Developing a Consistent, Reproducible Botulinum Toxin Type A Dosing Method for Upper Limb Tremor by Kinematic Analysis



Abstract
1. Introduction
2. Results
2.1. Dosing Method Development and Validation
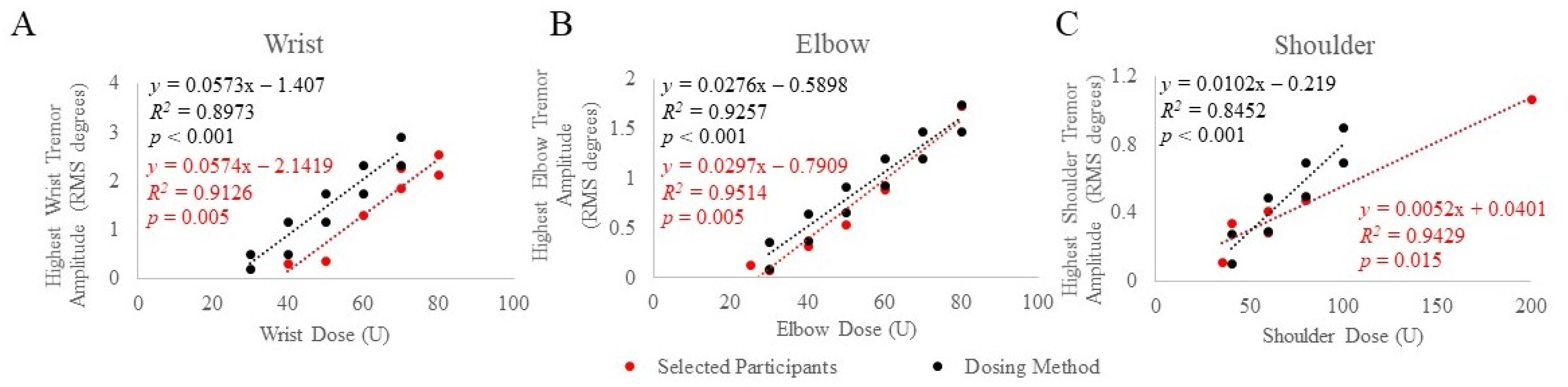
2.2. Associations between Tremor Reduction and Total Joint Dose
3. Discussion
4. Materials and Methods
4.1. Study Participants
4.2. Kinematic Tremor Assessment
4.3. Kinematic Tremor Analysis
4.4. Statistical Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sharma, S.; Pandey, S. Treatment of essential tremor: Current status. Postgrad. Med. J. 2019, 96, 84–93. [Google Scholar] [CrossRef]
- Ferreira, J.J.; Mestre, T.A.; Lyons, K.E.; Benito-León, J.; Tan, E.; Abbruzzese, G.; Hallett, M.; Haubenberger, D.; Elble, R.; Deuschl, G.; et al. MDS evidence-based review of treatments for essential tremor. Mov. Disord. 2019, 34, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Bhatia, K.P.; Bain, P.; Bajaj, N.; Elble, R.J.; Hallett, M.; Louis, E.D.; Raethjen, J.; Stamelou, M.; Testa, C.M.; Deuschl, G.; et al. Consensus Statement on the classification of tremors. from the task force on tremor of the International Parkinson and Movement Disorder Society. Mov. Disord. 2018, 33, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Mittal, S.O.; Lenka, A.; Jankovic, J. Botulinum toxin for the treatment of tremor. Park. Relat. Disord. 2019, 63, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Zakin, E.; Simpson, D. Botulinum Toxin in Management of Limb Tremor. Toxins 2017, 9, 365. [Google Scholar] [CrossRef]
- Niemann, N.; Jankovic, J. Botulinum Toxin for the Treatment of Hand Tremor. Toxins 2018, 10, 299. [Google Scholar] [CrossRef]
- Brin, M.; Lyons, K.; Doucette, J.; Adler, C.; Caviness, J.; Comella, C.; Dubinsky, R.; Friedman, J.; Manyam, B.; Matsumoto, J.; et al. A randomized, double masked, controlled trial of botulinum toxin type A in essential hand tremor. Neurology 2001, 56, 1523–1528. [Google Scholar] [CrossRef]
- Jankovic, J.; Schwartz, K.; Clemence, W.; Aswad, A.; Mordaunt, J. A randomized, double-blind, placebo-controlled study to evaluate botulinum toxin type A in essential hand tremor. Mov. Disord. 1996, 11, 250–256. [Google Scholar] [CrossRef]
- Pullman, S.L.; Greene, P.; Fahn, S.; Pedersen, S.F. Approach to the Treatment of Limb Disorders with Botulinum Toxin A. Experience with 187 patients. Arch. Neurol. 1996, 53, 617–624. [Google Scholar] [CrossRef]
- Mittal, S.O.; Machado, D.; Richardson, D.; Dubey, D.; Jabbari, B. Botulinum toxin in essential hand tremor—A randomized double-blind placebo-controlled study with customized injection approach. Park. Relat. Disord. 2018, 56, 65–69. [Google Scholar] [CrossRef]
- Mittal, S.O.; Machado, D.; Richardson, D.; Dubey, D.; Jabbari, B. Botulinum Toxin in Parkinson Disease Tremor: A Random-ized, Double-Blind, Placebo-Controlled Study with a Customized Injection Approach. Mayo Clin. Proc. 2017, 92, 1359–1367. [Google Scholar] [CrossRef]
