Botulinum Toxin Injection for the Treatment of Upper Esophageal Sphincter Dysfunction


Abstract
1. Introduction
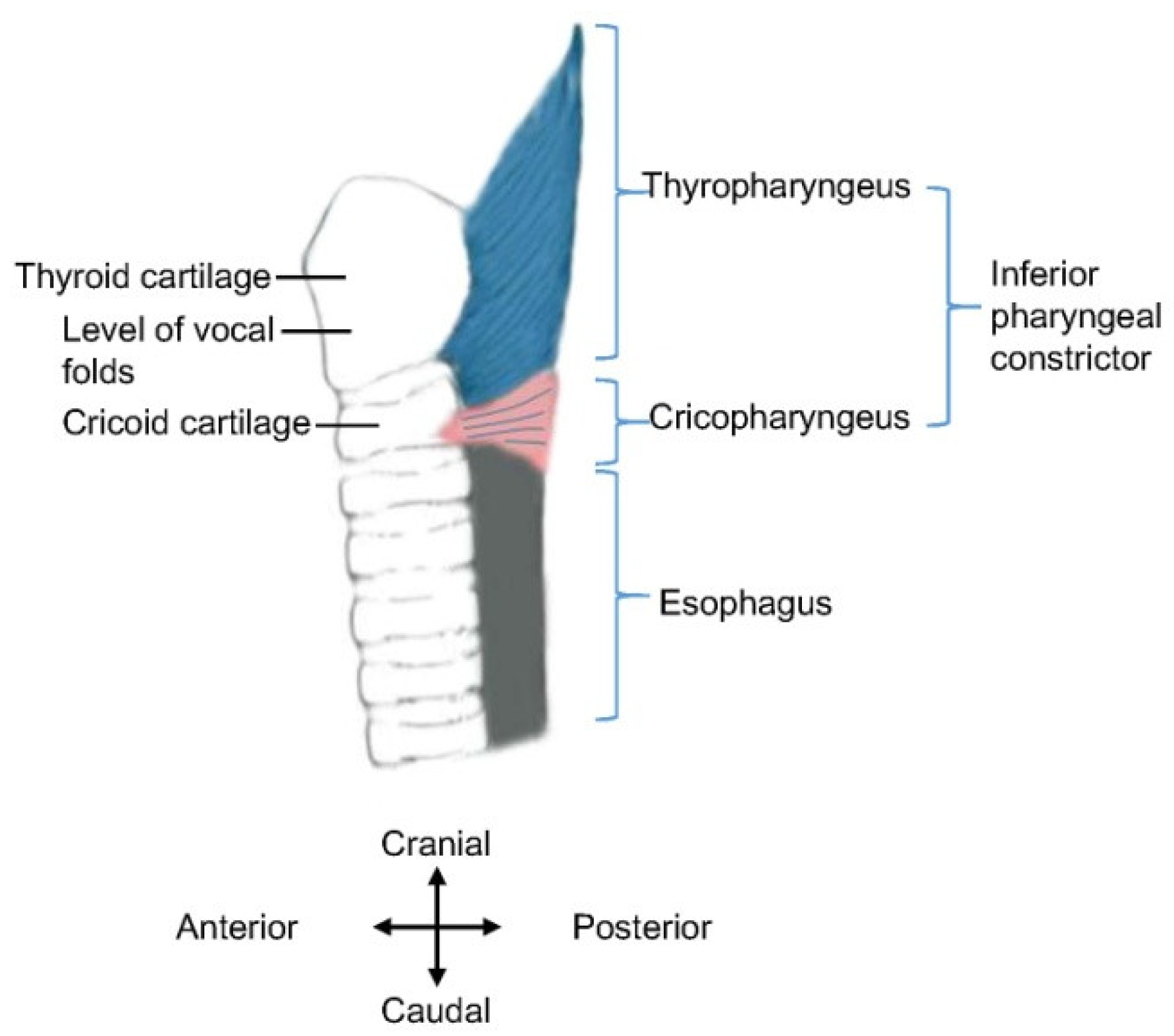
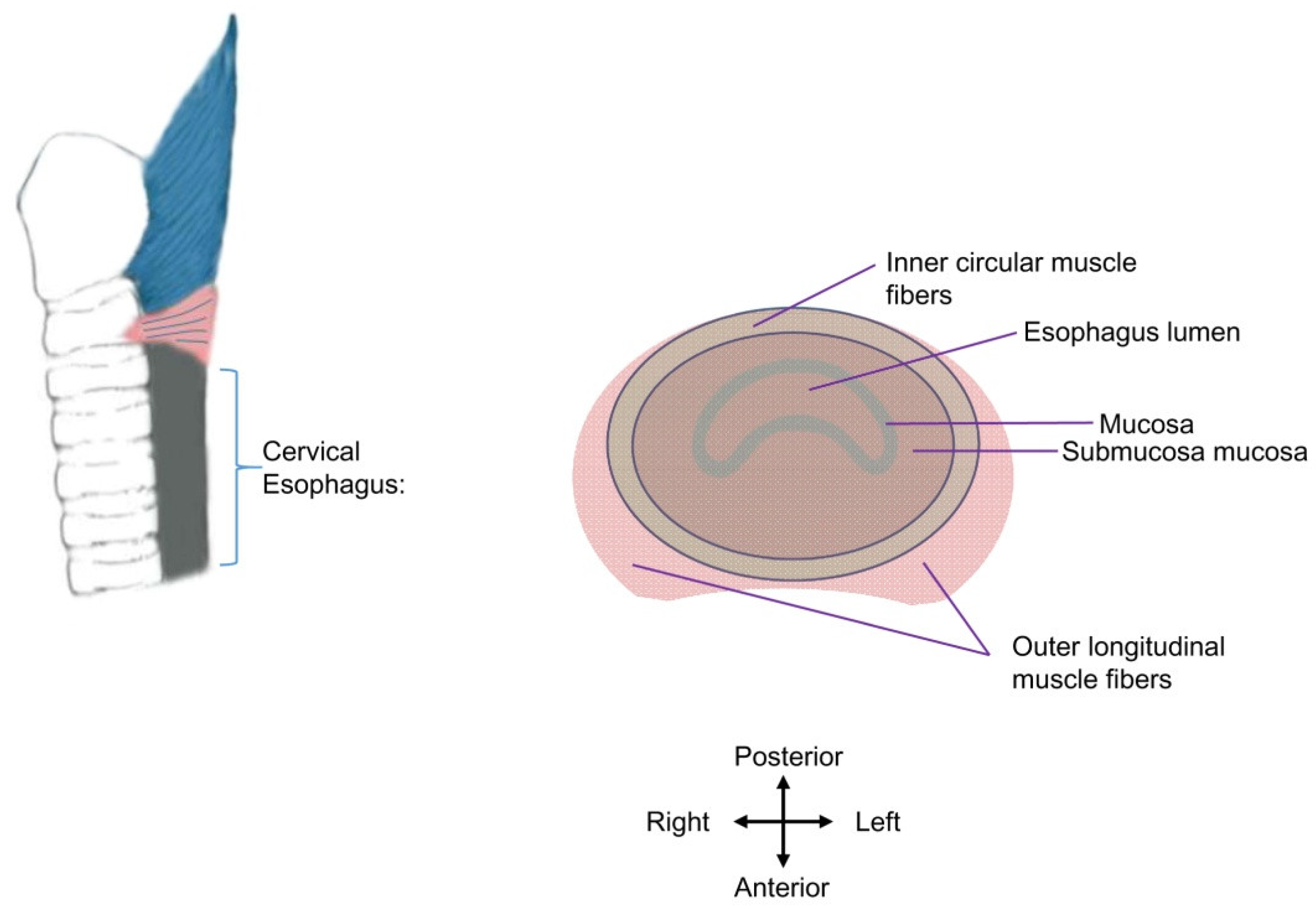
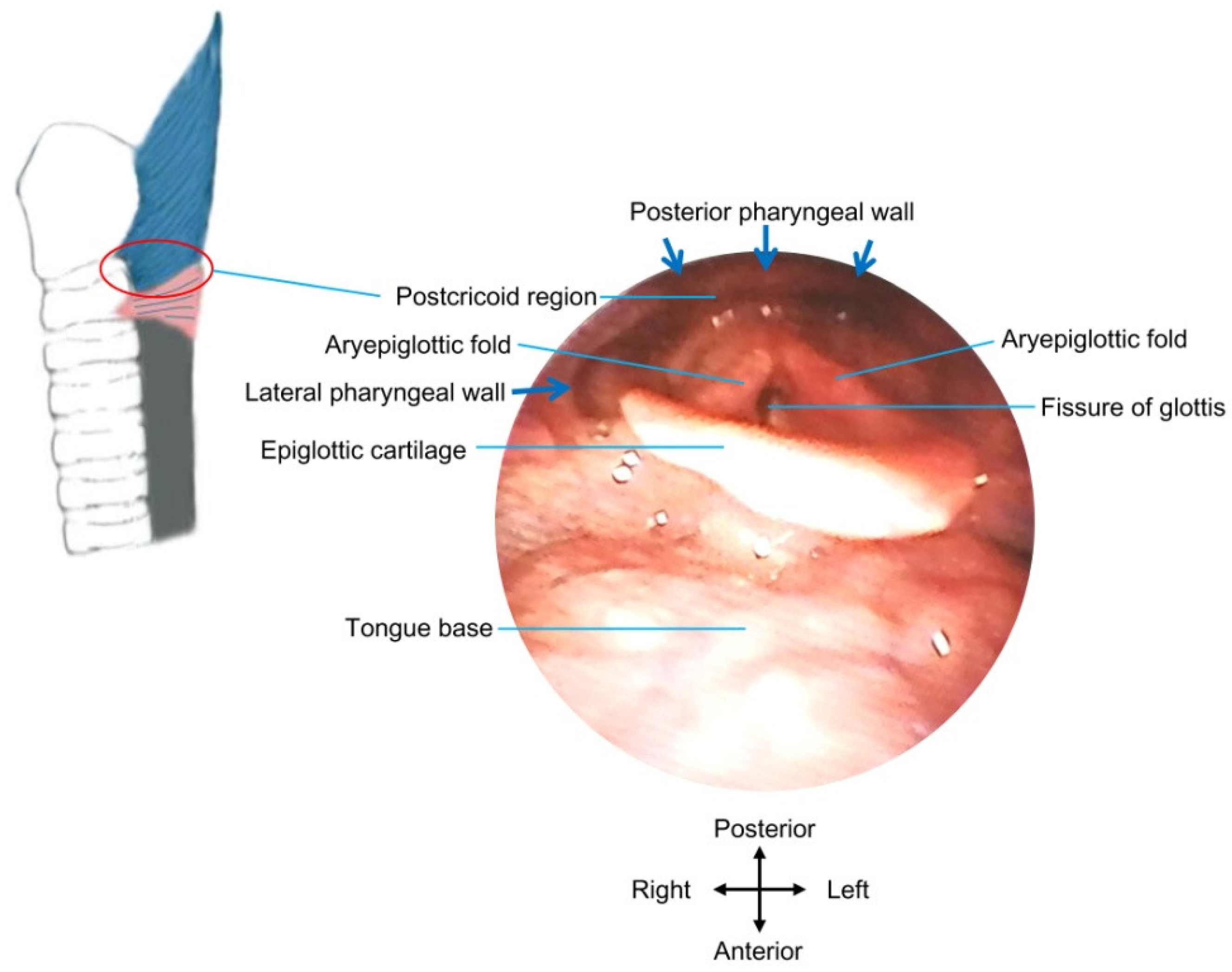
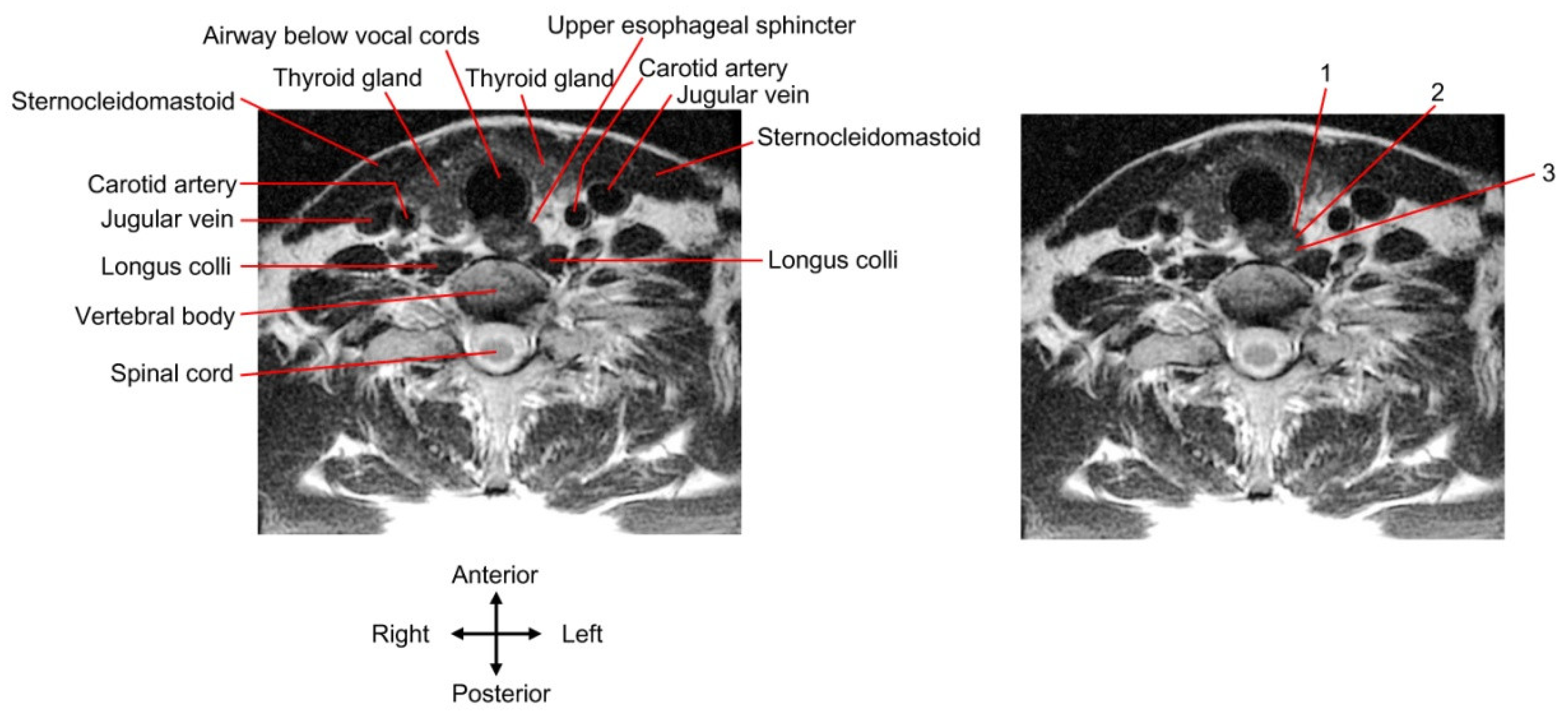
2. UES Anatomy and Function
3. Length of UES Dysfunction
4. Factors Influencing Effects of Botulinum Toxin Injection
5. Guiding Techniques for Botulinum Toxin Injection
6. Summary and Discussion
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Takizawa, C.; Gemmell, E.; Kenworthy, J.; Speyer, R.A. Systematic Review of the Prevalence of Oropharyngeal Dysphagia in Stroke, Parkinson’s Disease, Alzheimer’s Disease, Head Injury, and Pneumonia. Dysphagia 2016, 31, 434–441. [Google Scholar] [CrossRef] [PubMed]
- Espinosa-Val, M.C.; Martín-Martínez, A.; Graupera, M.; Arias, O.; Elvira, A.; Cabré, M.; Palomera, E.; Bolívar-Prados, M.; Clavé, P.; Ortega, O. Prevalence, Risk Factors, and Complications of Oropharyngeal Dysphagia in Older Patients with Dementia. Nutrients 2020, 12, 863. [Google Scholar] [CrossRef] [PubMed]
- Aldridge, K.J.; Taylor, N.F. Dysphagia is a common and serious problem for adults with mental illness: A systematic review. Dysphagia 2012, 27, 124–137. [Google Scholar] [CrossRef] [PubMed]
- Madhavan, A.; LaGorio, L.A.; Crary, M.A.; Dahl, W.J.; Carnaby, G.D. Prevalence of and Risk Factors for Dysphagia in the Community Dwelling Elderly: A Systematic Review. J. Nutr. Health Aging 2016, 20, 806–815. [Google Scholar] [CrossRef]
- Jadcherla, S. Dysphagia in the high-risk infant: Potential factors and mechanisms. Am. J. Clin. Nutr. 2016, 103, 622S–628S. [Google Scholar] [CrossRef]
- Jones, C.A.; Knigge, M.A.; McCulloch, T.M. Speech pathologist practice patterns for evaluation and management of suspected cricopharyngeal dysfunction. Dysphagia 2014, 29, 332–339. [Google Scholar] [CrossRef]
- Alfonsi, E.; Restivo, D.A.; Cosentino, G.; De Icco, R.; Bertino, G.; Schindler, A.; Todisco, M.; Fresia, M.; Cortese, A.; Prunetti, P.; et al. Botulinum Toxin Is Effective in the Management of Neurogenic Dysphagia. Clinical-Electrophysiological Findings and Tips on Safety in Different Neurological Disorders. Front. Pharmacol. 2017, 8, 80. [Google Scholar] [CrossRef]
- Sivarao, D.V.; Goyal, R.K. Functional anatomy and physiology of the upper esophageal sphincter. Am. J. Med. 2000, 108, 27S–37S. [Google Scholar] [CrossRef]
- Miller, L.S.; Dai, Q.; Sweitzer, B.A.; Thangada, V.; Kim, J.K.; Thomas, B.; Parkman, H.; Soliman, A.M. Evaluation of the upper esophageal sphincter (UES) using simultaneous high-resolution endoluminal sonography (HRES) and manometry. Dig. Dis. Sci. 2004, 49, 703–709. [Google Scholar] [CrossRef]
- Lang, I.M.; Shaker, R. Anatomy and physiology of the upper esophageal sphincter. Am. J. Med. 1997, 103, 50S–55S. [Google Scholar] [CrossRef]
- Singh, S.; Hamdy, S. The upper oesophageal sphincter. Neurogastroenterol. Motil. 2005, 17 (Suppl. S1), 3–12. [Google Scholar] [CrossRef] [PubMed]
