Reaching Low-Income Mothers to Improve Family Fruit and Vegetable Intake: Food Hero Social Marketing Campaign—Research Steps, Development and Testing


Abstract
:1. Introduction
2. Materials and Methods
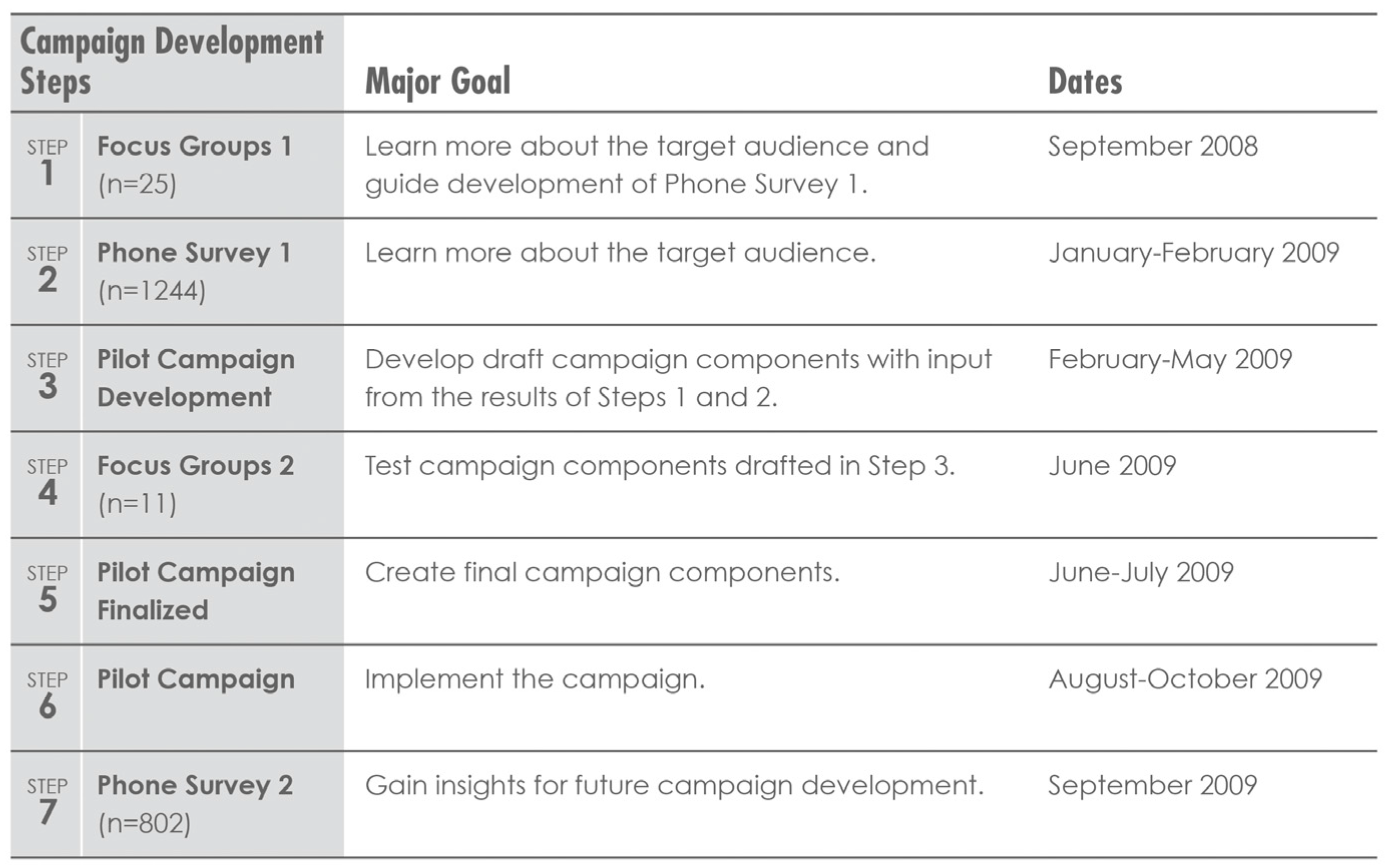
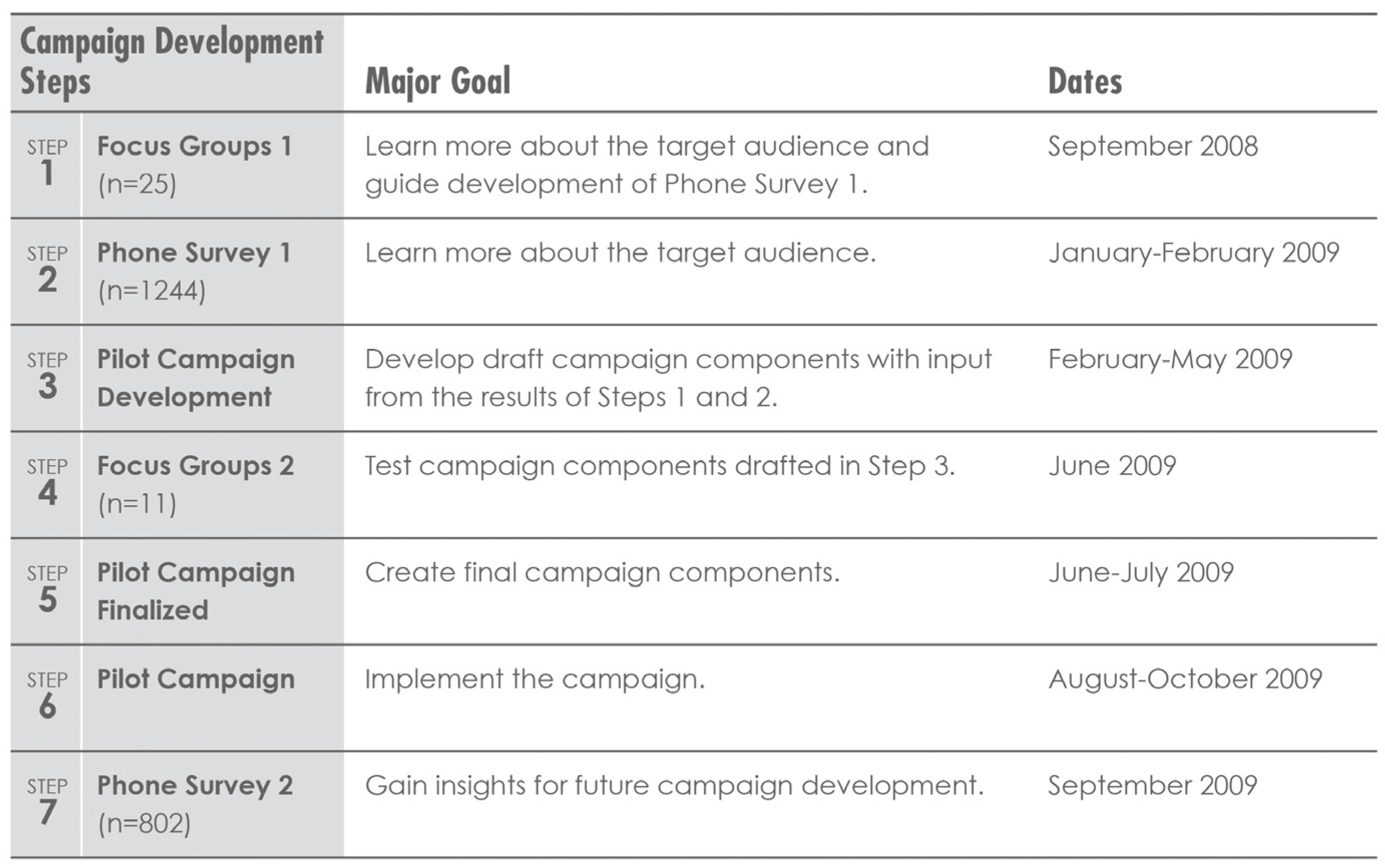
2.1. Study Overview
2.2. Study Design
2.3. Participants and Recruitment
2.4. Instruments and Procedures
