Associations of Fat Mass and Fat-Free Mass with Physical Fitness in 4-Year-Old Children: Results from the MINISTOP Trial

 , , ,
, , , 
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Body Composition
2.3. Physical Fitness
2.4. Physical Activity
2.5. Statistical Analysis
3. Results
3.1. Descriptive Statistics
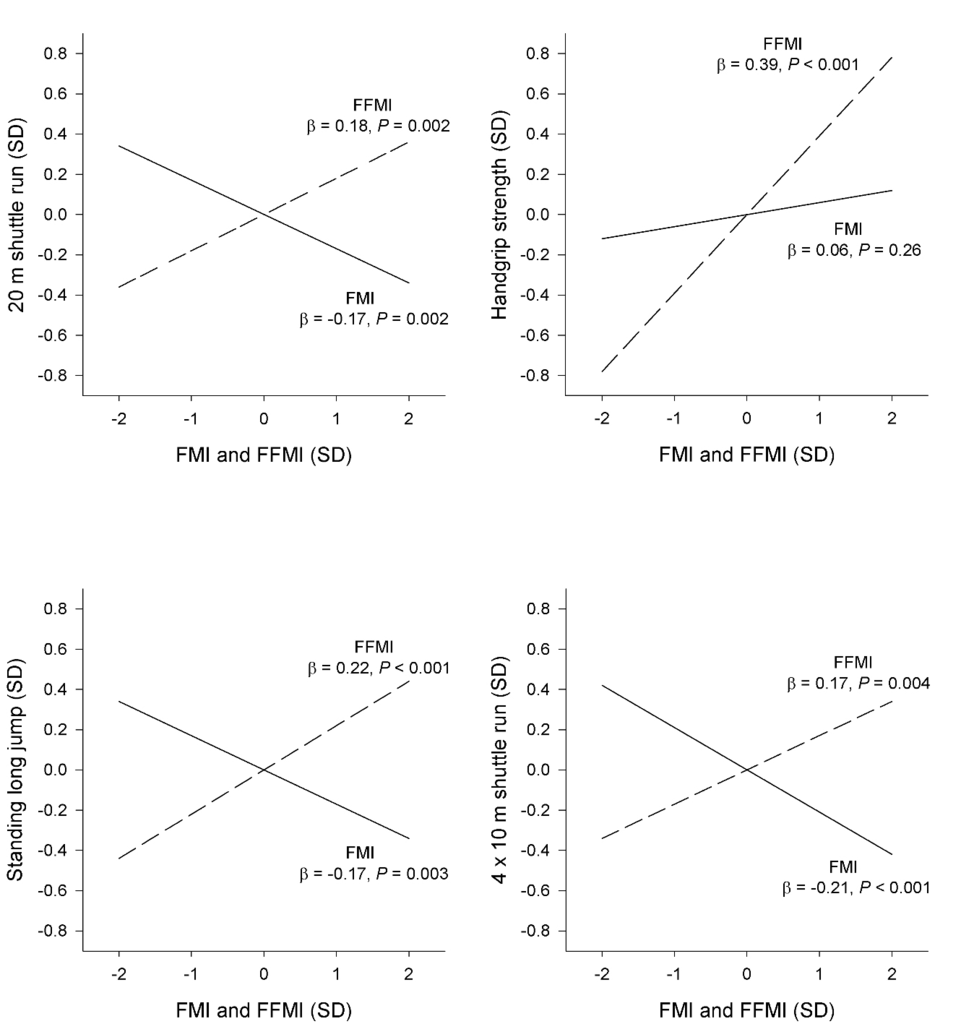
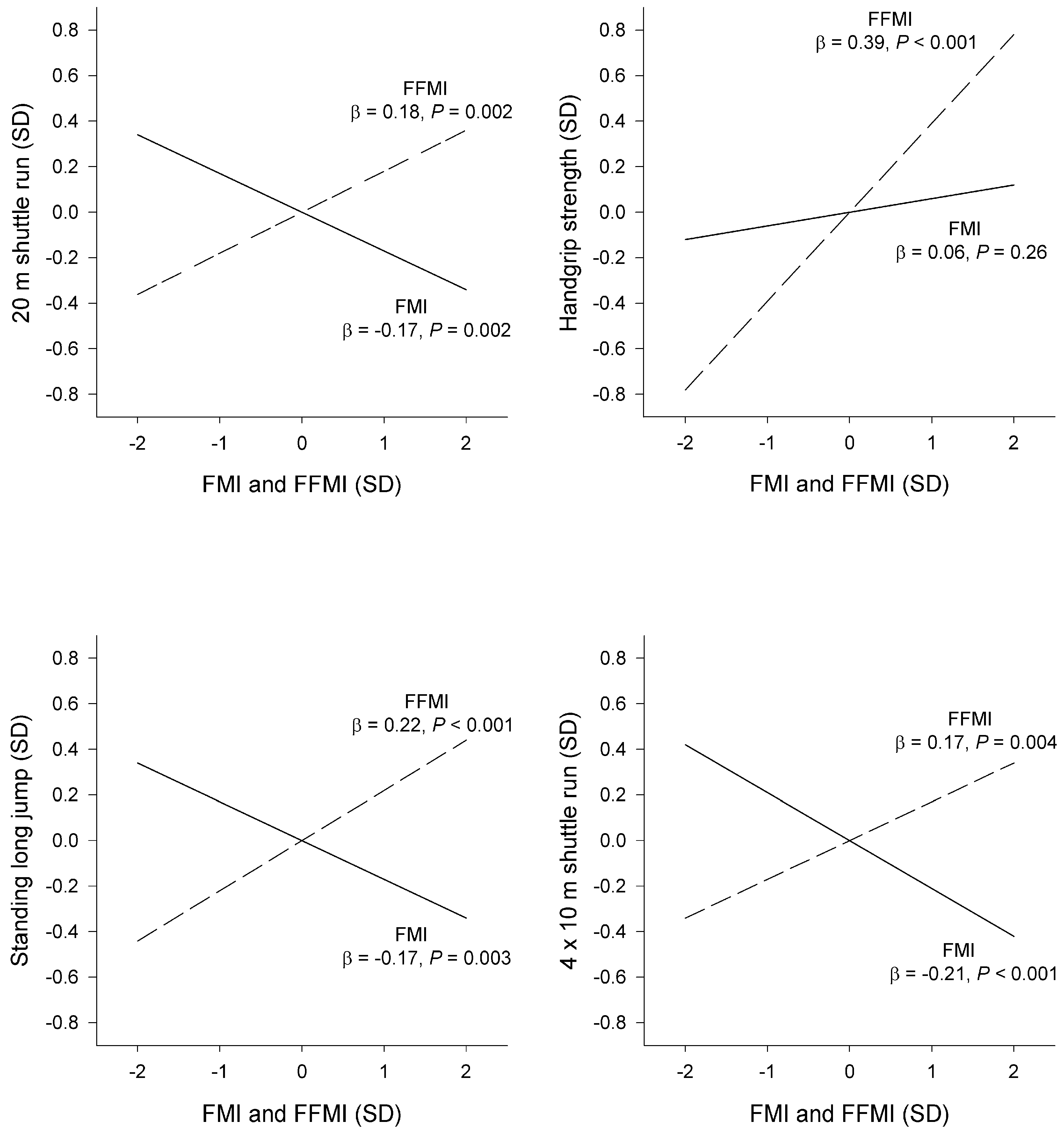
