Sugar- and Intense-Sweetened Drinks in Australia: A Systematic Review on Cardiometabolic Risk

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
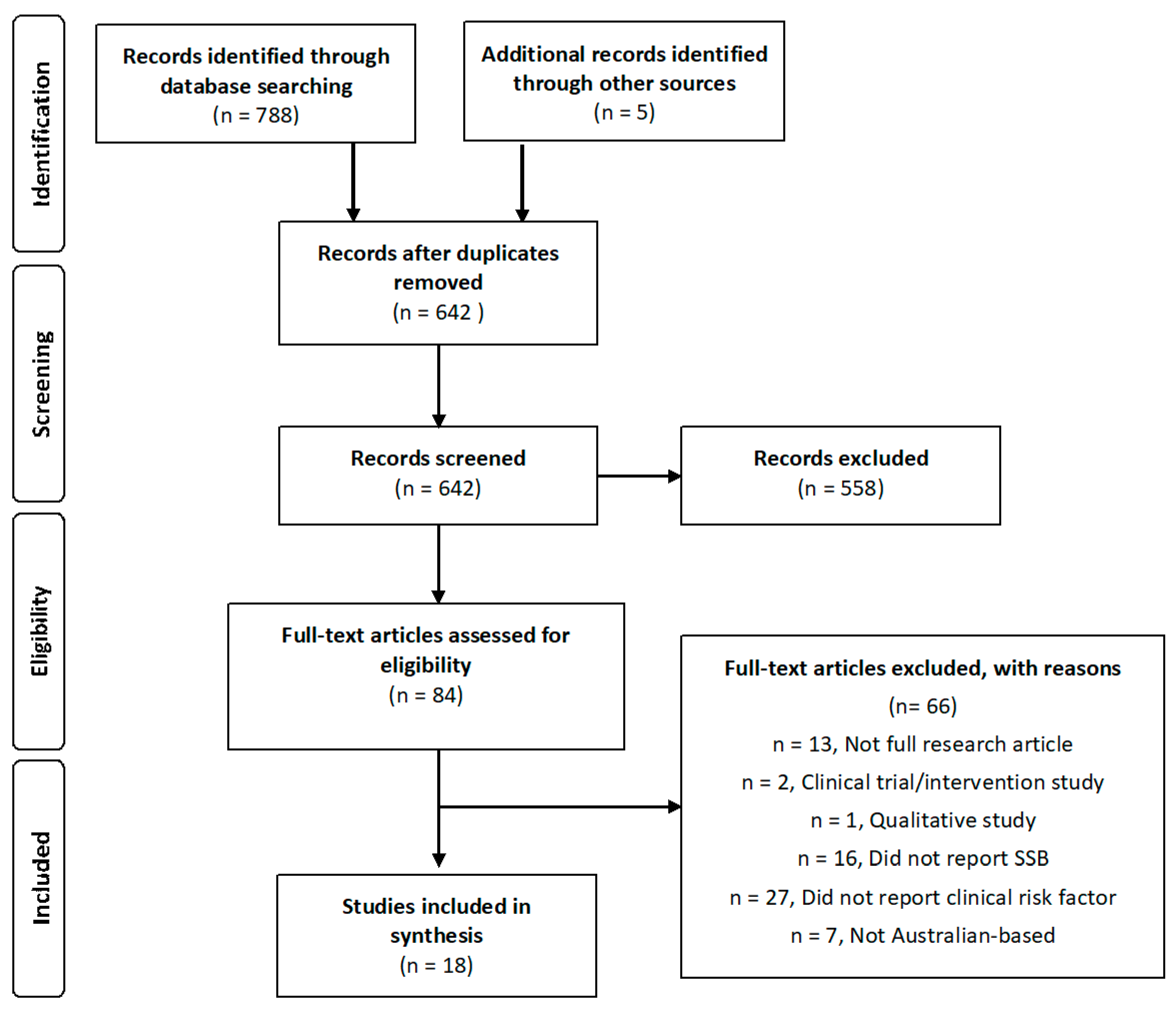
2.2. Search Strategy and Study Selection
2.3. Data Extraction
3. Results
3.1. Search Results
3.2. Outcomes
3.2.1. Adiposity-Related Risk Factors
3.2.2. Blood Pressure
3.2.3. Other Cardiovascular and Metabolic Risk Factors
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Marriott, B.P.; Olsho, L.; Hadden, L.; Connor, P. Intake of added sugars and selected nutrients in the United States, National Health and Nutrition Examination Survey (NHANES) 2003–2006. Crit. Rev. Food Sci. Nutr. 2010, 50, 228–258. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef] [PubMed]
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am. J. Public Health 2007, 97, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Australian Government. Australian New Zealand Food Standards Code—Standard 1.3.1—Food Additives; Legislation, F.R., Ed.; Australian Government: Canberra, Australia, 2016.
