Snakebite Envenoming a Challenging Diagnosis for the Forensic Pathologist: A Systematic Review

 ,
,  ,
,  ,
, 
Abstract
1. Introduction
2. Results
2.1. Characteristics of Eligible Studies
2.2. Epidemiological Findings
2.3. Post Mortem Examination Findings
3. Discussion
4. Conclusions
5. Materials and Methods
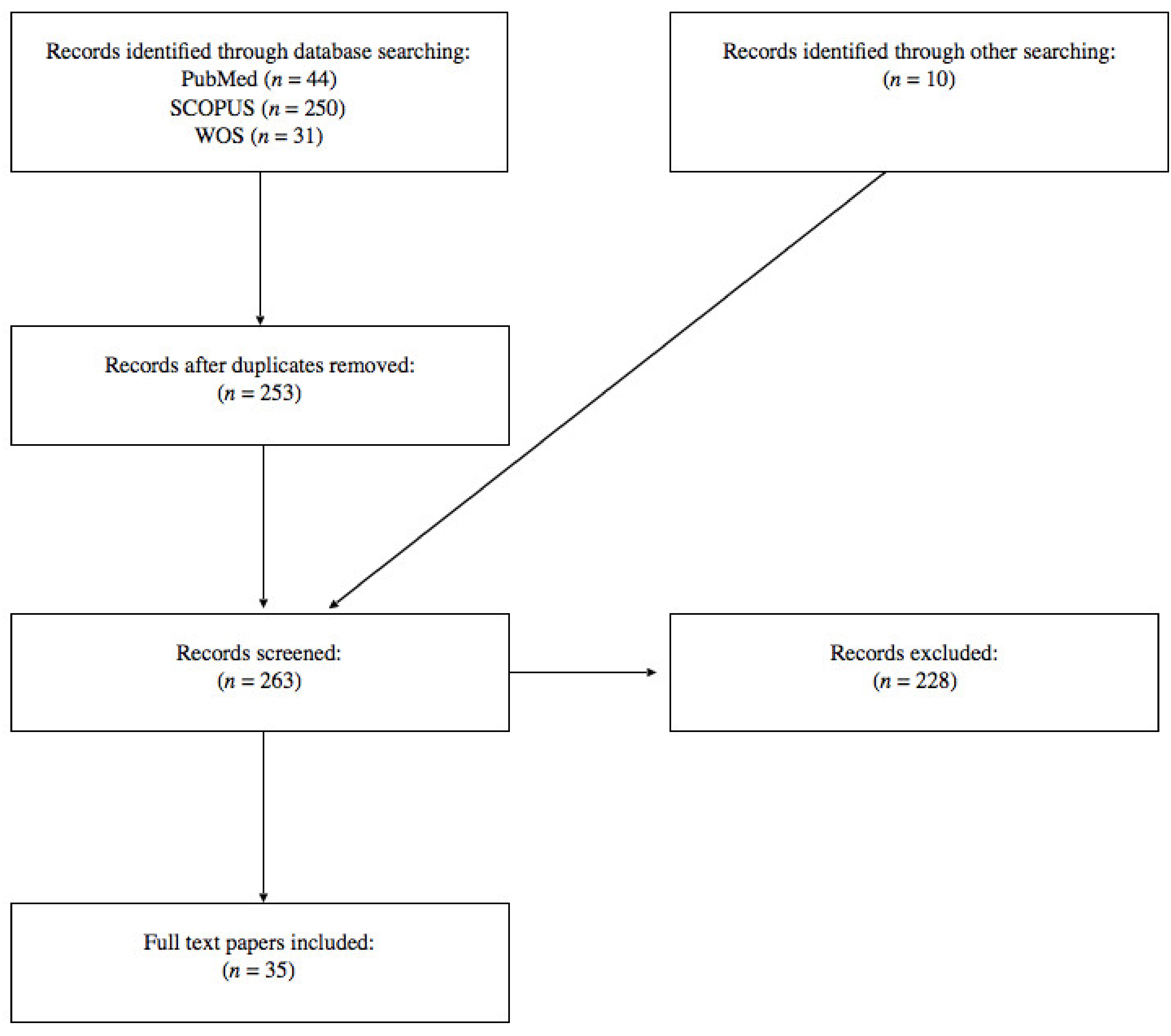
5.1. Literature Search
5.2. Inclusion and Exclusion Criteria
5.3. Data Extraction
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Williams, D.J.; Faiz, M.A.; Abela-Ridder, B.; Ainsworth, S.; Bulfone, T.C.; Nickerson, A.D.; Habib, A.G.; Junghanss, T.; Fan, H.W.; Turner, M.; et al. Strategy for a globally coordinated response to a priority neglected tropical disease: Snakebite envenoming. PLoS Negl. Trop. Dis. 2019, 13, e0007059. [Google Scholar] [CrossRef] [PubMed]
- WHO. Snakebite Envenoming. 2019. Available online: https://www.who.int/news-room/fact-sheets/detail/snakebite-envenoming (accessed on 30 September 2020).
- Sarkar, N.; Basu, S.; Chandra, P.; Chowdhuri, S.; Mukhopadhyay, P. Nephrotoxicity in krait bite: A rare case series of three fatalities in consecutive bites by a single snake. Egypt. J. Forensic Sci. 2018, 8, 12. [Google Scholar] [CrossRef]
- Gutiérrez, J.M. Global Availability of Antivenoms: The Relevance of Public Manufacturing Laboratories. Toxins 2018, 11, 5. [Google Scholar] [CrossRef] [PubMed]
- Laraba-Jebari, F.; Cherifi, F. Pathophysiological and Pharmacological Effects of Snake Venom Components: Molecular Targets. J. Clin. Toxicol. 2014, 4, 2. [Google Scholar] [CrossRef]
- Liu, C.-C.; Yu, J.-S.; Wang, P.-J.; Hsiao, Y.-C.; Chen, Y.-C.; Lai, P.-F.; Hsu, C.-P.; Fann, W.-C.; Lin, C.-C. Development of sandwich ELISA and lateral flow strip assays for diagnosing clinically significant snakebite in Taiwan. PLoS Negl. Trop. Dis. 2018, 12, e0007014. [Google Scholar] [CrossRef]
- WHO. Venomous Snakes Distribution and Species Risk Categories. 2010. Available online: https://apps.who.int/bloodproducts/snakeantivenoms/database/ (accessed on 30 September 2020).
- WHO. Guidelines for the Production, Control and Regulation of Snake Antivenom Immunoglobulins. 2018. Available online: https://www.who.int/bloodproducts/snake_antivenoms/snakeantivenomguide/en/ (accessed on 28 September 2020).
