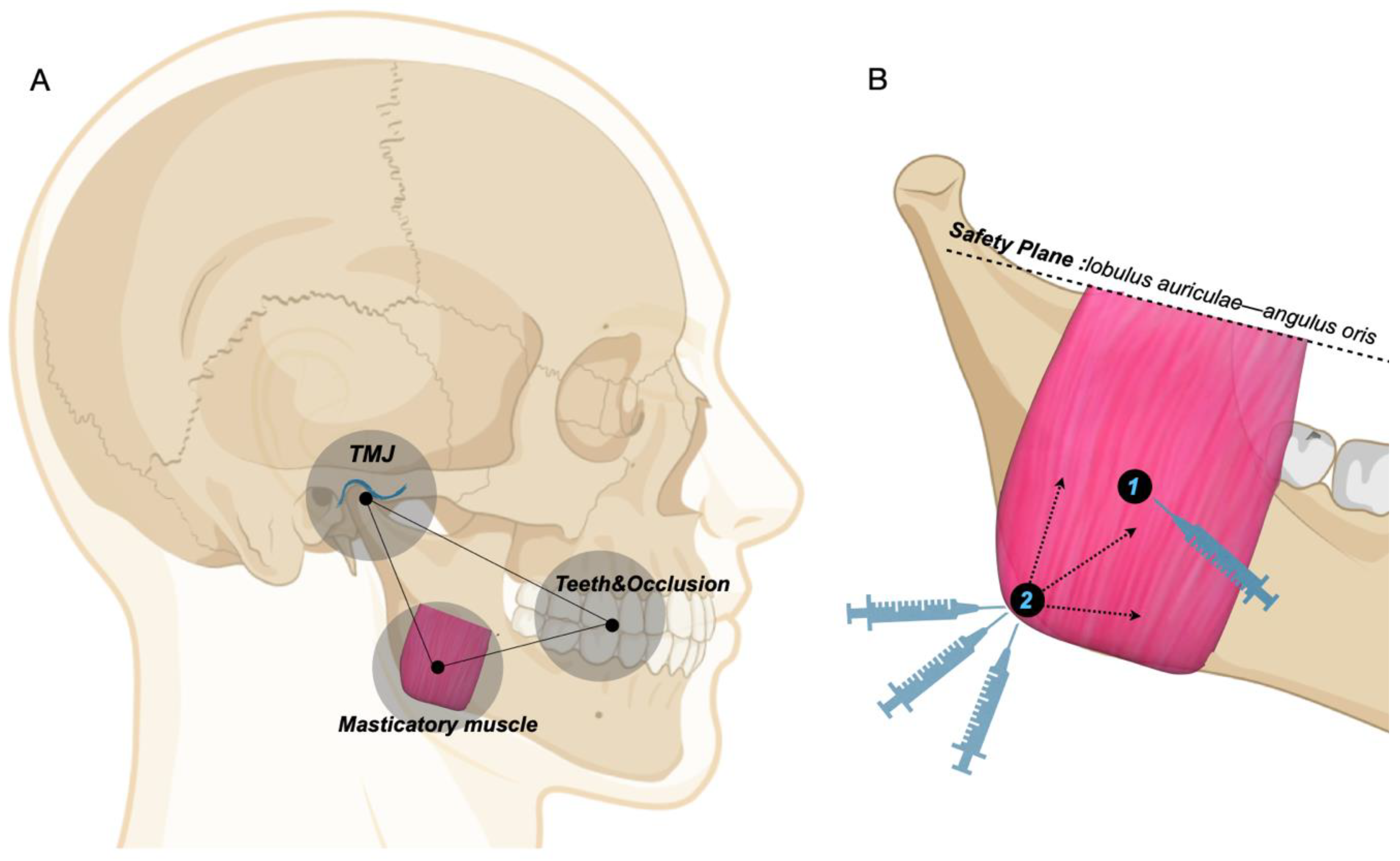
2.2. BTX-A Injection Method
2.3. CBCT Measurement Items and Methods
2.3.1. Masseter Muscle Index
2.3.2. Dental and Occlusal Indexes
2.3.3. Temporomandibular Joint Indexes
- Draw four parallel lines of FH from the superior to the inferior, tangent to the glenoid fossa, condyle, the lowest end of the articular eminence, and the sigmoid notch of the mandible, respectively, named L1, L2, L3, and L4. The vertical distance between L2 and L4 was defined as the condyle height (Ht.Co) and the vertical distance between L1 and L3 was defined as the fossa height (Ht.Fo). L3 intersected the posterior wall of the fossa, and the horizontal distance between the intersection point and the tangent point was defined as the fossa width (Wd.Fo).