- Samotus, O.; Lee, J.; Jog, M. Long-term tremor therapy for Parkinson and essential tremor with sensor-guided botulinum toxin type A injections. PLoS ONE 2017, 12, e0178670. [Google Scholar] [CrossRef] [PubMed]
- Samotus, O.; Lee, J.; Jog, M. Personalized Bilateral Upper Limb Essential Tremor Therapy with Botulinum Toxin Using Kinematics. Toxins 2019, 11, 125. [Google Scholar] [CrossRef]
- Samotus, O.; Lee, J.; Jog, M. Standardized algorithm for muscle selection and dosing of botulinum toxin for Parkinson tremor using kinematic analysis. Ther. Adv. Neurol. Disord. 2020, 13, 1756286420954083. [Google Scholar] [CrossRef] [PubMed]
- Jog, M.; Lee, J.; Scheschonka, A.; Chen, R.; Ismail, F.; Boulias, C.; Hobson, D.; King, D.; Althaus, M.; Simon, O.; et al. Tolerability and Efficacy of Customized IncobotulinumtoxinA Injections for Essential Tremor: A Randomized, Double-blind, Placebo-Controlled Study. Toxins 2020, 12, 807. [Google Scholar] [CrossRef]
- Rajan, R.; Srivastava, A.K.; Anandapadmanabhan, R.; Saini, A.; Upadhyay, A.; Gupta, A.; Vishnu, V.Y.; Pandit, A.K.; Vibha, D.; Singh, M.B.; et al. Assessment of Botulinum Neurotoxin Injection for Dystonic Hand Tremor: A Randomized Clinical Trial. JAMA Neurol. 2021, 78, 302–311. [Google Scholar] [CrossRef]
- Pacchetti, C.; Mancini, F.; Bulgheroni, M.; Zangaglia, R.; Cristina, S.; Sandrini, G.; Nappi, G. Botulinum toxin treatment for func-tional disability induced by essential tremor. Neurol. Sci. 2000, 21, 349–353. [Google Scholar] [CrossRef] [PubMed]
- Elble, R.J.; McNames, J. Using Portable Transducers to Measure Tremor Severity. Tremor Other Hyperkinetic Movements 2016, 6, 375. [Google Scholar] [CrossRef] [PubMed]
- Kamel, J.T.; Cordivari, C.; Catania, S. Treatment of Upper Limb Tremor with Botulinum Toxin: An Individualized Approach. Mov. Disord. Clin. Pract. 2019, 6, 652–655. [Google Scholar] [CrossRef]
- Mittal, S.O.; Jog, M.; Lee, J.; Jabbari, B. Novel Botulinum Toxin Injection Protocols for Parkinson Tremor and Essential Tremor the Yale Technique and Sensor-Based Kinematics Procedure for Safe and Effective Treatment. Tremor Other Hyperkinetic Mov. 2020, 10, 61. [Google Scholar] [CrossRef] [PubMed]
- Samotus, O.; Lee, J.; Jog, M. Personalized botulinum toxin type A therapy for cervical dystonia based on kinematic guidance. J. Neurol. 2018, 265, 1269–1278. [Google Scholar] [CrossRef] [PubMed]
- Sanes, J.N.; Hallett, M. Limb positioning and magnitude of essential tremor and other pathological tremors. Mov. Disord. 1990, 5, 304–309. [Google Scholar] [CrossRef] [PubMed]
- Dirkx, M.F.; Zach, H.; Bloem, B.R.; Hallett, M.; Helmich, R.C. The nature of postural tremor in Parkinson disease. Neurology 2018, 90, e1095–e1103. [Google Scholar] [CrossRef] [PubMed]
- Jinnah, H.A.; Goodmann, E.; Rosen, A.R.; Evatt, M.; Freeman, A.; Factor, S. Botulinum toxin treatment failures in cervical dystonia: Causes, management, and outcomes. J. Neurol. 2016, 263, 1188–1194. [Google Scholar] [CrossRef] [PubMed]