- Warrel, D.A. Guidelines for the Management of Snake Bite; World Health Organization: New Delhi, India, 2010. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzla, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematicreviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, 264–269. [Google Scholar] [CrossRef]
- Barraviera, B.; Júnior, J.C.B.; Arakaki, D.; Domingues, M.A.C.; Pereira, P.C.M.; Mendes, R.P.; Machado, J.M.; Meira, D.A.; Arkaki, D. A retrospective study of 40 victims of Crotalus snake bites: Analysis of the hepatic necrosis observed in one patient. Rev. Soc. Bras. Med. Trop. 1989, 22, 5–12. [Google Scholar] [CrossRef]
- Benvenuti, L.A.; França, F.O.S.; Barbaro, K.C.; Nunes, J.R.; Cardoso, J.L.C. Pulmonary haemorrhage causing rapid death after Bothrops jararacussu snakebite: A case report. Toxicon 2003, 42, 331–334. [Google Scholar] [CrossRef]
- Blaylock, R.S.M.; Tilbury, C.R.; Branch, W.R. Anaphylaxis following exposure to snake venoms in South Africa. Curr. Allergy Clin. Immunol. 2002, 15, 65–68. [Google Scholar]
- Blumenthal, R.; Scholtz, P.E.P.; Shuttleworth, J.-L. Black Mamba Death: Venom versus Antivenom? Am. J. Forensic Med. Pathol. 2019, 40, 356–360. [Google Scholar] [CrossRef]
- Chen, L.; Huang, G.-Z. Poisoning by toxic animals in China—18 autopsy case studies and a comprehensive literature review. Forensic Sci. Int. 2013, 232, e12–e23. [Google Scholar] [CrossRef]
- Curry, S.C.; Kunkel, D.B. Toxicology rounds. Death from a rattlesnake bite. Am. J. Emerg. Med. 1985, 3, 227–235. [Google Scholar] [CrossRef]
- Karlawad, M.; Nadaf, A.A.; Nayak, G.H. Snake bite at an unusual site—A case report. JKAMLS 2017, 26, 28–31. [Google Scholar]
- Keith, J.; White, J.; Pascu, O.; Fabian, V. Fatal Cerebellar Hemorrhage Following Australian Brown Snake Envenomation. Can. J. Neurol. Sci. J. Can. des Sci. Neurol. 2012, 39, 120–121. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kitchens, C.S.; Hunter, S.; Van Mierop, L.H. Severe myonecrosis in a fatal case of envenomation by the canebrake rattlesnake (Crotalus horridus atricaudatus). Toxicon 1987, 25, 455–458. [Google Scholar] [CrossRef]
- Malbranque, S.; Barbey, C.; Smadja, D.; Courcier, D.; Warrell, D.A.; Piercecchi-Marti, M.D.; Thomas, L.; Bucher, B.; Ridarch, A. Fatal Diffuse Thrombotic Microangiopathy after a Bite by the “Fer-de-Lance” Pit Viper (Bothrops lanceolatus) of Martinique. Am. J. Trop. Med. Hyg. 2008, 78, 856–861. [Google Scholar] [CrossRef]
- Malhotra, P.; Sharma, N.; Awasthi, A.; Vasishta, R.K. Fatal acute disseminated encephalomyelitis following treated snake bite in India. Emerg. Med. J. 2005, 22, 308–309. [Google Scholar] [CrossRef]
- Marsh, N.; DeRoos, F.; Touger, M. Gaboon viper (Bitis gabonica) envenomation resulting from captive specimens--a review of five cases. Clin. Toxicol. 2007, 45, 60–64. [Google Scholar] [CrossRef] [PubMed]
- McGarity, B.H.; Marshall, G.P.; A Loadsman, J.; Carr, S.J.; Harper, C.G. Fatal cerebral haemorrhage after tiger snake bite. Med. J. Aust. 1991, 155, 61–62. [Google Scholar] [CrossRef]
- Junior, R.M. Snake bites by the jararacucu (Bothrops jararacussu): Clinicopathological studies of 29 proven cases in Sao Paulo State, Brazil. QJM Int. J. Med. 1997, 90, 323–334. [Google Scholar] [CrossRef]
- Moar, J.J.; Hill, L.; Stewart, M. Histopatholological Findings in a Fatal Case of Rinkhals Envenomation: A New Forensic Pathology Finding? Am. J. Forensic Med. Pathol. 2016, 37, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Rathnayaka, R.N.; Ranathunga, P.N.; Ranaweera, J.; Jayasekara, K.; Kularatne, S. Cardiac arrest and atrial fibrillation in a patient after hump-nosed pit viper (Hypnale hypnale) bite. Toxicon 2018, 148, 33–39. [Google Scholar] [CrossRef]
- Rathnayaka, R.N.; Ranathunga, P.; Kularatne, S. Systemic bleeding including pulmonary haemorrhage following hump-nosed pit viper (Hypnale hypnale) envenoming: A case report from Sri Lanka. Toxicon 2019, 170, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Rathnayaka, R.N.; Kularatne, S.; Kumarasinghe, K.; Ranaweera, J.; Ranathunga, P.N. Ischemic brain infarcts and intracranial haemorrhages following Russell’s viper (Daboia russelii) bite in Sri Lanka. Toxicon 2017, 125, 70–73. [Google Scholar] [CrossRef]
- Norris, R.L.; Pfalzgraf, R.R.; Laing, G. Death following coral snake bite in the United States--first documented case (with ELISA confirmation of envenomation) in over 40 years. Toxicon 2009, 53, 693–697. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, O.; Nakashima, R.; Yamamoto, S.; Hashimoto, T.; Takasaki, T.; Tokuda, H.; Sato, S.; Gamachi, A.; Hashimoto, H.; Inagaki, N. A lethal case of mamushi (Gloydius blomhoffii) bite: Severe bowel symptoms as a lethal sign. Acute Med. Surgery 2016, 4, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Paulis, M.G.; Faheem, A.L. Homicidal Snake Bite in Children. J. Forensic Sci. 2015, 61, 559–561. [Google Scholar] [CrossRef]
- Kumar, G.P.; Arun, M.; Chandrakanth, H.; Balaraj, B. Uncommon combination of malignancy: Incidental diagnosis at forensic autopsy. Aust. J. Forensic Sci. 2013, 45, 49–53. [Google Scholar] [CrossRef]
- Quain, R. Bite from the Hooded Snake, (Cobra de Capello) Rapid Death; Autopsy. Lancet 1852, 60, 397–400. [Google Scholar] [CrossRef]
- Rathnayaka, R.N.; Ranathunga, P. Late onset of bilateral cerebral infarction following Russell’s viper (Daboia russelii) bite. Sri Lankan J. Anaesthesiol. 2017, 25, 35. [Google Scholar] [CrossRef]
