Influential Factors of Local Tissue Necrosis after Taiwan Cobra Bites: A Secondary Analysis of the Clinical Significance of Venom Detection in Patients of Cobra Snakebites


Abstract
1. Introduction
2. Results
2.1. Patient Characteristics
2.2. Influential Factors of Local Tissue Necrosis
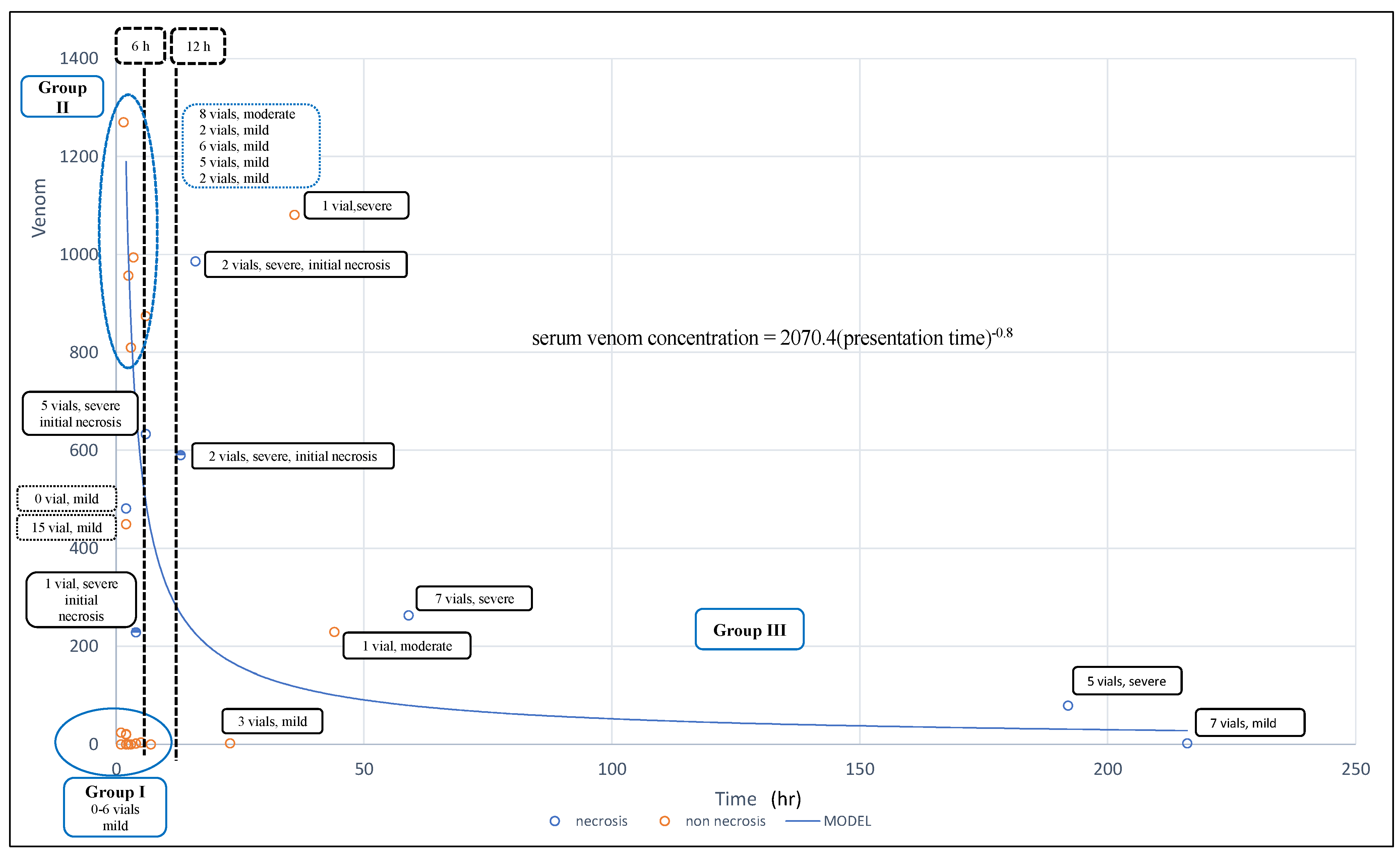
2.2.1. Patient Groups According to Presentation Time and Clinical Severity
2.2.2. Comparison between the Wound Necrosis and No Wound Necrosis Groups and Derived Influential Factors of Cobra Bites Associated with Wound Necrosis
or
(presentation time)0.8 × serum venom concentration = 2070.4
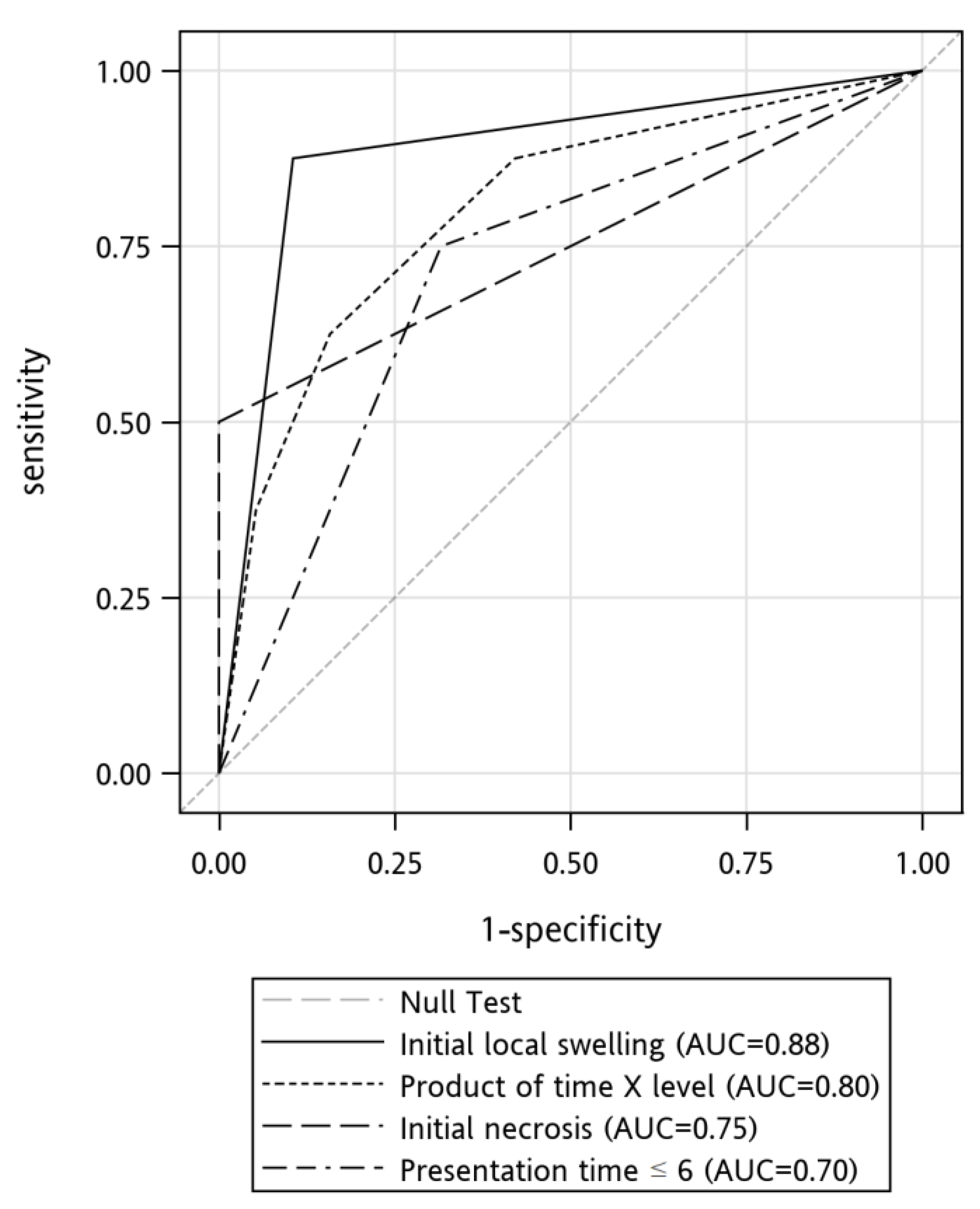
2.2.3. Development of the Clinical Prediction Rule for Wound Necrosis
3. Discussion
3.1. Influential Factors in Predicting the Development of Local Tissue Necrosis
3.2. Patient Presentation Time as an Influential Factor of Cobra-Bite Associated Wound Necrosis
3.3. Venom Level (Venom Load) As an Influential Factor of Cobra Bite Associated Wound Necrosis
3.4. Possible Clinical Applications of Our Study Findings in other Naja spp. Bites
3.5. Limitations
4. Conclusions
5. Materials and Methods
5.1. Settings, Patients, and Data Collection
5.2. The Severity of Local Manifestations of Envenomation
5.3. Study Protocol and Data Analysis
5.4. ELISA for Taiwan Cobra Venom
5.5. Statistics
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Alirol, E.; Sharma, S.K.; Bawaskar, H.S.; Kuch, U.; Chappuis, F. Snake bite in South Asia: A review. PLoS Negl. Trop. Dis. 2010, 4, e603. [Google Scholar] [CrossRef] [PubMed]
- FFaiz, M.A.; Ahsan, M.F.; Ghose, A.; Rahman, M.R.; Amin, R.; Hossain, M.; Tareq, M.N.; Jalil, M.A.; Kuch, U.; Theakston, R.D.; et al. Bites by the monocled cobra, Naja kaouthia, in Chittagong Division, Bangladesh: Epidemiology, clinical features of envenoming and management of 70 identified cases. Am. J. Trop. Med. Hyg. 2017, 96, 876–884. [Google Scholar] [CrossRef]
