Lutein, Zeaxanthin and Meso-zeaxanthin Supplementation Associated with Macular Pigment Optical Density


Abstract
:
1. Introduction
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection
2.3. Data Extraction and Study Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Literature Search
3.2. Study Characteristics
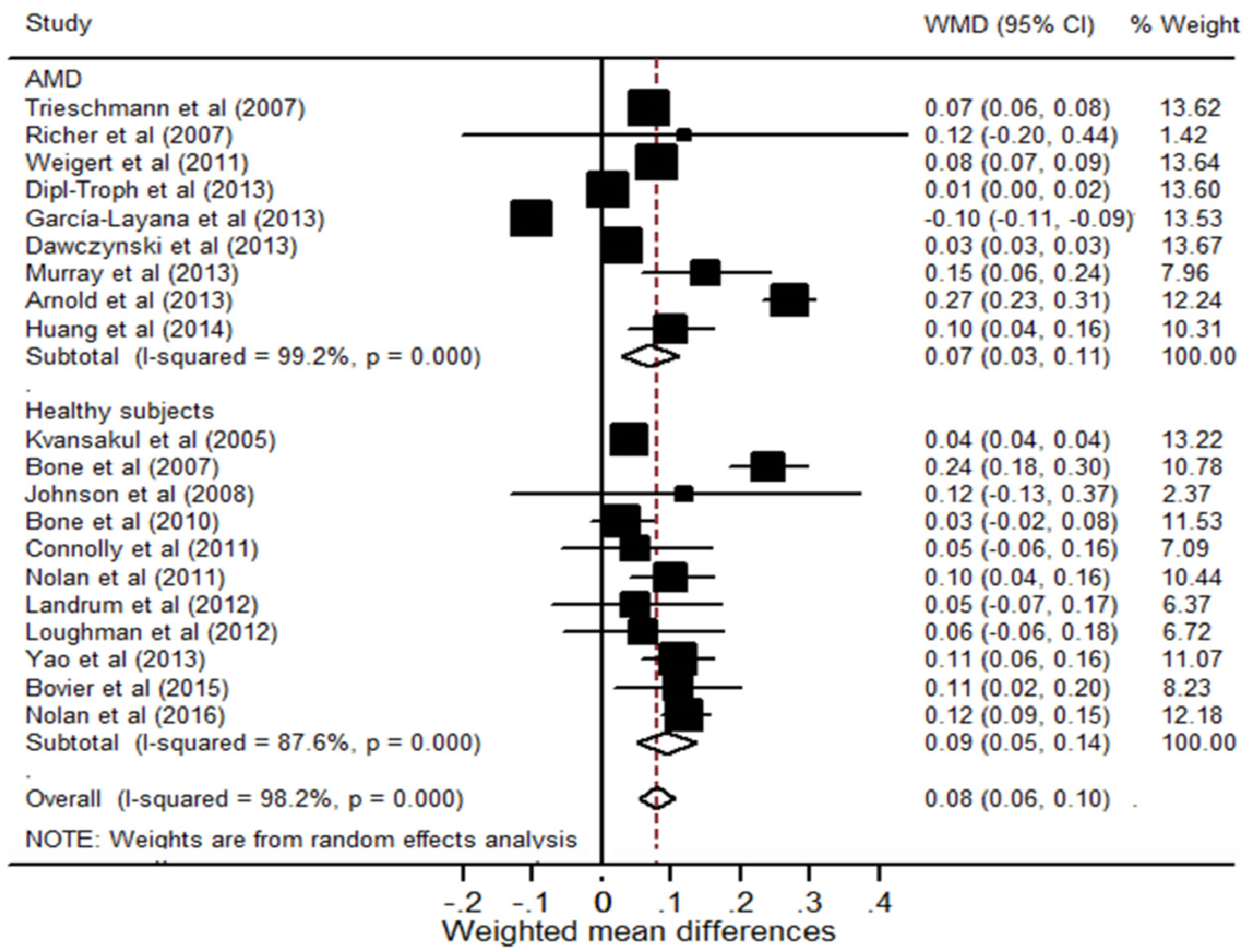
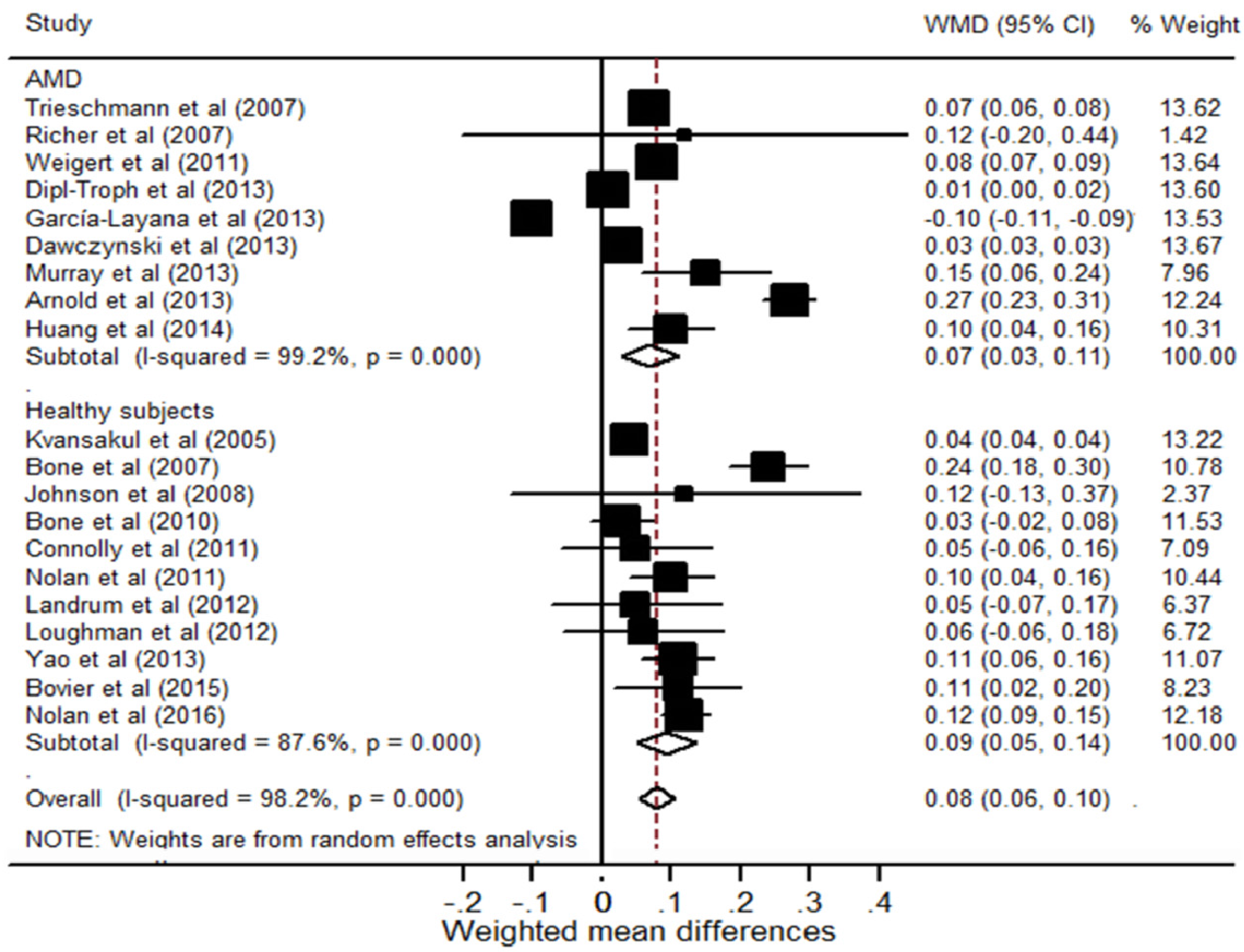
3.3. The Effect of Lutein, Zeaxanthin or/and Meso-zeaxanthin Supplementation on MPOD in Patients with AMD
3.4. The Effect of Lutein, Zeaxanthin or/and Meso-zeaxanthin Supplementation on MPOD in Healthy Subjects
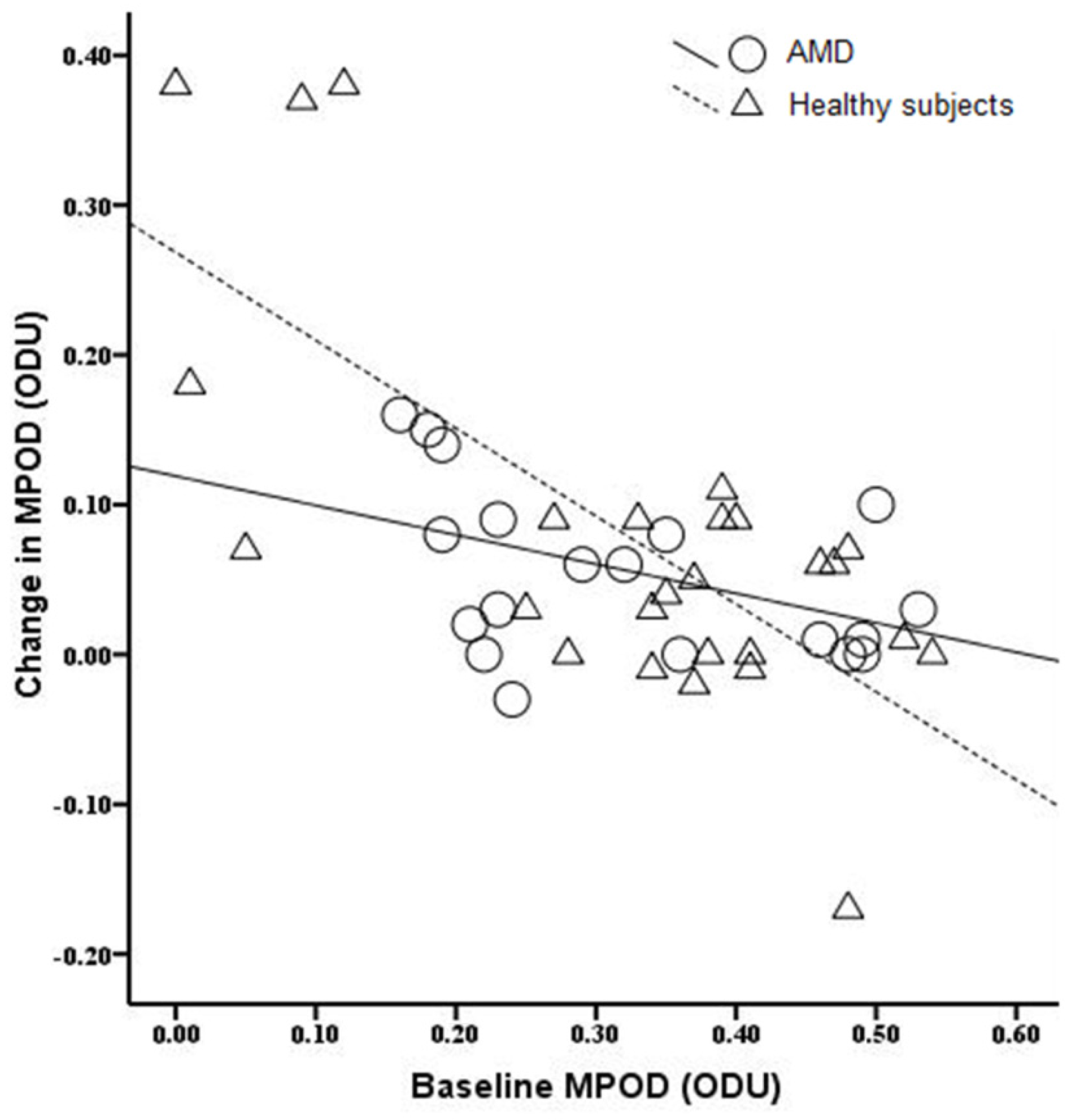
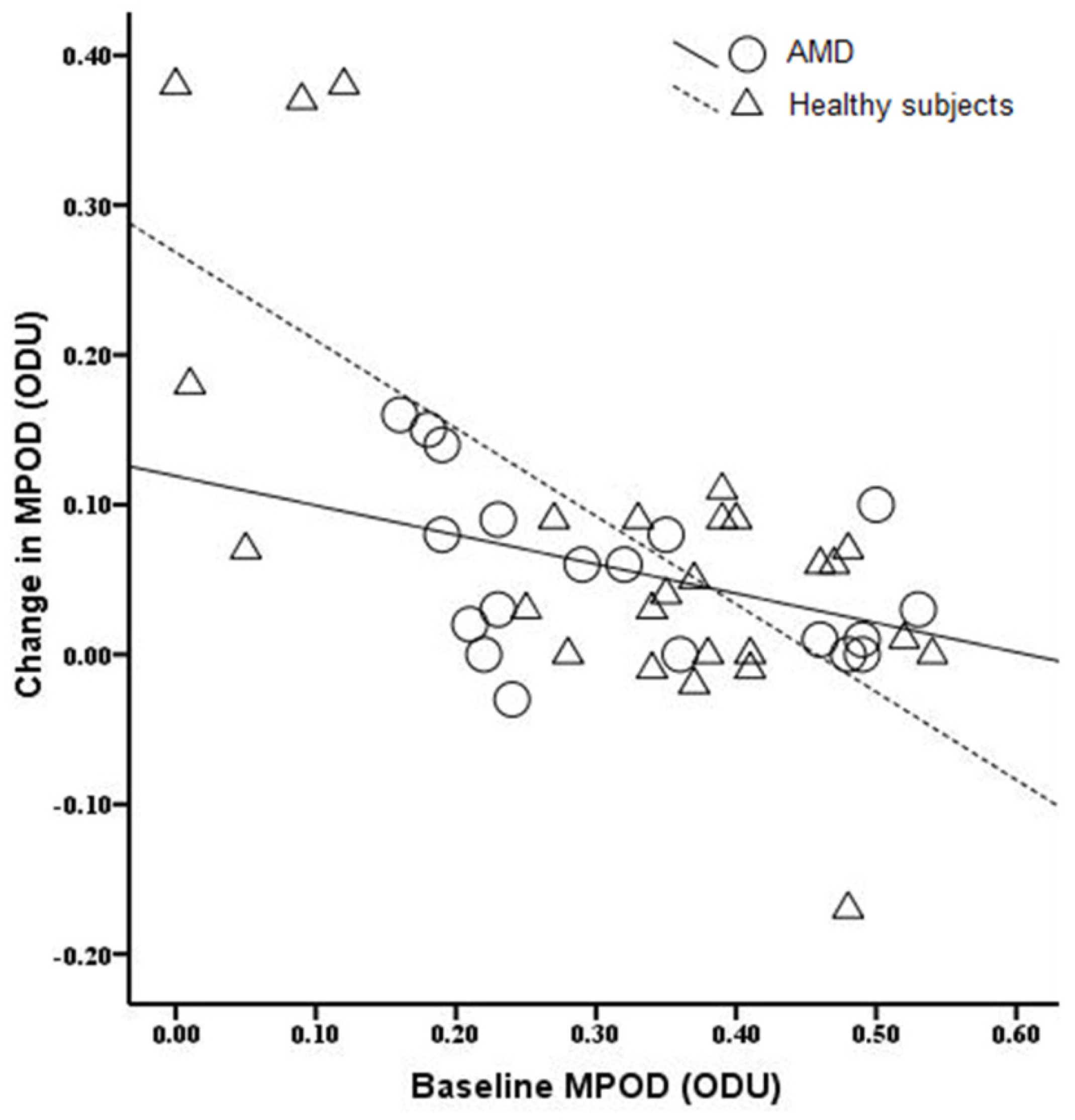
3.5. The Relationship between Baseline MPOD Levels and the Change in MPOD
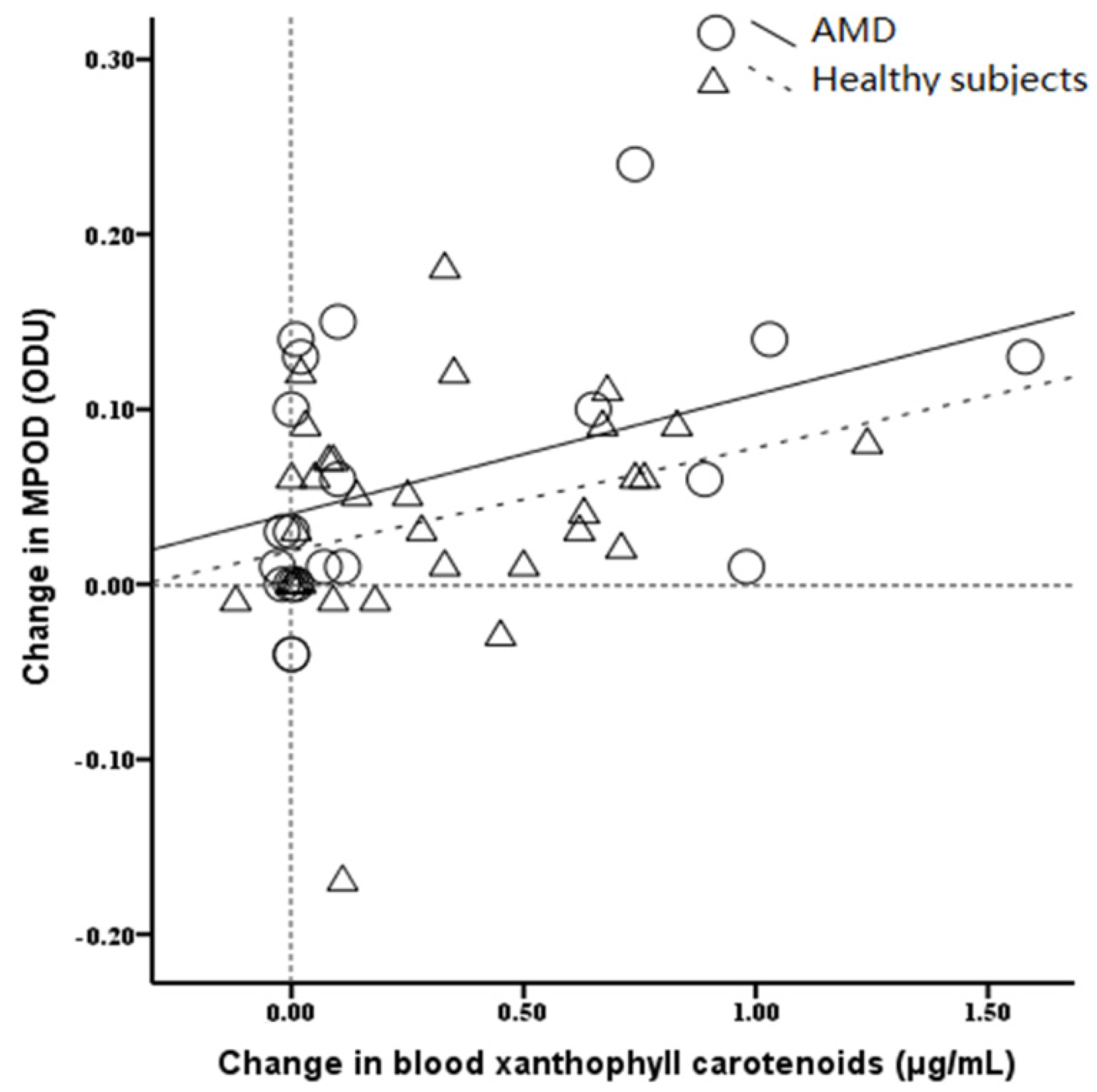
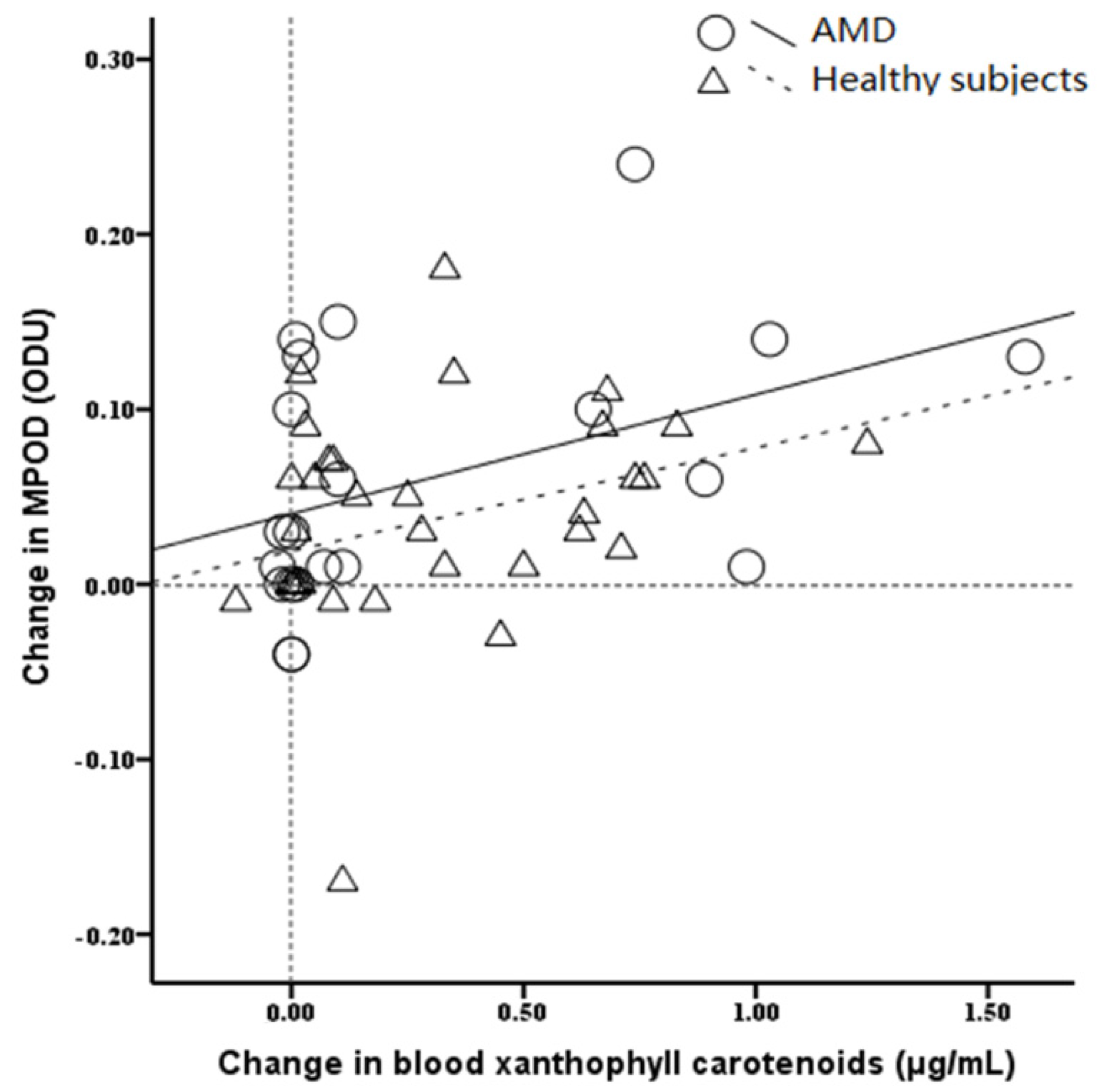
3.6. The Relationship between Blood Xanthophyll Carotenoids Concentration and the Change in MPOD
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Trevino, R.; Kynn, M.G. Macular function surveillance revisited. Optometry 2008, 79, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Koo, E.; Neuringer, M.; SanGiovanni, J.P. Macular xanthophylls lipoprotein-related genes and age-related macular degeneration. Am. J. Clin. Nutr. 2014, 100, 336S–346S. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Landrum, J.T.; Fernandez, L.; Tarsis, S.L. Analysis of the macular pigment by HPLC: Retinal distribution and age study. Invest. Ophthalmol. Vis. Sci. 1988, 29, 843–849. [Google Scholar] [PubMed]
- Meagher, K.A.; Thurnham, D.I.; Beatty, S.; Howard, A.N.; Connolly, E.; Cummins, W.; Nolan, J.M. Serum response to supplemental macular carotenoids in subjects with and without age-related macular degeneration. Br. J. Nutr. 2013, 110, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Ahmed, F.; Bernstein, P.S. Studies on the singlet oxygen scavenging mechanism of human macular pigment. Arch. Biochem. Biophys. 2010, 504, 56–60. [Google Scholar] [CrossRef] [PubMed]
- Thurnham, D.I.; Nolan, J.M.; Howard, A.N.; Beatty, S. Macular response to supplementation with differing xanthophyll formulations in subjects with and without age-related macular degeneration. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 1231–1243. [Google Scholar] [CrossRef] [PubMed]
- Connolly, E.E.; Beatty, S.; Thurnham, D.I.; Loughman, J.; Howard, A.N.; Stack, J.; Nolan, J.M. Augmentation of macular pigment following supplementation with all three macular carotenoids: An exploratory study. Curr. Eye Res. 2010, 35, 335–351. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Landrum, J.T.; Dixon, Z.; Chen, Y.; Llerena, C.M. Lutein and Zeaxanthin in the Eyes, Serum and Diet of Human Subjects. Exp. Eye Res. 2000, 71, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, H.; Howells, O.; Eperjesi, F. The role of macular pigment assessment in clinical practice: A review. Clin. Exp. Optom. 