Incidence Rate of Bee Venom Acupuncture Related Anaphylaxis: A Systematic Review

 ,
, 



Abstract
:1. Introduction
2. Results
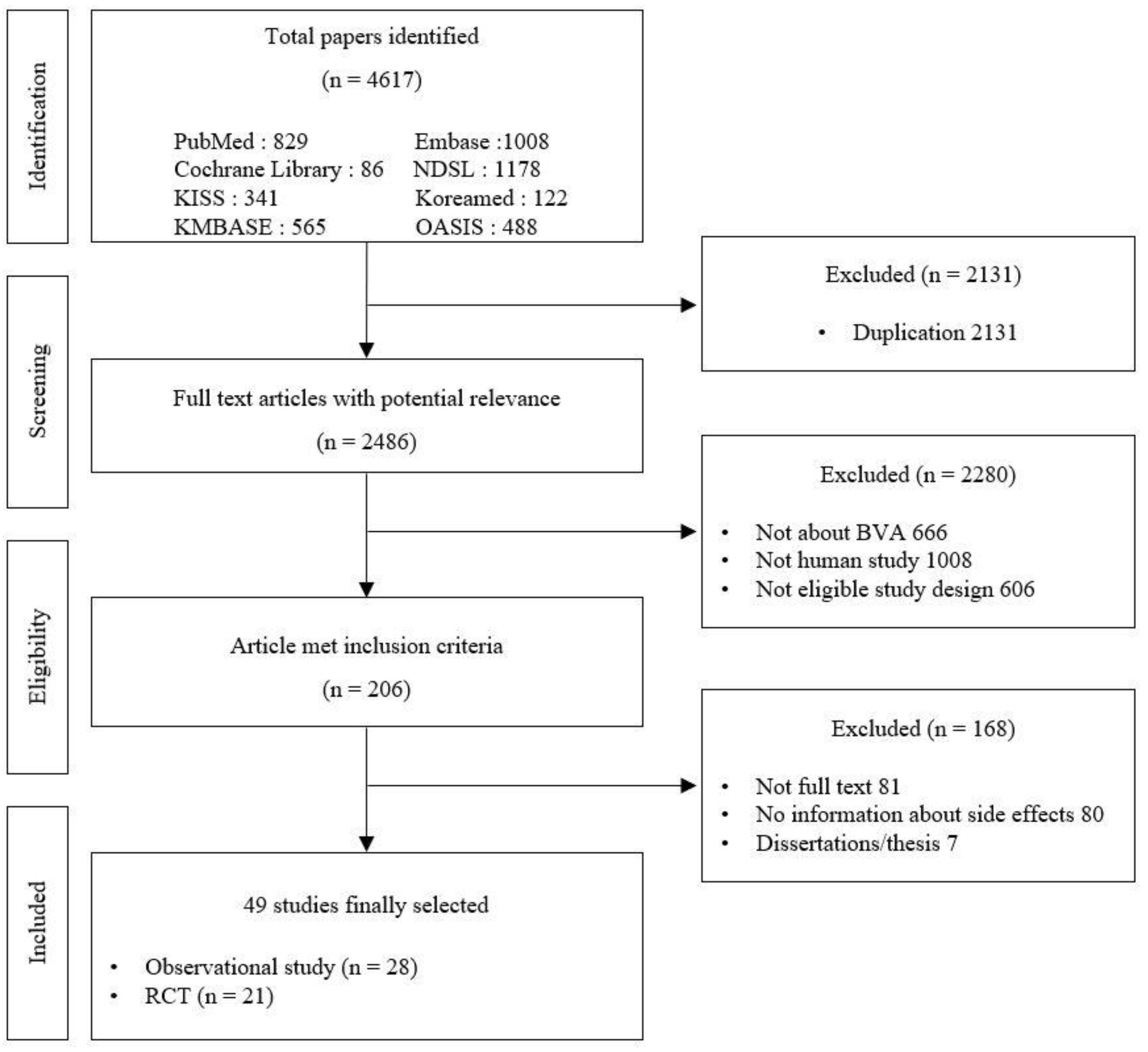
2.1. Characteristics of the Included Studies
2.2. Incidence of Anaphylaxis in Response to BVA
2.3. Incidence of Anaphylaxis in Response to BVA by Subgroup
2.4. Characteristics of Patients with Anaphylaxis
3. Discussion
4. Materials and Methods
4.1. Search Strategy
4.2. Inclusion and Exclusion Criteria
4.2.1. Types of Study Design
4.2.2. Types of Participants
4.2.3. Types of Interventions and Comparisons
4.2.4. Type of Outcome Measures
4.3. Data Extraction and Review Process
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Castro, H.J.; Mendez-Inocencio, J.I.; Omidvar, B.; Omidvar, J.; Santilli, J.; Nielsen, H.S., Jr.; Pavot, A.P.; Richert, J.R.; Bellanti, J.A. A phase I study of the safety of honeybee venom extract as a possible treatment for patients with progressive forms of multiple sclerosis. Allergy Asthma Proc. 2005, 26, 470–476. [Google Scholar] [PubMed]
- Ali, M.A.A.S.M. Studies on bee venom and its medical uses. Int. J. Adv. Res. Technol. 2012, 1, 69–83. [Google Scholar]
- Rady, I.; Siddiqui, I.A.; Rady, M.; Mukhtar, H. Melittin, a major peptide component of bee venom, and its conjugates in cancer therapy. Cancer Lett. 2017, 402, 16–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.J. Principle of Herbal Acupuncture and Clinical Application; Iljoongsa: Seoul, Korea, 1999. [Google Scholar]
- Park, J.S.; Lee, M.J.; Chung, K.H.; Ko, D.K.; Chung, H. Live Bee Acupuncture (Bong-Chim) Dermatitis: Dermatitis due to Live Bee Acupuncture Therapy in Korea. Int. J. Dermatol. 2013, 52, 1519–1524. [Google Scholar] [CrossRef]
- Abdela, N.; Jilo, K. Bee Venom and its Therapeutic Values: A Review. Adv. Life Sci. Technol. 2016, 44, 18–22. [Google Scholar]
- Komi, D.E.A.; Shafaghat, F.; Zwiener, R.D. Immunology of bee venom. Clin. Rev. Allergy Immunol. 2018, 54, 386–396. [Google Scholar] [CrossRef]
- Pucca, M.B.; Cerni, F.A.; Oliveira, I.S.; Jenkins, T.P.; Argemí, L.; Sørensen, C.V.; Ahmadi, S.; Barbosa, J.E.; Laustsen, A.H. Bee updated: Current knowledge on bee venom and bee envenoming therapy. Front. Immunol. 2019, 10, 2090. [Google Scholar] [CrossRef] [Green Version]
