1. Introduction
Bronchopulmonary dysplasia (BPD), a chronic lung disease of prematurity, is considered one of the major complications of premature birth [
1,
2,
3,
4]. The incidence of BPD is inversely proportional to gestational age, with rates reaching up to 60–90% in extremely preterm infants (22–25 weeks gestation). Infants suffering from BPD are at increased risk of death and long-term pulmonary and neurodevelopmental morbidities [
5,
6,
7].
The pathogenesis of BPD is initiated by the arrest in alveolar and lung vascular development, due to premature birth, and sustained by inflammatory events that play a paramount role in the progression of BPD [
3,
4,
8,
9]. The initiation of the inflammatory response can already occur in utero, in the setting of chorioamnionitis [
3,
4,
10,
11]. Nevertheless, postnatal stimuli, such as the ex-utero higher oxygen partial pressures, the need for oxygen administration or mechanical ventilation, and the occurrence of postnatal infections (including late onset sepsis (LOS) and necrotizing enterocolitis (NEC)), perpetuate inflammation and lead to the establishment of BPD [
12,
13,
14]. A dysregulation of the immune system, toward a sustained status of inflammation which is characteristic of very preterm infants, completes the multifactorial pathophysiological picture [
15].
Several treatments, most of which focused on anti-inflammatory or homeostasis-restoring properties, have been attempted in order to prevent or treat BPD [
16]. However, meta-analyses could confirm a reduction of BPD only for vitamin A and dexamethasone [
16,
17]. Moreover, vitamin A showed only a modest effect [
17], while the use of dexamethasone is limited in preterm infants by its well-known long- and short-term side effects [
18]. Adequate timing, dose, and formulation of steroid therapy is still under investigation in preterm infants at risk for BPD. Lately, regenerative medicine has received a great deal of attention as a promising therapeutic option for complications of prematurity, including BPD [
19,
20]. However, the knowledge of stem cell function is still incomplete, and further studies are needed to elucidate the impact of several manufacturing aspects that may determine the success or failure of this therapy [
19,