2010, 93, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Sabour-Pickett, S.; Beatty, S.; Connolly, E.; Loughman, J.; Stack, J.; Howard, A.; Klein, R.; Klein, B.E.; Meuer, S.M.; Myers, C.; et al. Supplementation with three different macular carotenoid formulations in patients with early age-related macular degeneration. Retina 2014, 34, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Barker, F.M.; Snodderly, D.M.; Johnson, E.J.; Schalch, W.; Koepcke, W.; Gerss, J.; Neuringer, M. Nutritional manipulation of primate retinas, V: Effects of lutein, zeaxanthin, and n-3 fatty acids on retinal sensitivity to blue-light-induced damage. Invest. Ophthalmol. Vis. Sci. 2011, 52, 3934–3942. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.M.; Stack, J.; O’Donovan, O.; Loane, E.; Beatty, S. Risk factors for age-related maculopathy are associated with a relative lack of macular pigment. Exp. Eye Res. 2007, 84, 61–74. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.M.; Akkali, M.C.; Loughman, J.; Howard, A.N.; Beatty, S. Macular carotenoid supplementation in subjects with atypical spatial profiles of macular pigment. Exp. Eye Res. 2012, 101, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Hammond, B.R.; Johnson, E.J.; Russell, R.M.; Krinsky, N.I.; Yeum, K.J.; Edwards, R.B.; Snodderly, D.M. Dietary modification of human macular pigment density. Invest. Ophthalmol. Vis. Sci. 1997, 38, 1795–1801. [Google Scholar] [PubMed]
- Berrow, E.J.; Bartlett, H.E.; Eperjesi, F.; Gibson, J.M. The effects of a lutein-based supplement on objective and subjective measures of retinal and visual function in eyes with age-related maculopathy-a randomised controlled trial. Br. J. Nutr. 2013, 109, 2008–2014. [Google Scholar] [CrossRef] [PubMed]
- Ho, L.; van Leeuwen, R.; Witteman, J.C.; van Duijn, C.M.; Uitterlinden, A.G.; Hofman, A.; de Jong, P.T.; Vingerling, J.R.; Klaver, C.C. Reducing the genetic risk of age-related macular degeneration with dietary antioxidants, zinc, and ω-3 fatty acids: The Rotterdam study. Arch. Ophthalmol. 2011, 129, 758–766. [Google Scholar] [CrossRef] [PubMed]
- Connolly, E.E.; Beatty, S.; Loughman, J.; Howard, A.N.; Louw, M.S.; Nolan, J.M. Supplementation with all three macular carotenoids: Response, stability, and safety. Invest. Ophthalmol. Vis. Sci. 2011, 52, 9207–9217. [Google Scholar] [CrossRef] [PubMed]
- Joachim, N.; Mitchell, P.; Rochtchina, E.; Tan, A.G.; Wang, J.J. Incidence and progression of reticular drusen in age-related macular degeneration: Findings from an older Australian cohort. Ophthalmology 2014, 121, 917–925. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Yan, S.F.; Huang, Y.M.; Lu, X.R.; Qian, F.; Pang, H.L.; Xu, X.R.; Zou, Z.Y.; Dong, P.C.; Xiao, X.; et al. Effect of lutein and zeaxanthin on macular pigment and visual function in patients with early age-related macular degeneration. Ophthalmology 2012, 119, 2290–2297. [Google Scholar] [CrossRef] [PubMed]