- Silva, A.; Gamlaksha, D.; Waidyaratne, D. Medico-legal significance of the identification of offending snake in a fatal snake bite: A case report. J. Forensic Leg. Med. 2013, 20, 965–967. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, S.S.; Freitas-De-Sousa, L.A.; Alves, E.C.; Ferreira, L.C.D.L.; Da Silva, I.M.; De Lacerda, M.V.G.; Fan, H.W.; Moura-Da-Silva, A.M.; Monteiro, W.M. Fatal stroke after Bothrops snakebite in the Amazonas state, Brazil: A case report. Toxicon 2017, 138, 102–106. [Google Scholar] [CrossRef]
- Soe, S.; Win, M.M.; Htwe, T.T.; Lwin, M.; Thet, S.S.; Kyaw, W.W. Renal histopathology following Russell’s viper (Vipera russelli) bite. Southeast Asian J. Trop. Med. Public Health 1993, 24, 193–197. [Google Scholar]
- Sutherland, S.K. Deaths from snake bite in Australia, 1981–1991. Med. J. Aust. 1992, 157, 740–746. [Google Scholar] [CrossRef] [PubMed]
- Than, T.; Francis, N.; Swe, T.-N.; Lwin, M.; Pe, T.; Soe, S.; Oo, M.-M.; Phillips, R.E.; Warrell, D.A. Contribution of focal haemorrhage and microvascular fibrin deposition to fatal envenoming by Russell’s viper (Vipera russelli siamensis) in Burma. Acta Trop. 1989, 46, 23–38. [Google Scholar] [CrossRef]
- Tibballs, J.; Henning, R.D.; Sutherland, S.K.; Kerr, A.R. Fatal cerebral haemorrhage after tiger snake (Notechis scutatus) envenomation. Med. J. Aust. 1991, 154, 275–276. [Google Scholar] [CrossRef]
- Tilbury, C.R.; Verster, J. A fatal bite from the burrowing asp Atractaspis corpulenta (Hallowell 1854). Toxicon 2016, 118, 21–26. [Google Scholar] [CrossRef]
- Trancă, S.; Cocis, M.; Antal, O. Lethal case of Vipera bersus bite. Clujul Med. 2016, 89, 435–437. [Google Scholar] [CrossRef]
- Varagunam, T.; Panabokke, R.G. Bilateral cortical necrosis of the kidneys following snakebite. Postgrad. Med. J. 1970, 46, 449–451. [Google Scholar] [CrossRef][Green Version]
- Wankhede, A.G. An unusual Russell’s viper bite mark: A case report. Med. Sci. Law 2004, 44, 87–89. [Google Scholar] [CrossRef]
- Warrell, D.; Barnes, H.; Piburn, M. Neurotoxic effects of bites by the Egyptian cobra (Naja haje) in Nigeria. Trans. R. Soc. Trop. Med. Hyg. 1976, 70, 78–79. [Google Scholar] [CrossRef]
- O’Malley, B. Clinical Anatomy and Physiology of Exotic Species; Elsevier Saunders: Philadelphia, PA, USA, 2005. [Google Scholar]
- Giugliano, P.; Feola, A.; La Sala, F.; Buonomo, C.; Della Pietra, B. A Case of suicide by a Large Number of sharp Force Injuries. Medico-Legal Updat. 2017, 18, 10. [Google Scholar] [CrossRef]
- Gold, B.S.; Dart, R.C.; Barish, R.A. Bites of Venomous Snakes. N. Engl. J. Med. 2002, 347, 347–356. [Google Scholar] [CrossRef]
- Luiselli, L.; Sale, L.; Akani, G.C.; Amori, G. Venomous Snake Abundance Within Snake Species’ Assemblages Worldwide. Diversity 2020, 12, 69. [Google Scholar] [CrossRef]
- Gutiérrez, J.M.; Theakston, R.D.G.; Warrell, D.A. Confronting the Neglected Problem of Snake Bite Envenoming: The Need for a Global Partnership. PLoS Med. 2006, 3, e150. [Google Scholar] [CrossRef]
- Slagboom, J.; Kool, J.; Harrison, R.A.; Casewell, N.R. Haemotoxic snake venoms: Their functional activity, impact on snakebite victims and pharmaceutical promise. Br. J. Haematol. 2017, 177, 947–959. [Google Scholar] [CrossRef]
- Zahradnicek, O.; Horáček, I.; Tucker, A.S. Viperous fangs: Development and evolution of the venom canal. Mech. Dev. 2008, 125, 786–796. [Google Scholar] [CrossRef]
- Adukauskienė, D.; Varanauskienė, E.; Adukauskaitė, A. Venomous Snakebites. Medicina 2011, 47, 461. [Google Scholar] [CrossRef]
- Hayes, W.K.; Corbit, A.G.; Cardwell, M.D.; Herbert, S.S. Interfang Distances of Rattlesnakes: Sexual, Interspecific, and Body Size-related Variation, and Implications for Snakebite Research and Management. Wilderness Environ. Med. 2017, 28, 101–107. [Google Scholar] [CrossRef]
- Thein, C.M.; Byard, R.W. Characteristics and relative numbers of lethal snake bite cases in medicolegal practice in central Myanmar—A five year study. J. Forensic Leg. Med. 2019, 63, 52–55. [Google Scholar] [CrossRef]
- Tasoulis, T.; Isbister, G.K. A Review and Database of Snake Venom Proteomes. Toxins 2017, 9, 290. [Google Scholar] [CrossRef]
- Pereañez, J.A.; Preciado, L.M.; Fernández, J.; Camacho, E.; Lomonte, B.; Castro, F.; Cañas, C.A.; Galvis, C.; Castaño, S. Snake venomics, experimental toxic activities and clinical characteristics of human envenomation by Bothrocophias myersi (Serpentes: Viperidae) from Colombia. J. Proteom. 2020, 220, 103758. [Google Scholar] [CrossRef]
- Sutherland, S.K. Rapid venom identification: Availability of kits. Med. J. Aust. 1979, 2, 602–603. [Google Scholar] [CrossRef] [PubMed]
- Theakston, R.; Laing, G.D. Diagnosis of Snakebite and the Importance of Immunological Tests in Venom Research. Toxins 2014, 6, 1667–1695. [Google Scholar] [CrossRef]
- Ho, M.; Warrell, M.; Warrell, D.; Bidwell, D.; Voller, A. A critical reappraisal of the use of enzyme-linked immunosorbent assays in the study of snake bite. Toxicon 1986, 24, 211–221. [Google Scholar] [CrossRef]
- Van Dong, L. Immunogenicity of venoms from four common snakes in the South of Vietnam and development of ELISA kit for venom detection. J. Immunol. Methods 2003, 282, 13–31. [Google Scholar] [CrossRef]
- Kulawickrama, S.; O’Leary, M.A.; Hodgson, W.C.; Brown, S.G.A.; Jacoby, T.; Davern, K.; Isbister, G.K. Development of a sensitive enzyme immunoassay for measuring taipan venom in serum. Toxicon 2010, 55, 1510–1518. [Google Scholar] [CrossRef]