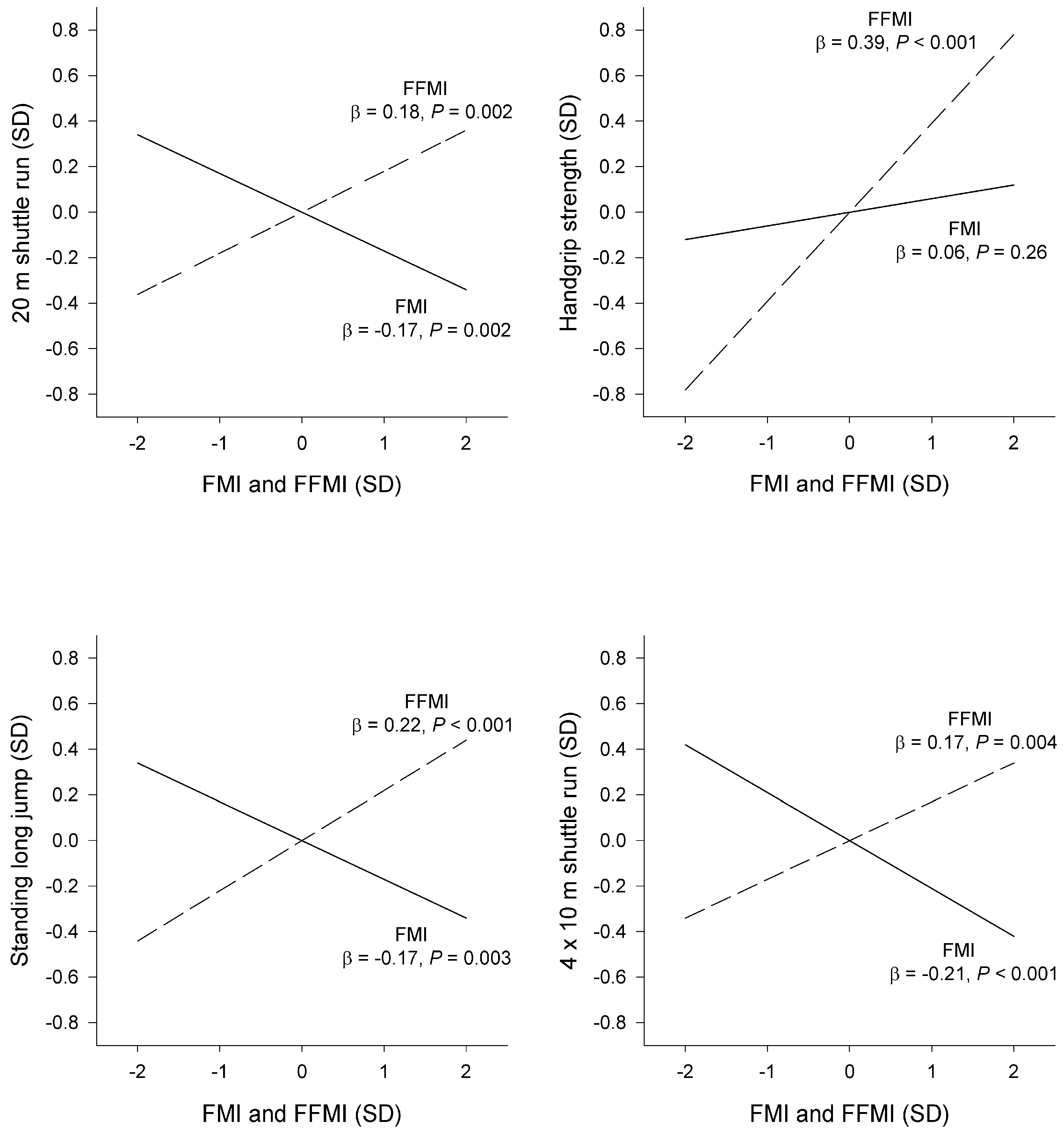
3.2. Associations of Body Composition with Physical Fitness
4. Discussion
4.1. Statement of Principal Findings
4.2. Comparison with Other Studies in Preschoolers
4.3. Comparison with Studies in Older Children
4.4. Direction of the Association between Body Composition and Physical Fitness
4.5. Strengths and Limitations
4.6. Interpretation and Implications
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| BMI | body mass index |
| FFM | fat-free mass |
| FM | fat mass |
| FFMI | fat-free mass index |
| FMI | fat-mass index |
| VPA | vigorous-intensity physical activity |
| %FM | percent fat mass |
References
- World Health Organization. Available online: http://www.who.int/dietphysicalactivity/childhood/en/ (accessed on 8 June 2016).