- Trieschmann, M.; Beatty, S.; Nolan, J.M.; Hense, H.W.; Heimes, B.; Austermann, U.; Fobker, M.; Pauleikhoff, D. Changes in macular pigment optical density and serum concentrations of its constituent carotenoids following supplemental lutein and zeaxanthin: The LUNA study. Exp. Eye Res. 2007, 84, 718–728. [Google Scholar] [CrossRef] [PubMed]
- Richer, S.; Devenport, J.; Lang, J.C. LAST II: Differential temporal responses of macular pigment optical density in patients with atrophic age-related macular degeneration to dietary supplementation with xanthophylls. Optometry 2007, 78, 213–219. [Google Scholar] [CrossRef] [PubMed]
- Loughman, J.; Nolan, J.M.; Howard, A.N.; Connolly, E.; Meagher, K.; Beatty, S. The impact of macular pigment augmentation on visual performance using different carotenoid formulations. Invest. Ophthalmol. Vis. Sci. 2012, 53, 7871–7880. [Google Scholar] [CrossRef] [PubMed]
- Yonova-Doing, E.; Hysi, P.G.; Venturini, C.; Williams, K.M.; Nag, A.; Beatty, S.; Liew, S.H.; Gilbert, C.E.; Hammond, C.J. Candidate gene study of macular response to supplemental lutein and zeaxanthin. Exp. Eye Res. 2013, 115, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Trieschmann, M.; van Kuijk, F.J.; Alexander, R.; Hermans, P.; Luthert, P.; Bird, A.C.; Pauleikhoff, D. Macular pigment in the human retina: Histological evaluation of localization and distribution. Eye (Lond.) 2008, 22, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Thurnham, D.I.; Howard, A.N. Studies on meso-zeaxanthin for potential toxicity and mutagenicity. Food Chem. Toxicol. 2013, 59, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Howells, O.; Eperjesi, F.; Bartlett, H. Measuring macular pigment optical density in vivo: A review of techniques. Graefe’s Arch. Clin. Exp. Ophthalmol. 2011, 249, 315–347. [Google Scholar] [CrossRef] [PubMed]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Begg, C.B.; Mazumdar, M. Operating characteristics of a rank correlation test for publication bias. Biometrics 1994, 50, 1088–1101. [Google Scholar] [CrossRef] [PubMed]
- Weigert, G.; Kaya, S.; Pemp, B.; Sacu, S.; Lasta, M.; Werkmeister, R.M.; Dragostinoff, N.; Simader, C.; Garhöfer, G.; Schmidt-Erfurth, U.; et al. Effects of lutein supplementation on macular pigment optical density and visual acuity in patients with age-related macular degeneration. Invest. Ophthalmol. Vis. Sci. 2011, 52, 8174–8178. [Google Scholar] [CrossRef] [PubMed]
- Arnold, C.; Jentsch, S.; Dawczynski, J.; Böhm, V. Age-related macular degeneration: Effects of a short-term intervention with an oleaginous kale extract-a pilot study. Nutrition 2013, 29, 1412–1417. [Google Scholar] [CrossRef] [PubMed]