- Elidan, J.; Shochina, M.; Gonen, B.; Gay, I. Electromyography of the inferior constrictor and cricopharyngeal muscles during swallowing. Ann. Otol. Rhinol. Laryngol. 1990, 99, 466–469. [Google Scholar] [CrossRef] [PubMed]
- Shipp, T.; Deatsch, W.W.; Robertson, K. Pharyngoesophageal muscle activity during swallowing in man. Laryngoscope 1970, 80, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Van Overbeek, J.J.; Wit, H.P.; Paping, R.H.; Segenhout, H.M. Simultaneous manometry and electromyography in the pharyngoesophageal segment. Laryngoscope 1985, 95, 582–584. [Google Scholar] [CrossRef]
- Cook, I.J.; Dodds, W.J.; Dantas, R.O.; Massey, B.; Kern, M.K.; Lang, I.M.; Brasseur, J.G.; Hogan, W.J. Opening mechanisms of the human upper esophageal sphincter. Am. J. Physiol. 1989, 257, G748–G759. [Google Scholar] [CrossRef] [PubMed]
- Kahrilas, P.J.; Dodds, W.J.; Dent, J.; Logemann, J.A.; Shaker, R. Upper esophageal sphincter function during deglutition. Gastroenterology 1988, 95, 52–62. [Google Scholar] [CrossRef]
- Sokol, E.M.; Heitmann, P.; Wolf, B.S.; Cohen, B.R. Simultaneous cineradiographic and manometric study of the pharynx, hypopharynx, and cervical esophagus. Gastroenterology 1966, 51, 960–974. [Google Scholar] [CrossRef]
- Nilsson, M.E.; Isberg, A.; Schiratzki, H. The location of the upper oesophageal sphincter and its behaviour during bolus propagation--a simultaneous cineradiographic and manometric investigation. Clin. Otolaryngol. Allied Sci. 1989, 14, 61–65. [Google Scholar] [CrossRef]
- Allen, J.E. Cricopharyngeal function or dysfunction: What’s the deal. Curr. Opin. Otolaryngol. Head Neck Surg. 2016, 24, 494–499. [Google Scholar] [CrossRef]
- Davis, M.V.; Merati, A.L.; Jaradeh, S.S.; Blumin, J.H. Myosin heavy chain composition and fiber size of the cricopharyngeus muscle in patients with achalasia and normal subjects. Ann. Otol. Rhinol. Laryngol. 2007, 116, 643–646. [Google Scholar] [CrossRef]
- Barnes, M.A.; Ho, A.S.; Malhotra, P.S.; Koltai, P.J.; Messner, A. The use of botulinum toxin for pediatric cricopharyngeal achalasia. Int. J. Pediatr. Otorhinolaryngol. 2011, 75, 1210–1214. [Google Scholar] [CrossRef] [PubMed]
- Chun, R.; Sitton, M.; Tipnis, N.A.; Arvedson, J.C.; Rao, A.; Dranove, J.; Brown, D.J. Endoscopic cricopharyngeal myotomy for management of cricopharyngeal achalasia (CA) in an 18-month-old child. Laryngoscope 2013, 123, 797–800. [Google Scholar] [CrossRef] [PubMed]
- Huoh, K.C.; Messner, A.H. Cricopharyngeal achalasia in children: Indications for treatment and management options. Curr. Opin. Otolaryngol. Head Neck Surg. 2013, 21, 576–580. [Google Scholar] [CrossRef] [PubMed]
- Scholes, M.A.; McEvoy, T.; Mousa, H.; Wiet, G.J. Cricopharyngeal achalasia in children: Botulinum toxin injection as a tool for diagnosis and treatment. Laryngoscope 2014, 124, 1475–1480. [Google Scholar] [CrossRef] [PubMed]
