Psychometric Properties of a Developed Questionnaire to Assess Knowledge, Attitude and Practice Regarding Vitamin D (D-KAP-38)

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Data Collection
2.2. Measures
2.3. Scale Development Procedure
2.4. Item Generation
2.5. Validity Assessment
2.6. Reliability Assessment
2.7. Scoring Method
2.8. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Duranton, F.; Rodriguez-Ortiz, M.E.; Duny, Y.; Rodriguez, M.; Daurès, J.P.; Argilés, A. Vitamin D treatment and mortality in chronic kidney disease: A systematic review and meta-analysis. Am. J. Nephrol. 2013, 37, 239–248. [Google Scholar] [CrossRef] [PubMed]
- Girgis, C.M.; Clifton-Bligh, R.J.; Hamrick, M.W.; Holick, M.F.; Gunton, J.E. The roles of vitamin D in skeletal muscle: Form, function, and metabolism. Endocr. Rev. 2013, 34, 33–83. [Google Scholar] [CrossRef] [PubMed]
- Rosen, C.J.; Adams, J.S.; Bikle, D.D.; Black, D.M.; Demay, M.B.; Manson, J.E.; Murad, M.H.; Kovacs, C.S. The nonskeletal effects of vitamin D: An Endocrine Society scientific statement. Endocr. Rev. 2012, 33, 456–492. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Guidelines for preventing and treating vitamin D deficiency and insufficiency revisited. J. Clin. Endocrinol. Metab. 2012, 97, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 Dietary Reference Intakes for Calcium and Vitamin D: What Dietetics Practitioners Need to Know. J. Am. Diet. Assoc. 2011, 111, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Hashemipour, S.; Larijani, B.; Adibi, H.; Javadi, E.; Sedaghat, M.; Pajouhi, M.; Soltani, A.; Shafaei, A.R.; Hamidi, Z.; Fard, A.R.; et al. Vitamin D deficiency and causative factors in the population of Tehran. BMC Public Health 2004, 4, 38. [Google Scholar] [CrossRef] [PubMed]
- Hovsepian, S.; Amini, M.; Aminorroaya, A.; Amini, P.; Iraj, B. Prevalence of vitamin D deficiency among adult population of Isfahan City, Iran. J. Health Popul. Nutr. 2011, 29, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Kazemi, A.; Sharifi, F.; Jafari, N.; Mousavinasab, N. High prevalence of vitamin D deficiency among pregnant women and their newborns in an Iranian population. J. Womens Health 2009, 18, 835–839. [Google Scholar] [CrossRef] [PubMed]
- Mithal, A.; Wahl, D.A.; Bonjour, J.P.; Burckhardt, P.; Dawson-Hughes, B.; Eisman, J.A.; El-Hajj, F.G.; Josse, R.G.; Lips, P.; Morales-Torres, J.; et al. Global vitamin D status and determinants of hypovitaminosis D. Osteoporos. Int. 2009, 20, 1807–1820. [Google Scholar] [CrossRef] [PubMed]