- García-Layana, A.; Recalde, S.; Alamán, A.S.; Robredo, P.F. Effects of lutein and docosahexaenoic acid supplementation on macular pigment optical density in a randomized controlled trial. Nutrients 2013, 5, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Dawczynski, J.; Jentsch, S.; Schweitzer, D.; Hammer, M.; Lang, G.E.; Strobel, J. Long term effects of lutein, zeaxanthin and omega-3-LCPUFAs supplementation on optical density of macular pigment in AMD patients: The LUTEGA study. Graefe’s Arch. Clin. Exp. Ophthalmol. 2013, 251, 2711–2723. [Google Scholar] [CrossRef] [PubMed]
- Murray, I.J.; Makridaki, M.; van der Veen, R.L.; Carden, D.; Parry, N.R.; Berendschot, T.T. Lutein supplementation over a one-year period in early AMD might have a mild beneficial effect on visual acuity: The CLEAR study. Invest. Ophthalmol. Vis. Sci. 2013, 54, 1781–1788. [Google Scholar] [CrossRef] [PubMed]
- Arnold, C.; Winter, L.; Fröhlich, K.; Jentsch, S.; Dawczynski, J.; Jahreis, G.; Böhm, V. Macular xanthophylls and ω-3 long-chain polyunsaturated fatty acids in age-related macular degeneration: A randomized trial. JAMA Ophthalmol. 2013, 131, 564–572. [Google Scholar]
- Huang, Y.M.; Dou, H.L.; Huang, F.F.; Xu, X.R.; Zou, Z.Y.; Lu, X.R.; Lin, X.M. Changes following supplementation with lutein and zeaxanthin in retinal function in eyes with early age-related macular degeneration: A randomised, double-blind, placebo-controlled trial. Br. J. Ophthalmol. 2015, 99, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Kvansakul, J.; Rodriguez-Carmona, M.; Edgar, D.F.; Barker, F.M.; Köpcke, W.; Schalch, W.; Barbur, J.L. Supplementation with the carotenoids lutein or zeaxanthin improves human visual performance. Ophthalmic. Physiol. Opt. 2006, 26, 362–371. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Landrum, J.T.; Cao, Y.; Howard, A.N.; Alvarez-Calderon, F. Macular pigment response to a supplement containing meso-zeaxanthin, lutein and zeaxanthin. Nutr. Metab. (Lond.) 2007, 4, 12. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.J.; Chung, H.Y.; Caldarella, S.M.; Snodderly, D.M. The influence of supplemental lutein and docosahexaenoic acid on serum, lipoproteins, and macular pigmentation. Am. J. Clin. Nutr. 2008, 87, 1521–1529. [Google Scholar] [PubMed]
- Bone, R.A.; Landrum, J.T. Dose-dependent response of serum lutein and macular pigment optical density to supplementation with lutein esters. Arch. Biochem. Biophys. 2010, 504, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.M.; Loughman, J.; Akkali, M.C.; Stack, J.; Scanlon, G.; Davison, P.; Beatty, S. The impact of macular pigment augmentation on visual performance in normal subjects: COMPASS. Vis. Res. 2011, 51, 459–469. [Google Scholar] [CrossRef] [PubMed]
- Landrum, J.; Bone, R.; Mendez, V.; Valenciaga, A.; Babino, D. Comparison of dietary supplementation with lutein diacetate and lutein: A pilot study of the effects on serum and macular pigment. Acta Biochim. Pol. 2012, 59, 167–169. [Google Scholar] [PubMed]
- Yao, Y.; Qiu, Q.H.; Wu, X.W.; Cai, Z.Y.; Xu, S.; Liang, X.Q. Lutein supplementation improves visual performance in Chinese drivers: 1-year randomized, double-blind, placebo-controlled study. Nutrition 2013, 29, 958–964. [Google Scholar] [CrossRef] [PubMed]