- Asherson, N. Achalasia of the cricopharyngeal sphincter; a record of case, with profile pharyngograms. J. Laryngol. Otol. 1950, 64, 747–758. [Google Scholar] [CrossRef] [PubMed]
- Brisinda, G.; Sivestrini, N.; Bianco, G.; Maria, G. Treatment of gastrointestinal sphincters spasms with botulinum toxin A. Toxins 2015, 7, 1882–1916. [Google Scholar] [CrossRef]
- Hickey, S.A. Neck and Upper Aerodigestive Tract-Pharynx. In Gray’s Anatomy, 39th ed.; Standring, S., Ed.; Churchill Livingstone: London, UK, 2004; pp. 628–632. [Google Scholar]
- Miwa, K.; Tsutsumi, M.; Fukino, K.; Eguchi, K.; Okada, R.; Akita, K. An anatomical study of the anterior wall of the hypopharyngeal and the cervical esophageal junction. Auris Nasus Larynx 2020, 47, 849–855. [Google Scholar] [CrossRef]
- Moriniere, S.; Hammoudi, K.; Marmouset, F.; Bakhos, D.; Beutter, P.; Patat, F. Ultrasound analysis of the upper esophageal sphincter during swallowing in the healthy subject. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2013, 130, 321–325. [Google Scholar] [CrossRef]
- Kacar, S.; Uysal, S.; Kuran, S.; Dagli, U.; Ozin, Y.; Karabulut, E.; Sasmaz, N. Transcutaneous cervical esophagus ultrasound in adults: Relation with ambulatory 24-h pH-monitoring and esophageal manometry. World J. Gastroenterol. 2007, 13, 5245–5252. [Google Scholar] [CrossRef]
- Mateen, M.A.; Kaffes, A.J.; Sriram, P.V.; Rao, G.V.; Reddy, D.N. Modified technique of high-resolution ultrasonography of the normal cervical esophagus. J. Gastroenterol. Hepatol. 2006, 21, 1660–1663. [Google Scholar] [CrossRef]
- Jacob, P.; Kahrilas, P.J.; Logemann, J.A.; Shah, V.; Ha, T. Upper esophageal sphincter opening and modulation during swallowing. Gastroenterology 1989, 97, 1469–1478. [Google Scholar] [CrossRef]
- Cock, C.; Jones, C.A.; Hammer, M.J.; Omari, T.I.; McCulloch, T.M. Modulation of upper esophageal sphincter (UES) relaxation and opening during volume swallowing. Dysphagia 2017, 32, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Logemann, J.A.; Pauloski, B.R.; Rademaker, A.W.; Colangelo, L.A.; Kahrilas, P.J.; Smith, C.H. Temporal and biomechanical characteristics of oropharyngeal swallow in younger and older men. J. Speech Lang. Hear. Res. 2000, 43, 1264–1274. [Google Scholar] [CrossRef] [PubMed]
- Popli, R.K.; Helm, J.F. Endoscopic images in cricopharyngeal dysfunction. Gastrointest. Endosc. 2001, 54, 752. [Google Scholar] [CrossRef]
- Hernandez, L.V.; Dua, K.S.; Surapaneni, S.N.; Rittman, T.; Shaker, R. Anatomic-manometric correlation of the upper esophageal sphincter: A concurrent US and manometry study. Gastrointest. Endosc. 2010, 72, 587–592. [Google Scholar] [CrossRef]
- Goyal, R.K.; Martin, S.B.; Shapiro, J.; Spechler, S.J. The role of cricopharyngeus muscle in pharyngoesophageal disorders. Dysphagia 1993, 8, 252–258. [Google Scholar] [CrossRef]
- Zaino, C.; Jacobson, H.G.; Lepow, H.; Ozturk, C. The Pharyngoesophageal Sphincter. Radiology 1967, 89, 639. [Google Scholar] [CrossRef]