- Ginde, A.A.; Liu, M.C.; Camargo, C.A., Jr. Demographic differences and trends of vitamin D insufficiency in the US population, 1988–2004. Arch. Intern. Med. 2009, 169, 626–632. [Google Scholar] [CrossRef] [PubMed]
- Bonevski, B.; Girgis, A.; Magin, P.; Horton, G.; Brozek, I.; Armstrong, B. Prescribing sunshine: A cross-sectional survey of 500 Australian general practitioners’ practices and attitudes about vitamin D. Int. J. Cancer 2012, 130, 2138–2145. [Google Scholar] [CrossRef] [PubMed]
- Gao, Q.; Liu, G.; Liu, Y. Knowledge, attitude and practice regarding solar ultraviolet exposure among medical university students in Northeast China. J. Photochem. Photobiol. B Biol. 2014, 140, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Kung, A.W.; Lee, K.-K. Knowledge of vitamin D and perceptions and attitudes toward sunlight among Chinese middle-aged and elderly women: A population survey in Hong Kong. BMC Public Health 2006, 6, 226. [Google Scholar] [CrossRef] [PubMed]
- Vu, L.H.; van der Pols, J.C.; Whiteman, D.C.; Kimlin, M.G.; Neale, R.E. Knowledge and attitudes about vitamin D and impact on sun protection practices among urban office workers in Brisbane, Australia. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1784–1789. [Google Scholar] [CrossRef] [PubMed]
- Al Bathi, B.A.; Al Zayed, K.E.; Al Qenai, M.; Makboul, G.; El-Shazly, M.K. Knowledge, attitude and practice of patients attending primary care centers toward vitamin D in Kuwait. Alex. J. Med. 2012, 48, 277–282. [Google Scholar] [CrossRef]
- Al-Saleh, Y.; Al-Daghri, N.M.; Khan, N.; Alfawaz, H.; Al-Othman, A.M.; Alokail, M.S.; Chrousos, G.P. Vitamin D status in Saudi school children based on knowledge. BMC Pediatr. 2015, 15, 53. [Google Scholar] [CrossRef] [PubMed]
- Boland, S.; Irwin, J.D.; Johnson, A.M. A Survey of University Students’ Vitamin D–Related Knowledge. J. Nutr. Educ. Behav. 2015, 47, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Christie, F.T.; Mason, L. Knowledge, attitude and practice regarding vitamin D deficiency among female students in Saudi Arabia: A qualitative exploration. Int. J. Rheum. Dis. 2011, 14, e22–e29. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.; Zhuang, W.; Yuan, Y.; Li, Z.; Cai, Y. Investigation on vitamin D knowledge, attitude and practice of university students in Nanjing, China. Public Health Nutr. 2016, 19, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Walker, N.; Love, T.D.; Baker, D.F.; Healey, P.B.; Haszard, J.; Edwards, A.S.; Black, K.E. Knowledge and attitudes to vitamin D and sun exposure in elite New Zealand athletes: A cross-sectional study. J. Int. Soc. Sports Nutr. 2014, 11, 47. [Google Scholar] [CrossRef] [PubMed]