20]. In summary, despite the continuous advances in neonatal care, BPD remains a significant burden for the premature population, lacking a safe, effective and easily available treatment.
Probiotics are defined as live micro-organisms which, when administered in adequate amounts, confer a health benefit on the host [
21,
22]. Probiotic supplementation in preterm infants is one of the most studied interventions in neonatal medicine [
23,
24,
25,
26,
27,
28,
29,
30]. Many randomized controlled trials (RCTs) involving the use of probiotics have been performed in the last years. Several meta-analyses combined these RCTs and demonstrated that probiotic supplementation reduces mortality, NEC, and LOS, as well as the time to achieve full enteral feeding in preterm infants [
23,
24,
25,
26,
27,
28,
29,
30,
31]. Although until now no study has been performed to analyze the effect of probiotics on BPD as primary outcome, a number of RCTs included BPD as a secondary outcome. There are several hypothetical mechanisms by which probiotics may exert a protective effect against BPD: (1) by reducing postnatal inflammatory processes such as NEC and LOS; (2) by modulating the immune function [
32,
33]; (3) by improving the nutritional status and growth of the infants [
30,
31,
34]; and (4) through the antioxidant properties of probiotics [
35]. Therefore, in the present systematic review we aimed to collect and analyze the current evidence on the effects of probiotic supplementation on the risk of developing BPD in preterm infants.
3. Results
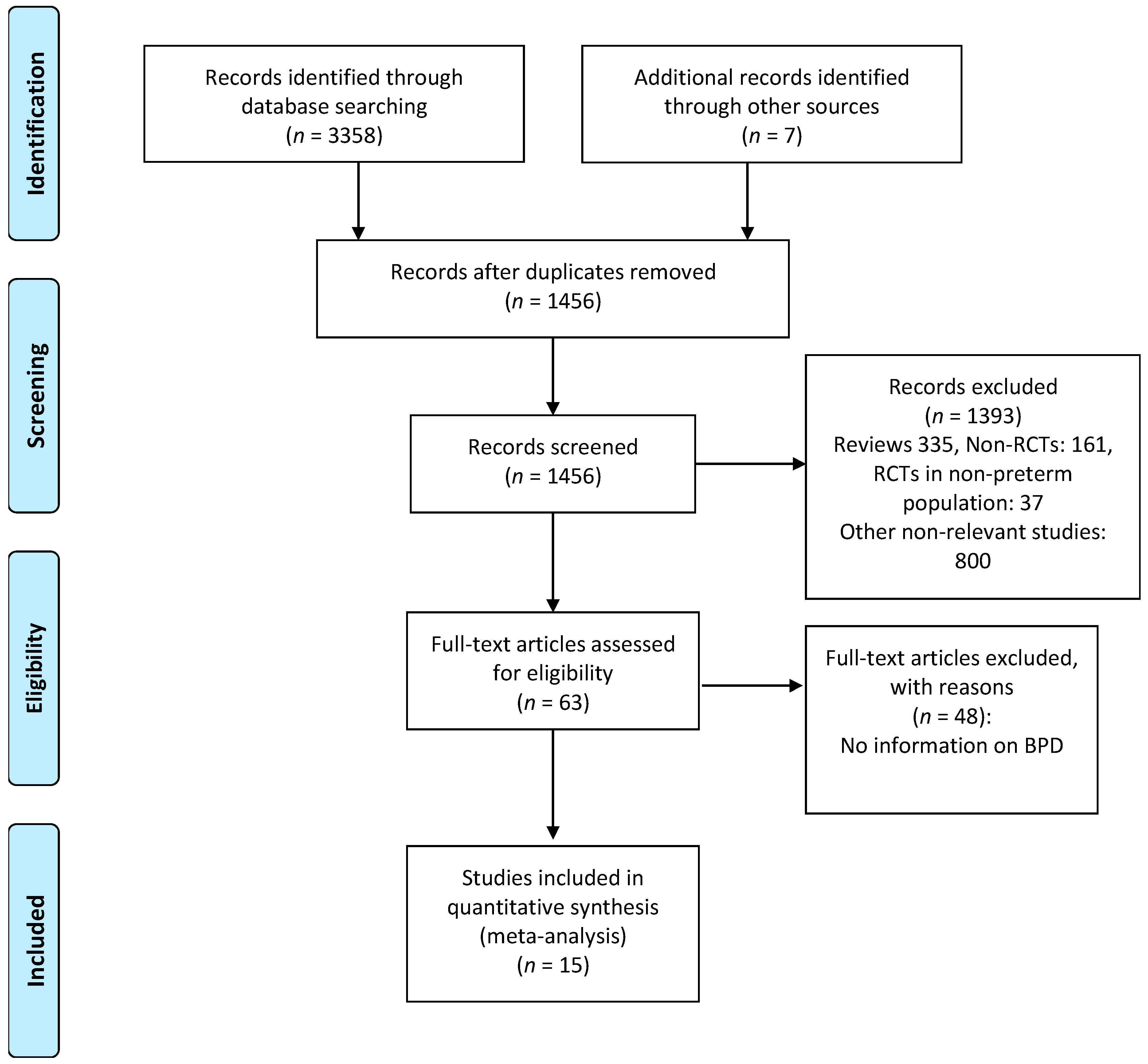
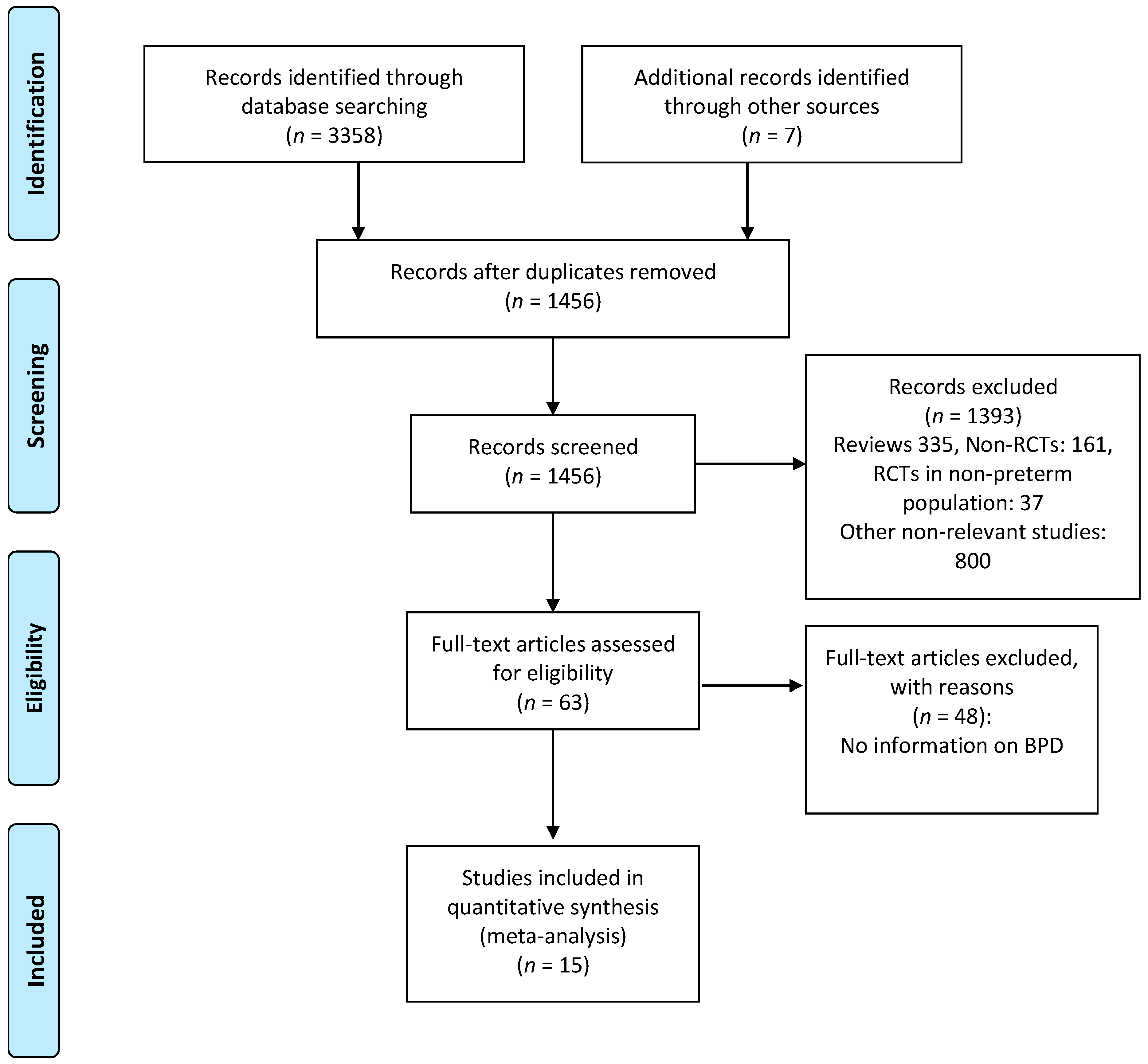
There was no substantial disagreement between reviewers on articles for inclusion, data extraction, and risk of bias assessment. Based on the titles and abstracts of 1456 citations, we identified 63 potentially relevant studies, of which 15 met the inclusion criteria [
48,
49,
50,
51,
52,
53,
54,
55,
56,
57,
58,
59,
60,
61,
62] (
Figure 1). The main characteristics of the studies are shown in
Table 1. The 15 studies included 4782 infants of which 2406 infants received probiotics. Twelve studies [
48,
49,
50,
51,
53,
54,
55,
56,
57,
58,
60,
62] included very preterm (GA < 32 weeks) and/or very low BW (VLBW) infants (<1500 g). One study [