- Magrioti, V.; Kokotos, G. Phospholipase A2 inhibitors as potential therapeutic agents for the treatment of inflammatory diseases. Expert Opin. Ther. Pat. 2010, 20, 1–18. [Google Scholar] [CrossRef]
- Cherniack, E.P.; Govorushko, S. To bee or not to bee: The potential efficacy and safety of bee venom acupuncture in humans. Toxicon 2018, 154, 74–78. [Google Scholar] [CrossRef]
- Choi, Y.C.; Kwon, K.R.; Choi, S.H. Purification of Peptide Components including Melittin from Bee Venom using gel filtration chromatography and propionic acid urea polyacrylamide gel electrophoresis. J. Korean Pharmacopunct. Inst. 2006, 9, 105–111. [Google Scholar]
- Yi, W.S.; Kim, S.S. Reporting of adverse events in randomized controlled trials of bee venom acupuncture: A systematic review. J. Korean Med. Rehabil. 2014, 24, 97–109. [Google Scholar]
- Jang, S.B.; Kim, K.H. Clinical effectiveness and adverse events of bee venom therapy: A systematic review of randomized controlled trials. Toxins 2020, 12, 558. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.J.; Ahn, Y.C.; Kim, Y.I.; Oh, M.S.; Park, Y.C.; Son, C.G. Incidence Rate of Hypersensitivity Reactions to Bee-Venom Acupuncture. Front. Pharmacol. 2020, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Weis, W.A.; Ripari, N.; Conte, F.L.; da Silva Honorio, M.; Sartori, A.A.; Matucci, R.H.; Sforcin, J.M. An overview about apitherapy and its clinical applications. Phytomedicine 2022, 2, 100239. [Google Scholar] [CrossRef]
- Park, J.H.; Yim, B.K.; Lee, J.-H.; Lee, S.; Kim, T.-H. Risk associated with bee venom therapy: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0126971. [Google Scholar] [CrossRef] [Green Version]
- Jo, N.; Roh, J. Systemic immediate hypersensitive reactions after treatment with sweet bee venom: A case report. J. Pharmacopunct. 2015, 18, 59. [Google Scholar]
- Kim, K.; Jeong, H.; Lee, G.; Jang, S.; Yook, T. Characteristics of Adverse Events in Bee Venom Therapy Reported in South Korea: A Survey Study. Toxins 2022, 14, 18. [Google Scholar] [CrossRef]
- Hwang, Y.J.; Lee, B.C. Clinical study of anaphylaxis on bee-venom acupuncture. J. Acupunct. Res. 2000, 17, 149–159. [Google Scholar]