- Deschasaux, M.; Souberbielle, J.C.; Partula, V.; Lécuyer, L.; Gonzalez, R.; Srour, B.; Guinot, C.; Malvy, D.; Latino-Martel, P.; Druesne-Pecollo, N.; et al. What Do People Know and Believe about Vitamin D? Nutrients 2016, 8, 718. [Google Scholar] [CrossRef] [PubMed]
- Lawshe, C.H. A quantitative approach to content validity1. Pers. Psychol. 1975, 28, 563–575. [Google Scholar] [CrossRef]
- Hooper, D.; Coughlan, J.; Mullen, M. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Kim, M.K.; Il Kang, M.; Won Oh, K.; Kwon, H.S.; Lee, J.H.; Lee, W.C.; Yoon, K.H.; Son, H.Y. The association of serum vitamin D level with presence of metabolic syndrome and hypertension in middle-aged Korean subjects. Clin. Endocrinol. 2010, 73, 330–338. [Google Scholar] [CrossRef] [PubMed]
- Toher, C.; Lindsay, K.; McKenna, M.; Kilbane, M.; Curran, S.; Harrington, L.; Uduma, O.; McAuliffe, F.M. Relationship between vitamin D knowledge and 25-hydroxyvitamin D levels amongst pregnant women. J. Hum. Nutr. Diet. 2014, 27, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Janda, M.; Youl, P.; Bolz, K.; Niland, C.; Kimlin, M. Knowledge about health benefits of vitamin D in Queensland Australia. Prev. Med. 2010, 50, 215–216. [Google Scholar] [CrossRef] [PubMed]
- Spong, C.Y.; Berghella, V.; Wenstrom, K.D.; Mercer, B.M.; Saade, G.R. Preventing the first cesarean delivery: Summary of a joint Eunice Kennedy Shriver national institute of child health and human development, society for maternal-fetal medicine, and American college of obstetricians and gynecologists workshop. Obstet. Gynecol. 2012, 120, 1181. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Variable | Number | % |
|---|---|---|
| Female | 308 | 54.1 |
| Married | 397 | 70.0 |
| Age (years) | ||
| ≤30 | 334 | 61.9 |
| >30 | 206 | 38.1 |
| Parity | ||
| 0 | 313 | 54.7 |
| 1 | 127 | 22.2 |
| ≥2 | 132 | 23.1 |
| Education level | ||
| Primary | 74 | 13.0 |
| Secondary | 222 | 39.0 |
| Higher | 273 | 48.0 |
| Employed | 324 | 58.1 |
| Residential area | ||
| North of Tehran | 184 | 36.0 |
| South of Tehran | 327 | 64.0 |
| Intake of vitamin D supplement | 148 | 26.1 |
| N | Questions | Factor Loading | |||
|---|---|---|---|---|---|
| General Knowledge | Nutrition Knowledge | Attitude | Practice | ||