- Brunda, G.; Sashidhar, R.; Sarin, R. Use of egg yolk antibody (IgY) as an immunoanalytical tool in the detection of Indian cobra (Naja naja naja) venom in biological samples of forensic origin. Toxicon 2006, 48, 183–194. [Google Scholar] [CrossRef]
- Chen, T.; Bjourson, A.J.; Orr, D.F.; Kwok, H.; Rao, P.; Ivanyi, C.; Shaw, C. Unmasking venom gland transcriptomes in reptile venoms. Anal. Biochem. 2002, 311, 152–156. [Google Scholar] [CrossRef]
- Jia, Y.; Olvera, P.; Rangel, F.; Mendez, B.; Reddy, S. Rapid Identification of Phospholipase A2 Transcripts from Snake Venoms. Toxins 2019, 11, 69. [Google Scholar] [CrossRef]
- Sharma, S.; Kuch, U.; Höde, P.; Bruhse, L.; Pandey, D.P.; Ghimire, A.; Chappuis, F.; Alirol, E. Use of Molecular Diagnostic Tools for the Identification of Species Responsible for Snakebite in Nepal: A Pilot Study. PLoS Negl. Trop. Dis. 2016, 10, e0004620. [Google Scholar] [CrossRef]
- Ranawaka, U.K.; Lalloo, D.G.; De Silva, H.J. Neurotoxicity in Snakebite—The Limits of Our Knowledge. PLoS Negl. Trop. Dis. 2013, 7, e2302. [Google Scholar] [CrossRef]
- Chacko, A.; Andronikou, S.; Ramanjam, V. Hypoxic brain injury and cortical blindness in a victim of a Mozambican spitting cobra bite. S. Afr. J. Surg. 2015, 53, 67. [Google Scholar] [CrossRef]
- Teixeira, C.; Fernandes, C.M.; Leiguez, E.; Chudzinski-Tavassi, A.M. Inflammation Induced by Platelet-Activating Viperid Snake Venoms: Perspectives on Thromboinflammation. Front. Immunol. 2019, 10, 2082. [Google Scholar] [CrossRef]
- Gopalakrishnakone, P. Clinical Toxinology in Asia Pacific and Africa; Springer: Dordrecht, The Netherlands, 2015. [Google Scholar]
- Liu, C.-C.; Chou, Y.-S.; Chen, C.-Y.; Liu, K.-L.; Huang, G.-J.; Yu, J.-S.; Wu, C.-J.; Liaw, G.-W.; Hsieh, C.-H.; Chen, C.-K. Pathogenesis of local necrosis induced by Naja atra venom: Assessment of the neutralization ability of Taiwanese freeze-dried neurotoxic antivenom in animal models. PLoS Negl. Trop. Dis. 2020, 14, e0008054. [Google Scholar] [CrossRef]
- Hogan, D.E.; Dire, D.J. Anaphylactic shock secondary to rattlesnake bite. Ann. Emerg. Med. 1990, 19, 814–816. [Google Scholar] [CrossRef]
- Marko, I. Çeko; Marko, S.; Alimehmeti, I.; Sulaj, Z. Anaphylactic Reactions due to Snakebite Vipera and Administration of Antivenom. Toxicol. Forensic Med. Open J. 2016, 1, 65–66. [Google Scholar] [CrossRef]
- Rencher, L.; Schwartz, J.; Wilson, A. An Anaphylactoid Reaction to Rattlesnake Envenomation in a Pediatric Patient. Pediatr. Emerg. Care 2018, 34, e109–e110. [Google Scholar] [CrossRef] [PubMed]
- Campobasso, C.P.; Procacci, R.; Caligara, M. Fatal Adverse Reaction to Ketorolac Tromethamine in Asthmatic Patient. Am. J. Forensic Med. Pathol. 2008, 29, 358–363. [Google Scholar] [CrossRef]
- Chaudhary, S.C.; Sawlani, K.K.; Malhotra, H.S.; Singh, J. Snake bite-induced leucoencephalopathy. BMJ Case Rep. 2013, 2013, 2012007515. [Google Scholar] [CrossRef]
- Kariyanna, P.T.; Jayarangaiah, A.; Kamran, H.; Schechter, J.; Soroka, S.; Amarnani, A.; Ray, J.; Yacoub, M.; Post, M.; Al-Bayati, S.; et al. Myocardial Infarction after Snakebite Envenomation: A Scoping Study. Scifed. J. Cardiol 2018, 2, 21. [Google Scholar]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D. The Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef] [PubMed]
- Nonaka, P.N.; Amorim, C.F.; Peres, A.C.P.; E Silva, C.A.M.; Zamuner, S.R.; Ribeiro, W.; Cogo, J.C.; Vieira, R.D.P.; Dolhnikoff, M.; De Oliveira, L.V.F. Pulmonary mechanic and lung histology injury induced by Crotalus durissus terrificus snake venom. Toxicon 2008, 51, 1158–1166. [Google Scholar] [CrossRef]
- Azevedo, E.; Figueiredo, R.G.; Pinto, R.V.; Ramos, T.D.C.F.; Sampaio, G.P.; Santos, R.P.B.; Guerreiro, M.L.D.S.; Biondi, I.; Trindade, S.C. Evaluation of systemic inflammatory response and lung injury induced by Crotalus durissus cascavella venom. PLoS ONE 2020, 15, e0224584. [Google Scholar] [CrossRef]
- Gopalakrishnan, N. Snake Envenoming—An Underreported Cause of Acute Kidney Injury. Kidney Int. Rep. 2019, 4, 643–646. [Google Scholar] [CrossRef]
- Ramachandran, S.; Perera, M.V.F. Survival in renal cortical necrosis due to snake bite. Postgrad. Med. J. 1974, 50, 314–316. [Google Scholar] [CrossRef]
- Vikrant, S.; Jaryal, A.; Parashar, A. Clinicopathological spectrum of snake bite-induced acute kidney injury from India. World J. Nephrol. 2017, 6, 150–161. [Google Scholar] [CrossRef]
- Rosenthal, R.; Meier, J.; Koelz, A.; Muller, C.; Wegmann, W.; Vogelbach, P. Intestinal ischemia after bushmaster (Lachesis muta) snakebite—A case report. Toxicon 2002, 40, 217–220. [Google Scholar] [CrossRef]
- Nault, J.-C.; Megarbane, B.; Theodore, J.; Deye, N.; Nemeth, J.; Valleur, P.; Baud, F.J. Poisoning-related bowel infarction: Characteristics and outcomes. Clin. Toxicol. 2009, 47, 412–418. [Google Scholar] [CrossRef]
- Garkowski, A.; Czupryna, P.; Zajkowska, A.; Pancewicz, S.; Moniuszko, A.; Kondrusik, M.; Grygorczuk, S.; Gołębicki, P.; Letmanowski, M.; Zajkowska, J. Vipera berus bites in Eastern Poland—A retrospective analysis of 15 case studies. Ann. Agric. Environ. Med. 2012, 19, 793–797. [Google Scholar]
- Malina, T.; Krecsák, L.; Korsós, Z.; Takacs, Z. Snakebites in Hungary—Epidemiological and clinical aspects over the past 36 years. Toxicon 2008, 51, 943–951. [Google Scholar] [CrossRef]