- Adams, C.L.; Lohan, S.; Bruce, A.; Kamalaraj, N.; Gunaratne, S.; White, R. Cricopharyngeal bar and dermatomyositis: A cause of rapidly progressive dysphagia. Int. J. Rheum. Dis. 2021, 24, 125–131. [Google Scholar] [CrossRef]
- Taira, K.; Yamamoto, T.; Mori-Yoshimura, M.; Sajima, K.; Takizawa, H.; Shinmi, J.; Oya, Y.; Nishino, I.; Takahashi, Y. Cricopharyngeal bar on videofluoroscopy: High specificity for inclusion body myositis. J. Neurol. 2021, 268, 1016–1024. [Google Scholar] [CrossRef]
- Choksi, Y.A.; Chaparro, J.; Blanco, M.; Sharda, R.; Sarker, S.; Ferguson, S.; Higginbotham, T.; Hiremath, G.; Revetta, F.; Washington, M.K.; et al. Impedance and histologic characteristics of the sub-laryngeal esophagus distinguish eosinophilic esophagitis from other esophageal disorders. Clin. Gastroenterol. Hepatol. 2020, 18, 1727–1735.e2. [Google Scholar] [CrossRef]
- Huai, J.; Hou, Y.; Guan, J.; Zhang, Y.; Wang, Y.; Zhang, Y.; Yue, S. Botulinum toxin A Injection using esophageal balloon radiography combined with CT guidance for the treatment of cricopharyngeal dysphagia. Dysphagia 2020, 35, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Levine, M.S.; Rubesin, S.E. Diseases of the esophagus: A pattern approach. Abdom. Radiol. 2017, 42, 2199–2218. [Google Scholar] [CrossRef] [PubMed]
- Gagic, N.M. Cricopharyngeal myotomy. Can. J. Surg. 1983, 26, 47–49. [Google Scholar] [PubMed]
- Benedict, E.B.; Sweet, R.H. Dysphagia due to hypertrophy of the cricopharyngeus muscle or hypopharyngeal bar. N. Engl. J. Med. 1955, 253, 1161–1162. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.B.; Tanaka, E.; Ensrud, E. Motions of the posterior pharyngeal wall in human swallowing: A quantitative videofluorographic study. Arch. Phys. Med. Rehabil. 2000, 81, 1520–1526. [Google Scholar] [CrossRef]
- Nilsson, M.E.; Isacsson, G.; Isberg, A.; Schiratzki, H. Mobility of the upper esophageal sphincter in relation to the cervical spine: A morphologic study. Dysphagia 1989, 3, 161–165. [Google Scholar] [CrossRef]
- Shimada, K.; Gasser, R.F. Variations of the pharyngeal raphe. Clin. Anat. 1988, 1, 285. [Google Scholar] [CrossRef]
- Aoki, K.R. Pharmacology and immunology of botulinum toxin serotypes. J. Neurol. 2001, 248 (Suppl. S1), 3–10. [Google Scholar] [CrossRef]
- Brin, M.F.; James, C.; Maltman, J. Botulinum toxin type A products are not interchangeable: A review of the evidence. Biologics 2014, 8, 227–241. [Google Scholar] [CrossRef]
- Ramirez-Castaneda, J.; Jankovic, J.; Comella, C.; Dashtipour, K.; Fernandez, H.H.; Mari, Z. Diffusion, spread, and migration of botulinum toxin. Mov. Disord. 2013, 28, 1775–1783. [Google Scholar] [CrossRef]
- Mu, L.; Sanders, I. Neuromuscular organization of the human upper esophageal sphincter. Ann. Otol. Rhinol. Laryngol. 1998, 107, 370–377. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.; Shah, P.; Collins, P.; Wigley, C. Heart and Mediastinum-Mediastinum. In Gray’s Anatomy, 39th ed.; Standring, S., Ed.; Churchill Livingstone: London, UK, 2004; pp. 986–987. [Google Scholar]