2.4.1. Focus Groups
2.4.2. Phone Surveys
2.5. Data Analysis
3. Results
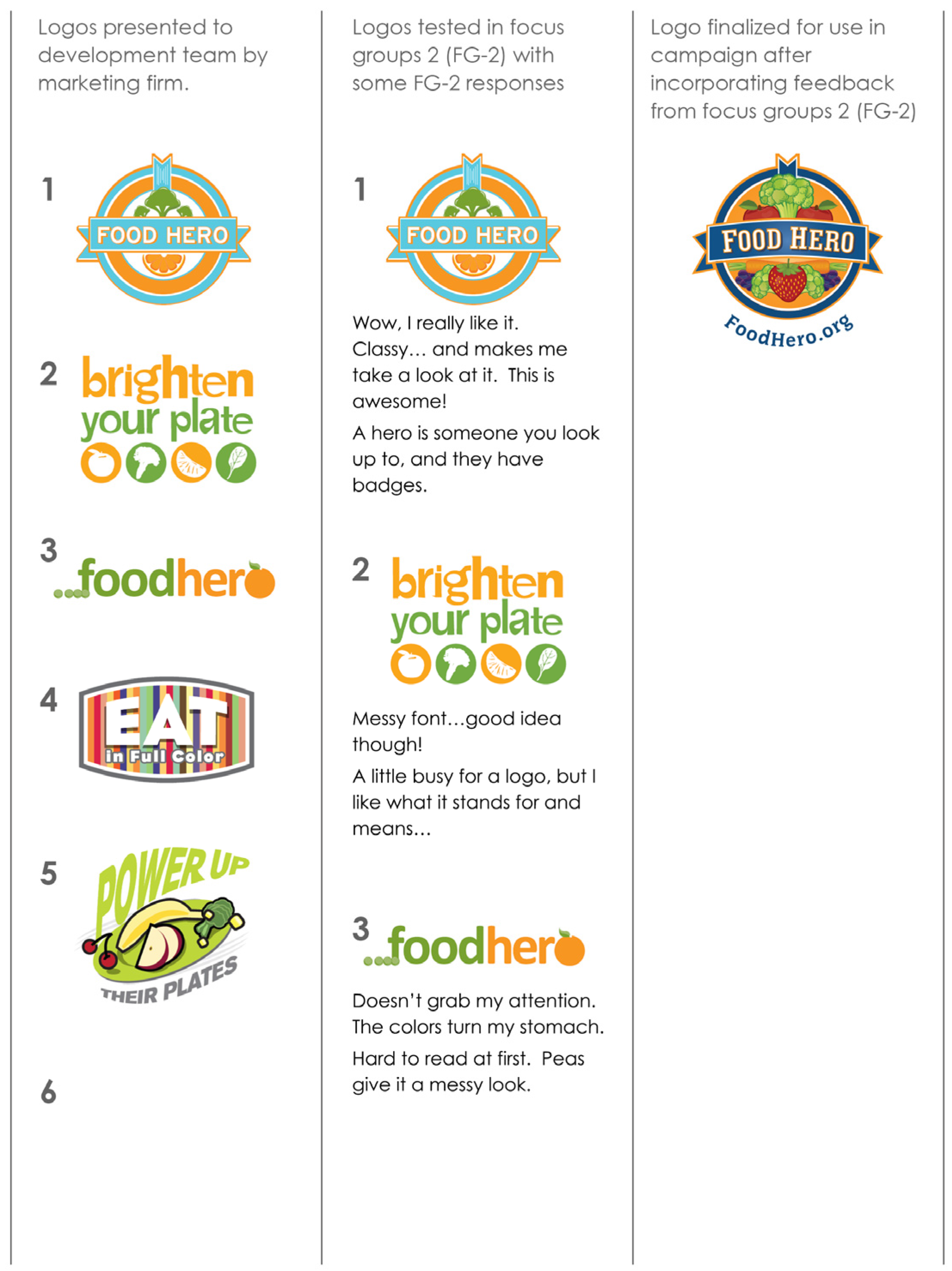
3.1. Focus Groups and Phone Survey 1
Main Themes
- “Potatoes are not just for dinner, we can have them for breakfast and lunch.”
- “Carrots are great. I have them as a snack.”
- “They are a good snack.”
- “My kids like the baby carrots so instead of buying the big long bugs bunny carrots they’ll eat the baby carrots.”
- “I always have them [bananas] in my house. They are a year round fruit for the most part. When they get home from school they have one.”
- “I make stir fry because my son’s not a big vegetable eater but he will eat it (stir fry). Now he likes broccoli, caluliflower, stuff like that.”
- “I buy fruits and vegetables in season…but I buy broccoli year round.”