- Valenta, J.; Stach, Z.; Stritesky, M.; Michalek, P. Common Viper Bites in the Czech Republic—Epidemiological and Clinical Aspects during 15 Year Period (1999–2013). Prague Med. Rep. 2014, 115, 120–127. [Google Scholar] [CrossRef]


{kind=link}
| References | Country | Victim Age/Sex | Work-Related | Hospital Admission / Antivenom | Time Interval Bite-Death | Snake Family | Bite Area Site Macroscopical Findings | Bite Area Histological Findings | Autopsy Macroscopical Findings | Autopsy Histological Pattern |
|---|---|---|---|---|---|---|---|---|---|---|
| Barraviera B et al., 1989 [11] | Brazil | 60/M | n.a. | Yes/Yes | 4–5 d | Rattlesnake Viperidae | Right leg. Ulceration covered with a blood-stained scab. | Local edema and inflammatory signs. Focal myonecrosis. | n.a. | K: acute tubular necrosis |
| Barraviera B et al.,1989 [11] | Brazil | 59/M | n.a. | Yes/Yes | 5 d | Rattlesnake Viperidae | Right leg. Two punctiform erythematous lesions. | No signs of inflammation. | n.a. | Li: parenchymal necrosis. |
| Benvenuti LA et al., 2003 [12] | Brazil | 36/F | n.a. | Yes; No | 45 min | Bothrops jararacussu Viperidae | Left ankle. Two puncture wounds 25 mm apart. Ecchymosis on the left leg along the great saphenous vein. | Local hemorrhage, thrombosis, and coagulative necrosis of the subcutaneous and muscular tissue. | L: hemorrhage. | PG: normal. H: fibrosis and interstitial hemorrhage. L: extensive alveolar hemorrhage and edema with numerous platelet thrombi in capillaries and venules. DIC. |
| Blaylock RSM et al., 2002 [13] | South Africa | 40/M | Yes | Yes; Yes | 1 h 15 min | Puff Adder (Bitis Arientas) Viperidae | Left wrist. Single puncture wound. | Extensive hemorrhage between muscle bundles and connective tissue. | H: myocardium soft and flabby with hemorrhagic RA. L: edema and congestion. Li; K: pale aspect. | n.a. |
| Blumenthal R et al., 2019 [14] | South Africa | 27/M | Yes | Yes; Yes | 3 d | Black Mamba (Dendroaspis polylepis) Elapidae | Right hand. Single puncture mark. | Subcutaneous hemorrhage. Minimal skin necrosis and hemorrhage at the puncture site. | Diffuse fresh hemorrhages around the vocal cords, the epiglottis, and in the LV. H: petechiae overlying the anterior and posterior epicardial. | B: hypoxic-ischemic encephalopathy. H: diffuse hemorrhages. L: fibrinosuppurative consolidation. |
| Chen L et al., 2013 [15] | China | 43/M | n.a. | Yes (at the end); n.a. | 5 d | Agkistrodom halysViperidae | Right foot. 0.3 cm-long laceration made of two pairs of thin stripes. Right foot swollen and ecchymotic. | Subcutaneous hemorrhage and cellulitis. | Diffuse edema and congestion. | K: Toxic nephropathy, proximal tubular epithelial degeneration, and necrosis, protein and pigment cast in the distal tubules. |
| Chen L et al., 2013 [15] | China | 4/M | n.a. | Yes; n.a. | 2 d | Agkistrodom halysViperidae | Right foot. 1.2 × 0.5 cm snakebite wound. | n.a. | Diffuse edema and congestion.S: anemic aspect. | B, T, K: congestion. H, L: edema and congestion. |
| Curry SC et al., 1985 [16] | USA | 44/F | No | Yes; Yes | 15 d | Rattlesnake Viperidae | Right calf. Two fang marks surrounded by an area of discoloration. | Area of tissue disruption leading toward a vein. Small eschar over the site of fang penetration through epidermidis. | B, Li, S: enlarged and congested. H: lightly dilated and flabby; superficial hemorrhages. L: expanded and indurated. | B: focal hemorrhages in the leptomeninges. L: severe ARDS. K: eosinophilic proteinaceous casts in small tubules. |
| Karlawad M et al., 2017 [17] | India | 75/M | Yes | Yes; Yes | 3 h | n.a. | Scrotum. Two punctured wounds surrounded by an area of discoloration. | Ulcerated stratified squamous epithelium with sub-epithelial tissue showing congested blood vessels and edema. | Diffuse congestion. | L: interstitial and intra-alveolar edema with rupture of alveoli. H: unremarkable. |
| Keith J et al., 2012 [18] | Australia | 69/F | No | Yes; Yes | 2 d | Australian Brown Snake (Pseudonaja textilis) Elapidae | Foot. | n.a. | B: swollen with tonsillar herniation and V-shaped hemorrhage within the cerebellum. | Unremarkable. |
| Kitchens CS et al., 1987 [19] | USA | 67/M | No | Yes; Yes | 2 d 12 h | Canebrake Rattlesnake (Crotalus Horridus Atricaudatus) Viperidae | Left Hand. Two puncture wounds. | Rhabdomyolysis. The left thenar muscle disclosed a sparse infiltration of PMNs. | M: soft consistency underlying the bite. | H: patchy myocardial necrosis. L: hemorrhagic pulmonary edema; small scattered pulmonary thrombi consistent with terminal DIC. K: massive acute tubular necrosis. M: rhabdomyolysis of the skeletal muscles. |
| Malbranque S et al., 2008 [20] | Martinique | 74/M | Yes | Yes; Yes | 10 d | Fer-de-Lance (Bothrops lanceolatus) Viperidae | Left elbow. Fang puncture marks 20 mm apart surrounded by a swollen area. | n.a. | Serous effusions in the peritoneal, pericardial, and pleural cavities. B: edema with petechiae. H: infarcts of different ages and sizes. L: edematous and congested. | B: ischemic changes; thrombotic lesions were confined to the sub-arachnoid space. H: Fibrinous pericarditis and scattered ischemic foci in the LV. L: thrombotic lesion within the small pulmonary arteries and the capillaries of the inter-alveolar septa. K: thrombotic lesion within the small renal inter-lobular vessels and, to a localized extent. I: thrombotic lesion in the small intestine and colon. |