- Bovier, E.R.; Hammond, B.R. A randomized placebo-controlled study on the effects of lutein and zeaxanthin on visual processing speed in young healthy subjects. Arch. Biochem. Biophys. 2015, 572, 54–57. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.M.; Power, R.; Stringham, J.; Dennison, J.; Stack, J.; Kelly, D.; Moran, R.; Akuffo, K.; Corcoran, L.; Beatty, S. Enrichment of Macular Pigment Enhances Contrast Sensitivity in Subjects Free of Retinal Disease: Central Retinal Enrichment Supplementation Trials—Report 1. Invest. Ophthalmol. Vis. Sci. 2016, 57, 3429–3439. [Google Scholar] [CrossRef] [PubMed]
- Beatty, S.; Murray, I.J.; Henson, D.B.; Carden, D.; Koh, H.H.; Boulton, M.E. Macular pigment and risk for age-related macular degeneration in subjects from a Northern European population. Invest. Ophthalmol. Vis. Sci. 2001, 42, 439–446. [Google Scholar] [PubMed]
- Neuringer, M.; Sandstrom, M.M.; Johnson, E.J.; Snodderly, D.M. Nutritional manipulation of primate retinas, I: Effects of lutein or zeaxanthin supplements on serum and macular pigment in xanthophyll-free rhesus monkeys. Invest. Ophthalmol. Vis. Sci. 2004, 45, 3234–3243. [Google Scholar] [CrossRef] [PubMed]
- Hammond, B.R.; Fletcher, L.M.; Roos, F.; Wittwer, J.; Schalch, W. A Double-Blind, Placebo-Controlled Study on the Effects of Lutein and Zeaxanthin on Photostress Recovery, Glare Disability, and Chromatic Contrast. Invest. Ophthalmol. Vis. Sci. 2014, 55, 8583–8589. [Google Scholar] [CrossRef] [PubMed]
- Lien, E.L.; Hammond, B.R. Nutritional influences on visual development and function. Prog. Retin. Eye Res. 2011, 30, 188–203. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.; Mrejen, S.; Fung, A.T.; Marsiglia, M.; Loh, B.K.; Spaide, R.F. Retinal pigment epithelial cell loss assessed by fundus autofluorescence imaging in neovascular age-related macular degeneration. Ophthalmology 2013, 120, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Thomson, L.R.; Toyoda, Y.; Delori, F.C.; Garnett, K.M.; Wong, Z.Y.; Nichols, C.R.; Cheng, K.M.; Craft, N.E.; Dorey, C.K. Long term dietary supplementation with zeaxanthin reduces photoreceptor death in light-damaged Japanese quail. Exp. Eye Res. 2002, 75, 529–542. [Google Scholar] [CrossRef] [PubMed]
- Yu, C.C.; Nandrot, E.F.; Dun, Y.; Finnemann, S.C. Dietary antioxidants prevent age-related retinal pigment epithelium actin damage and blindness in mice lacking αvβ5 integrin. Free Radic. Biol. Med. 2012, 52, 660–670. [Google Scholar] [CrossRef] [PubMed]
- Bone, R.A.; Landrum, J.T.; Mayne, S.T.; Gomez, C.M.; Tibor, S.E.; Twaroska, E.E. Macular pigment in donor eyes with and without AMD: A case-control study. Invest. Ophthalmol. Vis. Sci. 2001, 42, 235–240. [Google Scholar] [PubMed]