48] included extremely low BW preterm infants (<1000 g). Two studies included larger preterm infants; one [
52] included infants with GA < 34 weeks and the other [
59] included infants with GA < 37 weeks. The included studies randomized infants to different preparations, times of initiation, and duration of therapy (
Table 1). Details of the risk of bias analysis are depicted in
Appendix A,
Table A1. None of the included studies reported serious adverse events potentially associated with the use of probiotics.
BPD was not the primary outcome in any of the included studies. Six studies [
53,
55,
58,
60,
61,
62] clearly defined BPD as BPD28 and/or BPD36, whereas nine studies did not [
48,
49,
50,
51,
52,
54,
56,
57,
59]. A clarification on BPD definition was kindly provided by the authors of eight studies [
48,
49,
50,
51,
52,
54,
56,
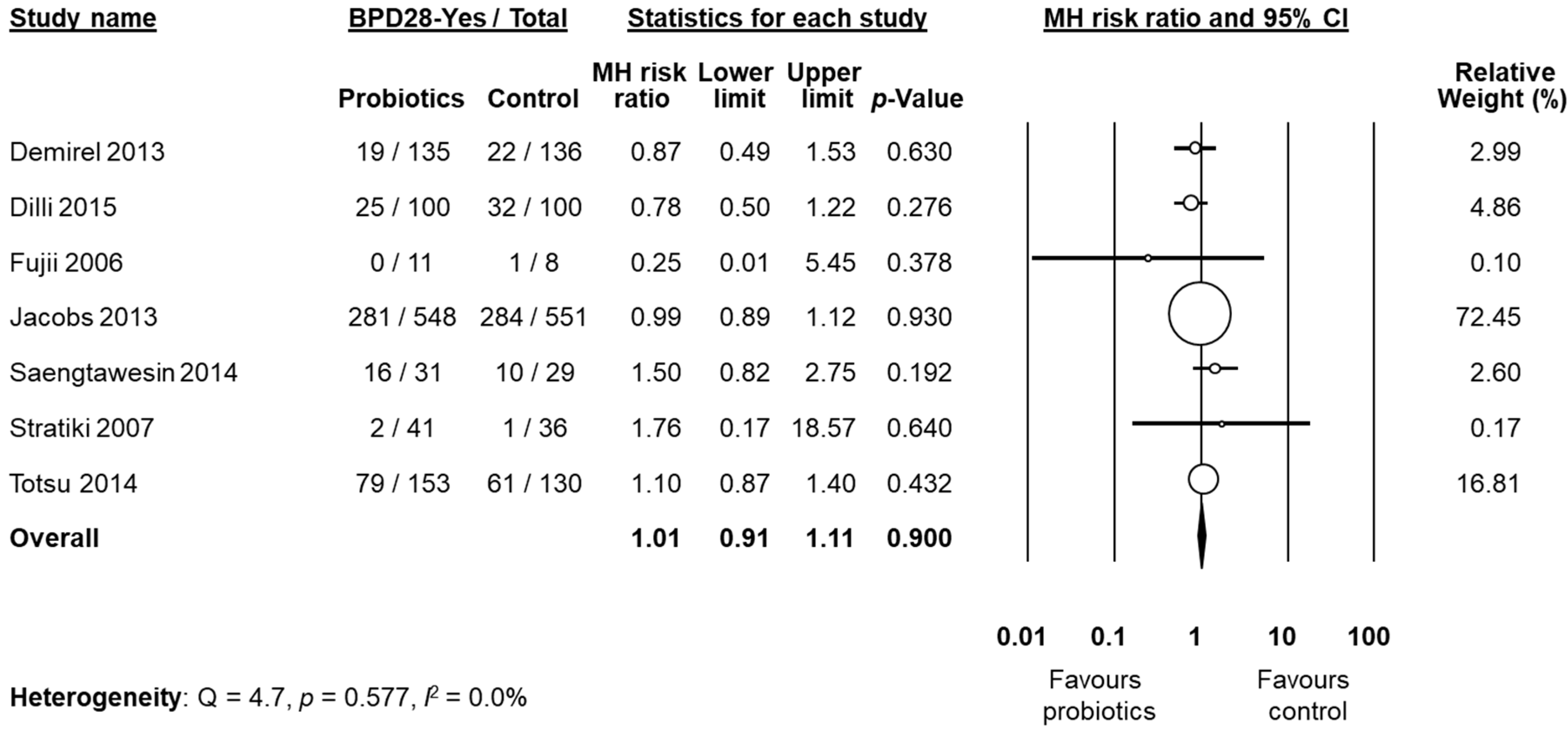
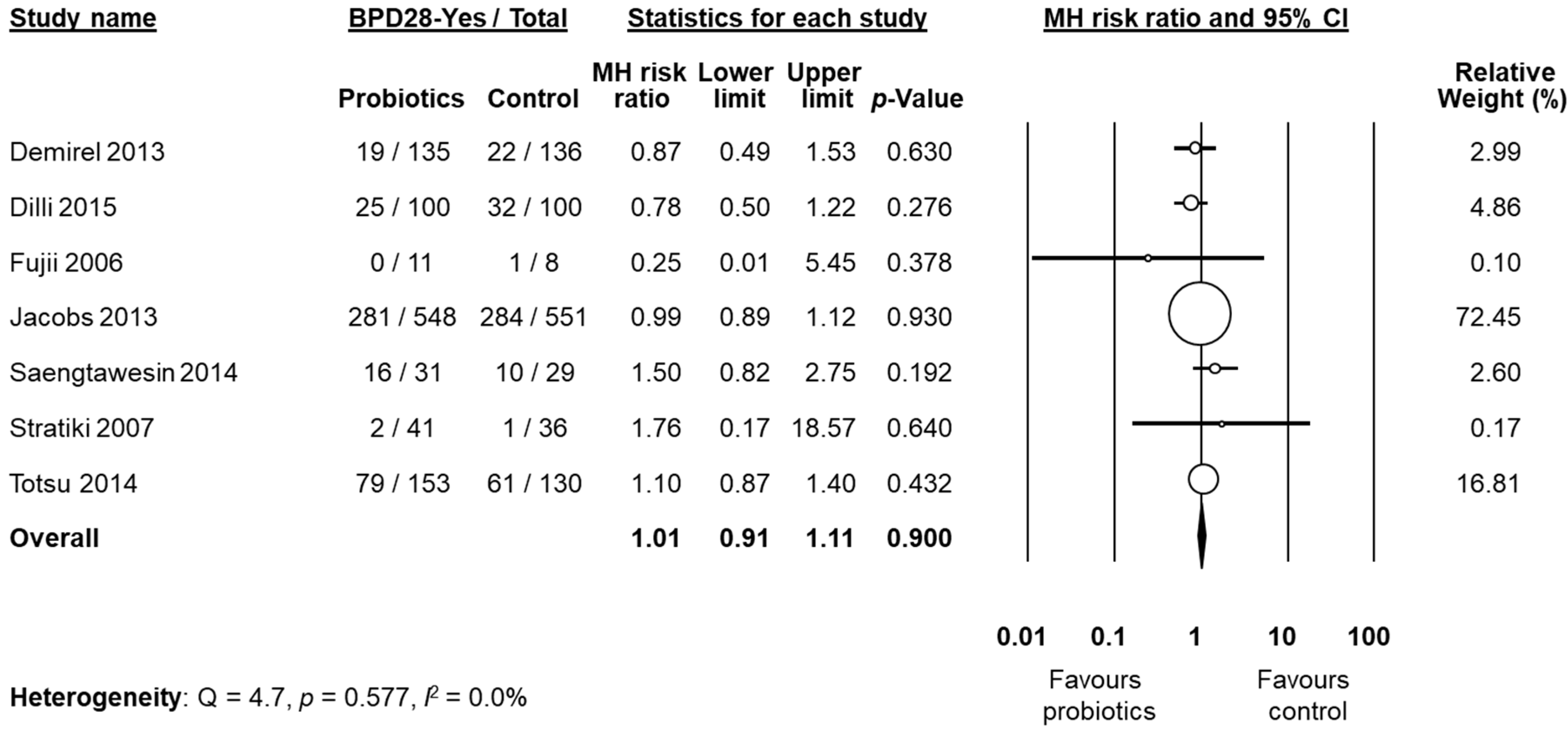
57]. After these clarifications, data on BPD28 were available from six studies [
50,
51,
52,
53,
56,
60]. We decided to pool the study of Stratiki et al. [
59] that did not specify a BPD definition, with studies reporting BPD28. Neither the individual studies nor the meta-analysis could detect a significant effect of probiotic supplementation on BPD28 (RR 1.01, 95% CI 0.91 to 1.11,
p = 0.900,
Figure 2). The use of a fixed effect model instead of a random effects model did not significantly affect the results of the meta-analysis (RR 1.00, 95% CI 0.91 to 1.10,
p = 0.999). In sensitivity analyses, excluding one study at a time, the summary RR ranged from 0.99 (95% CI 0.89–1.10,
p = 0.900), when the study of Totsu et al. [
60] was excluded, to 1.04 (95% CI 0.86–1.25,
p = 0.703), when the study of Jacobs et al. [
53] was excluded (
Appendix A,
Table A2). The study of Fujii et al. [
52] included larger infants than the other five studies (
Table 1). However, when this study was excluded, overall results were not substantially affected (RR 1.01, 95% CI 0.91–1.11,
p = 0.983). Exclusion of the study by Stratiki et al. [
59], in which BPD was not clearly defined, did not significantly affect results (RR 1.01 95% CI 0.91–1.11,
p = 0.829). Further sensitivity analysis and assessment of publication bias were not performed for BPD28 due to the low number of studies.