- Kularatne, S.A.; Budagoda, B.D.; Gawarammana, I.B.; Kularatne, W.K. Epidemiology, clinical profile and management issues of cobra (Naja naja) bites in Sri Lanka: First authenticated case series. Trans. R. Soc. Trop. Med. Hyg. 2009, 103, 924–930. [Google Scholar] [CrossRef] [PubMed]
- Pochanugool, C.; Limthongkul, S.; Wilde, H. Management of Thai cobra bites with a single bolus of antivenin. Wilderness Environ. Med. 1997, 8, 20–23. [Google Scholar] [CrossRef]
- Tilbury, C.R. Observations on the bite of the Mozambique spitting cobra (Naja mossambica mossambica). S. Afr. Med. J. 1982, 61, 308–313. [Google Scholar]
- Watt, G.; Padre, L.; Tuazon, L.; Theakston, R.D.; Laughlin, L. Bites by the Philippine cobra (Naja naja philippinensis): Prominent neurotoxicity with minimal local signs. Am. J. Trop. Med. Hyg. 1988, 39, 306–311. [Google Scholar] [CrossRef] [PubMed]
- Warrell, D.A.; Greenwood, B.M.; Davidson, N.M.; Ormerod, L.D.; Prentice, C.R.M. Necrosis, haemorrhage and complement depletion following bites by the spitting cobra (Naja nigricollis). QJM Int. J. Med. 1976, 45, 1–22. [Google Scholar]
- Chen, C.K.; Lin, C.C.; Shih, F.Y.; Chaou, C.H.; Lin, J.C.C.; Lai, T.I.; Tseng, C.Y.; Fang, C.C. Population-based study of venomous snakebite in Taiwan. J. Acute Med. 2015, 5, 38–42. [Google Scholar] [CrossRef]
- Kuo, T.P.; Wu, C.S. Clinico-pathological studies on snakebites in Taiwan. J. Formos Med. Assoc. 1972, 71, 447–466. [Google Scholar]
- Liao, W.B.; Lee, C.W.; Tsai, Y.S.; Liu, B.M.; Chung, K.J. Influential factors affecting prognosis of snakebite patients management: Kaohsiung Chang Gung Memorial Hospital experience. Chang Gung Med. J. 2000, 23, 577–583. [Google Scholar]
- Mao, Y.C.; Liu, P.Y.; Chiang, L.C.; Lai, C.S.; Lai, K.L.; Ho, C.H.; Wang, T.H.; Yang, C.C. Naja atra snakebite in Taiwan. Clin. Toxicol. 2018, 56, 273–280. [Google Scholar] [CrossRef]
- Rivel, M.; Solano, D.; Herrera, M.; Vargas, M.; Villalta, M.; Segura, Á.; Arias, A.S.; León, G.; Gutiérrez, J.M. Pathogenesis of dermonecrosis induced by venom of the spitting cobra, Naja nigricollis: An experimental study in mice. Toxicon 2016, 119, 171–179. [Google Scholar] [CrossRef]