- Brand-Miller, J.C.; Barclay, A.W. Declining consumption of added sugars and sugar-sweetened beverages in Australia: A challenge for obesity prevention. Am. J. Clin. Nutr. 2017, 105, 854–863. [Google Scholar] [CrossRef] [PubMed]
- Forshee, R.A.; Anderson, P.A.; Storey, M.L. Sugar-sweetened beverages and body mass index in children and adolescents: A meta-analysis. Am. J. Clin. Nutr. 2008, 87, 1662–1671. [Google Scholar] [PubMed]
- Gibson, S. Sugar-sweetened soft drinks and obesity: A systematic review of the evidence from observational studies and interventions. Nutr. Res. Rev. 2008, 21, 134–147. [Google Scholar] [CrossRef] [PubMed]
- Imamura, F.; O’Connor, L.; Ye, Z.; Mursu, J.; Hayashino, Y.; Bhupathiraju, S.N.; Forouhi, N.G. Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit juice and incidence of type 2 diabetes: Systematic review, meta-analysis, and estimation of population attributable fraction. BMJ 2015. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Després, J.-P.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes a meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, D.; Threapleton, D.; Evans, C.; Cleghorn, C.; Nykjaer, C.; Woodhead, C.; Burley, V. Association between sugar-sweetened and artificially sweetened soft drinks and type 2 diabetes: Systematic review and dose-response meta-analysis of prospective studies. Br. J. Nutr. 2014, 112, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Yu, M.; Fang, L.; Hu, R.Y. Association between sugar-sweetened beverages and type 2 diabetes: A meta-analysis. J. Diabetes Investig. 2015, 6, 360–366. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.M.; Hawkes, C. Sweetening of the global diet, particularly beverages: Patterns, trends, and policy responses. Lancet Diabetes Endocrinol. 2016, 4, 174–186. [Google Scholar] [CrossRef]
- Pollard, C.M.; Meng, X.; Hendrie, G.A.; Hendrie, D.; Sullivan, D.; Pratt, I.S.; Kerr, D.A.; Scott, J.A. Obesity, socio-demographic and attitudinal factors associated with sugar-sweetened beverage consumption: Australian evidence. Aust. N. Z. J. Public Health 2016, 40, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Millar, L.; Rowland, B.; Nichols, M.; Swinburn, B.; Bennett, C.; Skouteris, H.; Allender, S. Relationship between raised BMI and sugar sweetened beverage and high fat food consumption among children. Obesity 2014, 22, E96–E103. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, G.L.; Oddy, W.H.; Huang, R.C.; Mori, T.A.; Beilin, L.J.; Jebb, S.A. Prospective associations between sugar-sweetened beverage intakes and cardiometabolic risk factors in adolescents. Am. J. Clin. Nutr. 2013, 98, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Talley, N.J. National health summit on obesity calls for Australia to take action to stem the pandemic. Med. J. Aust. 2017, 206, 106–107. [Google Scholar] [CrossRef] [PubMed]
- Avogaro, A. Postprandial glucose: Marker or risk factor? Diabetes Care 2011, 34, 2333–2335. [Google Scholar] [CrossRef] [PubMed]
- Jameel, F.; Phang, M.; Wood, L.G.; Garg, M.L. Acute effects of feeding fructose, glucose and sucrose on blood lipid levels and systemic inflammation. Lipids Health Dis. 2014, 13, 195. [Google Scholar] [CrossRef] [PubMed]
- Barr, E.L.; Zimmet, P.Z.; Welborn, T.A.; Jolley, D.; Magliano, D.J.; Dunstan, D.W.; Cameron, A.J.; Dwyer, T.; Taylor, H.R.; Tonkin, A.M. Risk of cardiovascular and all-cause mortality in individuals with diabetes mellitus, impaired fasting glucose, and impaired glucose tolerance the Australian diabetes, obesity, and lifestyle study (AusDiab). Circulation 2007, 116, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Varsamis, P.; Larsen, R.N.; Dunstan, D.W.; Jennings, G.L.; Owen, N.; Kingwell, B.A. The sugar content of soft drinks in Australia, Europe and the United States. Med. J. Aust. 2017, 206, 454–455. [Google Scholar] [CrossRef] [PubMed]
- Bantle, J.P.; Raatz, S.K.; Thomas, W.; Georgopoulos, A. Effects of dietary fructose on plasma lipids in healthy subjects. Am. J. Clin. Nutr. 2000, 72, 1128–1134. [Google Scholar] [PubMed]
- Basciano, H.; Federico, L.; Adeli, K. Fructose, insulin resistance, and metabolic dyslipidemia. Nutr. Metab. 2005, 2, 5. [Google Scholar] [CrossRef] [PubMed]
- Chong, M.F.; Fielding, B.A.; Frayn, K.N. Mechanisms for the acute effect of fructose on postprandial lipemia. Am. J. Clin. Nutr. 2007, 85, 1511–1520. [Google Scholar] [PubMed]
- Australian Bureau of Statistics. Australian Health Survey 2011–2012; Australian Bureau of Statistics: Canberra, Australia, 2012.