| Malhotra P et al., 2005 [21] | India | 27/F | n.a. | Yes; Yes | n.a. | n.a. | Left foot. Fang marks. | n.a. | Unremarkable. | B: extensive perivascular demyelination and limphocyte cuffing. K: acute tubular necrosis. |
| Marsh N, et al., 2007 [22] | USA (captivity) | 33/F | No | No; No | n.a. | Gaboon viper (Bitis gabonica) Viperidae | Left hand. Two puncture wounds 11–12 mm apart surrounded by a swollen and bloody area. | n.a. | Ecchymoses of the head, trunk and extremities, the periorbital areas, and left orolaryngeal/mandibular angle. L: hemorrhagic appearance and congestion. | n.a. |
| McGarity BH et al., 1991 [23] | Australia | 40/M | n.a. | Yes; Yes | 2 d | Tiger snake (Notechis scutatus) Elapidae | Left heel. | n.a. | B: edematous; right tentorial and subfalcial herniation; massive right intracerebral hemorrhage, with rupture into the right basal ganglia and cerebellum. | n.a. |
| Milani R Jr et al., 1997 [24] | Brazil | 3/F | No | Yes; Yes | 18 h 40 min | Jararacuçu (Bothrops jararacussu) Viperidae | Left thigh. Three widely spaced fang puncture marks. | Extensive rhabdomyolysis with hemorrhagic foci. Hemorrhage and necrosis in the dermis and hemorrhage in subcutaneous fat near the site. | B: edema. | L: hemorrhages with inflammatory infiltration of neutrophils in septa and alveoli and deposition of intra-alveolar fibrin. Li: hepatic sinusoids and portal tracts infiltrated with PMNs. P: fatty necrosis with hemorrhage of the parenchymal cells. |
| Milani R Jr et al., 1997 [24] | Brazil | 65/M | n.a. | Yes; Yes | 4 d 9 h | Jararacuçu (Bothrops jararacussu) Viperidae | Left calf. Two fang punctures surrounded by a ring of bruising. | Necrosis of muscle fibers and interstitial hemorrhage in the region of the wound. | B: subarachnoid petechiae and edema. | B: ischemic necrosis of the mucosa and in small cortical and meningeal vessels with local meningeal hemorrhage and cerebral edema. Li: fatty (alcoholic) liver with evidence of shock. I: fibrin thrombi in small sub-mucosal vessels. AG: focal hemorrhages in the medulla, with depletion of the zona fasciculata. K: acute tubular necrosis DIC. |
| Moar JJ et al., 2016 [25] | South Africa | 23/M | Yes | Yes; No | Several hours | Rinkhal (Hemachatus haemachatus) Elapidae | Right forearm. Two bite marks each 3 mm in diameter and 1.5 cm apart. | Displaced and disrupted fragments of adnexal structures into the depths of the wound, together with hemorrhaging into the surrounding interstitium, and compression of the collagen bundles of the dermis with collagen displacement and disruption. | B, L: edema and petechial hemorrhages. | B: Extravasation of erythrocytes into the surrounding Virchow–Robin spaces. H: in LV marked interstitial vascular dilatation and congestion with focal subendocardial papillary muscle fibrosis. L: ARDS. Li: portal vessels congestion and widening by reticulin and a portal triaditis. S: sinusoidal dilatation and congestion; mantle zone hyperplasia. K: interstitial vascular and glomerular capillary loop dilatation and congestion with a chronic inflammatory cell infiltrate. |
| Namal Rathnayaka RMMK et al., 2018 [26] | Sri Lanka | 42/M | Yes | Yes; No | 16 d | Hump nose Viper (Hypnale Hypnale) Viperidae | Right foot. | n.a. | B: a small infarct (1.5 cm–1 cm) in the basal ganglia. H: reduced lumen of the left coronary artery. | L: hemorrhages. K: acute tubular necrosis. H: normal. |
| Namal Rathnayaka RMMK et al., 2019 [27] | Sri Lanka | 66/M | No | Yes; No | 4 d | Hump nose Viper (Hypnale Hypnale) Viperidae | Left foot. Two fang punctures. | n.a. | B, H, L: hemorrhages. | L: edema and hemorrhage. |
| Namal Rathnayaka RMMK et al., 2017 [28] | Sri Lanka | 43/M | No | Yes; Yes | 11 d | Russell’s viper (Daboia russelii) Viperidae | Right foot. Swelling of the leg. | n.a. | B: infarcted area of parietal lobes. K: petechial hemorrhages. | B: hemorrhages, thrombi, and congested blood vessels. H, L, K: normal. |
| Norris RL et al., 2009 [29] | USA | 38/M | No | No; No | 2 h | Coral snake (Micrurus fulvius) Elapidae | Right Hand; Left Arm. Fresh 6 mm linear abrasion and multiple punctuate abrasions in a small group. | n.a. | L: congestion. | Unremarkable. |
| Okamoto O et al., 2017 [30] | Japan | 84/F | Yes | Yes; Yes | 35 d | Mamushi (Gloydius Blomhoffii) Viperidae | Right elbow. | n.a. | Li: acute necrosis. I: extensive patchy necrosis at the small intestine; multiple ulcers and bleeding at the ascending colon. K: cortical necrosis. | Li: necrosis around the central vein. I: necrosis extended to the muscle layer. K: glomerular necrosis. |
| Paulis MG et al., 2016 [31] | Egypt | 9/F | No | No; Yes | n.a. | Egyptian Cobra (Naja Haje) Elapidae | Right leg. Five pairs of fang marks with almost fixed distance between the paired ones, all surrounded by erythema and little swelling. | n.a. | Internal organ congestion. | n.a. |
| Paulis MG et al., 2016 [31] | Egypt | 6/F | No | No; No. | n.a. | Egyptian Cobra (Naja Haje) Elapidae | Left leg. Two pairs of fang marks, each pair was symmetrical, all surrounded by erythema and little swelling. | n.a. | Internal organ congestion. | n.a. |
| Paulis MG et al., 2016 [31] | Egypt | 4/F | No | No; No. | n.a. | Egyptian Cobra (Naja Haje) Elapidae | Right leg. Multiple fang marks close to each other surrounded by erythema. | n.a. | Internal organ congestion. | n.a. |
| Pramod Kumar GN et al., 2013 [32] | India | 68/M | n.a. | Yes; n.a. | 4 d | n.a. | Right thigh. Bluish black discoloration of the outer aspect of the right thigh and of the right leg. Multiple blisters and ulcerative necrosis. Extravasation of blood in the subcutaneous plane. | n.a. | Unremarkable (coexistence of gastric and kidney cancers). | n.a. |