- Liu, C.C.; Chou, Y.S.; Chen, C.Y.; Liu, K.L.; Huang, G.J.; Yu, J.S.; Wu, C.J.; Liaw, G.W.; Hsieh, C.H.; Chen, C.K. Pathogenesis of local necrosis induced by Naja atra venom: Assessment of the neutralization ability of Taiwanese freeze-dried neurotoxic antivenom in animal models. PLoS Negl. Trop. Dis. 2020, 14, e0008054. [Google Scholar] [CrossRef]
- Lin, C.C.; Chaou, C.H.; Tseng, C.Y. An investigation of snakebite antivenom usage in Taiwan. J. Formos Med. Assoc. 2016, 115, 672–677. [Google Scholar] [CrossRef]
- Wu, M.S.; Lee, J.T.; Sun, T.B.; Cheng, L.F.; Wang, C.H.; Hsu, H.D.; Huang, C.C.; Chien, S.H. Treatment of venomous snakebites in eastern Taiwan. JPSAROC 2009, 18, 257–265. [Google Scholar]
- Hung, D.Z.; Liau, M.Y.; Lin-Shiau, S.Y. The clinical significance of venom detection in patients of cobra snakebite. Toxicon 2003, 41, 409–415. [Google Scholar] [CrossRef]
- Wang, W.; Chen, Q.F.; Yin, R.X.; Zhu, J.J.; Li, Q.B.; Chang, H.H.; Wu, Y.B.; Michelson, E. Clinical features and treatment experience: A review of 292 Chinese cobra snakebites. Environ. Toxicol. Pharmacol. 2014, 37, 648–655. [Google Scholar] [CrossRef]
- Saravu, K.; Somavarapu, V.; Shastry, A.B.; Kumar, R. Clinical profile, species-specific severity grading, and outcome determinants of snake envenomation: An Indian tertiary care hospital-based prospective study. Indian J. Crit. Care Med. 2012, 16, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Iddon, D.; Theakston, R.D.G.; Ownby, C.L. A study of the pathogenesis of local skin necrosis induced by Naja nigricollis (spitting cobra) venom using simple histological staining techniques. Toxicon 1987, 25, 665–672. [Google Scholar] [CrossRef]
- Wongtongkam, N.; Wilde, H.; Sitthi-Amorn, C.; Ratanabanangkoon, K. A study of Thai cobra (Naja kaouthia) bites in Thailand. Mil. Med. 2005, 170, 336–341. [Google Scholar] [CrossRef]