| 1 | People, who work indoors, are at high risk of vitamin D deficiency. | 0.642 | −0.156 | 0.004 | 0.059 |
| 2 | Vitamin D intake more than dietary recommendations could be harmful. | 0.599 | −0.108 | −0.130 | −0.043 |
| 3 | Elderly people are at high risk of vitamin D deficiency. | 0.498 | 0.149 | 0.037 | 0.102 |
| 4 | Inappropriate dietary intakes are related to vitamin D deficiency. | 0.495 | 0.280 | −0.074 | −0.083 |
| 5 | Vitamin D supplement intake requirements, differ for different age groups. | 0.449 | 0.263 | 0.110 | −0.092 |
| 6 | Pregnant and lactating women are at high risk of vitamin D deficiency. | 0.439 | −0.012 | 0.048 | 0.040 |
| 7 | Most of the vitamin D required is produced when the skin is directly exposed to the sun. | 0.395 | −0.171 | 0.081 | −0.069 |
| 8 | Currently, vitamin D deficiency is one of the most important health issues in Iran. | 0.379 | 0.265 | 0.227 | 0.161 |
| 9 | Bone pain and fatigue are among the vitamin D deficiency symptoms. | 0.330 | 0.227 | −0.040 | 0.133 |
| 10 | Vitamin D supplement intake requirements, differ in various seasons of the year. | 0.321 | 0.127 | 0.202 | −0.124 |
| 11 | Both men and women are at risk of vitamin D deficiency. | 0.320 | 0.068 | −0.106 | 0.211 |
| 12 | All age groups are at risk of vitamin D deficiency. | 0.249 | 0.153 | 0.087 | −0.057 |
| 13 | Fatty fishes are one of the main dietary sources of vitamin D. | 0.394 | 0.336 | 0.097 | −0.042 |
| 14 | Dairy products are one of the main dietary sources of vitamin D. | −0.125 | −0.646 | −0.051 | −0.100 |
| 15 | Eggs are one of the main dietary sources of vitamin D. | −0.133 | −0.571 | −0.171 | −0.046 |
| 16 | Meat and poultry are the main dietary sources of vitamin D. | 0.029 | −0.526 | −0.074 | 0.044 |
| 17 | Fruits are one of the main dietary sources of vitamin D. | 0.053 | −0.300 | 0.051 | −0.052 |
| 18 | Clothes prevent the skin from producing vitamin D. | 0.125 | 0.159 | 0.054 | 0.072 |
| 19 | Sun exposure through glass, prevents the skin from producing vitamin D. | 0.048 | 0.154 | 0.031 | 0.023 |
| 20 | Urbanization prevents sun exposure and production of required vitamin D. | 0.212 | −0.039 | 0.575 | −0.261 |
| 21 | A shortage of public places for outdoor activities prevents the sun exposure required for production of vitamin D. | 0.235 | −0.151 | 0.558 | 0.005 |
| 22 | Full time indoor occupation prevents the sun exposure required for production of vitamin D. | 0.300 | −0.131 | 0.552 | −0.089 |