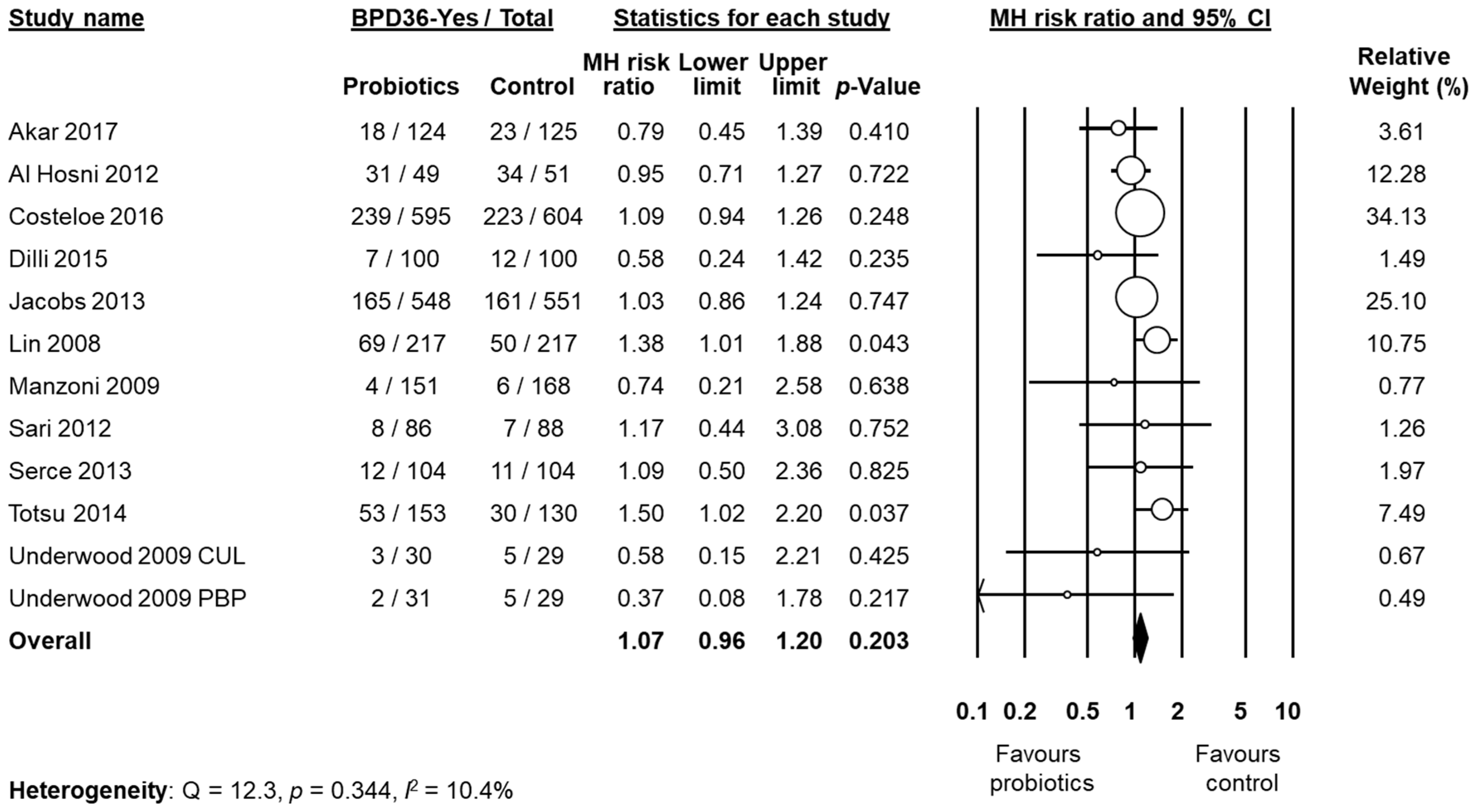
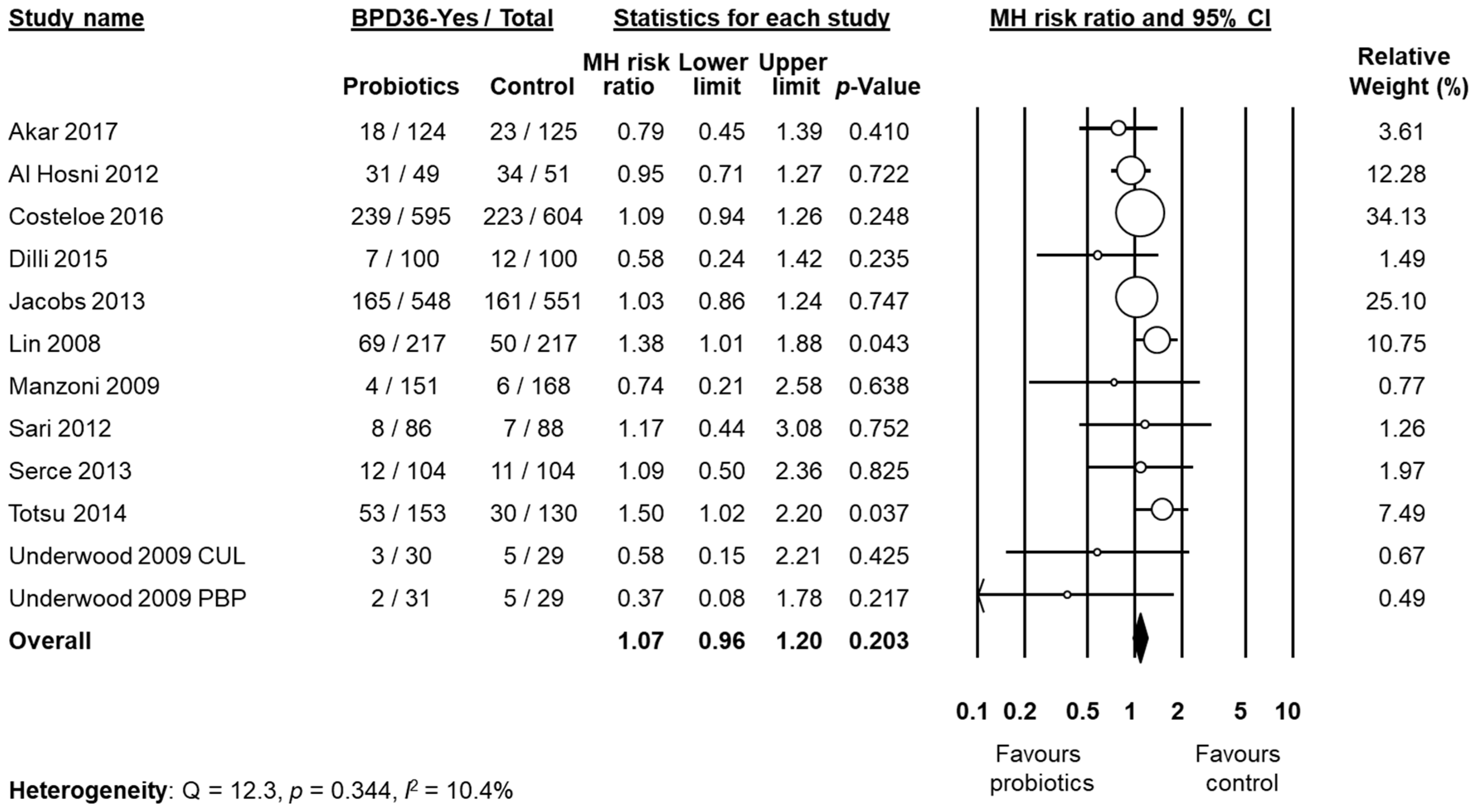
Data on BPD36 were available from 11 studies [
48,
49,
51,
53,
54,
55,
57,
58,
60,
61,
62]. The study of Underwood et al. [
61] randomized infants into three different groups: a placebo group and two treatment groups based on different probiotic preparations (
Table 1). For the purposes of this analysis, the two treatment groups of the trial of Underwood et al. [
61] were considered as two separate studies. The study of Lin et al. [
54], showed a significant increase of the BPD36 risk in the infants receiving probiotics (RR 1.38, 95% CI 1.01 to 1.88,
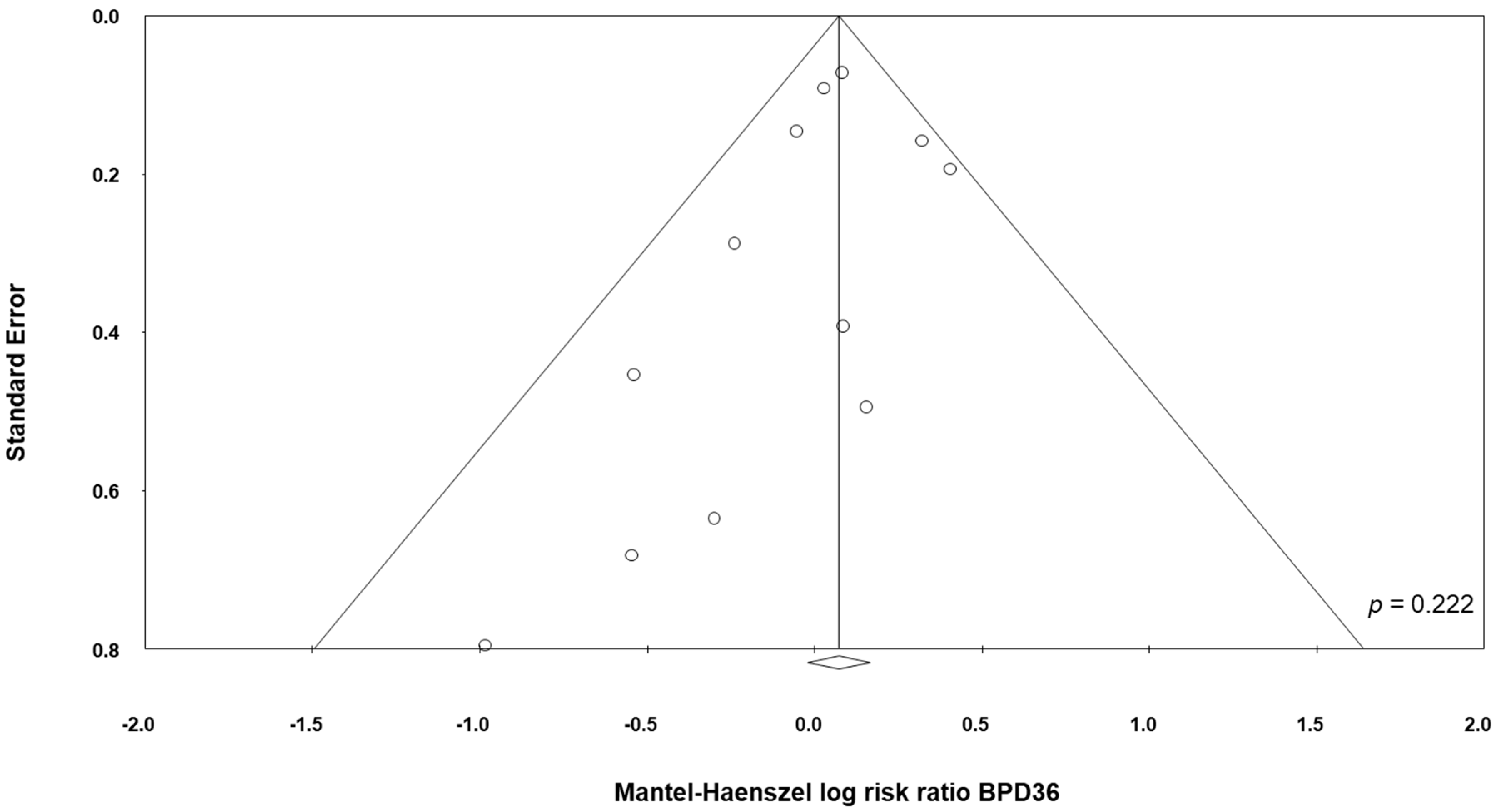
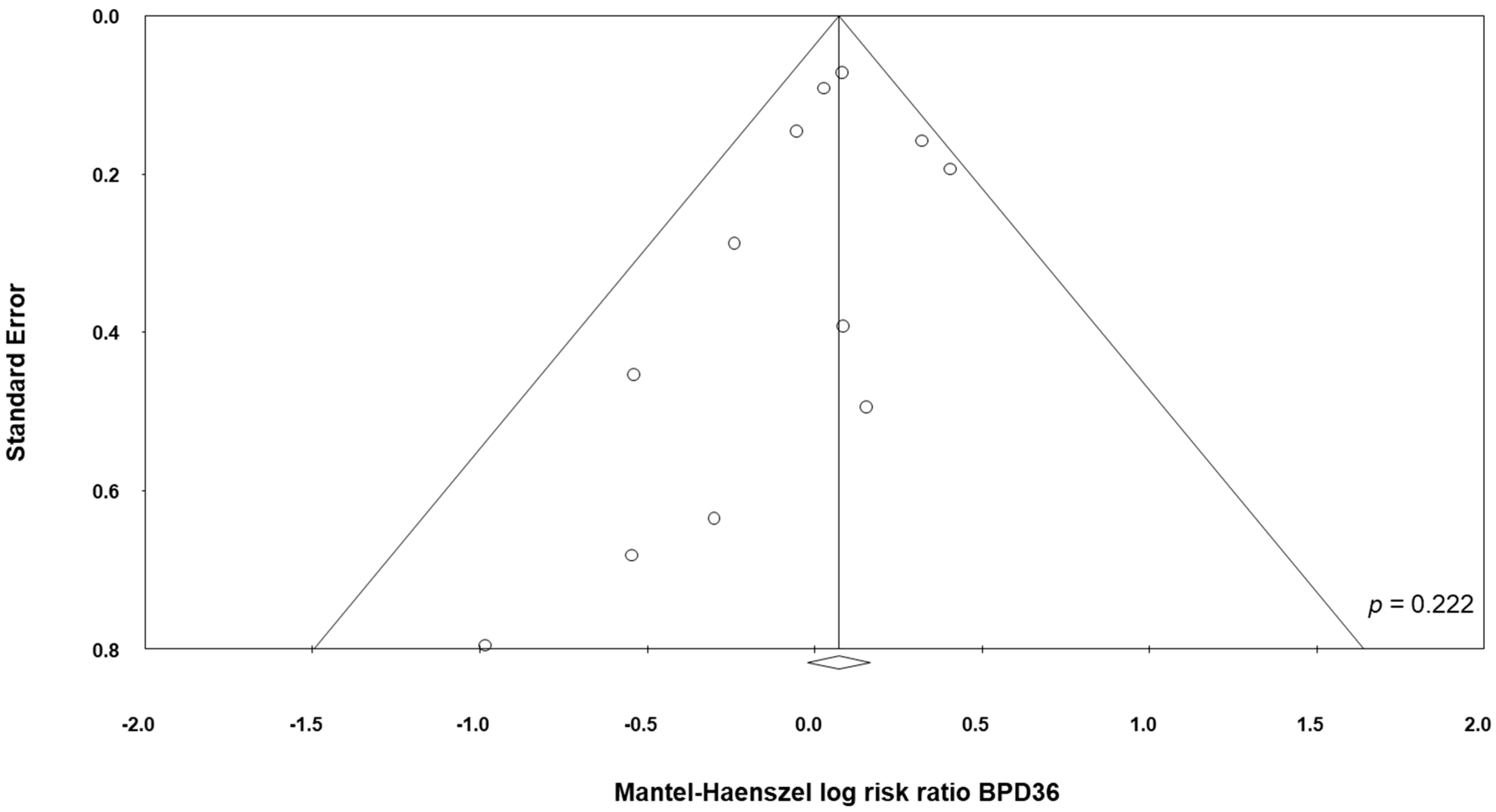
p = 0.043). In contrast, neither the other individual studies nor the meta-analysis could detect a significant effect of probiotic supplementation on BPD36 (RR 1.07, 95% CI 0.96 to 1.20,
p = 0.203,
Figure 3). Although some degree of asymmetry was observed by visual inspection of the funnel plot, Egger's test could not show any evidence of publication bias (
Figure 4). The use of a fixed effect model instead of a random effects model did not significantly affect the results of the meta-analysis (RR 1.08, 95% CI 0.98 to 1.18,
p = 0.123). In sensitivity analyses, excluding one study at a time, the summary RR ranged from 1.04 (95% CI 0.93–1.17,
p = 0.488), when the study of Lin et al. [
54] was excluded, to 1.09 (95% CI 0.97–1.23,
p = 0.138), when the study of Al Hosni et al. [
48] was excluded (
Appendix A Table A3).