- Taking the tangent point of L1 (superior fossa (SF) point) as the starting point, draw three new tangent lines from the anterior to the posterior, which were tangent to the posterior slope of the articular eminence, the anterior edge of the condyle, and the posterior edge of the condyle, respectively, named T1, T2, and T3. The angle between T1 and FH was defined as the articular eminence inclination (AEI).
- Joint spaces were measured using the Kamelchuk method [66]. The distance between the tangent point of L1 and L2 was measured as the superior joint space (SJS). The perpendicular distance from T2 tangent point to the posterior slope of articular eminence was defined as anterior joint space (AJS), and the perpendicular distance from T3 tangent point to the posterior wall of fossa was defined as posterior joint space (PJS).
2.4. Statistical Analysis
3. Results
3.1. Changes in the CBCT Masticatory Complex
3.1.1. Changes in the Masseter Muscle Thickness
3.1.2. Changes in Dental Occlusion
3.1.3. Changes in TMJ
3.2. Correlation Analysis of the Components of the Masticatory Complex in Short-Faced Patients
4. Discussion
4.1. Effects of BTX-A on Homeostasis Reconstruction of the Masticatory Complex
4.1.1. BTX-A and Masticatory Muscle
4.1.2. BTX-A and Teeth and Occlusion
4.1.3. BTX-A and TMJ
4.2. Preliminary Study on the Homeostasis Mechanisms of the Masticatory Complex
4.3. Limitations
4.4. Future Perspective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BTX-A | botulinum toxin-A | FH | frankfort horizontal plane |
| MS | masticatory system | AOP | anterior occlusal plane |
| SS | stomatognathic system | POP | posterior occlusal plane |
| TMJ | temporomandibular joint | COS | curve of Spee |
| TMD | temporomandibular joint disorders | COW | curve of Wilson |
| CBCT | cone-beam computed tomography | AEI | articular eminence inclination |
| MMT | masseter muscle thickness | AJS | anterior joint space |
| MP | mandibular plane | SJS | superior joint space |
| PP | palatal plane | PJS | posterior joint space |
References
- Okeson, J.P. Evolution of occlusion and temporomandibular disorder in orthodontics: Past, present, and future. Am. J. Orthod. Dentofac. Orthop. 2015, 147, S216–S223. [Google Scholar] [CrossRef] [PubMed]
- Kandasamy, S.; Greene, C.S. The evolution of temporomandibular disorders: A shift from experience to evidence. J. Oral Pathol. Med. 2020, 49, 461–469. [Google Scholar] [CrossRef] [PubMed]
- Zonnenberg, A.J.J.; Türp, J.C.; Greene, C.S. Centric relation critically revisited—What are the clinical implications? J. Oral Rehabil. 2021, 48, 1050–1055. [Google Scholar] [CrossRef] [PubMed]
- Angle, E.H. Classification of malocclusion. Dent. Cosmos. 1899, 41, 246–264. [Google Scholar]
- Summers, C.J. The occlusal index: A system for identifying and scoring occlusal disorders. Am. J. Orthod. 1971, 59, 552–567. [Google Scholar] [CrossRef][Green Version]
- Andrews, L.F. The six keys to normal occlusion. Am. J. Orthod. 1972, 62, 296–309. [Google Scholar] [CrossRef]
- Roth, R.H. The maintenance system and occlusal dynamics. Dent. Clin. N. Am. 1976, 20, 761–788. [Google Scholar] [CrossRef]
- Roth, R.H. Functional occlusion for the orthodontist. J. Clin. Orthod. 1981, 15, 32–51. [Google Scholar]
- Dawson, P.E. Functional Occlusion: From TMJ to Smile Design, 1st ed.; Elsevier Health Sciences: St. Louis, MO, USA, 2006; pp. 4–5. [Google Scholar]
- Goodacre, C.J.; Roberts, W.E.; Goldstein, G.; Wiens, J.P. Does the Stomatognathic System Adapt to Changes in Occlusion? Best Evidence Consensus Statement. J. Prosthodont. 2021, 30, 5–11. [Google Scholar] [CrossRef]