| 23 | Inefficient education regarding benefits of sun exposure prevents production of required vitamin D through sun exposure. | 0.323 | −0.061 | 0.531 | 0.070 |
| 24 | The undesirable taste of sea foods for Iranians is one of the barriers to their consumption of dietary sources of vitamin D. | 0.257 | 0.140 | 0.467 | 0.019 |
| 25 | In vitamin D deficiency, supplement intake is more effective compared to dietary intake and sun exposure. | −0.182 | 0.075 | 0.464 | 0.218 |
| 26 | Taking vitamin D supplement, unless recommended by physicians is wrong. | 0.036 | −0.080 | 0.430 | 0.019 |
| 27 | Unwillingness of individuals to take vitamin D supplement is one of the barriers of providing this nutrient. | 0.020 | 0.161 | 0.424 | 0.192 |
| 28 | Taking supplements is beneficial in case of not consuming dietary sources of vitamin D. | 0.081 | 0.041 | −0.401 | −0.116 |
| 29 | Taking supplements is necessary for treatment of vitamin D deficiency but not for its prevention. | −0.155 | 0.135 | 0.398 | −0.008 |
| 30 | Permanent using of sunscreens on face, neck and hands prevents the sun exposure required for production of vitamin D. | −0.078 | 0.026 | 0.396 | 0.077 |
| 31 | To prevent vitamin D deficiency, taking supplements is easier, compared to dietary intakes and sun exposure. | −0.255 | 0.217 | 0.355 | 0.103 |
| 32 | Taking supplements is only necessary in case of lack of exposure to sunlight. | 0.165 | 0.258 | 0.301 | 0.057 |
| 33 | A high expense of dietary sources of vitamin D is one of the barriers of providing this nutrient. | 0.009 | −0.325 | 0.303 | 0.257 |
| 34 | Cloudy weather prevents absorption of ultra violet and producing vitamin D by skin. | −0.018 | 0.028 | 0.251 | 0.006 |
| 35 | Vitamin D supplementation is recommended for individuals suffering from vitamin D deficiency. | 0.026 | 0.113 | 0.224 | −0.042 |
| 36 | Vegetarians are at high risk of vitamin D deficiency. | 0.112 | 0.128 | 0.204 | 0.130 |
| 37 | Air pollution prevents absorption of ultra violet and production of vitamin D by skin. | 0.130 | 0.152 | 0.169 | 0.080 |
| 38 | For sufficient exposure to sunlight I regularly engage in outdoor physical activities. | −0.073 | 0.038 | 0.089 | 0.691 |
| 39 | To be vitamin D sufficient, I consume fortified milk. | −0.063 | 0.102 | 0.119 | 0.661 |
| 40 | In order to be vitamin D sufficient, I consume fish at least twice a week. | −0.032 | 0.170 | 0.125 | 0.618 |
| 41 | For sufficient exposure to sunlight I walk outdoors daily. | 0.096 | −0.055 | 0.055 | 0.616 |