- Trindade de Almeida, A.R.; Marques, E.; de Almeida, J.; Cunha, T.; Boraso, R. Pilot study comparing the diffusion of two formulations of botulinum toxin type A in patients with forehead hyperhidrosis. Dermatol. Surg. 2007, 33, S37–S43. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.Y.; Chen, S.J.; Zhou, J. Diffuseness comparison of two kinds of botulinum toxins type A on the forehead. Chin. J. Med. Aesthet. Cosmetol. 2016, 22, 150–153. [Google Scholar]
- Carli, L.; Montecucco, C.; Rossetto, O. Assay of diffusion of different botulinum neurotoxin type a formulations injected in the mouse leg. Muscle Nerve 2009, 40, 374–380. [Google Scholar] [CrossRef]
- Hallett, M. Explanation of timing of botulinum neurotoxin effects, onset and duration, and clinical ways of influencing them. Toxicon 2015, 107, 64–67. [Google Scholar] [CrossRef]
- Elwischger, K.; Kasprian, G.; Weber, M.; Meyerspeer, M.; Linder, C.; Auff, E.; Prayer, D.; Sycha, T.; Kranz, G. Intramuscular distribution of botulinum toxin–visualized by MRI. J. Neurol. Sci. 2014, 344, 76–79. [Google Scholar] [CrossRef]
- Kim, H.S.; Hwang, J.H.; Jeong, S.T.; Lee, Y.T.; Lee, P.K.; Suh, Y.L.; Shim, J.S. Effect of muscle activity and botulinum toxin dilution volume on muscle paralysis. Dev. Med. Child. Neurol. 2003, 45, 200–206. [Google Scholar] [CrossRef]
- Hsu, T.S.; Dover, J.S.; Arndt, K.A. Effect of volume and concentration on the diffusion of botulinum exotoxin A. Arch. Dermatol. 2004, 140, 1351–1354. [Google Scholar] [CrossRef]
- Atkinson, S.I.; Rees, J. Botulinum toxin for cricopharyngeal dysphagia: Case reports of CT-guided injection. J. Otolaryngol. 1997, 26, 273–276. [Google Scholar]
- Kelly, E.A.; Koszewski, I.J.; Jaradeh, S.S.; Merati, A.L.; Blumin, J.H.; Bock, J.M. Botulinum toxin injection for the treatment of upper esophageal sphincter dysfunction. Ann. Otol. Rhinol. Laryngol. 2013, 122, 100–108. [Google Scholar] [CrossRef]
- Schneider, I.; Thumfart, W.F.; Pototschnig, C.; Eckel, H.E. Treatment of dysfunction of the cricopharyngeal muscle with botulinum A toxin: Introduction of a new, noninvasive method. Ann. Otol. Rhinol. Laryngol. 1994, 103, 31–35. [Google Scholar] [CrossRef] [PubMed]
- Brant, C.Q.; Siqueira, E.S.; Ferrari, A.P., Jr. Botulinum toxin for oropharyngeal dysphagia: Case report of flexible endoscope-guided injection. Dis. Esophagus 1999, 12, 68–73. [Google Scholar] [CrossRef] [PubMed]
- Alberty, J.; Oelerich, M.; Ludwig, K.; Hartmann, S.; Stoll, W. Efficacy of botulinum toxin A for treatment of upper esophageal sphincter dysfunction. Laryngoscope 2000, 110, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Shaw, G.Y.; Searl, J.P. Botulinum toxin treatment for cricopharyngeal dysfunction. Dysphagia 2001, 16, 161–167. [Google Scholar] [CrossRef]
- Haapaniemi, J.J.; Laurikainen, E.A.; Pulkkinen, J.; Marttila, R.J. Botulinum toxin in the treatment of cricopharyngeal dysphagia. Dysphagia 2001, 16, 171–175. [Google Scholar] [CrossRef]