- Nakamura, S.S.; Donatelli, D.; Rosenberg, E.S. Posterior bite collapse: Guidelines for treatment based on form and function. Int. J. Periodontics Restor. Dent. 2022, 42, 351–359. [Google Scholar] [CrossRef]
- D’Amico, C.; Bocchieri, S.; Sambataro, S.; Surace, G.; Stumpo, C.; Fiorillo, L. Occlusal load considerations in implant-supported fixed restorations. Prosthesis 2020, 2, 252–265. [Google Scholar] [CrossRef]
- Sheridan, R.A.; Decker, A.M.; Plonka, A.B.; Wang, H.L. The role of occlusion in implant therapy: A comprehensive updated review. Implant. Dent. 2016, 25, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Dommisch, H.; Walter, C.; Difloe-Geisert, J.C.; Gintaute, A.; Jepsen, S.; Zitzmann, N.U. Efficacy of tooth splinting and occlusal adjustment in patients with periodontitis exhibiting masticatory dysfunction: A systematic review. Clin. Periodontol. 2021; ahead of print. [Google Scholar]
- Passanezi, E.; Sant’Ana, A.C.P. Role of occlusion in periodontal disease. Periodontol 2000. 2019, 79, 129–150. [Google Scholar] [CrossRef] [PubMed]
- Gund, M.P.; Wrbas, K.-T.; Hannig, M.; Rupf, S. Apical periodontitis after intense bruxism. BMC Oral Health 2022, 22, 91. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhang, C.; Liu, Q.; Zhou, K.; Yin, N.; Zhang, H.; Shi, M.; Liu, X.; Wang, M. Dental malocclusion stimulates neuromuscular circuits associated with temporomandibular disorders. Eur. J. Oral Sci. 2018, 126, 466–475. [Google Scholar] [CrossRef]
- Ribeiro-Lages, M.B.; Martins, M.L.; Magno, M.B.; Masterson Ferreira, D.; Tavares-Silva, C.M.; Fonseca-Gonçalves, A.; Serra-Negra, J.M.; Maia, L.C. Is there association between dental malocclusion and bruxism? A systematic review and meta-analysis. J. Oral Rehabil. 2020, 47, 1304–1318. [Google Scholar] [CrossRef]
- Buvinic, S.; Balanta-Melo, J.; Kupczik, K.; Vásquez, W.; Beato, C.; Toro-Ibacache, V. Muscle-Bone Crosstalk in the Masticatory System: From Biomechanical to Molecular Interactions. Front. Endocrinol. 2021, 11, 606947. [Google Scholar] [CrossRef]
- Pepicelli, A.; Woods, M.; Briggs, C. The mandibular muscles and their importance in orthodontics: A contemporary review. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 774–780. [Google Scholar] [CrossRef]
- Saadeh, M.; Fayyad-Kazan, H.; Haddad, R.; Ayoub, F. Facial soft tissue thickness differences among different vertical facial patterns. Forensic. Sci. Int. 2020, 317, 110468. [Google Scholar] [CrossRef]
- Yamada, T.; Sugiyama, G.; Mori, Y. Masticatory muscle function affects the pathological conditions of dentofacial deformities. Jpn. Dent. Sci. Rev. 2020, 56, 56–61. [Google Scholar] [CrossRef]
- Kattiney de Oliveira, L.; Fernandes Neto, A.J.; Moraes Mundim Prado, I.; Guimarães Henriques, J.C.; Beom Kim, K.; de Araújo Almeida, G. Evaluation of the condylar position in younger and older adults with or without temporomandibular symptoms by using cone beam computed tomography. J. Prosthet. Dent. 2022, 127, 445–452. [Google Scholar] [CrossRef] [PubMed]
- Chamberland, S. Progressive idiopathic condylar resorption: Three case reports. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 531–544. [Google Scholar] [CrossRef] [PubMed]
- Almukhtar, R.M.; Fabi, S.G. The masseter muscle and its role in facial contouring, aging, and quality of life: A literature review. Plast. Reconstr. Surg. 2019, 143, 39e–48e. [Google Scholar] [CrossRef] [PubMed]