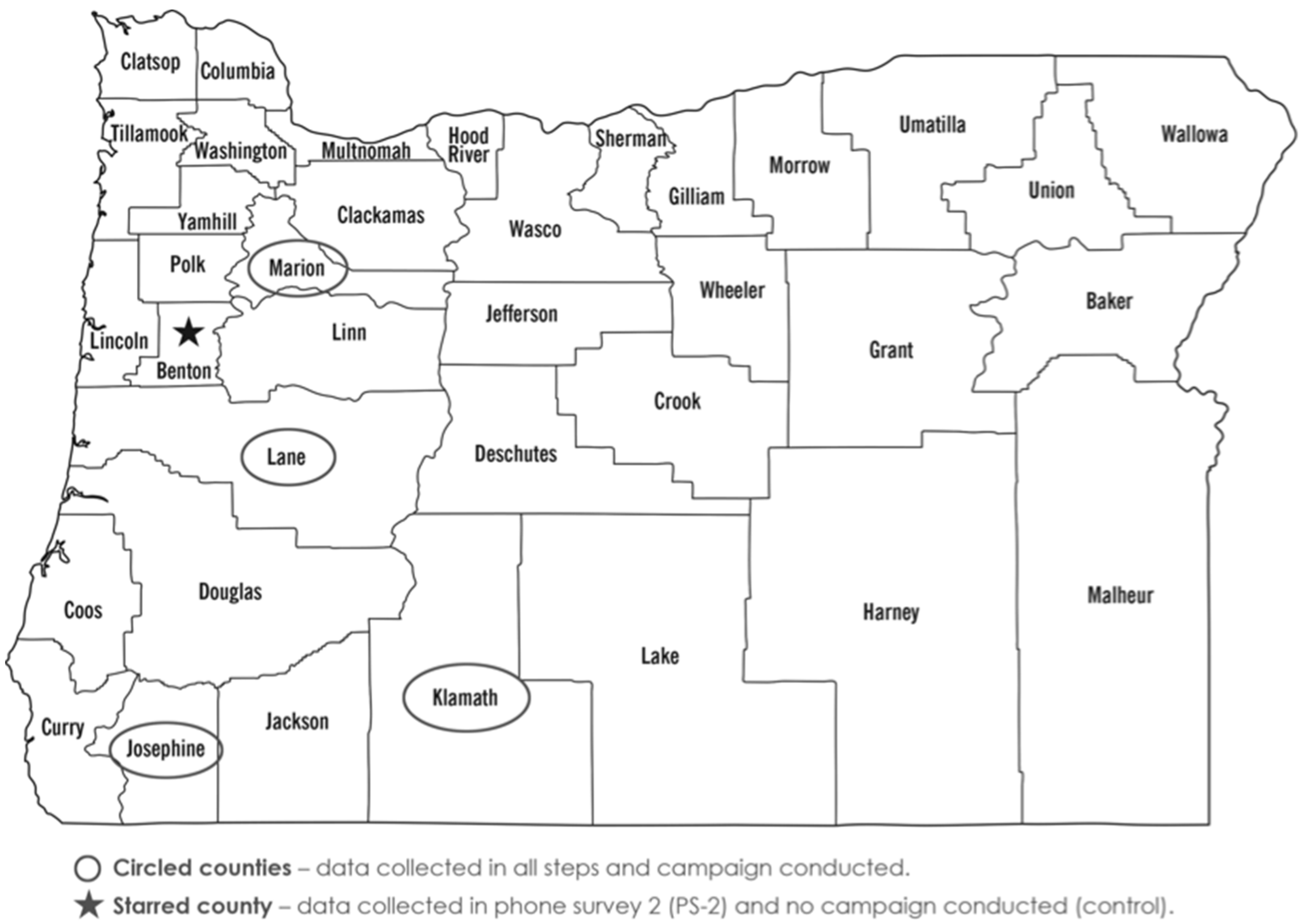
3.2. Phone Survey 2
Main Themes
4. Discussion
4.1. Study Strengths
4.2. Limitations
4.3. Implications for Research and Practice
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| FV | Fruits and Vegetables |
| SNAP | Supplemental Nutrition Assistance Program |
| BRFSS | Behavioral Risk Factor Surveillance System |
| SNAP-Ed | Supplemental Nutrition Assistance Program—Education |
| DHS | The Oregon Department of Human Services |
| PSE | Policy Systems and Environmental change efforts |
| FG | Focus Group |
| PS | Phone Survey |
| SM | Social Marketing |
| SCT | Social Cognitive Theory |
| USDA | United States Department of Agriculture |
References
- Association of Arizona Food Banks. Feeding America. Map the Meal Gap. Available online: http://www.azfoodbanks.org/index.php/hunger/ (accessed on 7 September 2016).