- Kumar, V.; Maheshwari, R.; Verma, H.K. Toxicity and symptomatic identification of species involved in snakebites in the Indian subcontinent. J. Venom. Anim. Toxins Incl. Trop. Dis. 2006, 12, 3–18. [Google Scholar] [CrossRef]
- Lin, J.H.; Sung, W.C.; Liao, J.W.; Hung, D.Z. A rapid and international applicable diagnostic device for cobra (Genus Naja) Snakebites. Toxins 2020, 12, 572. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.R.; Otten, E.J. Snakebites and other reptiles. In Goldfrank’s Toxicologic Emergencies, 5th ed.; Goldfrank, L.R., Ed.; Appleton & Lange: Norwalk, CT, USA, 1994; pp. 1297–1312. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Variables | Wound Necrosis Group n = 8; n (%) | No Wound Necrosis Group n = 19; n (%) | p |
|---|---|---|---|
| Patient characteristics | |||
| Age # | 45.5 (33.5–61.5) | 48 (34–59) | 0.99 |
| Male sex | 1 (12.5) | 5 (26.3) | 0.90 |
| Bite information | |||
| Lower extremity | 5 (62.5) | 12 (63.2) | 0.79 |
| Upper extremity | 3 (37.5) | 6 (31.6) | |
| Face | 0 (0.00) | 1 (5.3) | |
| Fang mark | 0.09 | ||
| 0 | 0 (0.00) | 3(15.8) | |
| 1 | 0 (0.00) | 5 (26.3) | |
| 2 | 8 (100) | 11 (57.9) | |
| Clinical Features | |||
| Initial local swelling | 0.006 | ||
| None to mild | 1 (12.5) | 17 (89.5) | |
| Moderate to severe | 7 (87.5) | 2 (10.5) | |
| Initial necrosis | 4 (50) | 0 (0.00) | 0.004 |
| Systemic Symptoms/signs | |||
| No | 0 (0.00) | 11 (57.9) | |
| Neurologic (muscle weakness) | 3 (37.5) | 4 (21.1) | 0.14 |
| Gastrointestinal | 5 (62.5) | 4 (21.1) | 0.37 |
| Antivenom before sampling | 0.01 | ||
| 0 vial | 3 (37.5) | 16 (84.2) | |
| 1 vial | 5 (62.5) | 2 (10.5) | |
| 2 vials | 0 (0.00) | 1 (5.2) | |
| Serum venom level (ng/mL) # | 372 (153.5–611.5) | 21 (0–874) | 0.31 |
| Presentation time (h) # | 14.5 (5–125.5) | 3 (2–6) | 0.02 |
| Product of time × level # | 5734 (937–15,342.5) | 42 (0–2430) | 0.01 |
| Treatment Modalities | |||
| Total antivenom (vial) | 3.5 (1.5–6) | 2 (1–6) | 0.52 |
| Operation needed | 8 (29.6) | 1 (3.7) | <0.0001 |