One study [
62] also included, besides BPD36, the category severe BPD (defined as any baby at 36 weeks PMA still receiving mechanical ventilator support or in at least 30% oxygen or more than 0.1 L/min of low flow oxygen) (
Table 2). They report that the probiotics group did not have a significantly different risk of severe BPD compared to the control group (RR 1.21, 95% CI 0.90 to 1.62,
p = 0.200).
For the outcome BPD36, we conducted additional sensitivity analysis by excluding studies that had uncertain/high risk of bias in the different domains. In addition, we carried out subgroup analyses of studies where
Bifidobacterium was part of the supplementation, studies where
Lactobacillus was part of the supplementation, studies where multiple-strain supplements were used, studies where single-strain supplements were used, and studies where infants had a mean BW < 1250 g. No subgroup analysis could demonstrate a significant effect of probiotics on BPD36 (
Table 2).
All the included studies reported data on NEC (
Table 3) and, when pooled, we observed that probiotics significantly reduced the risk of developing NEC (RR 0.52, 95% CI 0.33–0.81,
p = 0.004,
Table 4). This significant reduction of NEC was also observed when we pooled the studies that reported BPD28 (RR 0.40, 95% CI 0.18–0.88,
p = 0.022), and when we pooled the studies that reported BPD36 (RR 0.48, 95% CI 0.29–0.81,
p = 0.006,
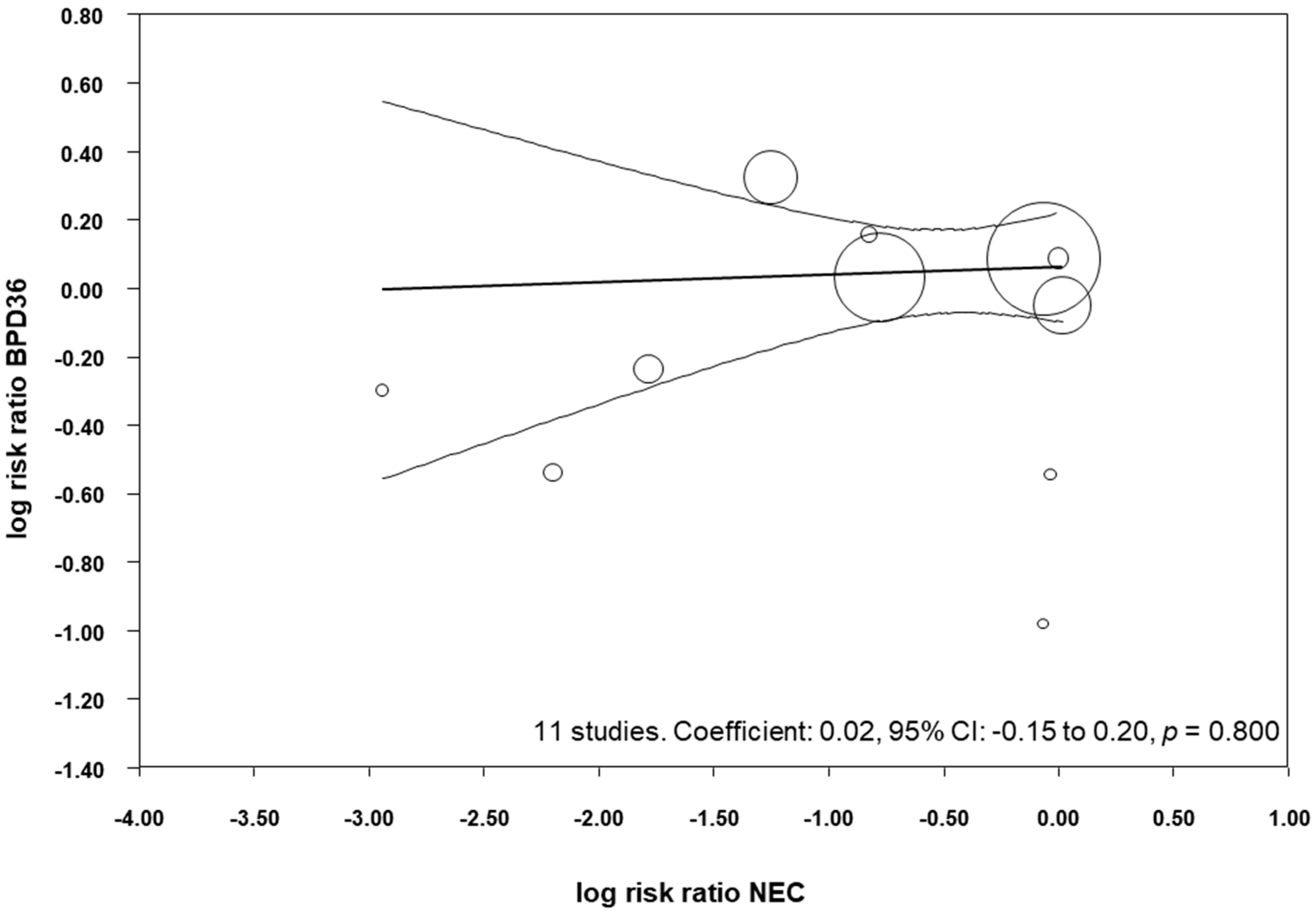
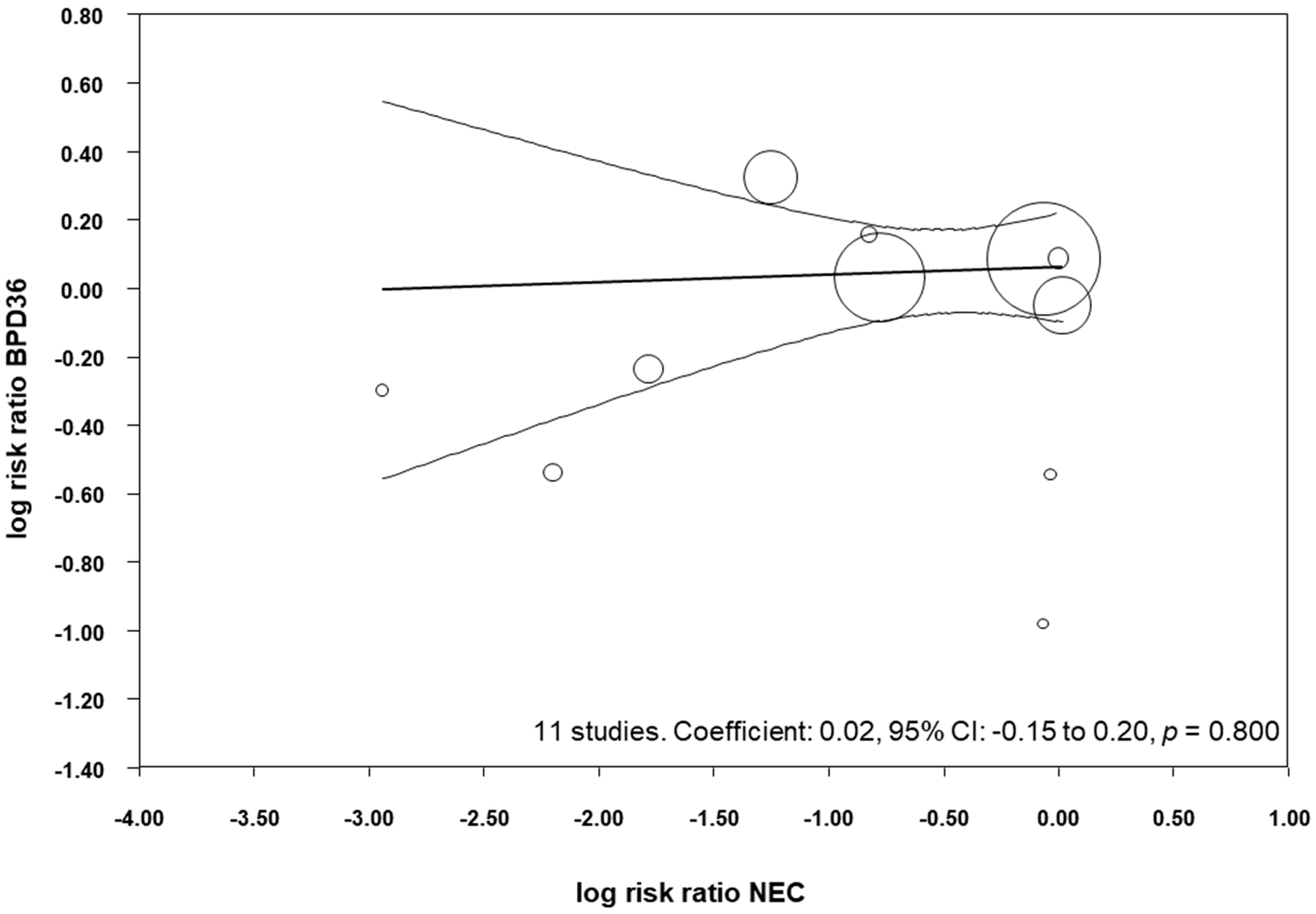
Table 4). We performed meta-regression analyses (methods of moments) to investigate the possible correlation between the effect size for NEC and the effect size for BPD. As shown in
Figure 5, meta-regression could not detect a statistically significant correlation between the reduction in NEC produced by the probiotics and the effect size for BPD36.