- Moerman, M.; Callier, Y.; Dick, C.; Vermeersch, H. Botulinum toxin for dysphagia due to cricopharyngeal dysfunction. Eur. Arch. Otorhinolaryngol. 2002, 259, 1–3. [Google Scholar] [CrossRef]
- Terré, R.; Panadés, A.; Mearin, F. Botulinum toxin treatment for oropharyngeal dysphagia in patients with stroke. Neurogastroenterol. Motil. 2013, 25, 896-e702. [Google Scholar] [CrossRef]
- Jeong, S.H.; Kim, Y.J.; Kim, Y.J.; Park, K.D.; Kim, E.J.; Chung, J.W.; Kwon, K.A.; Kim, K.O.; Park, D.K.; Kim, J.H.; et al. Endoscopic botulinum toxin injection for treatment of pharyngeal dysphagia in patients with cricopharyngeal dysfunction. Scand. J. Gastroenterol. 2018, 53, 1201–1205. [Google Scholar] [CrossRef]
- Kim, B.W.; Kim, H.J.; Hyun, J.K.; Kim, S.Y.; Kim, T.U. Botulinum toxin injection in the treatment of postextubation dysphagia: A case report. Ann. Rehabil. Med. 2018, 42, 358–362. [Google Scholar] [CrossRef]
- Parameswaran, M.S.; Soliman, A.M. Endoscopic botulinum toxin injection for cricopharyngeal dysphagia. Ann. Otol. Rhinol. Laryngol. 2002, 111, 871–874. [Google Scholar] [CrossRef]
- Zaninotto, G.; Marchese Ragona, R.; Briani, C.; Costantini, M.; Rizzetto, C.; Portale, G.; Zanetti, L.; Masiero, S.; Costantino, M.; Nicoletti, L.; et al. The role of botulinum toxin injection and upper esophageal sphincter myotomy in treating oropharyngeal dysphagia. J. Gastrointest. Surg. 2004, 8, 997–1006. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.W.; Tarnopolsky, M.; Armstrong, D. Injection of botulinum toxin A to the upper esophageal sphincter for oropharyngeal dysphagia in two patients with inclusion body myositis. Can. J. Gastroenterol. 2004, 18, 397–399. [Google Scholar] [CrossRef] [PubMed]
- Chiu, M.J.; Chang, Y.C.; Hsiao, T.Y. Prolonged effect of botulinum toxin injection in the treatment of cricopharyngeal dysphagia: Case report and literature review. Dysphagia 2004, 19, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.Y.; Park, C.I.; Ohn, S.H.; Moon, J.Y.; Chang, W.H.; Park, S.W. Botulinum toxin type A for poststroke cricopharyngeal muscle dysfunction. Arch. Phys. Med. Rehabil. 2006, 87, 1346–1351. [Google Scholar] [CrossRef] [PubMed]
- Krause, E.; Schirra, J.; Gürkov, R. Botulinum toxin a treatment of cricopharyngeal dysphagia after subarachnoid hemorrhage. Dysphagia 2008, 23, 406–410. [Google Scholar] [CrossRef]
- Wang, Y.C.; Wu, C.H.; Shyu, S.G.; Hsiao, M.Y.; Wang, T.G. Ultrasonography-guided botulinum toxin injection to the cricopharyngeus muscle: A case report and technical notes. Med. Ultrason. 2020, 22, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Luan, S.; Wu, S.L.; Xiao, L.J.; Yang, H.Y.; Liao, M.X.; Wang, S.L.; Fan, S.N.; Ma, C. Comparison studies of ultrasound-guided botulinum toxin injection and balloon catheter dilatation in the treatment of neurogenic cricopharyngeal muscle dysfunction. NeuroRehabilitation 2021, 49, 629–639. [Google Scholar] [CrossRef]