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- Singh, A.; Mulder, C.; Twisk, J.; Mechelen, W.; Chinapaw, M. Tracking of childhood overweight into adulthood: A systematic review of the literature. Obes. Rev. 2008, 9, 474–488. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Castro-Pinero, J.; Artero, E.G.; Ortega, F.B.; Sjostrom, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef] [PubMed]
- Gutin, B.; Basch, C.; Shea, S.; Contento, I.; DeLozier, M.; Rips, J.; Irigoyen, M.; Zybert, P. Blood pressure, fitness, and fatness in 5- and 6-year-old children. JAMA 1990, 264, 1123–1127. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.J.; Arslanian, S.A. Cardiorespiratory fitness and abdominal adiposity in youth. Eur. J. Clin. Nutr. 2007, 61, 561–565. [Google Scholar] [CrossRef] [PubMed]
- Stigman, S.; Rintala, P.; Kukkonen-Harjula, K.; Kujala, U.; Rinne, M.; Fogelholm, M. Eight-year-old children with high cardiorespiratory fitness have lower overall and abdominal fatness. Int. J. Pediatr. Obes. 2009, 4, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Willig, A.L.; Hunter, G.R.; Casazza, K.; Heimburger, D.C.; Beasley, T.M.; Fernandez, J.R. Body fat and racial genetic admixture are associated with aerobic fitness levels in a multiethnic pediatric population. Obesity 2011, 19, 2222–2227. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjostrom, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2008, 32, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Silventoinen, K.; Tynelius, P.; Rasmussen, F. Muscular strength in male adolescents and premature death: Cohort study of one million participants. BMJ 2012, 345, e7279. [Google Scholar] [CrossRef] [PubMed]
- Galvan, M.; Uauy, R.; Lopez-Rodriguez, G.; Kain, J. Association between childhood obesity, cognitive development, physical fitness and social-emotional wellbeing in a transitional economy. Ann. Hum. Biol. 2014, 41, 99–104. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Tellez, B.; Sanchez-Delgado, G.; Cadenas-Sanchez, C.; Mora-Gonzalez, J.; Martin-Matillas, M.; Löf, M.; Ortega, F.B.; Ruiz, J.R. Health-related physical fitness is associated with total and central body fat in preschool children aged 3 to 5 years. Pediatr. Obes. 2015. [Google Scholar] [CrossRef] [PubMed]
- Niederer, I.; Kriemler, S.; Zahner, L.; Burgi, F.; Ebenegger, V.; Marques, P.; Puder, J.J. BMI group-related differences in physical fitness and physical activity in preschool-age children: A cross-sectional analysis. Res. Q. Exerc. Sport 2012, 83, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Reeves, L.; Broeder, C.E.; Kennedy-Honeycutt, L.; East, C.; Matney, L. Relationship of fitness and gross motor skills for five- to six-year-old children. Percept. Mot. Skills 1999, 89, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Agha-Alinejad, H.; Farzad, B.; Salari, M.; Kamjoo, S.; Harbaugh, B.L.; Peeri, M. Prevalence of overweight and obesity among Iranian preschoolers: Interrelationship with physical fitness. J. Res. Med. Sci. 2015, 20, 334–431. [Google Scholar] [PubMed]
- Cadenas-Sanchez, C.; Artero, E.G.; Concha, F.; Leyton, B.; Kain, J. Anthropometric Characteristics and Physical Fitness Level in Relation to Body Weight Status in Chilean Preschool Children. Nutr. Hosp. 2015, 32, 346–353. [Google Scholar] [PubMed]