| Quain, 1852 [33] | England (captivity) | 30/M | Yes | Yes: No. | 1 h 30 min | Hooded Snake - Cobra de Capello (Naja tripudians) Elapidae | Face. Three puncture marks surrounded by an ecchymotic area. | n.a. | Congestion of all internal organs, particularly of the spleen. | n.a. |
| Rathnayaka RMMKN et al., 2017 [34] | Sri Lanka | 53/M | n.a. | Yes; Yes | 26 d | Russell’s viper (Daboia russelii) Viperidae | Right Leg. Swollen area. | n.a. | B: infarcted area of parietal lobes of the brain. K: reduced cortico-medullary demarcation in both kidneys and petechial hemorrhages. | n.a. |
| Sarkar N et al., 2018 [3] | India | 27/M | No | No; No. | almost 6 h | Banded Krait (Bungarus faciatus) Elapidae | Hand. Two pin-point punctured wounds, subcutaneous deep, placed 8 mm apart. | n.a. | Internal organ congestion K: bilateral cortico-medullary hemorrhage and congestion. | K: interstitial hemorrhage; inflammatory cell infiltration and swelling. |
| Sarkar N et al., 2018 [3] | India | 26/F | No | No; No | almost 6 h | Banded Krait (Bungarus faciatus) Elapidae | Right shoulder. Two pin-point punctured wounds. | n.a. | Internal organ congestion K: bilateral cortico-medullary hemorrhage and congestion. | K: interstitial hemorrhage and inflammatory cell infiltration. |
| Sarkar N et al., 2018 [3] | India | 4/F | No | No; No | almost 6 h | Banded Krait (Bungarus faciatus) Elapidae | Right foot. | n.a. | Internal organ congestion. K: bilateral cortico-medullary hemorrhage and congestion. | K: increased cytoplasmatic eosinophilia and occasional surface blebbing of the renal tubular epithelial cell (early ischemic injury). |
| Silva A et al., 2013 [35] | Sri Lanka | 19/M | No | Yes; Yes | 1 d 22 h | Indian Krait (Bungarus caeruleus) Elapidae | n.a. | n.a. | H, L, K: Petechial hemorrhages and edema. | n.a. |
| Silva de Oliveira S et al., 2017 [36] | Brazil | 59/F | No | Yes; Yes | 2 d | Jaracaca do Norte (Bothrops atrox) Viperidae | Right foot. Ecchymotic and swollen area. | n.a. | B: Subarachnoid and intraparenchymal hemorrhage. | n.a. |
| Soe S et al.,1993 [37] | Myanmar | 13/M | n.a. | n.a.; n.a. | n.a. | Russell’s Viper (Vipera Russelli) Viperidae | n.a. | n.a. | n.a. | K: Glomerular changes: endothelial swelling, increased cells; degeneration and necrosis of the tubules, and fibrin deposition. |
| Soe S et al.,1993 [37] | Myanmar | 15/F | n.a. | n.a.; n.a. | n.a. | Russell’s Viper (Vipera Russelli) Viperidae | n.a. | n.a. | n.a. | K: Glomerular changes: endothelial swelling, increased cells; degeneration and necrosis of the tubules, and fibrin deposition. |
| Soe S et al.,1993 [37] | Myanmar | 15/F | n.a. | n.a.; n.a. | n.a. | Russell’s Viper (Vipera Russelli) Viperidae | n.a. | n.a. | n.a. | K: Glomerular changes: endothelial swelling, increased cells; degeneration and necrosis of the tubules, and fibrin deposition. |
| Soe S et al.,1993 [37] | Myanmar | 49/M | n.a. | n.a.; n.a. | n.a. | Russell’s Viper (Vipera Russelli) Viperidae | n.a. | n.a. | n.a. | K: Glomerular changes: endothelial swelling, increased cells; degeneration and necrosis of the tubules, and fibrin deposition |
| Sutherland SK, 1992 [38] | Australia | 16/F | No | Yes; n.a. | 1 h | Brown snake (Pseudonaja Textilis) Elapidae | Right heel. Fang marks 5 mm apart. | n.a. | Unremarkable. | n.a. |
| Sutherland SK, 1992 [38] | Australia | 27/F | n.a. | Yes; n.a. | 1 h 30 min | Brown snake Elapidae | n.a. | n.a. | Unremarkable. | n.a. |
| Sutherland SK, 1992 [38] | Australia | 61/F | NO | Yes; No | 1 h 30 min | Brown snake Elapidae | Right ankle. | n.a. | Small retroperitoneal hemorrhage. | n.a. |
| Sutherland SK, 1992 [38] | Australia | 51/M | n.a. | Yes; Yes | 1 h | Taipan Elapidae | n.a. | n.a. | Unremarkable. | n.a. |
| Sutherland SK, 1992 [38] | Australia | 2/F | No | No; No | n.a. | Brown snake Elapidae | Left leg. Two minute puncture wounds. | n.a. | L: congestion and edema with numerous petechial hemorrhages on the visceral pleurae. | n.a. |
| Sutherland SK, 1992 [38] | Australia | 42/M | No | Yes; Yes | 5 h 30 min | Taipan Elapidae | n.a. | n.a. | Unremarkable. | n.a. |
| Sutherland SK, 1992 [38] | Australia | 60/M | Yes | Yes; Yes | 25 min | Brown snake Elapidae | Right Foot. | n.a. | Unremarkable. | n.a. |
| Sutherland SK, 1992 [38] | Australia | 35/M | No | No; No | 35 min | Brown snake (Pseudonaja Textilis) Elapidae | Right hand. | n.a. | H: Coronary arteries disease. Li: cirrhosis. | n.a. |
| Sutherland SK, 1992 [38] | Australia | 48/F | No | No; No | 30 min | n.a. | Right Foot. Two tiny puncture wounds. | n.a. | n.a. | Quantities of venom in urine that reacted to tiger snake venom. |
| Than-Than et al., 1989 [39] | Myanmar | 19/M | Yes | Yes (at the end); Yes | 14 h | Russell’s Viper (Vipera Russelli Siamensis) Viperidae | Ankle. bruising area. | n.a. | L: petechial hemorrhages. | PG: marked acute congestion. L: intraseptal capillaries were congested and contained fibrin thrombi as did some of the large pulmonary vessels, erythrocytes in the alveoli but no definite hemorrhage. S: red pulp congested with pseudoamyloid change in the central arterioles of some of the malpighian corpuscles. Li: congested with some nonspecific inflammatory cells. K: the glomerular tufts were congested and some contained fibrin thrombi; early tubular necrosis. B, H, AG: normal. |