- Kim, M.R.; Shin, J.S.; Lee, J.; Lee, Y.J.; Ahn, Y.J.; Park, K.B.; Lee, H.D.; Lee, Y.; Kim, S.G.; Ha, I.H. Safety of Acupuncture and Pharmacopuncture in 80,523 Musculoskeletal Disorder Patients: A Retrospective Review of Internal Safety Inspection and Electronic Medical Records. Medicine 2016, 95, e3635. [Google Scholar] [CrossRef]
- Tupper, J.; Visser, S. Anaphylaxis: A review and update. Can. Fam. Physician 2010, 56, 1009–1011. [Google Scholar]
- Dhopeshwarkar, N.; Sheikh, A.; Doan, R.; Topaz, M.; Bates, D.W.; Blumenthal, K.G.; Zhou, L. Drug-induced anaphylaxis documented in electronic health records. J. Allergy Clin. Immunol. Pract. 2019, 7, 103–111. [Google Scholar] [CrossRef] [PubMed]
- Barton, S. Which clinical studies provide the best evidence?: The best RCT still trumps the best observational study. BMJ 2000, 321, 255–256. [Google Scholar] [CrossRef] [PubMed]
- Rudders, S.A.; Banerji, A.; Clark, S.; Camargo, C.A., Jr. Age-related differences in the clinical presentation of food-induced anaphylaxis. J. Pediatr. 2011, 158, 326–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richter, A.G.; Nightingale, P.; Huissoon, A.P.; Krishna, M.T. Risk factors for systemic reactions to bee venom in British beekeepers. Ann. Allergy Asthma Immunol. 2011, 106, 159–163. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, S.H.; Park, H.D.; Kim, W.Y.; Hong, E.S. Predictors of Anaphylactic Shock in Patients with Anaphylaxis after Exposure to Bee Venom. J. Korean Soc. Clin. Toxicol. 2010, 8, 30–36. [Google Scholar]
- Salvati, L.; Vitiello, G.; Parronchi, P. Gender differences in anaphylaxis. Curr. Opin. Allergy Clin. Immunol. 2019, 19, 417–424. [Google Scholar] [CrossRef]
- Baker, A.; Empson, M.; The, R.; Fitzharris, P. Skin testing for immediate hypersensitivity to corticosteroids: A case series and literature review. Clin. Exp. Allergy 2015, 45, 669–676. [Google Scholar] [CrossRef]
- Chu, C.S.; Park, H.S.; Kim, M.K.; Cha, B.C.; Lee, E.; Kwon, K.R. Expermental Studies of quantitative evaluation using HPLC and safety of Sweet Bee Venom. J. Pharmacopunct. 2007, 10, 81–86. [Google Scholar] [CrossRef]
- Kang, K.S.; Kwon, K.R. Experimental studies of validation and stability of sweet bee venom using HPLC. J. Pharmacopunct. 2009, 12, 33–50. [Google Scholar] [CrossRef]
- The ICD-10 Version. Available online: https://icd.who.int/browse10/2019/en#/ (accessed on 23 February 2022).