- Oregon Department of Human Services. July snap caseloads, 2000 through 2013. Unpublished work; 2015. [Google Scholar]
- Oregon Department of Human Services, Oregon Public Health. Oregon Overweight, Obesity, Physical Activity and Nutrition Facts. Available online: http://library.state.or.us/blogs/ReadAllAboutItOregon/wordpress/2012/05/oregon-overweight-obesity-physical-activity-and-nutrition-facts/ (accessed on 7 September 2016).
- Centers for Disease Control and Prevention (CDC). Nutrition, Physical Activity and Obesity Data, Trends and Maps. Available online: https://nccd.cdc.gov/NPAO_DTM/ (accessed on 7 September 2016).
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [PubMed]
- Drewnowski, A.; Darmon, N. The economics of obesity: Dietary energy density and energy cost. Am. J. Clin. Nutr. 2005, 82, 265S–273S. [Google Scholar] [PubMed]
- 2015 Dietary Guidelines Advisory Committee. Scientific Report of the 2015 Dietary Guidelines Advisory Committee. Available online: https://health.gov/dietaryguidelines/2015/guidelines/ (accessed on 7 September 2016).
- Haynes-Maslow, L.; Parsons, S.E.; Wheeler, S.B.; Leone, L.A. A qualitative study of perceived barriers to fruit and vegetable consumption among low-income populations, North Carolina, 2011. Prev. Chronic Dis. 2013. [Google Scholar] [CrossRef] [PubMed]
- Mcgurie, S. State Indicator Report on Fruits and Vegetables, 2013, Centers for Disease Control and Prevention, Atlanta, GA. Adv. Nutr. 2013, 4, 665–666. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Agriculture; U.S. Department of Health and Human Services. Dietary Guidelines for Americans, 2015; U.S. Government Printing Office: Washington, DC, USA, 2015.
- Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Data; U.S. Department of Health and Human Services: Atlanta, GA, USA.
- Moser, R.; Clayton, P.F. Obesity, Physical Activity And Nutrition In Kansas. Available online: http://www.kdheks.gov/brfss/PDF/2013_Kansas_Obesity_Burden_Document.pdf (accessed on 7 September 2016).
- Carins, J.E.; Rundle-Thiele, S.R. Eating for the better: A social marketing review (2000–2012). Public Health Nutr. 2014, 17, 1628–1639. [Google Scholar] [CrossRef] [PubMed]
- Gordon, R.; McDermott, L.; Stead, M.; Angus, K. The effectiveness of social marketing interventions for health improvement: What’s the evidence? Public Health 2006, 120, 1133–1139. [Google Scholar] [CrossRef] [PubMed]
- Pollard, C.M.; Miller, M.R.; Daly, A.M.; Crouchley, K.E.; O’Donoghue, K.J.; Lang, A.J.; Binns, C.W. Increasing fruit and vegetable consumption: Success of the Western Australian go for 2 & 5 campaign. Public Health Nutr. 2008, 11, 314–320. [Google Scholar] [PubMed]
- Kotler, P.; Lee, N.; Rothschild, M. Social Marketing: Influencing Behaviors for Good; Sage Publications: Thousand Oaks, CA, USA, 2006. [Google Scholar]
- Hopwood, T.; Merritt, R. Big pocket guide. In Social Marketing National Benchmark Criteria, 3rd ed.; UK National Social Marketing Centre: London, UK, 2011. [Google Scholar]
- Thomson, C.A.; Ravia, J. A systematic review of behavioral interventions to promote intake of fruit and vegetables. J. Am. Diet. Assoc. 2011, 111, 1523–1535. [Google Scholar] [CrossRef] [PubMed]
- Truong, V.D. Social marketing: A systematic review of research 1998–2012. Soc. Mark. Q. 2014, 20, 15–34. [Google Scholar] [CrossRef]
- Lefebvre, R.C. Theories and models in social marketing. In Handbook of Marketing and Society; Bloom, P.N., Gundlach, G.T., Eds.; Sage Publications: Newbury Park, CA, USA, 2000. [Google Scholar]
- Serdula, M.; Coates, R.; Byers, T.; Mokdad, A.; Jewell, S.; Chavez, N.; Maresperlman, J.; Newcomb, P.; Ritenbaugh, C.; Treiber, F.; et al. Evaluation of a brief telephone questionnaire to estimate fruit and vegetable consumption in diverse study populations. Epidemiology 1993, 4, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Oregon State University. Food Hero Website. Available online: http://www.foodhero.org/ (accessed on 7 September 2016).