- Hafekost, K.; Mitrou, F.; Lawrence, D.; Zubrick, S.R. Sugar sweetened beverage consumption by Australian children: Implications for public health strategy. BMC Public Health 2011, 11, 950. [Google Scholar] [CrossRef] [PubMed]
- French, S.; Rosenberg, M.; Wood, L.; Maitland, C.; Shilton, T.; Pratt, I.S.; Buzzacott, P. Soft drink consumption patterns among western Australians. J. Nutr. Educ. Behav. 2013, 45, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Health Survey: Nutrition First Results—Foods and Nutrients, 2011–2012; Australian Bureau of Statistics: Canberra, Australia, 2014.
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef] [PubMed]
- Thurber, K.A.; Dobbins, T.; Neeman, T.; Banwell, C.; Banks, E. Body mass index trajectories of Indigenous Australian children and relation to screen time, diet, and demographic factors. Obesity 2017, 25, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Clifton, P.M.; Chan, L.; Moss, C.L.; Miller, M.D.; Cobiac, L. Beverage intake and obesity in Australian children. Nutr. Metab. 2011, 8, 87. [Google Scholar] [CrossRef] [PubMed]
- Grimes, C.A.; Riddel, L.J.; Campbell, K.J.; Nowson, C.A. Dietary Salt Intake, sugar-sweetened beverage consumption, and obesity risk. Pediatrics 2013, 131, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Hardy, L.L.; Grunseit, A.; Khambalia, A.; Bell, C.; Wolfenden, L.; Milat, A.J. Co-occurrence of obesogenic risk factors among adolescents. J. Adolesc. Health 2012, 51, 265–271. [Google Scholar] [CrossRef] [PubMed]
- Jensen, B.W.; Nichols, M.; Allender, S.; de Silva-Sanigorski, A.; Millar, L.; Kremer, P.; Lacy, K.; Swinburn, B. Inconsistent associations between sweet drink intake and 2-year change in BMI among Victorian children and adolescents. Pediatr. Obes. 2013, 8, 271–283. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.; Barclay, A.W.; Brand-Miller, J.C.; Louie, J.C.Y. Dietary glycaemic index and glycaemic load among Australian children and adolescents: Results from the 2011–2012 Australian Health Survey. Br. J. Nutr. 2016, 116, 178–187. [Google Scholar] [CrossRef] [PubMed]
- Sanigorski, A.M.; Bell, A.C.; Swinburn, B.A. Association of key foods and beverages with obesity in Australian schoolchildren. Public Health Nutr. 2007, 10, 152–157. [Google Scholar] [CrossRef] [PubMed]
- Zheng, M.; Allman-Farinelli, M.; Heitmann, B.L.; Toelle, B.; Marks, G.; Cowell, C.; Rangan, A. Liquid versus solid energy intake in relation to body composition among Australian children. J. Hum. Nutr. Diet. 2015, 28, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Sluyter, J.D.; Scragg, R.K.R.; Plank, L.D.; Waqa, G.D.; Fotu, K.F.; Swinburn, B.A. Sizing the association between lifestyle behaviours and fatness in a large, heterogeneous sample of youth of multiple ethnicities from 4 countries. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 115–139. [Google Scholar] [CrossRef] [PubMed]
- Wheaton, N.; Millar, L.; Allender, S.; Nichols, M. The stability of weight status through the early to middle childhood years in Australia: A longitudinal study. BMJ Open 2015, 5, e006963. [Google Scholar] [CrossRef] [PubMed]
- Trapp, G.S.A.; Allen, K.L.; O’Sullivan, T.; Robinson, M.; Jacoby, P.; Oddy, W.H. Energy drink consumption among young Australian adults: Associations with alcohol and illicit drug use. Drug Alcohol Depend. 2014, 134, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Pase, M.P.; Grima, N.; Cockerell, R.; Pipingas, A. Habitual intake of fruit juice predicts central blood pressure. Appetite 2015, 84, 68–72. [Google Scholar] [CrossRef] [PubMed]
- Gearon, E.; Backholer, K.; Hodge, A.; Peeters, A. The mediating role of dietary factors and leisure time physical activity on socioeconomic inequalities in body mass index among Australian adults. BMC Public Health 2013, 13, 1214. [Google Scholar] [CrossRef] [PubMed]