- Xie, M.; Zeng, P.; Wan, G.; An, D.; Tang, Z.; Li, C.; Wei, X.; Shi, J.; Zhang, Y.; Dou, Z.; et al. The effect of combined guidance of botulinum toxin injection with ultrasound, catheter balloon, and electromyography on neurogenic cricopharyngeal dysfunction: A prospective study. Dysphagia 2021. [Google Scholar] [CrossRef]
- Chen, J.M.; Chen, Y.J.; Ni, J.; Wang, Z.Y. Ultrasound, electromyography, and balloon guidance for injecting botulinum toxin for cricopharyngeal achalasia: A case report. Medicine 2021, 100, e24909. [Google Scholar] [CrossRef]
- Zhu, L.; Chen, J.; Shao, X.; Pu, X.; Zheng, J.; Zhang, J.; Wu, X.; Wu, D. Botulinum toxin A injection using ultrasound combined with balloon guidance for the treatment of cricopharyngeal dysphagia: Analysis of 21 cases. Scand. J. Gastroenterol. 2022, 1–7. [Google Scholar] [CrossRef]
- Wei, P.; Xu, Y.; Zhang, Z.; Zhang, S.; Lv, Z. Treatment for upper esophageal sphincter dysfunction in a patient with poststroke dysphagia: A case report. Medicine 2019, 98, e14988. [Google Scholar] [CrossRef] [PubMed]
- Murry, T.; Wasserman, T.; Carrau, R.L.; Castillo, B. Injection of botulinum toxin A for the treatment of dysfunction of the upper esophageal sphincter. Am. J. Otolaryngol. 2005, 26, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Blitzer, A.; Brin, M.F. Use of botulinum toxin for diagnosis and management of cricopharyngeal achalasia. Otolaryngol. Head Neck Surg. 1997, 116, 328–330. [Google Scholar] [CrossRef]
- Woisard-Bassols, V.; Alshehri, S.; Simonetta-Moreau, M. The effects of botulinum toxin injections into the cricopharyngeus muscle of patients with cricopharyngeus dysfunction associated with pharyngo-laryngeal weakness. Eur. Arch. Otorhinolaryngol. 2013, 270, 805–815. [Google Scholar] [CrossRef]
- Masiero, S.; Briani, C.; Marchese-Ragona, R.; Giacometti, P.; Costantini, M.; Zaninotto, G. Successful treatment of long-standing post-stroke dysphagia with botulinum toxin and rehabilitation. J. Rehabil. Med. 2006, 38, 201–203. [Google Scholar] [CrossRef][Green Version]
- Restivo, D.A.; Marchese-Ragona, R.; Lauria, G.; Squatrito, S.; Gullo, D.; Vigneri, R. Botulinum toxin treatment for oropharyngeal dysphagia associated with diabetic neuropathy. Diabetes Care 2006, 29, 2650–2653. [Google Scholar] [CrossRef]
- Restivo, D.A.; Marchese-Ragona, R.; Patti, F.; Solaro, C.; Maimone, D.; Zappala, G.; Pavone, A. Botulinum toxin improves dysphagia associated with multiple sclerosis. Eur. J. Neurol. 2011, 18, 486–490. [Google Scholar] [CrossRef]
- Alfonsi, E.; Merlo, I.M.; Ponzio, M.; Montomoli, C.; Tassorelli, C.; Biancardi, C.; Lozza, A.; Martignoni, E. An electrophysiological approach to the diagnosis of neurogenic dysphagia: Implications for botulinum toxin treatment. J. Neurol. Neurosurg. Psychiatry 2010, 81, 54–60. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Literature | Toxin | Dose | Dilution Volume | Injection Sites | Guiding Techniques |
|---|---|---|---|---|---|