- Tobey, L.N.; Manore, M.M. Social media and nutrition education: The food hero experience. J. Nutr. Educ. Behav. 2014, 46, 128–133. [Google Scholar] [CrossRef] [PubMed]
- US Department of Labor. Household Activities. Available online: http://www.bls.gov/tus/charts/household.htm (accessed on 7 September 2016).
- US Department of Labor. Purchasing Goods and Services. Available online: http://www.bls.gov/tus/current/purchasing.htm (accessed on 7 September 2016).
- Pew Research Center. Internet, Broadband and Cell Phone Statistics. Available online: http://www.pewinternet.org/2010/01/05/internet-broadband-and-cell-phone-statistics/ (accessed on 7 September 2016).
- Pew Research Center. Internet User Demographics. Available online: http://www.pewinternet.org/data-trend/teens/internet-user-demographics/ (accessed on 7 September 2016).
- Pew Research Center. Social Media User Demographics. Available online: http://www.pewinternet.org/data-trend/social-media/social-media-user-demographics/ (accessed on 7 September 2016).
- Treiman, K.; Freimuth, V.; Damron, D.; Lasswell, A.; Anliker, J.; Havas, S.; Langenberg, P.; Feldman, R. Attitudes and behaviors related to fruits and vegetables among low-income women in the WIC program. J. Nutr. Educ. 1996, 28, 149–156. [Google Scholar] [CrossRef]
- United States Department of Agriculture. Maximizing the Message: Helping Moms and Kids Make Healthier Food Choices. Available online: https://snaped.fns.usda.gov/materials/maximizing-message-helping-moms-and-kids-make-healthier-food-choices (accessed on 7 September 2016).
- McLaughlin, C.; Tarasuk, V.; Kreiger, N. An examination of at-home food preparation activity among low-income, food-insecure women. J. Am. Diet. Assoc. 2003, 103, 1506–1512. [Google Scholar] [CrossRef] [PubMed]
- Monsivais, P.; Aggarwal, A.; Drewnowski, A. Time spent on home food preparation and indicators of healthy eating. Am. J. Prev. Med. 2014, 47, 796–802. [Google Scholar] [CrossRef] [PubMed]
- Keim, N.L.; Forester, S.M.; Lyly, M.; Aaron, G.J.; Townsend, M.S. Vegetable variety is a key to improved diet quality in low-income women in California. J. Acad. Nutr. Diet. 2014, 114, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Meengs, J.S.; Roe, L.S.; Rolls, B.J. Vegetable variety: An effective strategy to increase vegetable intake in adults. J. Acad. Nutr. Diet. 2012, 112, 1211–1215. [Google Scholar] [CrossRef] [PubMed]
- Rickman, J.C.; Barret, D.M.; Bruhn, C.M. Nutritional comparison of fresh, frozen and canned fruits and vegetables. Part 1. Vitamins C and B and phenolic compounds. J. Sci. Food Agric. 2007, 87, 930–944. [Google Scholar] [CrossRef]
- Rickman, J.C.; Bruhn, C.M.; Barrett, D.M. Nutritional comparison of fresh, frozen, and canned fruits and vegetables II. Vitamin A and carotenoids, vitamin E, minerals and fiber. J. Sci. Food Agric. 2007, 87, 1185–1196. [Google Scholar] [CrossRef]
- Freedman, M.R.; Fulgoni, V.L., III. Canned vegetable and fruit consumption is associated with changes in nutrient intake and higher diet quality in children and adults: National health and nutrition examination survey 2001–2010. J. Acad. Nutr. Diet. 2016, 116, 940–948. [Google Scholar] [CrossRef] [PubMed]
- Comerford, K.B. Frequent canned food use is positively associated with nutrient-dense food group consumption and higher nutrient intakes in us children and adults. Nutrients 2015, 7, 5586–5600. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.R.; Knudson, W.A. Nutrition and cost comparisons of select canned, frozen, and fresh fruits and vegetables. Am. J. Lifestyle Med. 2014, 8, 430–437. [Google Scholar] [CrossRef]
- Hornick, B.A.; Childs, N.M.; Smith Edge, M.; Kapsak, W.R.; Dooher, C.; White, C. Is it time to rethink nutrition communications? A 5-year retrospective of Americans’ attitudes toward food, nutrition, and health. J. Acad. Nutr. Diet. 2013, 113, 14–23. [Google Scholar] [CrossRef] [PubMed]
- United States Department of Agriculture. SNAP Households Must Balance Multiple Priorities to Achieve A Healthful Diet. Available online: http://www.ers.usda.gov/amber-waves/2014-november/snap-households-must-balance-multiple-priorities-to-achieve-a-healthful-diet.aspx#.V8kaFjXENOc (accessed on 7 September 2016).