| Variable | Sensitivity (%) | Specificity (%) | PPV # (%) | NPV # (%) | Accuracy (%) |
|---|---|---|---|---|---|
| Initial local swelling | 87.50 | 89.47 | 77.78 | 94.44 | 88.89 |
| time × serum level (Cut-off point 3500) | 62.50 | 84.21 | 62.50 | 84.21 | 77.78 |
| Initial necrosis | 50.00 | 100 | 100 | 82.61 | 85.19 |
| Presentation time | 62.50 | 78.95 | 55.56 | 83.33 | 74.07 |
| Envenoming Severity | Definition |
|---|---|
| dry bite | no swelling or erythema around the fang marks |
| mild degree | limb swelling, erythema limited to one joint area, or was equal to or less than 10 cm in size |
| moderate degree | swelling and erythema around the fang marks were 10–20 cm and/or small necrotic change (less than 2 cm in diameter) |
| Severe degree | limb swelling greater than 20 cm, extended over two joints, and/or significant local tissue necrosis |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, C.-C.; Chaou, C.-H.; Gao, S.-Y. Influential Factors of Local Tissue Necrosis after Taiwan Cobra Bites: A Secondary Analysis of the Clinical Significance of Venom Detection in Patients of Cobra Snakebites. Toxins 2021, 13, 338. https://doi.org/10.3390/toxins13050338
Lin C-C, Chaou C-H, Gao S-Y. Influential Factors of Local Tissue Necrosis after Taiwan Cobra Bites: A Secondary Analysis of the Clinical Significance of Venom Detection in Patients of Cobra Snakebites. Toxins. 2021; 13(5):338. https://doi.org/10.3390/toxins13050338
Chicago/Turabian StyleLin, Chih-Chuan, Chung-Hsien Chaou, and Shi-Ying Gao. 2021. "Influential Factors of Local Tissue Necrosis after Taiwan Cobra Bites: A Secondary Analysis of the Clinical Significance of Venom Detection in Patients of Cobra Snakebites" Toxins 13, no. 5: 338. https://doi.org/10.3390/toxins13050338
APA StyleLin, C.-C., Chaou, C.-H., & Gao, S.-Y. (2021). Influential Factors of Local Tissue Necrosis after Taiwan Cobra Bites: A Secondary Analysis of the Clinical Significance of Venom Detection in Patients of Cobra Snakebites. Toxins, 13(5), 338. https://doi.org/10.3390/toxins13050338