All the included studies reported data on LOS (
Table 3), and meta-analysis demonstrated a close to significant reduction of LOS in the probiotics group (RR 0.82, 95% CI 0.65–1.03,
p = 0.084,
Table 4). Similarly, the meta-analysis of studies that reported BPD28 found a close to significant effect of probiotics on LOS (RR 0.79, 95% CI 0.63–1.00,
p = 0.054), and the meta-analysis of studies that reported BPD36 found a close to significant reduction in LOS (RR 0.80, 95% CI 0.62–1.04,
p = 0.090,
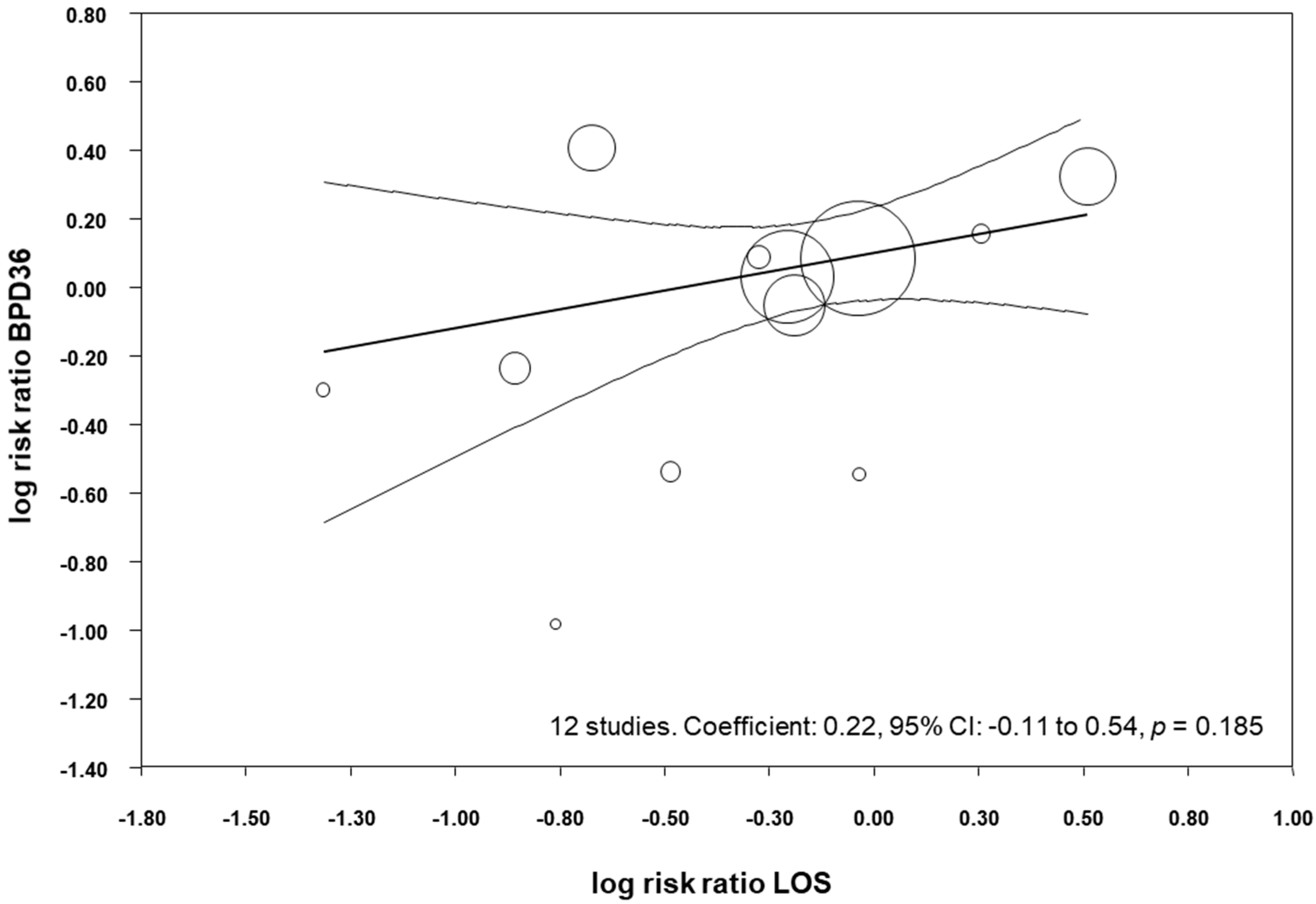
Table 4). We performed meta-regression analyses (methods of moments) to investigate the possible correlation between the effect size for LOS and the effect size for BPD36. As shown in
Figure 6, meta-regression could not detect a statistically significant correlation between the reduction in LOS produced by the probiotics and the effect size for BPD36.
All the included studies reported data on mortality (
Table 3), but meta-analysis could not demonstrate a significant reduction of mortality in the probiotics group (RR 0.80, 95% CI 0.60–1.06,
p = 0.114,
Table 4). Moreover, the meta-analysis of studies that reported BPD28 could not find a significant effect of probiotics on mortality (RR 0.78, 95% CI 0.37 to 1.66,
p = 0.518), and neither could the meta-analysis of studies that reported BPD36 (RR 0.77, 95% CI 0.56 to 1.05,
p = 0.101). We performed meta-regression analyses (methods of moments) to investigate the possible correlation between the effect size for mortality and the effect size for BPD36. This meta-regression could not detect a statistically significant correlation between the changes in mortality produced by the probiotics and the effect size for BPD36 (coefficient 0.04, 95% CI −0.13 to 0.21,
p = 0.638).