- Mushi-Brunt, C.; Haire-Joshu, D.; Elliott, M. Food spending behaviors and perceptions are associated with fruit and vegetable intake among parents and their preadolescent children. J. Nutr. Educ. Behav. 2007, 39, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Buzby, J.C.; Wells, H.F.; Kumcu, A.; Lin, B.-H.; Lucier, G.; Perez, A. Canned Fruit and Vegetable Consumption in the United States, an Updated Report to Congress; US Department of Agriculture, Economic Research Service: Washington, DC, USA, 2010.
- Produce for Better Health Foundation. State of the Plate, 2015 Study on America’s Consumption of Fruit and Vegetables. Available online: http://www.pbhfoundation.org/pdfs/about/res/pbh_res/State_of_the_Plate_2015_WEB_Bookmarked.pdf (accessed on 7 September 2016).
- Eikenberry, N.; Smith, C. Healthful eating: Perceptions, motivations, barriers, and promoters in low-income minnesota communities. J. Am. Diet. Assoc. 2004, 104, 1158–1161. [Google Scholar] [CrossRef] [PubMed]
- Black, M.M.; Hurley, K.M.; Oberlander, S.E.; Hager, E.R.; McGill, A.E.; White, N.T.; Quigg, A.M. Participants’ comments on changes in the revised special supplemental nutrition program for women, infants, and children food packages: The maryland food preference study. J. Am. Diet. Assoc. 2009, 109, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Wansink, B.; Pope, L. When do gain-framed health messages work better than fear appeals? Nutr. Rev. 2015, 73, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.E.; Satia, J.A.; Kristal, A.R.; Neuhouser, M.L.; Drewnowski, A. Is there a consumer backlash against the diet and health message? J. Am. Diet. Assoc. 2001, 101, 37–41. [Google Scholar] [CrossRef]
- Gallagher, K.M.; Updegraff, J.A. Health message framing effects on attitudes, intentions, and behaviors: A meta-analytic review. Ann. Behav. Med. 2013, 46, 127. [Google Scholar] [CrossRef]
- Rothman, A.J.; Salovey, P. Shaping perceptions to motivate healthy behavior: The role of message framing. Psychol. Bull. 1997, 121, 3–19. [Google Scholar] [CrossRef] [PubMed]
- Pivonka, E.; Seymour, J.; McKenna, J.; Baxter, S.D.; Williams, S. Development of the behaviorally focused fruits & veggies—More matters public health initiative. J. Am. Diet. Assoc. 2011, 111, 1570–1577. [Google Scholar] [PubMed]
- Shive, S.E.; Morris, M.N. Evaluation of the energize your life! Social marketing campaign pilot study to increase fruit intake among community college students. J. Am. Coll. Health 2006, 55, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Glasson, C.; Chapman, K.; Wilson, T.; Gander, K.; Hughes, C.; Hudson, N.; James, E. Increased exposure to community-based education and ‘below the line’ social marketing results in increased fruit and vegetable consumption. Public Health Nutr. 2013, 16, 1961–1970. [Google Scholar] [CrossRef] [PubMed]
- Woodhouse, L.; Bussell, P.; Jones, S.; Lloyd, H.; Macdowall, W.; Merritt, R. Bostin value: An intervention to increase fruit and vegetable consumption in a deprived neighborhood of dudley, United Kingdom. Soc. Mark. Q. 2012, 18, 221–233. [Google Scholar] [CrossRef]
- Dharod, J.M.; Drewette-Card, R.; Crawford, D. Development of the Oxford Hills Healthy Moms Project using a social marketing process: A community-based physical activity and nutrition intervention for low-socioeconomic-status mothers in a rural area in Maine. Health Promot. Pract. 2011, 12, 312–321. [Google Scholar] [CrossRef] [PubMed]