- Biondi, K.; Lorusso, P.; Fastuca, R.; Mangano, A.; Zecca, P.A.; Bosco, M.; Caprioglio, A.; Levrini, L. Evaluation of masseter muscle in different vertical skeletal patterns in growing patients. Eur. J. Paediatr. Dent. 2016, 17, 47–52. [Google Scholar]
- Takeuchi-Sato, T.; Arima, T.; Mew, M.; Svensson, P. Relationships between craniofacial morphology and masticatory muscle activity during isometric contraction at different interocclusal distances. Arch. Oral. Biol. 2019, 98, 52–60. [Google Scholar] [CrossRef]
- Lione, R.; Franchi, L.; Noviello, A.; Bollero, P.; Fanucci, E.; Cozza, P. Three-dimensional evaluation of masseter muscle in different vertical facial patterns: A cross-sectional study in growing children. Ultrason Imaging 2013, 35, 307–317. [Google Scholar] [CrossRef]
- Piancino, M.G.; Tortarolo, A.; Di Benedetto, L.; Crincoli, V.; Falla, D. Chewing patterns and muscular activation in deep bite malocclusion. J. Clin. Med. 2022, 11, 1702. [Google Scholar] [CrossRef]
- Arponen, H.; Suominen, A.; Svedström-Oristo, A.L. Longitudinal analysis of the quality of orthodontic treatment outcome and stability of occlusal traits. Acta Odontol. Scand. 2022, 80, 234–240. [Google Scholar] [CrossRef]
- Pollard, D.; Akyalcin, S.; Wiltshire, W.A.; Rody, W.J. Relapse of orthodontically corrected deepbites in accordance with growth pattern. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 477–483. [Google Scholar] [CrossRef]
- Rozzi, M.; Mucedero, M.; Pezzuto, C.; Lione, R.; Cozza, P. Long-term stability of curve of Spee levelled with continuous archwires in subjects with different vertical patterns: A retrospective study. Eur. J. Orthod. 2019, 41, 286–293. [Google Scholar] [CrossRef]
- Santander, P.; Quast, A.; Olbrisch, C.; Rose, M.; Moser, N.; Schliephake, H.; Meyer-Marcotty, P. Comprehensive 3D analysis of condylar morphology in adults with different skeletal patterns–a cross-sectional study. Head Face Med. 2020, 16, 33. [Google Scholar] [CrossRef]
- Barbosa, L.A.G.; Araujo, E.; Behrents, R.G.; Buschang, P.H. Longitudinal cephalometric growth of untreated subjects with Class II Division 2 malocclusion. Am. J. Orthod. Dentofac. Orthop. 2017, 151, 914–920. [Google Scholar] [CrossRef] [PubMed]
- Paes-Souza, S.D.A.; Marañón-Vásquez, G.A.; Galisteu-Luiz, K.; Ferreira, D.M.T.P.; Maia, L.C.; Nojima, M.D.C.G. Is there variation in the depth of the curve of Spee in individuals with different dentoskeletal patterns? A systematic review with meta-analysis. Eur. J. Orthod. 2022, 2, cjab078. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, E.M.; Sato, S. Longitudinal alteration of the occlusal plane and development of different dentoskeletal frames during growth. Am. J. Orthod. Dentofac. Orthop. 2008, 134, 602.e1–602.e11. [Google Scholar] [CrossRef]
- Charalampidou, M.; Kjellberg, H.; Georgiakaki, I.; Kiliaridis, S. Masseter muscle thickness and mechanical advantage in relation to vertical craniofacial morphology in children. Acta Odontol. Scand. 2008, 66, 23–30. [Google Scholar] [CrossRef]
- Oliveira, S.S.I.; Pannuti, C.M.; Paranhos, K.S.; Tanganeli, J.P.C.; Laganá, D.C.; Sesma, N.; Duarte, M.; Frigerio, M.L.M.A.; Cho, S.C. Effect of occlusal splint and therapeutic exercises on postural balance of patients with signs and symptoms of temporomandibular disorder. Clin. Exp. Dent. Res. 2019, 5, 109–115. [Google Scholar] [CrossRef]
- Hong, S.W.; Kang, J.H. Decreased mandibular cortical bone quality after botulinum toxin injections in masticatory muscles in female adults. Sci. Rep. 2020, 10, 3623. [Google Scholar] [CrossRef]
- Sellin, L.C. The action of botulinum toxin at the neuromuscular junction. Med. Biol. 1981, 59, 11–20. [Google Scholar]