- Woll, A.; Worth, A.; Mundermann, A.; Holling, H.; Jekauc, D.; Bos, K. Age- and sex-dependent disparity in physical fitness between obese and normal weight children and adolescents. J. Sports Med. Phys. Fit. 2013, 53, 48–55. [Google Scholar]
- Forsum, E.; Flinke Carlsson, E.; Henriksson, H.; Henriksson, P.; Löf, M. Total body fat content versus BMI in 4-year-old healthy Swedish children. J. Obes. 2013, 2013, 206715. [Google Scholar] [CrossRef] [PubMed]
- Freedman, D.S.; Wang, J.; Maynard, L.M.; Thornton, J.C.; Mei, Z.; Pierson, R.N.; Dietz, W.H.; Horlick, M. Relation of BMI to fat and fat-free mass among children and adolescents. Int. J. Obes. 2005, 29, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Delisle, C.; Sandin, S.; Forsum, E.; Henriksson, H.; Trolle-Lagerros, Y.; Larsson, C.; Maddison, R.; Ortega, F.B.; Ruiz, J.R.; Silfvernagel, K.; et al. A web- and mobile phone-based intervention to prevent obesity in 4-year-olds (MINISTOP): A population-based randomized controlled trial. BMC Public Health 2015, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Leppanen, M.H.; Nystrom, C.D.; Henriksson, P.; Pomeroy, J.; Ruiz, J.R.; Ortega, F.B.; Cadenas-Sánchez, C.; Löf, M. Physical activity intensity, sedentary behavior, body composition and physical fitness in 4-year-old children: Results from the MINISTOP trial. Int. J. Obes. 2016. [Google Scholar] [CrossRef] [PubMed]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatr. Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Wikland, K.A.; Luo, Z.C.; Niklasson, A.; Karlberg, J. Swedish population-based longitudinal reference values from birth to 18 years of age for height, weight and head circumference. Acta. Paediatr. 2002, 91, 739–754. [Google Scholar] [CrossRef] [PubMed]
- Fields, D.A.; Allison, D.B. Air-displacement plethysmography pediatric option in 2–6 Years old using the four-compartment model as a criterion method. Obesity 2012, 20, 1732–1737. [Google Scholar] [CrossRef] [PubMed]
- Ortega, F.B.; Cadenas-Sanchez, C.; Sanchez-Delgado, G.; Mora-Gonzalez, J.; Martinez-Tellez, B.; Artero, E.G.; Castro-Piñero, J.; Labayen, I.; Chillón, P.; Löf, M.; et al. Systematic review and proposal of a field-based physical fitness-test battery in preschool children: The PREFIT battery. Sports Med. 2015, 45, 533–555. [Google Scholar] [CrossRef] [PubMed]
- Cadenas-Sanchez, C.; Nystrom, C.D.; Sanchez-Delgado, G.; Martinez-Tellez, B.; Mora-Gonzalez, J.; Risinger, A.S.; Ruiz, J.R.; Ortega, F.B.; Löf, M. Prevalence of overweight/obesity and fitness level in preschool children from the north compared with the south of Europe: An exploration with two countries. Pediatr. Obes. 2015. [Google Scholar] [CrossRef] [PubMed]
- Collings, P.J.; Brage, S.; Ridgway, C.L.; Harvey, N.C.; Godfrey, K.M.; Inskip, H.M.; Cooper, C.; Wareham, N.J.; Ekelund, U. Physical activity intensity, sedentary time, and body composition in preschoolers. Am. J. Clin. Nutr. 2013, 97, 1020–1028. [Google Scholar] [CrossRef] [PubMed]
- Chandler, J.L.; Brazendale, K.; Beets, M.W.; Mealing, B.A. Classification of physical activity intensities using a wrist-worn accelerometer in 8–12-year-old children. Pediatr. Obes. 2015. [Google Scholar] [CrossRef] [PubMed]