- Biesalski, H.K.; Aggett, P.J.; Anton, R.; Bernstein, P.S.; Blumberg, J.; Heaney, R.P.; Henry, J.; Nolan, J.M.; Richardson, D.P.; van Ommen, B.; et al. 26th Hohenheim Consensus Conference, September 11, 2010 Scientific substantiation of health claims: Evidence-based nutrition. Nutrition 2011, 27, S1–S20. [Google Scholar] [CrossRef] [PubMed]
- Puell, M.C.; Palomo-Alvarez, C.; Barrio, A.R.; Gómez-Sanz, F.J.; Pérez-Carrasco, M.J. Relationship between macular pigment and visual acuity in eyes with early age-related macular degeneration. Acta. Ophthalmol. 2013, 91, e298–e303. [Google Scholar] [CrossRef] [PubMed]
- Johnson, E.J.; Maras, J.E.; Rasmussen, H.M.; Tucker, K.L. Intake of lutein and zeaxanthin differ with age, sex and ethnicity. J. Am. Diet. Assoc. 2010, 110, 1357–1362. [Google Scholar] [CrossRef] [PubMed]
- Trumbo, P.R.; Ellwood, K.C. Lutein and zeaxanthin intakes and risk of age-related macular degeneration and cataracts: An evaluation using the Food and Drug Administration’s evidence-based review system for health claims. Am. J. Clin. Nutr. 2006, 84, 971–974. [Google Scholar] [PubMed]
- Granado, F.; Blázquez, S.; Olmedilla, B. Changes in carotenoid intake from fruit and vegetables in the Spanish population over the period 1964–2004. Public Health Nutr. 2007, 10, 1018–1023. [Google Scholar] [CrossRef] [PubMed]
- Wisniewska, A.; Subczynski, W.K. Distribution of macular xanthophylls between domains in a model of photoreceptor outer segment membranes. Free Radic. Biol. Med. 2006, 41, 1257–1265. [Google Scholar] [CrossRef] [PubMed]
- Vachali, P.P.; Besch, B.M.; Gonzalez-Fernandez, F.; Bernstein, P.S. Carotenoids as possible interphotoreceptor retinoid-binding protein (IRBP) ligands: A surface plasmon resonance (SPR) based study. Arch. Biochem. Biophys. 2013, 539, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Bhosale, P.; Li, B.; Sharifzadeh, M.; Gellermann, W.; Frederick, J.M.; Tsuchida, K.; Bernstein, P.S. Purification and partial characterization of a lutein-binding protein from human retina. Biochemistry 2009, 48, 4798–4807. [Google Scholar] [CrossRef] [PubMed]
- Schalch, W.; Cohn, W.; Barker, F.M.; Köpcke, W.; Mellerio, J.; Bird, A.C.; Robson, A.G.; Fitzke, F.F.; van Kuijk, F.J. Xanthophyll accumulation in the human retina during supplementation with lutein or zeaxanthin-the LUXEA (LUtein Xanthophyll Eye Accumulation) study. Arch. Biochem. Biophys. 2007, 458, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Bhosale, P.; Bernstein, P.S. Vertebrate and invertebrate carotenoid-binding proteins. Arch. Biochem. Biophys. 2007, 458, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.M.; Beatty, S.; Meagher, K.A.; Howard, A.N.; Kelly, D.; Thurnham, D.I. Verification of Meso-Zeaxanthin in Fish. J. Food Process Technol. 2014, 5, 335. [Google Scholar] [CrossRef] [PubMed]
- Beaty, S.; Boulton, M.; Henson, D.; Koh, H.H.; Murray, I.J. Macular pigment and age related macular degeneration. Br. J. Ophthalmol. 1999, 83, 867–877. [Google Scholar] [CrossRef]