- Serrera-Figallo, M.A.; Ruiz-De-León-Hernández, G.; Torres-Lagares, D.; Castro-Araya, A.; Torres-Ferrerosa, O.; Hernández-Pacheco, E.; Gutierrez-Perez, J.L. Use of botulinum toxin in orofacial clinical practice. Toxins 2020, 12, 112. [Google Scholar] [CrossRef]
- Kumar, A.; Spivakovsky, S. Bruxism-is botulinum toxin an effective treatment? Evid. Based Dent. 2018, 19, 59. [Google Scholar] [CrossRef]
- Sendra, L.A.; Montez, C.; Vianna, K.C.; Barboza, E.P. Clinical outcomes of botulinum toxin type A injections in the management of primary bruxism in adults: A systematic review. J. Prosthet. Dent. 2020, 126, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Cooper, L.; Lui, M.; Nduka, C. Botulinum toxin treatment for facial palsy: A systematic review. J. Plast. Reconstr. Aesthetic Surg. 2017, 70, 833–841. [Google Scholar] [CrossRef] [PubMed]
- Sipahi Calis, A.; Colakoglu, Z.; Gunbay, S. The use of botulinum toxin-a in the treatment of muscular temporomandibular joint disorders. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 322–325. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-S.; Yun, P.-Y.; Kim, Y.-K. A clinical evaluation of botulinum toxin-A injections in the temporomandibular disorder treatment. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 5. [Google Scholar] [CrossRef]
- Berweck, S.; Bonikowski, M.; Kim, H.; Althaus, M.; Flatau-Baqué, B.; Mueller, D.; Banach, M.D. Placebo-Controlled Clinical Trial of IncobotulinumtoxinA for Sialorrhea in Children. Neurology 2021, 97, e1425–e1436. [Google Scholar] [CrossRef]
- Bakke, M.; Baram, S.; Dalager, T.; Biernat, H.B.; Møller, E. Oromandibular dystonia, mental distress and oro-facial dysfunction—A follow-up 8-10 years after start of treatment with botulinum toxin. J. Oral Rehabil. 2019, 46, 441–449. [Google Scholar] [CrossRef]
- Choi, J.W.; Kim, H.J.; Moon, J.W.; Kang, S.H.; Tak, H.J.; Lee, S.H. Compensatory dentoalveolar supraeruption and occlusal plane cant after botulinum-induced hypotrophy of masticatory closing muscles in juvenile rats. Arch. Oral Biol. 2019, 101, 34–42. [Google Scholar] [CrossRef]
- Yoshimi, T.; Koga, Y.; Nakamura, A.; Fujishita, A.; Kohara, H.; Moriuchi, E.; Yoshimi, K.; Tsai, C.Y.; Yoshida, N. Mechanism of motor coordination of masseter and temporalis muscles for increased masticatory efficiency in mice. J. Oral Rehabil. 2017, 44, 363–374. [Google Scholar] [CrossRef]
- Tsai, C.Y.; Chiu, W.C.; Liao, Y.H.; Tsai, C.M. Effects on craniofacial growth and development of unilateral botulinum neurotoxin injection into the masseter muscle. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 142.e1–142.e6. [Google Scholar] [CrossRef]
- Liu, J.; Liu, S.Y.; Zhao, Y.J.; Gu, X.; Li, Q.; Jin, Z.L.; Chen, Y.J. Effects of occlusion on mandibular morphology and architecture in rats. J. Surg. Res. 2016, 200, 533–543. [Google Scholar] [CrossRef]
- Navarrete, A.L.; Rafferty, K.L.; Liu, Z.J.; Ye, W.; Greenlee, G.M.; Herring, S.W. Botulinum neurotoxin type A in the masseter muscle: Effects on incisor eruption in rabbits. Am. J. Orthod. Dentofac. Orthop. 2013, 143, 499–506. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.H.; Singer, S.R.; Mupparapu, M. Review of cone beam computed tomography guidelines in North America. Quintessence Int. 2019, 50, 136–145. [Google Scholar]