- Bürgi, F.; Meyer, U.; Granacher, U.; Schindler, C.; Marques-Vidal, P.; Kriemler, S.; Puder, J.J. Relationship of physical activity with motor skills, aerobic fitness and body fat in preschool children: A cross-sectional and longitudinal study (Ballabeina). Int. J. Obes. 2011, 35, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Zaqout, M.; Vyncke, K.; Moreno, L.A.; De Miguel-Etayo, P.; Lauria, F.; Molnar, D.; Lissner, L.; Hunsberger, M.; Veidebaum, T.; Tornaritis, M.; et al. Determinant factors of physical fitness in European children. Int. J. Public Health 2016. [Google Scholar] [CrossRef] [PubMed]
- Artero, E.G.; Espana-Romero, V.; Ortega, F.B.; Jimenez-Pavon, D.; Ruiz, J.R.; Vicente-Rodriguez, G.; Bueno, M.; Marcos, A.; Gómez-Martínez, S.; Urzangui, A.; et al. Health-related fitness in adolescents: Underweight, and not only overweight, as an influencing factor. The AVENA study. Scand. J. Med. Sci. Sports 2010, 20, 418–427. [Google Scholar] [CrossRef] [PubMed]
- Moliner-Urdiales, D.; Ruiz, J.R.; Vicente-Rodriguez, G.; Ortega, F.B.; Rey-Lopez, J.P.; España-Romero, V.; Casajús, J.A.; Molnar, D.; Widhalm, K.; Dallongeville, J.; et al. Associations of muscular and cardiorespiratory fitness with total and central body fat in adolescents: The HELENA study. Br. J. Sports Med. 2011, 45, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Ervin, R.B.; Fryar, C.D.; Wang, C.Y.; Miller, I.M.; Ogden, C.L. Strength and body weight in US children and adolescents. Pediatrics 2014, 134, e782–e789. [Google Scholar] [CrossRef] [PubMed]
- Cadenas-Sanchez, C.; Martinez-Tellez, B.; Sanchez-Delgado, G.; Mora-Gonzalez, J.; Castro-Pinero, J.; Löf, M.; Ruiz, J.R.; Ortega, F.B. Assessing physical fitness in preschool children: Feasibility, reliability and practical recommendations for the PREFIT battery. J. Sci. Med. Sport 2016. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| All | Boys | Girls | p a | ||||
|---|---|---|---|---|---|---|---|
| n | Value | n | Value | n | Value | ||
| Age (years) | 303 | 4.48 ± 0.15 | 168 | 4.49 ± 0.15 | 135 | 4.47 ± 0.15 | 0.34 |
| Weight (kg) | 303 | 18.3 ± 2.5 | 168 | 18.5 ± 2.4 | 135 | 18.1 ± 2.6 | 0.11 |
| Weight for age z-score b | 303 | −0.07 ± 1.11 | 168 | −0.07 ± 1.11 | 135 | −0.07 ± 1.10 | 0.97 |
| Height (cm) | 303 | 107.6 ± 4.2 | 168 | 107.9 ± 4.3 | 135 | 107.1 ± 4.1 | 0.10 |
| Height for age z-score b | 303 | −0.04 ± 0.97 | 168 | −0.03 ± 1.00 | 135 | −0.05 ± 0.94 | 0.85 |
| Proportion of overweight/obesity c | 303 | 26 (8.6%) | 168 | 14 (8.3%) | 135 | 12 (8.9%) | 0.86 |
| BMI (kg/m2) | 303 | 15.8 ± 1.4 | 168 | 15.8 ± 1.3 | 135 | 15.7 ± 1.4 | 0.28 |
| FMI (kg/m2) | 303 | 4.1 ± 0.9 | 168 | 4.0 ± 0.8 | 135 | 4.3 ± 1.0 | 0.001 |
| FFMI (kg/m2) | 303 | 11.6 ± 1.0 | 168 | 11.9 ± 1.0 | 135 | 11.4 ± 0.9 | <0.001 |
| FM (%) | 303 | 26.0 ± 4.4 | 168 | 25.0 ± 3.9 | 135 | 27.3 ± 4.7 | <0.001 |
| Physical fitness test characteristics | |||||||
| 20 m shuttle run (laps) | 296 | 5.9 ± 2.6 | 162 | 5.7 ± 2.6 | 134 | 6.1 ± 2.6 | 0.20 |
| Handgrip strength (kg) | 302 | 6.4 ± 1.6 | 168 | 6.8 ± 1.6 | 134 | 6.0 ± 1.4 | <0.001 |
| Standing long jump (cm) | 303 | 71.7 ± 15.2 | 168 | 72.3 ± 15.6 | 134 | 70.9 ± 14.6 | 0.43 |
| 4 × 10 m shuttle run d (s) | 303 | 18.2 ± 1.9 | 168 | 18.2 ± 2.2 | 134 | 18.0 ± 1.6 | 0.34 |