- Hampson, S.E.; Martin, J.; Jorgensen, J.; Barker, M. A social marketing approach to improving the nutrition of low-income women and children: An initial focus group study. Public Health Nutr. 2009, 12, 1563–1568. [Google Scholar] [CrossRef] [PubMed]
- Sugerman, S.; Backman, D.; Foerster, S.B.; Ghirardelli, A.; Linares, A.; Fong, A. Using an opinion poll to build an obesity-prevention social marketing campaign for low-income asian and hispanic immigrants: Report of findings. J. Nutr. Educ. Behav. 2011, 43, S53–S66. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Message Priority Given by Participants from Highest (1) to Lowest (7) Preference | |
|---|---|
| Messages Tested in Focus Groups 2 (FG-2) |
|
| Messages Used in Campaign and then Tested in Phone Survey 2 (PS-2) |
|
| Belief Statement | PS-1 Mean ± SD | PS-2 Mean ± SD | p Value (PS-1 vs. PS-2) | PS-2 Control Mean ± SD | p Value (PS-2 vs. Control) |
|---|---|---|---|---|---|
| 4.25 ± 1.06 | 4.25 ± 1.08 | p = 0.50 | 4.23 ± 1.16 | p = 0.44 |
| 4.33 ± 1.03 | 4.35 ± 1.09 | p = 0.35 | 4.13 ± 1.14 | p = 0.03 2 |
| 2.17 ± 1.17 | 2.21 ± 1.25 | p = 0.30 | 1.93 ± 0.96 | p = 0.01 2 |
| 2.90 ± 1.37 | 3.00 ± 1.30 | p = 0.065 | 2.91 ± 1.25 | p = 0.24 |
| 3.73 ± 1.30 | 3.82 ± 1.26 | p = 0.055 | 3.79 ± 1.22 | p = 0.38 |
| 4.37 ± 1.00 | 4.49 ± 0.90 | p = 0.005 2 | 4.43 ± 1.06 | p = 0.27 |
| 3.42 ± 1.39 | 3.17 ± 1.45 | p = 0.0005 2 | 3.06 ± 1.30 | p = 0.21 |
| 2.45 ± 1.31 | 2.29 ± 1.27 | p = 0.005 2 | 2.45 ± 1.28 | p = 0.09 |
| Focus Groups 1 (FG-1) | Phone Survey 1 (PS-1) | Focus Groups 2 (FG-2) | Phone Survey 2 (PS-2) | |
|---|---|---|---|---|
| Subjects (n) | n = 25, 4 FG | n = 1244 | n = 11, 2 FG | n = 802 |
| Female (%) | 92 | 86 | 100 | 84 (Control) 86 (Intervention) |
| Mean age (year) | 36.7 | 34.5 | 42.9 | 33.2 (Control) 34.7 (Intervention) |
| Household size (3–4 people) (%) | 65 | 55 | 36 | 55 (Control) 54 (Intervention) |
| Household size (1–2 children) (%) | 76 | 71 | 64 | 77 (Control) 71 (Intervention) |
| Single parent households (%) | 52 | 39 | 45 | 45 (Control) 43 (Intervention) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tobey, L.N.; Koenig, H.F.; Brown, N.A.; Manore, M.M. Reaching Low-Income Mothers to Improve Family Fruit and Vegetable Intake: Food Hero Social Marketing Campaign—Research Steps, Development and Testing. Nutrients 2016, 8, 562. https://doi.org/10.3390/nu8090562
Tobey LN, Koenig HF, Brown NA, Manore MM. Reaching Low-Income Mothers to Improve Family Fruit and Vegetable Intake: Food Hero Social Marketing Campaign—Research Steps, Development and Testing. Nutrients. 2016; 8(9):562. https://doi.org/10.3390/nu8090562
Chicago/Turabian StyleTobey, Lauren N., Harold F. Koenig, Nicole A. Brown, and Melinda M. Manore. 2016. "Reaching Low-Income Mothers to Improve Family Fruit and Vegetable Intake: Food Hero Social Marketing Campaign—Research Steps, Development and Testing" Nutrients 8, no. 9: 562. https://doi.org/10.3390/nu8090562
APA StyleTobey, L. N., Koenig, H. F., Brown, N. A., & Manore, M. M. (2016). Reaching Low-Income Mothers to Improve Family Fruit and Vegetable Intake: Food Hero Social Marketing Campaign—Research Steps, Development and Testing. Nutrients, 8(9), 562. https://doi.org/10.3390/nu8090562