- Lee, H.J.; Kim, S.J.; Lee, K.J.; Yu, H.S.; Baik, H.S. Repeated injections of botulinum toxin into the masseter muscle induce bony changes in human adults: A longitudinal study. Korean J. Orthod. 2017, 47, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Demehri, S.; Muhit, A.; Zbijewski, W.; Stayman, J.W.; Yorkston, J.; Packard, N.; Senn, R.; Yang, D.; Foos, D.; Thawait, G.K.; et al. Assessment of image quality in soft tissue and bone visualization tasks for a dedicated extremity cone-beam CT system. Eur. Radiol. 2015, 25, 1742–1751. [Google Scholar] [CrossRef] [PubMed]
- Becht, M.P.; Mah, J.; Martin, C.; Razmus, T.; Gunel, E.; Ngan, P. Évaluation De La Morphologie Du Muscle Masséter Dans Différents Types De Malocclusions En Utilisant La Tomographie Volumétrique À Faisceau Conique. Int. Orthod. 2014, 12, 32–48. [Google Scholar] [CrossRef]
- Iyer, A.; Thor, M.; Onochie, I.; Hesse, J.; Zakeri, K.; Locastro, E.; Jiang, J.; Veeraraghavan, H.; Elguindi, S.; Lee, N.Y.; et al. Prospectively-validated deep learning model for segmenting swallowing and chewing structures in CT. Phys. Med. Biol. 2022, 67, 024001. [Google Scholar] [CrossRef]
- Hu, Z.J.; He, J.; Zhao, F.D.; Fang, X.Q.; Zhou, L.N.; Fan, S.W. An assessment of the intra- and inter-reliability of the lumbar paraspinal muscle parameters using CT scan and magnetic resonance imaging. Spine 2011, 36, 868–874. [Google Scholar] [CrossRef]
- Pan, Y.; Wang, Y.; Li, G.; Chen, S.; Xu, T. Validity and reliability of masseter muscles segmentation from the transverse sections of Cone-Beam CT scans compared with MRI scans. Int. J. Comput. Assist. Radiol. Surg. 2022, 17, 751–759. [Google Scholar] [CrossRef]
- Xu, J.A.; Yuasa, K.; Yoshiura, K.; Kanda, S. Quantitative analysis of masticatory muscles using computed tomography. Dentomaxillofac. Radiol. 1994, 23, 154–158. [Google Scholar] [CrossRef]
- Esenlik, E.; Sabuncuoglu, F.A. Alveolar and symphysis regions of patients with skeletal class ii division 1 anomalies with different vertical growth patterns. Eur. J. Dent. 2012, 6, 123–132. [Google Scholar] [CrossRef][Green Version]
- Ning, R.; Guo, J.; Li, Q.; Martin, D. Maxillary width and hard palate thickness in men and women with different vertical and sagittal skeletal patterns. Am. J. Orthod. Dentofac. Orthop. 2021, 159, 564–573. [Google Scholar] [CrossRef] [PubMed]
- Al-Qawasmi, R.; Coe, C. Genetic influence on the curves of occlusion in children seeking orthodontic treatment. Int. Orthod. 2021, 19, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.Y.; Song, J.M.; Kim, Y.D.; Chung, I.K.; Shin, S.H. Clinical changes of TMD and condyle stability after two jaw surgery with and without preceding TMD treatments in class III patients. Maxillofac. Plast. Reconstr. Surg. 2015, 37, 9. [Google Scholar] [CrossRef]
- Kamelchuk, L.S.; Grace, M.G.A.; Major, P.W. Post-imaging temporomandibular joint space analysis. Cranio 1996, 14, 23–29. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Hsu, S.H.; McGee, J.S. Botulinum toxin injections for masseter reduction in east asians. Dermatol. Surg. 2019, 45, 566–572. [Google Scholar] [CrossRef]
- Diracoglu, D.; Sahbaz, T.; Alptekin, K.; Dogan, N. Effects of ultrasound-assisted botulinum neurotoxin-A injection in patients with bruxism and masseter hypertrophy. Turk. J. Phys. Med. Rehabil. 2021, 67, 351–356. [Google Scholar] [CrossRef]
- Lee, H.H.; Kim, S.T.; Lee, K.J.; Baik, H.S. Effect of a second injection of botulinum toxin on lower facial contouring, as evaluated using 3-dimensional laser scanning. Dermatol. Surg. 2015, 41, 439–444. [Google Scholar] [CrossRef]
- Zhang, L.D.; Liu, Q.; Zou, D.R.; Yu, L. feng. Occlusal force characteristics of masseteric muscles after intramuscular injection of botulinum toxin A(BTX–A)for treatment of temporomandibular disorder. Br. J. Oral Maxillofac. Surg. 2016, 54, 736–740. [Google Scholar] [CrossRef]