| [7] | Xeomin | 15 or 20 U | 5 U/0.1 mL | The cricopharyngeus (on the side showing greater muscle hyperactivity) | EMG |
| [42] | Hengli | 75 U | 100 U/2 mL | The cricopharyngeus muscle at three different locations | CT + balloon |
| [62] | BOTOX | 15–100 U | 0.4–0.5 mL | Horizontal component of the posterior belly of the cricopharyngeus | EMG, or laryngoscopy |
| [63] | Dysport | 80–120 U | 2.5 mL | Dorsomedial part, bilaterally ventrolateral parts | Rigid esophagoscopy + EMG |
| [65] | BOTOX | 100 U | 2.5 mL | Posterior and both lateral sides of the cricopharyngeus | Rigid laryngoscope |
| [66] | BOTOX | 25–50 U | 25 U/mL | Rigid endoscopy: 4 quadrants; flexible endoscopy: dorsomedial part and bilateral ventromedial parts | Rigid endoscopy + EMG, or flexible endoscopy |
| [67] | BOTOX | 14–50 U | 100 U/mL | Two posterolateral parts | Hypopharygoscopy |
| [68] | BOTOX | 100 U | 0.5 mL | Dorsomedially, and ventrolaterally on both sides | Nasopharyngolaryngoscopy |
| [69] | BOTOX | 100 U | 1 mL | Posterior part (40 U) and both lateral sides (30 U each) of the cricopharyngeus muscle | Flexible endoscope |
| [76] | BOTOX | 100 U | 2 mL | Posterior part (50 U) and both lateral sides (25 U each) of the cricopharyngeal muscle | Flexible endoscope |
| [77] | Dysport | 180 U | 200 U/mL | Dorsal part of cricopharyngeal muscle | Endoscopy |
| [79] | BOTOX | 50 U | 1 mL | Left side of the cricopharyngeus | Ultrasound |
| [80] | BOTOX | 30–100 U | 100 U/mL | Left or right side of the cricopharyngeus | Ultrasound + balloon + EMG |
| [81] | BOTOX | 30 U | 0.4 mL | The cricopharyngeus muscle | Ultrasound + balloon + EMG |
| [83] | Hengli | 60 U | 20 U/0.1 mL | Left side of the cricopharyngeus muscle | Ultrasound + balloon |
| [84] | BOTOX | 100 U | 2 mL | The cricopharyngeus, 2 cm above (i.e., inferior constrictor), and 1–2 cm below t (i.e., cervical esophagus) | EMG |
| [86] | BOTOX or Dysport | Low: 10–15 U BOTOX or 30–60 U Dysport; Intermediate: 20 U BOTOX or 80 U Dysport; High: 25–30 U BOTOX or up to 100 U Dysport | Dysport 500 U/2.5 mL; BOTOX 100 U/2 mL | One or two sides in the cricopharyngeal muscle | EMG |
| [88] | Dysport | 60 U | 30 U/2 mL | Bilateral cricopharyngeal muscle | EMG |
| [89] | BOTOX | 20 U | 10 U/2 mL | Each side of the cricopharyngeal muscle | EMG |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, P. Botulinum Toxin Injection for the Treatment of Upper Esophageal Sphincter Dysfunction. Toxins 2022, 14, 321. https://doi.org/10.3390/toxins14050321
Wei P. Botulinum Toxin Injection for the Treatment of Upper Esophageal Sphincter Dysfunction. Toxins. 2022; 14(5):321. https://doi.org/10.3390/toxins14050321
Chicago/Turabian StyleWei, Pengxu. 2022. "Botulinum Toxin Injection for the Treatment of Upper Esophageal Sphincter Dysfunction" Toxins 14, no. 5: 321. https://doi.org/10.3390/toxins14050321
APA StyleWei, P. (2022). Botulinum Toxin Injection for the Treatment of Upper Esophageal Sphincter Dysfunction. Toxins, 14(5), 321. https://doi.org/10.3390/toxins14050321