- Cleland, V.J.; Schmidt, M.D.; Dwyer, T.; Venn, A.J. Television viewing and abdominal obesity in young adults: Is the association mediated by food and beverage consumption during viewing time or reduced leisure-time physical activity? Am. J. Clin. Nutr. 2008, 87, 1148–1155. [Google Scholar] [PubMed]
- Frary, C.D.; Johnson, R.K.; Wang, M.Q. Children and adolescents’ choices of foods and beverages high in added sugars are associated with intakes of key nutrients and food groups. J. Adolesc. Health 2004, 34, 56–63. [Google Scholar] [CrossRef]
- Arsenault, B.J.; Lamarche, B.; Després, J.-P. Targeting Overconsumption of sugar-sweetened beverages vs. overall poor diet quality for cardiometabolic diseases risk prevention: Place your bets! Nutrients 2017, 9, 600. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Powell, L.M. Consumption patterns of sugar-sweetened beverages in the United States. J. Acad. Nutr. Diet. 2013, 113, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Hulsegge, G.; Spijkerman, A.M.; van der Schouw, Y.T.; Bakker, S.J.; Gansevoort, R.T.; Smit, H.A.; Verschuren, W.M. Trajectories of metabolic risk factors and biochemical markers prior to the onset of cardiovascular disease—The doetinchem cohort study. PLoS ONE 2016, 11, e0155978. [Google Scholar] [CrossRef] [PubMed]
- Varsamis, P.; Larsen, R.N.; Owen, N.; Dunstan, D.W.; Jennings, G.L.; Kingwell, B.A. A comparison of the composition of sugars in popular soft drinks in Australia, Europe and the USA. J. Nutr. Intermed. Metab. 2017, 8, 104. [Google Scholar] [CrossRef]
- Dobbins, M.; Husson, H.; DeCorby, K.; LaRocca, R.L. School-based physical activity programs for promoting physical activity and fitness in children and adolescents aged 6 to 18. Cochrane Database Syst. Rev. 2013, 2. [Google Scholar] [CrossRef]
- Australian Beverage Council. The Role of Beverages in the Australian Diet; Australian Beverage Council: Waterloo, Australia, 2015. [Google Scholar]
- Brown, R.J.; De Banate, M.A.; Rother, K.I. Artificial sweeteners: A systematic review of metabolic effects in youth. Int. J. Pediatr. Obes. 2010, 5, 305–312. [Google Scholar] [CrossRef] [PubMed]
- Suez, J.; Korem, T.; Zeevi, D.; Zilberman-Schapira, G.; Thaiss, C.A.; Maza, O.; Israeli, D.; Zmora, N.; Gilad, S.; Weinberger, A. Artificial sweeteners induce glucose intolerance by altering the gut microbiota. Nature 2014, 514, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Fox, C.S.; Jacques, P.F.; Speliotes, E.K.; Hoffmann, U.; Smith, C.E.; Saltzman, E.; McKeown, N.M. Sugar-sweetened beverage, diet soda, and fatty liver disease in the framingham heart study cohorts. J. Hepatol. 2015, 63, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Abdelmalek, M.F.; Day, C. Sugar sweetened beverages and fatty liver disease: Rising concern and call to action. J. Hepatol. 2015, 63, 306–308. [Google Scholar] [CrossRef] [PubMed]
- International Business Times. To Lower Australia’s Rising Obesity Rates, Tax Soft Drinks; International Business Times: Sydney, Australia, 2011. [Google Scholar]
- Roberto, C.A.; Swinburn, B.; Hawkes, C.; Huang, T.T.; Costa, S.A.; Ashe, M.; Zwicker, L.; Cawley, J.H.; Brownell, K.D. Patchy progress on obesity prevention: Emerging examples, entrenched barriers, and new thinking. Lancet 2015, 385, 2400–2409. [Google Scholar] [CrossRef]
- Marwick, T. The campaign against Heart Disease Must Keep Ticking. Available online: https://myaccount.news.com.au/theaustralian/subscribe?pkgDef=TA_SDO_P0415A_W04&directSubscribe=true&b=true&sourceCode=TAWEB_WRE170_a&mode=premium&dest=http://www.theaustralian.com.au/opinion/the-campaign-against-heart-disease-must-keep-ticking/news-story/6409de46044b887558d73621b9d6d067&memtype=anonymous (accessed on 27 September 2017).