| 42 | I use caps/hats to avoid severe sun exposure. | −0.122 | 0.078 | 0.038 | −0.515 |
| 43 | To be vitamin D sufficient, I take vitamin D supplements. | −0.058 | 0.242 | 0.161 | 0.512 |
| 44 | I use sunscreen on my hands. | 0.069 | −0.178 | 0.032 | −0.455 |
| 45 | During the day I am directly exposed to sunlight (outdoors). | 0.028 | −0.263 | 0.015 | 0.395 |
| 46 | During the day I am indirectly exposed to sunlight (through glass). | −0.071 | 0.265 | −0.126 | −0.316 |
| 47 | I use sunscreen on my face. | −0.072 | −0.265 | 0.056 | −0.300 |
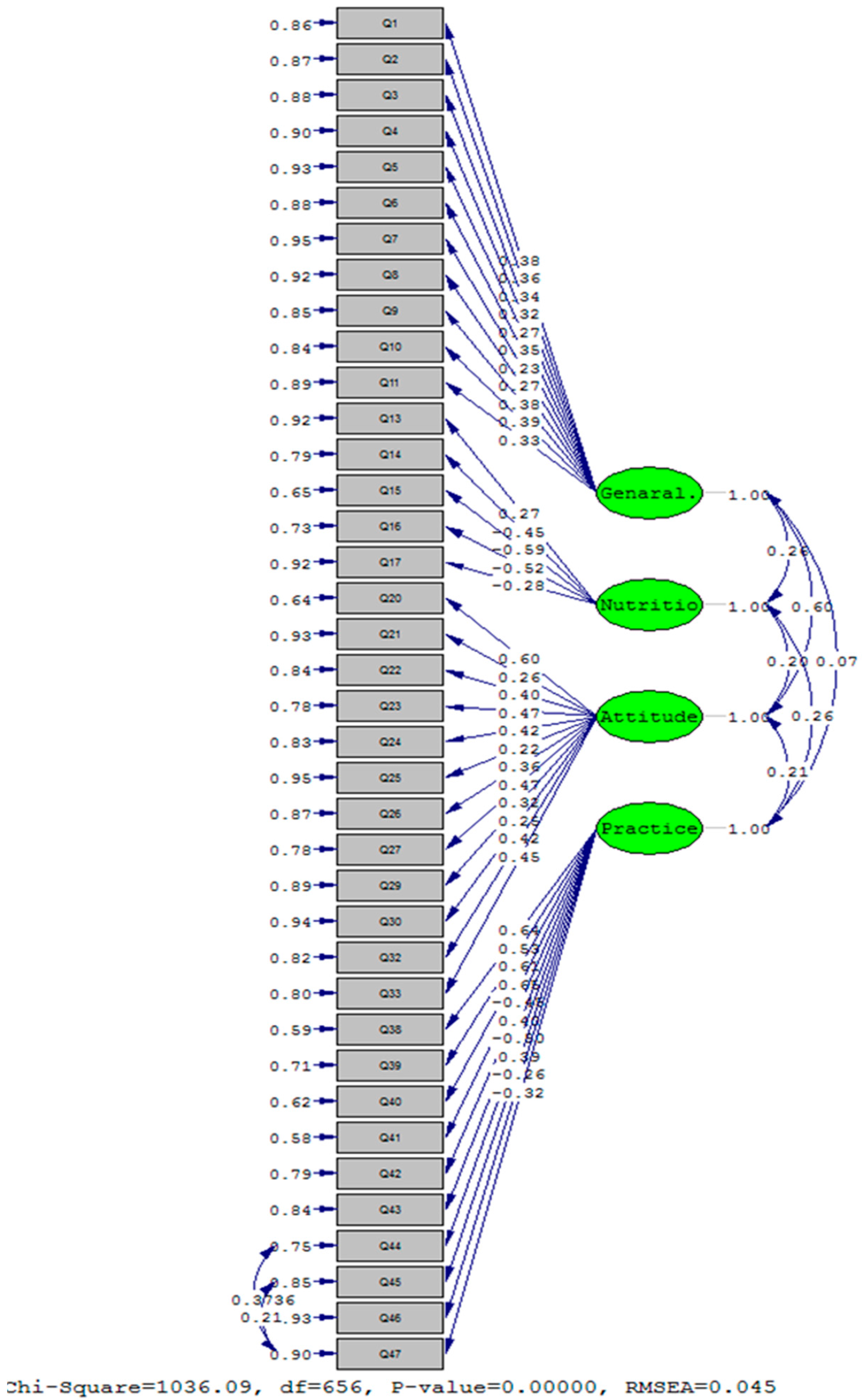
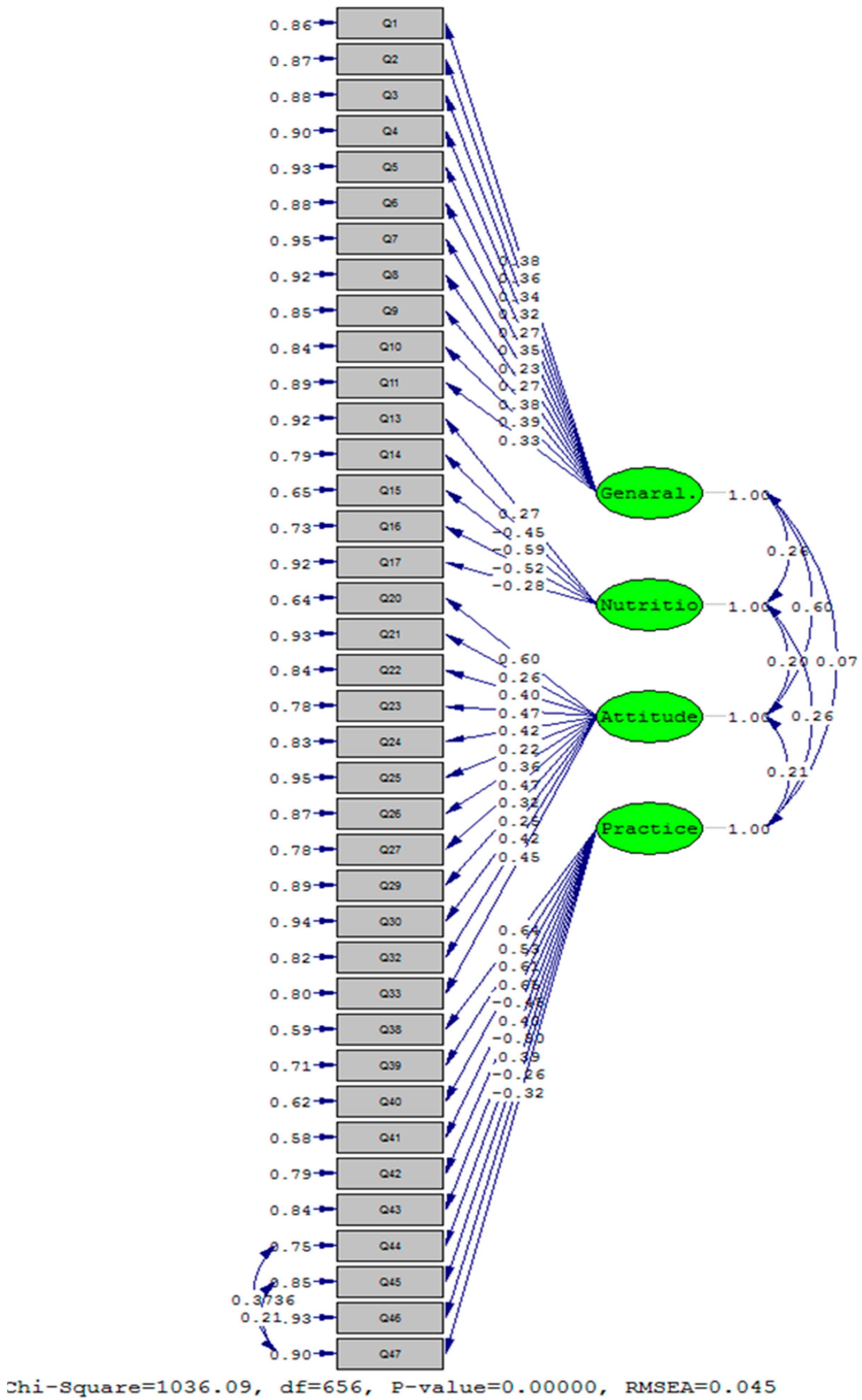
| χ2 | DF | χ2/df | RMSEA | GFI | CFI | SRMSR | NFI | IFI | |
|---|---|---|---|---|---|---|---|---|---|
| Model 1 | 1177.55 | 659 | 1.78 | 0.05 | 0.90 | 0.99 | 0.07 | 0.99 | 0.99 |
| Model 2 | 1036.10 | 656 | 1.58 | 0.05 | 0.92 | 0.99 | 0.07 | 0.99 | 0.99 |
| Constructs | n | Mean | Median | SD | Min | Max | Floor (%), Ceiling (%) | Cronbach’s α |
|---|---|---|---|---|---|---|---|---|
| General knowledge | 11 | 79.6 | 81.8 | 14.5 | 4.5 | 100.0 | 2.4, 1.2 | 0.62 |
| Nutrition knowledge | 5 | 42.6 | 40.0 | 20.4 | 0.0 | 100.0 | 8.7, 0.00 | 0.60 |
| Attitude | 12 | 75.4 | 75.0 | 9.5 | 50.9 | 100.0 | 1.1, 0.00 | 0.68 |
| Practice | 10 | 58.7 | 58.0 | 8.6 | 32.0 | 94.0 | 0.00, 0.00 | 0.74 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amiri, P.; Asghari, G.; Sadrosadat, H.; Karimi, M.; Amouzegar, A.; Mirmiran, P.; Azizi, F. Psychometric Properties of a Developed Questionnaire to Assess Knowledge, Attitude and Practice Regarding Vitamin D (D-KAP-38). Nutrients 2017, 9, 471. https://doi.org/10.3390/nu9050471
Amiri P, Asghari G, Sadrosadat H, Karimi M, Amouzegar A, Mirmiran P, Azizi F. Psychometric Properties of a Developed Questionnaire to Assess Knowledge, Attitude and Practice Regarding Vitamin D (D-KAP-38). Nutrients. 2017; 9(5):471. https://doi.org/10.3390/nu9050471
Chicago/Turabian StyleAmiri, Parisa, Golaleh Asghari, Hoda Sadrosadat, Mehrdad Karimi, Atieh Amouzegar, Parvin Mirmiran, and Fereidoun Azizi. 2017. "Psychometric Properties of a Developed Questionnaire to Assess Knowledge, Attitude and Practice Regarding Vitamin D (D-KAP-38)" Nutrients 9, no. 5: 471. https://doi.org/10.3390/nu9050471
APA StyleAmiri, P., Asghari, G., Sadrosadat, H., Karimi, M., Amouzegar, A., Mirmiran, P., & Azizi, F. (2017). Psychometric Properties of a Developed Questionnaire to Assess Knowledge, Attitude and Practice Regarding Vitamin D (D-KAP-38). Nutrients, 9(5), 471. https://doi.org/10.3390/nu9050471