- Kim, J.H.; Shin, J.H.; Kim, S.T.; Kim, C.Y. Effects of two different units of botulinum toxin type a evaluated by computed tomography and electromyographic measurements of human masseter muscle. Plast. Reconstr. Surg. 2007, 119, 711–717. [Google Scholar] [CrossRef]
- Kim, K.S.; Byun, Y.S.; Kim, Y.J.; Kim, S.T. Muscle weakness after repeated injection of botulinum toxin type A evaluated according to bite force measurement of human masseter muscle. Dermatol. Surg. 2009, 35, 1902–1907. [Google Scholar] [CrossRef]
- Wong, A.; Woods, M.G.; Stella, D. Three-dimensional computed tomographic assessment of mandibular muscles in growing subjects with different vertical facial patterns. Aust. Orthod. J. 2016, 32, 2–17. [Google Scholar] [CrossRef] [PubMed]
- Acar, A.; Alcan, T.; Erverdi, N. Evaluation of the relationship between the anterior component of occlusal force and postretention crowding. Am. J. Orthod. Dentofac. Orthop. 2002, 122, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Teng, F.; Du, F.Y.; Chen, H.Z.; Jiang, R.P.; Xu, T.M. Three-dimensional analysis of the physiologic drift of adjacent teeth following maxillary first premolar extractions. Sci. Rep. 2019, 9, 14549. [Google Scholar] [CrossRef] [PubMed]
- Alkhatib, R.; Chung, C.H. Buccolingual inclination of first molars in untreated adults: A CBCT study. Angle Orthod. 2017, 87, 598–602. [Google Scholar] [CrossRef]
- Golshah, A.; Rezaei, N.; Heshmati, S. Buccolingual Inclination of Canine and First and Second Molar Teeth and the Curve of Wilson in Different Sagittal Skeletal Patterns of Adults Using Cone-Beam Computed Tomography. Int. J. Dent. 2020, 2020, 8893778. [Google Scholar] [CrossRef]
- Seok, H.; Kim, S.G. Correction of malocclusion by botulinum neurotoxin injection into masticatory muscles. Toxins 2018, 10, 27. [Google Scholar] [CrossRef]
- Dai, F.; Wang, L.; Chen, G.; Chen, S.; Xu, T. Three-dimensional modeling of an individualized functional masticatory system and bite force analysis with an orthodontic bite plate. Int. J. Comput. Assist. Radiol. Surg. 2016, 11, 217–229. [Google Scholar] [CrossRef]
- Kiliaridis, S.; Georgiakaki, I.; Katsaros, C. Masseter muscle thickness and maxillary dental arch width. Eur. J. Orthod. 2003, 25, 259–263. [Google Scholar] [CrossRef]
- Koyano, K.; Tsukiyama, Y.; Kuwatsuru, R. Rehabilitation of occlusion–science or art? J. Oral Rehabil. 2012, 39, 513–521. [Google Scholar] [CrossRef]
- Fueki, K.; Yoshida, E.; Okano, K.; Igarashi, Y. Association between occlusal curvature and masticatory movements with different test foods in human young adults with permanent dentitions. Arch. Oral Biol. 2013, 58, 674–680. [Google Scholar] [CrossRef]
- Yu, X.; Lu, D.; Tian, S.; Yuan, X.; Cheng, Q. Influence of cranial base angle and posterior occlusal plane inclination on sagittal dentoskeletal types. Chin. J. Tissue Eng. Res. 2020, 24, 1659–1665. [Google Scholar]
- Santhosh Kumar, M.P. The emerging role of botulinum toxin in the treatment of orofacial disorders: Literature update. Asian J. Pharm. Clin. Res. 2017, 10, 21–29. [Google Scholar] [CrossRef]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.-P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Oksanen, E.; Männistö, V.; Kormi, E.; Vallioniemi, H.; Suojanen, J. Temporomandibular disorder patients benefit from intramuscular botulinum toxin type A injections. J. Craniofac. Surg. 2021; ahead of print. [Google Scholar]