- Mueller, H.L. Diagnosis and treatment of insect sensitivity. J. Asthma Res. 1966, 3, 331–333. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Items | Observational Studies | RCTs | Total |
|---|---|---|---|
| Number of studies (%) | 28 (57) | 21 (43) | 49 (100) |
| Number of participants (%) | 59,030 (99) | 703 (1) | 59,733 (100) |
| Men/Women | 5227 (48)/5739 (52) | 176 (33)/371 (67) | 5403/6110 |
| No information a | 48,064 | 156 | 48,220 |
| Mean age (years) b | 47.5 ± 8.6 | 55.5 ± 6.83 | 51.1 ± 8.8 |
| Main complaints (No. of participants, studies) | |||
| G00–G99 c | 93 (4) | 20 (1) | 113 (5) |
| S00–T98 d | 16 (1) | 61 (2) | 77 (3) |
| M00–M99 e | 57,897 (15) | 551 (16) | 58,448 (31) |
| Others (obesity) | 0 (0) | 51 (1) | 51 (1) |
| No information a | 1024 (8) | 20 (1) | 1044 (9) |
| Skin test (No. of participants, studies) | |||
| Yes | 16,585 (14) | 375 (13) | 16,960 (27) |
| No | 0 (0) | 0 (0) | 0 (0) |
| No information a | 42,445 (14) | 328 (8) | 42,773 (22) |
| Publication year (No. of participants, studies) | |||
| –1999 | 31 (1) | 60 (1) | 91 (2) |
| 2000–2009 | 32,350 (10) | 409 (9) | 32,759 (19) |
| 2010–2021 | 26,649 (17) | 234 (11) | 26,883 (28) |
| Country (No. of participants, studies) | |||
| South Korea | 58,953 (26) | 683 (20) | 59,636 (46) |
| France | 0 (0) | 20 (1) | 20 (1) |
| Romania | 26 (1) | 0 (0) | 26 (1) |
| USA | 51 (1) | 0 (0) | 51 (1) |
| Group | Incidence (%, 95% CI) | ||
|---|---|---|---|
| Observational Studies (59,030 Participants) | RCTs (703 Participants) | Total (59,733 Participants) | |
| No. of anaphylaxis | 26 | 1 | 27 |
| Overall incidence in all studies | 0.044 (0.027–0.061) | 0.142 (−0.136 to 0.421) | 0.045 (0.028–0.062) |
| Incidence by subgroup (No. studies that presented data) | |||
| Sex (37) | |||
| Men | 0.019 (−0.019 to 0.057) | 0 | 0.019 (−0.018 to 0.055) |
| Women | 0.089 (0.011–0.167) | 0 | 0.083 (0.010–0.157) |
| Main complaints (39) | |||
| G00-G99 a | 1.075 (−1.021 to 3.171) | 0 | 0.885 (−0.842 to 2.612) |
| S00-T98 b | 0 | 1.639 (−1.547 to 4.826) | 1.299 (−1.230 to 3.828) |
| M00-M99 c | 0.043 (0.026–0.060) | 0 | 0.043 (0.026–0.060) |
| Others (obesity) | 0 | 0 | 0 |
| No information d | 0 | 0 | 0 |
| Skin test (49) | |||
| Yes | 0.036 (0.007–0.065) | 0.267 (−0.255 to 0.789) | 0.041 (0.011–0.072) |
| No | |||
| No information d | 0.047 (0.026–0.068) | 0 | 0.047 (0.026–0.067) |
| Publication year (49) | |||
| –1999 | 3.226 (−2.994 to 9.446) | 0 | 1.099 (−1.043 to 3.241) |
| 2000–2009 | 0.049 (0.025–0.074) | 0 | 0.049 (0.025–0.073) |