| ActiGraph characteristics | |||||||
| Valid days e | 295 | 6.7 ± 0.8 | 166 | 6.7 ± 0.7 | 129 | 6.6 ± 1.0 | 0.089 |
| Awake wearing time (min/day) | 295 | 841 ± 56 | 166 | 840 ± 59 | 129 | 843 ± 53 | 0.67 |
| VPA f (min/day) | 295 | 7.4 ± 4.9 | 166 | 8.1 ± 5.6 | 129 | 6.5 ± 3.6 | 0.004 |
| Body Composition Measures (x) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BMI (kg/m2) | FMI (kg/m2) | FFMI (kg/m2) | FM (%) | |||||||||
| Physical fitness tests (y) | b | SE | p | b | SE | p | b | SE | p | b | SE | p |
| 20 m shuttle run (laps) | ||||||||||||
| Unadjusted | 0.01 | 0.11 | 0.92 | −0.46 | 0.16 | 0.006 | 0.44 | 0.16 | 0.006 | −0.12 | 0.03 | <0.001 |
| Adjusted b | 0.01 | 0.11 | 0.95 | −0.50 | 0.16 | 0.002 | 0.48 | 0.16 | 0.002 | −0.12 | 0.03 | <0.001 |
| Adjusted b + VPA | −0.05 | 0.10 | 0.61 | −0.45 | 0.15 | 0.003 | 0.33 | 0.15 | 0.030 | −0.11 | 0.03 | 0.001 |
| Handgrip strength (kg) | ||||||||||||
| Unadjusted | 0.40 | 0.06 | <0.001 | 0.07 | 0.10 | 0.50 | 0.72 | 0.09 | <0.001 | −0.04 | 0.02 | 0.070 |
| Adjusted b | 0.38 | 0.06 | <0.001 | 0.10 | 0.09 | 0.26 | 0.64 | 0.09 | <0.001 | −0.01 | 0.02 | 0.64 |
| Adjusted b + VPA | 0.37 | 0.06 | <0.001 | 0.11 | 0.09 | 0.24 | 0.61 | 0.09 | <0.001 | −0.01 | 0.02 | 0.79 |
| Standing long jump (cm) | ||||||||||||
| Unadjusted | 0.43 | 0.64 | 0.50 | −2.66 | 0.94 | 0.005 | 3.30 | 0.88 | <0.001 | −0.74 | 0.19 | <0.001 |
| Adjusted b | 0.36 | 0.64 | 0.57 | −2.77 | 0.94 | 0.003 | 3.38 | 0.91 | <0.001 | −0.69 | 0.20 | 0.001 |
| Adjusted b + VPA | 0.09 | 0.64 | 0.88 | −2.71 | 0.94 | 0.004 | 2.85 | 0.92 | 0.002 | −0.65 | 0.20 | 0.001 |
| 4 × 10 m shuttle run c (s) | ||||||||||||
| Unadjusted | 0.05 | 0.08 | 0.55 | 0.41 | 0.12 | 0.001 | −0.28 | 0.11 | 0.015 | 0.10 | 0.03 | <0.001 |
| Adjusted b | 0.05 | 0.08 | 0.53 | 0.45 | 0.12 | <0.001 | −0.33 | 0.12 | 0.004 | 0.10 | 0.03 | <0.001 |
| Adjusted b + VPA | 0.09 | 0.08 | 0.27 | 0.41 | 0.12 | <0.001 | −0.23 | 0.11 | 0.043 | 0.09 | 0.02 | <0.001 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Henriksson, P.; Cadenas-Sanchez, C.; Leppänen, M.H.; Delisle Nyström, C.; Ortega, F.B.; Pomeroy, J.; Ruiz, J.R.; Löf, M. Associations of Fat Mass and Fat-Free Mass with Physical Fitness in 4-Year-Old Children: Results from the MINISTOP Trial. Nutrients 2016, 8, 473. https://doi.org/10.3390/nu8080473
Henriksson P, Cadenas-Sanchez C, Leppänen MH, Delisle Nyström C, Ortega FB, Pomeroy J, Ruiz JR, Löf M. Associations of Fat Mass and Fat-Free Mass with Physical Fitness in 4-Year-Old Children: Results from the MINISTOP Trial. Nutrients. 2016; 8(8):473. https://doi.org/10.3390/nu8080473
Chicago/Turabian StyleHenriksson, Pontus, Cristina Cadenas-Sanchez, Marja H. Leppänen, Christine Delisle Nyström, Francisco B. Ortega, Jeremy Pomeroy, Jonatan R. Ruiz, and Marie Löf. 2016. "Associations of Fat Mass and Fat-Free Mass with Physical Fitness in 4-Year-Old Children: Results from the MINISTOP Trial" Nutrients 8, no. 8: 473. https://doi.org/10.3390/nu8080473
APA StyleHenriksson, P., Cadenas-Sanchez, C., Leppänen, M. H., Delisle Nyström, C., Ortega, F. B., Pomeroy, J., Ruiz, J. R., & Löf, M. (2016). Associations of Fat Mass and Fat-Free Mass with Physical Fitness in 4-Year-Old Children: Results from the MINISTOP Trial. Nutrients, 8(8), 473. https://doi.org/10.3390/nu8080473