4. Discussion
Inflammatory events, such as NEC and LOS, are not only life-threatening for (very) preterm infants but also may mediate major short- and long-term adverse outcomes [
63,
64]. Current evidence indicates that probiotic supplementation significantly reduces NEC and LOS in preterm infants, but our data suggest that this decrease is not accompanied by a concomitant reduction in BPD. The present meta-analysis could not demonstrate any significant effect of probiotic supplementation on the risk of developing of BPD. Similarly, in a recent meta-analysis we found that probiotics did not significantly affect the risk of retinopathy of prematurity (ROP) [
44]. However, our results should be interpreted with caution since the included RCTs showed relevant methodological differences in terms of enrolment criteria, timing, dose, and formulation of the probiotics used. Moreover, BPD was not the primary outcome in any of the studies and the number of RCTs of probiotics reporting on BPD as secondary outcome was relatively small. In addition, none of the included studies specifically targeted the most vulnerable population for BPD (infants < 28 weeks GA).
Inflammatory processes such as NEC and LOS may increase the risk of developing BPD through direct and indirect mechanisms. Proinflammatory cytokines may exert a direct effect on lung development or sensitize the lung to the effects of oxygen, mechanical ventilation, or other stressors [
8,
9,
15,
65]. On the other hand, infants suffering from NEC and LOS often require more aggressive and prolonged mechanical ventilation, that may lead to increased lung injury [
8,
9,
15,
65]. It has been suggested that avoiding postnatal infection is more important than avoiding invasive mechanical ventilation to decrease the inflammatory response in developing lungs [
65]. Studies directed at evaluating the impact of quality improvement efforts to reduce LOS in preterm infants showed that a reduction in LOS is accompanied by decreased rates of BPD [
66,
67]. However, BPD is a multifactorial condition in which genetic predisposition, as well as prenatal and prenatal conditions all play a role [
1,
2,
3,
4]. In an interesting study, Lapcharoensap et al. showed a positive relationship between the reduction in LOS and the reduction in BPD with a coefficient of determination (
r2) of 0.08, suggesting that only the 8% of the reduction of BPD is attributable to the reduction in nosocomial infection rates [
67].
The 15 studies included in our meta-analysis represent a subset of the larger number of RCTs included in the meta-analyses on probiotics for NEC and LOS prevention. Therefore, we analysed whether the protective effects of probiotics on NEC and/or LOS were also present in the RCTs included in our study. Pooling the 15 studies showed a significant reduction of NEC (RR 0.52, 95% CI 0.33 to 0.81) and a close to significant reduction of LOS (RR 0.82 95% CI 0.65 to 1.03) in the probiotics group. We speculated that studies with higher protective effects against NEC and/or LOS would show more effect on the development of BPD. However, meta-regression did not show a significant correlation between the RR for NEC and LOS and the RR for BPD. This suggests that the reduction in postnatal inflammatory events did not translate into a reduction of BPD.
Several meta-analyses showed that probiotics reduce mortality among VLBW infants [
23,
25,
38]. It has been suggested that improved survival of VLBW infants may result in increased numbers of patients with BPD [
68]. In the group of studies included in our meta-analysis, we could not observe a significant effect of probiotics on mortality (RR 0.80, 95% CI 0.60 to 1.06). In addition, meta-regression could not show a significant correlation between the RR for mortality and the RR for BPD. Therefore, our data suggest that the effect of probiotics on mortality did not affect the rate of BPD in the RCTs. Nevertheless, a robust conclusion from meta-regression would require a larger number of included studies [
46,
47].
One important limitation inherent to any meta-analysis on BPD is the heterogeneity of the definition of the condition [
16,
69,
70]. In a systematic review which included 47 RCTs of drugs for BPD, 34% did not identify the definition of BPD that was used. Of the trials that defined BPD, 22 used oxygen dependency at 36 weeks PMA, with two trials refining that definition with a test of oxygen need [
16]. Fourteen trials provided data on oxygen requirement and four trials used both oxygen supplementation at 28 days and oxygen supplementation at 36 weeks PMA [
16]. Similarly, in our meta-analysis only six out of 15 RCTs reported a definition of BPD. Upon request, the authors of eight studies kindly clarified their definition. Even after clarification, there was marked heterogeneity in BPD definition. As pointed out by Jobe and Bancalari [
69], current definitions of BPD lack precision and do not have good predictive values for later pulmonary and neurodevelopmental outcomes. There are substantial efforts being made to develop better diagnostic criteria for BPD [
69], but it will take time before these improved definitions of BPD are reflected in RCTs and meta-analyses.
As mentioned above, the RCTs included in our analysis had important differences in the type, amount, and timing of probiotic supplementation. The choice of probiotic strain(s) is crucial and meta-analyses on probiotics have been criticized because, in most of them, probiotics administered for treatment/prevention of a specific disease or condition were all evaluated together [
26,
71,
72,
73]. It is now generally accepted that different bacterial strains of the same genus and species, verified also by genomic information, may exert completely different effects on the host [
72]. Separate meta-analyses analysing the effects of well-defined individual, single-strain or multiple-strain probiotic preparations appear to be more appropriate, but the important heterogeneity of the RCTs makes this approach very difficult [
26,
71,
72,
73]. We attempted to explore whether the studies using
Lactobacillus or
Bifidobacterium species showed a different effect on BPD. We also performed a separate analysis for multi-strain probiotics because recent meta-analyses suggest that the use of more than one strain has a stronger effect in the prevention of NEC [
74]. None of these subgroup analyses suggested a significant preventive effect of probiotics on BPD. However, the number of studies included in the subgroup analysis was low, making the results inconclusive.
Besides their effect on NEC and LOS prevention, there are some other mechanisms of action ascribed to probiotics which may directly counteract the disruption of lung development prompting to BPD [
26,
75]. In the first place, the immature immune system of premature infants is unable to balance pro-inflammatory responses, leading to a sustained status of inflammation that contributes significantly to several neonatal diseases, including BPD [
15]. A decreased number of T regulatory cells (Tregs), which constitute the anti-inflammatory lymphocytic subset, and higher proportions of activated pro-inflammatory T cells have been related with the development of BPD [
76,
77]. Probiotics seem to have a role in improving Treg generation, expansion and activity, while decreasing activation/proliferation of the pro-inflammatory lymphocytic subsets. These effects may result in the recovery of the immune homeostasis with polarization of the immune system toward an anti-inflammatory phenotype [
78,
79]. Secondly, it has been suggested that each additional day of antibiotic therapy in the first 2 weeks of life in VLBW infants may be associated with an increased BPD rate and severity [
80]. This could be explained by the antibiotic-induced decrease in diversity of lung microbiota which has been linked to BPD development [
81]. Probiotics are known to restore intestinal microbiota after antibiotic therapy [
82] and to produce a strong suppressive effect on airway inflammation [
83]. Lastly, poor nutrition is associated with lung underdevelopment and the occurrence of BPD [
84]. In experimental NEC, probiotic supplementation reversed the detrimental effects of combined hyperoxia and suboptimal nutrition on lung vascular endothelial growth factor (VEGF) levels, suggesting that this strategy may help improve lung vasculogenesis [
85].
In conclusion, our study could not demonstrate any significant effect of probiotic supplementation on the risk of developing of BPD. Given the remarkable theoretical benefits of probiotics supplementation in ameliorating several aspects of BPD pathogenesis and the limitations of the analysis, our data should be seen as a starting point rather than definitive results. The main merit of our study was to collect, for the first time, the available data on the role of probiotic supplementation in the prevention of BPD, and to revise the possible specific mechanisms of action. Nevertheless, further experimental and clinical data are needed to draw more solid conclusions. Particularly, more studies designed to select the optimal probiotic preparation, dosing, and duration of therapy are still needed [
29]. These studies should compare probiotic strains that have been reported to be safe and effective in previous trials [
73] and include outcomes, such as BPD, which can be indirectly affected by the changes in immunity and nutritional status induced by probiotic supplementation.

 ,
, 


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}