| 2010–2021 | 0.034 (0.012–0.056) | 0.379 (−0.362 to 1.120) | 0.037 (0.014–0.060) |
| Patient Number | Sex/Age | Concentration during Anaphylaxis | Volume during Anaphylaxis | No. Treatments until Anaphylaxis | Administration | Anaphylaxis Grade c | Treatment Result |
|---|---|---|---|---|---|---|---|
| P1 | Unknown | Unknown | Unknown | 4 | Unknown | III | Recovered |
| P2–5 | 4 patients /(Unknown) | Unknown | Unknown | Unknown | Unknown | Unknown | Unknown |
| P6–16 a | 11 patients /(40.9 ± 12 a) | Unknown | 1.6 cc ± 0.5 | 10.9 ± 6.8 | Unknown | Unknown | Recovered |
| P17 b | Unknown | Unknown | 0.4 cc | 24 | Intradermal | Unknown | Unknown |
| P18 | Unknown | 10,000:1 | Unknown | Unknown | Unknown | IV | Recovered |
| P19 | F/36 | Unknown | 2 cc | 6 | Intradermal | Unknown | Recovered |
| P20 | F/61 | 10,000:1 | 0.5 cc | 1 | Unknown | III | Recovered |
| P21 | F/65 | 10,000:1 | 0.1 cc | Test | Unknown | III | Recovered |
| P22 | F/77 | 10,000:1 | 1 cc | Unknown | Unknown | IV | Recovered |
| P23 | M/70 | 10,000:1 | 2 cc | 6 | Intramuscular | III | Recovered |
| P24 | F/59 | 10,000:1 | 2 cc | 2 | Intramuscular | IV | Recovered |
| P25 | F/62 | 10,000:1 | 2 cc | 13 | Intramuscular | III | Recovered |
| P26 | F/60 | 10,000:1 | 2 cc | 6 | Intramuscular | III | Recovered |
| P27 | F/42 | 10,000:1 | 2 cc | 22 | Intramuscular | IV | Recovered |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ko, S.-H.; Oh, H.-M.; Kwon, D.-Y.; Yang, J.-E.; Kim, B.-J.; Ha, H.-J.; Lim, E.-J.; Oh, M.-S.; Son, C.-G.; Lee, E.-J. Incidence Rate of Bee Venom Acupuncture Related Anaphylaxis: A Systematic Review. Toxins 2022, 14, 238. https://doi.org/10.3390/toxins14040238
Ko S-H, Oh H-M, Kwon D-Y, Yang J-E, Kim B-J, Ha H-J, Lim E-J, Oh M-S, Son C-G, Lee E-J. Incidence Rate of Bee Venom Acupuncture Related Anaphylaxis: A Systematic Review. Toxins. 2022; 14(4):238. https://doi.org/10.3390/toxins14040238
Chicago/Turabian StyleKo, Seong-Hwan, Hyeon-Muk Oh, Do-Young Kwon, Jae-Eun Yang, Byung-Jun Kim, Hyun-Ju Ha, Eun-Jin Lim, Min-Seok Oh, Chang-Gue Son, and Eun-Jung Lee. 2022. "Incidence Rate of Bee Venom Acupuncture Related Anaphylaxis: A Systematic Review" Toxins 14, no. 4: 238. https://doi.org/10.3390/toxins14040238
APA StyleKo, S.-H., Oh, H.-M., Kwon, D.-Y., Yang, J.-E., Kim, B.-J., Ha, H.-J., Lim, E.-J., Oh, M.-S., Son, C.-G., & Lee, E.-J. (2022). Incidence Rate of Bee Venom Acupuncture Related Anaphylaxis: A Systematic Review. Toxins, 14(4), 238. https://doi.org/10.3390/toxins14040238