- Akuffo, K.O.; Beatty, S.; Stack, J.; Dennison, J.; O’Regan, S.; Meagher, K.A.; Peto, T.; Nolan, J. Central Retinal Enrichment Supplementation Trials (CREST): Design and methodology of the CREST randomized controlled trials. Ophthalmic. Epidemiol. 2014, 21, 111–123. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors (Year) | Study Participants | Trial Duration | No. of Groups | Lnterventions | Measurement Method for MPOD | Follow-Up Rates (%) | Quality Score * |
|---|---|---|---|---|---|---|---|
| Trieschmann et al. (2007) [20] | 130 AMD patients aged (71.4 ± 7.6) years in Germany | 6 months | 2 | 12 mg lutein and 1 mg zeaxanthin combined with other antioxidants; placebo | Fundus autofluorescence | 94.6 | 3 |
| Richer et al. (2007) [21] | 90 AMD patients aged (74.1 ± 7.5) years in the USA | 12 months | 3 | 10 mg lutein; 10 mg lutein combined with other antioxidants; placebo | HFP | 84.4 | 5 |
| Weigert et al. (2011) [30] | 126 AMD patients aged (71.6 ± 8.6) years in Austria | 6 months | 2 | 20 mg lutein daily in months 1 to 3 and 10 mg lutein daily in months 4 to 6; placebo | Spectral fundus reflectance | 87.3 | 3 |
| Arnold C et al. (2013) [31] | 20 AMD patients aged (66.0 ± 8.0) years in Germany | 10 weeks | 2 | 10 mg lutein plus 3 mg zeaxanthin; placebo | VISUCAM NM/FA | 100.0 | 5 |
| García-Layana et al. (2013) [32] | 44 AMD patients aged (68.5 ± 8.5) years in Spain | 12 months | 2 | 12 mg lutein plus 0.6 mg zeaxanthin combined with other antioxidants; placebo | HFP | NR | 3 |
| Dawczynski et al. (2013) [33] | 172 AMD patients aged (70.0 ± 10.0) years in Germany | 12 months | 3 | 10 mg lutein, 1 mg zeaxanthin combined with other antioxidants; 20 mg lutein, 2 mg zeaxanthin combined with other antioxidants; placebo | VISUCAM NM/FA | 84.3 | 3 |
| Murray et al. (2013) [34] | 72 AMD patients aged (70.5 ± 8.7) years in UK | 12 months | 2 | 10 mg lutein daily; placebo | HFP | 86.9 | 5 |
| Arnold C et al. (2013) [35] | 172 AMD patients aged (69.0 ± 10.0) years in Germany | 12 months | 3 | 10 mg lutein plus 1 mg zeaxanthin combined with other antioxidants; 20 mg lutein plus 2 mg zeaxanthin combined with other antioxidants; placebo | VISUCAM NM/FA | 84.3 | 5 |
| Huang et al. (2015) [36] | 112 AMD patients aged (69.1 ± 7.4) years in China | 24 months | 4 | 10 mg lutein; 20 mg lutein; 10 mg lutein plus 10 mg zeaxanthin; placebo | Fundus autofluorescence | 96.4 | 5 |
| Kvansakul et al. (2005) [37] | 92 healthy men in UK | 12 months | 4 | 10 mg lutein; 10 mg zeaxanthin; 10 mg lutein plus 10 mg zeaxanthin in months 1 to 6 and 20 mg lutein; 20 mg zeaxanthin; 10 mg lutein plus 10 mg zeaxanthin in months 7 to 12; placebo | MAP | 79.3 | 4 |
| Bone et al. (2007) [38] | 19 healthy subjects in the USA | 120 days | 2 | 14.9 mg of meso-zeaxanthin, 5.5 mg of lutein, and 1.4 mg of zeaxanthin; placebo | HFP | NR | 3 |