- Contarino, M.F.; Smit, M.; Van den Dool, J.; Volkmann, J.; Tijssen, M.A.J. Unmet needs in the management of cervical dystonia. Front. Neurol. 2016, 7, 1–7. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Participant ID | Condition | Arm Joint | Task to Produce Highest Tremor Amplitude | BoNT-A Joint Dose * (U) | Baseline Tremor Amplitude (RMS Degrees) | Change in Tremor Amplitude ** (RMS Degrees) |
|---|---|---|---|---|---|---|
| 1 | PD | Wrist | Rest-1 | 70 | 1.87 | −0.30 |
| 2 | ET | Wrist | Load-2 | 50 | 0.36 | −0.29 |
| Elbow | Load-2 | 25 | 0.13 | −0.01 | ||
| 3 | PD | Elbow | Load-2 | 30 | 0.09 | −0.01 |
| 4 | ET | Wrist | Load-1 | 60 | 1.32 | −1.27 |
| 5 | ET | Wrist | Posture-2 | 70 | 2.27 | −2.16 |
| Shoulder | Load-2 | 40 | 0.34 | −0.32 | ||
| 6 | PD | Wrist | Posture-1 | 40 | 0.32 | −0.29 |
| 7 | PD | Wrist | Rest-2 | 80 | 2.56 | −1.59 |
| 8 | ET | Shoulder | Load-2 | 200 | 1.07 | −0.48 |
| 9 | PD | Wrist | Load-2 | 80 | 2.13 | −2.08 |
| 10 | PD | Elbow | Load-2 | 40 | 0.32 | −0.22 |
| 11 | PD | Elbow | Load-2 | 60 | 0.90 | −0.57 |
| Shoulder | Load-2 | 80 | 0.48 | −0.27 | ||
| 12 | PD | Elbow | Load-2 | 50 | 0.54 | −0.40 |
| 13 | ET | Shoulder | Load-2 | 35 | 0.11 | −0.01 |
| 14 | ET | Shoulder | Load-2 | 60 | 0.28 | −0.17 |
| 15 | ET | Elbow | Load-2 | 80 | 1.73 | −1.45 |
| Shoulder | Load-2 | 60 | 0.42 | −0.32 | ||
| Wrist | ET: 3; PD: 4 | n = 7 | Mean ± SD | 64 ± 15 | 1.54 ± 0.91 | −1.14 ± 0.84 |
| Elbow | ET: 2; PD: 4 | n = 6 | 47 ± 20 | 0.62 ± 0.62 | −0.44 ± 0.54 | |
| Shoulder | ET: 5; PD: 1 | n = 6 | 79 ± 61 | 0.45 ±0.37 | −0.26 ± 0.16 |
| Arm Joint | Dosing Equation | Degree(s) of Freedom | Muscle |
|---|---|---|---|
| Wrist | F + R | Flexor Carpi Radialis (FCR) | |
| F + U | Flexor Carpi Ulnaris (FCU) | ||
| E + R | Extensor Carpi Radialis (ECR) | ||
| E + U | Extensor Capri Ulnaris (ECU) | ||
| P | Pronator Teres (PT) | ||
| P | Pronator Quadratus (PQ) | ||
| S | Supinator | ||
| Elbow | F | Biceps | |
| E | Triceps | ||
| Shoulder | F + Add | Pectoris Major | |
| E | Teres Major | ||
| Abd | Deltoid | ||
| Abd | Supraspinatus |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samotus, O.; Lee, J.; Jog, M. Developing a Consistent, Reproducible Botulinum Toxin Type A Dosing Method for Upper Limb Tremor by Kinematic Analysis. Toxins 2021, 13, 264. https://doi.org/10.3390/toxins13040264
Samotus O, Lee J, Jog M. Developing a Consistent, Reproducible Botulinum Toxin Type A Dosing Method for Upper Limb Tremor by Kinematic Analysis. Toxins. 2021; 13(4):264. https://doi.org/10.3390/toxins13040264
Chicago/Turabian StyleSamotus, Olivia, Jack Lee, and Mandar Jog. 2021. "Developing a Consistent, Reproducible Botulinum Toxin Type A Dosing Method for Upper Limb Tremor by Kinematic Analysis" Toxins 13, no. 4: 264. https://doi.org/10.3390/toxins13040264
APA StyleSamotus, O., Lee, J., & Jog, M. (2021). Developing a Consistent, Reproducible Botulinum Toxin Type A Dosing Method for Upper Limb Tremor by Kinematic Analysis. Toxins, 13(4), 264. https://doi.org/10.3390/toxins13040264