- Pihut, M.; Ferendiuk, E.; Szewczyk, M.; Kasprzyk, K.; Wieckiewicz, M. The efficiency of botulinum toxin type A for the treatment of masseter muscle pain in patients with temporomandibular joint dysfunction and tension-type headache. J. Headache Pain 2016, 17, 29. [Google Scholar] [CrossRef] [PubMed]
- Al-Wayli, H. Treatment of chronic pain associated with nocturnal bruxism with botulinum toxin. A prospective and randomized clinical study. J. Clin. Exp. Dent. 2017, 9, e112–e117. [Google Scholar] [CrossRef]
- Shi, Z.; Lv, J.; Xiaoyu, L.; Zheng, L.W.; Yang, X.W. Condylar degradation from decreased occlusal loading following masticatory muscle atrophy. Biomed. Res. Int. 2018, 2018, 6947612. [Google Scholar] [CrossRef]
- Rafferty, K.L.; Liu, Z.J.; Ye, W.; Navarrete, A.L.; Nguyen, T.T.; Salamati, A.; Herring, S.W. Botulinum toxin in masticatory muscles: Short- and long-term effects on muscle, bone, and craniofacial function in adult rabbits. Bone 2012, 50, 651–662. [Google Scholar] [CrossRef] [PubMed]
- Kün-Darbois, J.D.; Libouban, H.; Chappard, D. Botulinum toxin in masticatory muscles of the adult rat induces bone loss at the condyle and alveolar regions of the mandible associated with a bone proliferation at a muscle enthesis. Bone 2015, 77, 75–82. [Google Scholar] [CrossRef]
- Raphael, K.G.; Janal, M.N.; Tadinada, A.; Santiago, V.; Sirois, D.A.; Lurie, A.G. Effect of multiple injections of botulinum toxin into painful masticatory muscles on bone density in the temporomandibular complex. J. Oral Rehabil. 2020, 47, 1319–1329. [Google Scholar] [CrossRef]
- Dickinson, E.; Fitton, L.C.; Kupczik, K. Ontogenetic changes to muscle architectural properties within the jaw-adductor musculature of Macaca fascicularis. Am. J. Phys. Anthropol. 2018, 167, 291–310. [Google Scholar] [CrossRef]
- Jiménez-Silva, A.; Tobar-Reyes, J.; Vivanco-Coke, S.; Pastén-Castro, E.; Palomino-Montenegro, H. Centric relation–intercuspal position discrepancy and its relationship with temporomandibular disorders. A systematic review. Acta Odontol. Scand. 2017, 75, 463–474. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Standardization Coefficient β | Significance | Adjusted R2 | p Value | |
|---|---|---|---|---|
| (Intercept) | 10.08 | 0.0002 | 0.871 | 0.0003 |
| COW | −0.11 | 0.003 | ||
| AJS | 2.73 | 0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, X.; Feng, X.; Li, J.; Bao, X.; Xu, J.; Lin, J. Can Botulinum Toxin-A Contribute to Reconstructing the Physiological Homeostasis of the Masticatory Complex in Short-Faced Patients during Occlusal Therapy? A Prospective Pilot Study. Toxins 2022, 14, 374. https://doi.org/10.3390/toxins14060374
Li X, Feng X, Li J, Bao X, Xu J, Lin J. Can Botulinum Toxin-A Contribute to Reconstructing the Physiological Homeostasis of the Masticatory Complex in Short-Faced Patients during Occlusal Therapy? A Prospective Pilot Study. Toxins. 2022; 14(6):374. https://doi.org/10.3390/toxins14060374
Chicago/Turabian StyleLi, Xin, Xiaoyan Feng, Juan Li, Xinyu Bao, Jinghong Xu, and Jun Lin. 2022. "Can Botulinum Toxin-A Contribute to Reconstructing the Physiological Homeostasis of the Masticatory Complex in Short-Faced Patients during Occlusal Therapy? A Prospective Pilot Study" Toxins 14, no. 6: 374. https://doi.org/10.3390/toxins14060374
APA StyleLi, X., Feng, X., Li, J., Bao, X., Xu, J., & Lin, J. (2022). Can Botulinum Toxin-A Contribute to Reconstructing the Physiological Homeostasis of the Masticatory Complex in Short-Faced Patients during Occlusal Therapy? A Prospective Pilot Study. Toxins, 14(6), 374. https://doi.org/10.3390/toxins14060374