- Shim, J.-S.; Oh, K.; Kim, H.C. Dietary assessment methods in epidemiologic studies. Epidemiol. Health 2014, 36, e2014009. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Study (Author/Year) | n | BMI/Overweight/Obesity | Waist Circumference | T2DM | Blood Pressure | Insulin Resistance | Glucose | Glycaemic Index | Triglycerides | Cholesterol | Metabolic Syndrome | Controlled for Physical Activity | Controlled for Diet | Other | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Obj | Sub | ||||||||||||||
| Ambrosini et al. (2013) [15] | 1433 | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ | √ 1 | |||
| Cleland et al. (2008) [42] | 2001 | √ | √ 2 | ||||||||||||
| Clifton et al. (2011) [30] | 4400 | √ | |||||||||||||
| French et al. (2013) [26] | 1015 | √ | |||||||||||||
| Gearon et al. (2013) [41] | 30,630 | √ | √ 3 | ||||||||||||
| Grimes et al. (2013) [31] | 4283 | √ | √ | √ | √ 4 | ||||||||||
| Hardy et al. (2012) [32] | 1568 | √ | |||||||||||||
| Jensen et al. (2013) [33] | 1465 | √ | √ 5 | ||||||||||||
| Jones et al. (2016) [34] | 1876 | √ | |||||||||||||
| Millar et al. (2014) [14] | 4164 | √ | |||||||||||||
| Pase et al. (2015) [40] | 160 | √ | √ 6 | ||||||||||||
| Pollard et al. (2016) [13] | 13,596 | √ | |||||||||||||
| Sanigorski et al. (2007) [35] | 1944 | √ | |||||||||||||
| Sluyter et al. (2013) [37] | 1673 | √ | √ 7 | ||||||||||||
| Trapp et al. (2014) [39] | 1234 | √ | |||||||||||||
| Thurber et al. (2017) [29] | 887 | √ | |||||||||||||
| Wheaton et al. (2015) [38] | 4169 | √ | √ 8 | ||||||||||||
| Zheng et al. (2015) [36] | 158 | √ | √ | √ 9 | |||||||||||
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hoare, E.; Varsamis, P.; Owen, N.; Dunstan, D.W.; Jennings, G.L.; Kingwell, B.A. Sugar- and Intense-Sweetened Drinks in Australia: A Systematic Review on Cardiometabolic Risk. Nutrients 2017, 9, 1075. https://doi.org/10.3390/nu9101075
Hoare E, Varsamis P, Owen N, Dunstan DW, Jennings GL, Kingwell BA. Sugar- and Intense-Sweetened Drinks in Australia: A Systematic Review on Cardiometabolic Risk. Nutrients. 2017; 9(10):1075. https://doi.org/10.3390/nu9101075
Chicago/Turabian StyleHoare, Erin, Pia Varsamis, Neville Owen, David W. Dunstan, Garry L. Jennings, and Bronwyn A. Kingwell. 2017. "Sugar- and Intense-Sweetened Drinks in Australia: A Systematic Review on Cardiometabolic Risk" Nutrients 9, no. 10: 1075. https://doi.org/10.3390/nu9101075
APA StyleHoare, E., Varsamis, P., Owen, N., Dunstan, D. W., Jennings, G. L., & Kingwell, B. A. (2017). Sugar- and Intense-Sweetened Drinks in Australia: A Systematic Review on Cardiometabolic Risk. Nutrients, 9(10), 1075. https://doi.org/10.3390/nu9101075