| Than-Than et al., 1989 [39] | Myanmar | 17/M | Yes | Yes (at the end); Yes | 1 d 12 h | Russell’s Viper (Vipera Russelli Siamensis) Viperidae | Foot. | Hemorrhage, necrosis, and the presence of fibrin thrombi in small vessels. Subcutaneous fibrofatty tissue heavily infiltrated by a mixture of PMNs, leucocytes, lymphocytes, and eosinophils. Dense acidophilic homogeneous fibrin-like material in the surrounding blood vessels. | Serous fluid in the pleural and peritoneal cavities. B: edema. PG, AG: diffusely hemorrhagic. H, L: petechial hemorrhages. K: demarcation between dark red medulla and pale cortex. | PG: congestion and hemorrhage with foci of fibrinous material. H: numerous focal hemorrhages on the epicardial and endocardial surfaces. L: intense capillary wall congestion. AG: patchy congestion and focal hemorrhages. K: glomerular congestion; marked congestion of the medulla and corticomedullary junction with interstitial hemorrhages; early tubular necrosis. |
| Than-Than et al., 1989 [39] | Myanmar | 15/F | Yes | Yes; Yes | 2 d 4 h | Russell’s Viper (Vipera Russelli Siamensis) Viperidae | Foot. | n.a. | B: edematous and congested. Large blood clot (5 × 12 mm) in the pituitary fossa. PG: dark grey in color and hemorrhagic parenchyma. L, H, St: subserosal hemorrhage. AG: hemorrhagic. K: Blood clots in the pelvises. Contrasting red medulla and pale cortex. | B: edematous with dilatation of perineuronal and Virchow-Robin spaces. PG: extensive areas of hemorrhage and intense congestion of the sinusoids. L: acute alveolar wall congestion without hemorrhage, fibrin thrombi or edema. S: expansion of the red pulp. K: glomerular congestion with slight increase in cellularity. Early tubular necrosis. |
| Tibballs J et al., 1991 [40] | Australia | 11/M | No | Yes; Yes | Less than 1 d | Tiger snake (Notechis scutatus) Elapidae | Left wrist. | n.a. | B: multiple intracerebral hemorrhages and subarachnoid collections of blood. | n.a. |
| Tilbury CR et al., 2016 [41] | Congo | 46/M | Yes | Yes; Yes | 2 h 20 min | Burrowing Asps (Atractaspis corpulenta) Lamprophiidae | Left hand. Punctuation-shaped wound (!), 2.5 mm in length surrounded by a non-specified rash. | Disruption of the epidermal and dermal tissue layers, with associated fresh hemorrhage. | Diffuse congestion of the organs. H: flabby. L: edematous and congested. | H: acute ischemic changes, foci of contraction band necrosis with no accompanying inflammatory response. L: prominent pulmonary edema and severe pulmonary congestion. |
| Tranca S et al., 2016 [42] | Romania | 56/M | n.a. | Yes; Yes | n.a. | Vipera Berus Viperidae | Right tight. Two puncture wounds surrounded by a purpuric area. | Diffuse epidermal necrosis associated with micro-hemorrhages and micro-thrombosis in the dermis and hypodermis. | H, L: edema. | B: edema and hemorrhagic lesions in the leptomeninges. H: myocardial fibrosis, epicardial and interstitial hemorrhages. L: atelectasia and pulmonary hemorrhagic edema. Li: diffuse hepatic necrosis. I: enteral necrosis and acute mucosal hemorrhages. K: acute tubular necrosis. |
| Varagunam T et al., 1970 [43] | Sri Lanka | 30/M | Yes | Yes; No | 11 d | Pit-Viper (Agkistrodom hypnale) Viperidae | Left hand. Scars of two fang marks. | n.a. | K: larger, external surface was smooth with many areas of necrosis or hemorrhage; necrotic areas confined to the cortices; the medullae were congested. H, L, Li, S, I, AG: normal. | Li: early fatty changes. K: irregular areas of coagulative necrosis in the cortices; both glomeruli and tubules were involved in the necrotic process; Necrosis in many intralobular arteries and arterioles. |
| Wankhede AG, 2004 [44] | India | 25/M | Yes | Yes, n.a. | 1 d | Russell’s Viper (Vipera Russelli Siamensis) Viperidae | Right ankle. Two puncture wounds of diameter 1.5 mm each and 2.3 cm apart and puncture lacerated wounds one 7 mm below the lateral puncture wound, 1.5 cm in length, and the second 1.6 cm below the medial puncture wound 6 mm in length. | n.a. | B: petechial hemorrhages, congestion and edema. L: congestion and edema. | Unremarkable. |
| Warrell DA et al., 1976 [45] | Nigeria | 10/M | No | No; No | 2 h | Egyptian Cobra (Naja Haje) Elapidae | Right hand. Two fang punctures 2 cm apart, surrounded by a swollen area. | n.a. | Unremarkable. | B, H: normal. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feola, A.; Marella, G.L.; Carfora, A.; Della Pietra, B.; Zangani, P.; Campobasso, C.P. Snakebite Envenoming a Challenging Diagnosis for the Forensic Pathologist: A Systematic Review. Toxins 2020, 12, 699. https://doi.org/10.3390/toxins12110699
Feola A, Marella GL, Carfora A, Della Pietra B, Zangani P, Campobasso CP. Snakebite Envenoming a Challenging Diagnosis for the Forensic Pathologist: A Systematic Review. Toxins. 2020; 12(11):699. https://doi.org/10.3390/toxins12110699
Chicago/Turabian StyleFeola, Alessandro, Gian Luca Marella, Anna Carfora, Bruno Della Pietra, Pierluca Zangani, and Carlo Pietro Campobasso. 2020. "Snakebite Envenoming a Challenging Diagnosis for the Forensic Pathologist: A Systematic Review" Toxins 12, no. 11: 699. https://doi.org/10.3390/toxins12110699
APA StyleFeola, A., Marella, G. L., Carfora, A., Della Pietra, B., Zangani, P., & Campobasso, C. P. (2020). Snakebite Envenoming a Challenging Diagnosis for the Forensic Pathologist: A Systematic Review. Toxins, 12(11), 699. https://doi.org/10.3390/toxins12110699