| Johnson et al. (2008) [39] | 57 healthy women in the USA | 4 months | 3 | 12 mg lutein plus 0.5 mg zeaxanthin;12 mg lutein plus 800 mg DHA; placebo | HFP | 86.0 | 4 |
| Bone et al. (2010) [40] | 100 healthy subjects in the USA | 140 days | 4 | 5 mg lutein; 10 mg lutein; 20 mg lutein; placebo | HFP | 87.0 | 4 |
| Connolly et al. (2011) [17] | 44 healthy subjects in Ireland | 6 months | 2 | 10.6 mg meso-zeaxanthin, 5.9 mg lutein, and 1.2 mg zeaxanthin; placebo | HFP | 79.5 | 5 |
| Nolan et al. (2011) [41] | 121 healthy subjects in Ireland | 12 months | 2 | 12 mg lutein, 1 mg zeaxanthin combined with other antioxidants; placebo | HFP | 62.8 | 4 |
| Landrum et al. (2012) [42] | 30 healthy subjects in the USA | 24 weeks | 3 | 20 mg lutein diacetate; 20 mg lutein; placebo | HFP | NR | 3 |
| Loughman et al. (2012) [22] | 36 healthy subjects in Ireland | 6 months | 3 | 20 mg lutein plus 2 mg zeaxanthin; 10 mg meso-zeaxanthin, 10 mg lutein plus 2 mg zeaxanthin; placebo | HFP | 88.9 | 5 |
| Yao et al. (2013) [43] | 120 healthy subjects in China | 12 months | 2 | 20 mg lutein; placebo | HFP | 82.5 | 4 |
| Bovier et al. (2015) [44] | 102 healthy subjects in the USA | 4 months | 3 | 20 mg zeaxanthin; 8 mg lutein plus 26 mg zeaxanthin combined with other antioxidants; placebo | HFP | 67.6 | 4 |
| Nolan et al. (2016) [45] | 105 healthy subjects in Ireland | 12 months | 2 | 10 mg lutein, 2 mg zeaxanthin, and 10 mg meso-zeaxanthin; placebo | Autofluorescence | 80.0 | 5 |
| Subgroup | AMD Patients | Healthy Populations | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| N | WMD | 95% CI | Pz | Ph | N | WMD | 95% CI | Pz | Ph | |
| Dose of supplement | ||||||||||
| >10 mg | 10 | 0.07 | 0.04, 0.12 | <0.001 | 0.93 | 15 | 0.12 | 0.09, 0.15 | <0.001 | 0.01 |
| ≤10 mg | 4 | 0.09 | −0.07, 0.19 | 0.40 | 4 | 0.05 | 0.03, 0.07 | 0.02 | ||
| Duration of intervention | ||||||||||
| ≥12 months | 11 | 0.17 | 0.09, 0.24 | <0.001 | 0.05 | 6 | 0.07 | 0.04, 0.10 | <0.001 | 0.83 |
| <12 months | 3 | 0.05 | 0.01, 0.09 | <0.001 | 13 | 0.08 | 0.03, 0.13 | <0.001 | ||
| Mean age | ||||||||||
| >70 years | 7 | 0.06 | 0.03, 0.09 | <0.001 | 0.85 | |||||
| ≤70 years | 7 | 0.11 | 0.02, 0.19 | <0.001 | ||||||
| Zeaxanthin | ||||||||||
| With | 9 | 0.07 | 0.04, 0.11 | <0.001 | 0.60 | 11 | 0.09 | 0.06, 0.13 | <0.001 | 0.21 |
| Without | 5 | 0.08 | 0.07, 0.09 | 0.41 | 8 | 0.08 | 0.03, 0.08 | 0.03 | ||
| Meso-zeaxanthin | ||||||||||
| With | 4 | 0.13 | 0.05, 0.22 | 0.001 | 0.02 | |||||
| Without | 15 | 0.06 | 0.03, 0.08 | <0.001 | ||||||
| Other antioxidants | ||||||||||
| With | 7 | 0.08 | 0.04, 0.13 | <0.001 | 0.97 | 3 | 0.10 | 0.05, 0.15 | 0.99 | 0.55 |
| Without | 7 | 0.08 | 0.04, 0.13 | <0.001 | 16 | 0.07 | 0.05, 0.10 | <0.001 | ||
| Geographic area | ||||||||||
| Europe | 9 | 0.08 | 0.04, 0.11 | <0.001 | 0.80 | 8 | 0.06 | 0.03, 0.09 | <0.001 | 0.50 |
| Asia | 3 | 0.10 | 0.05, 0.15 | 0.27 | 1 | 0.11 | 0.06, 0.16 | - | ||
| USA | 2 | 0.12 | −0.15, 0.38 | 0.97 | 10 | 0.09 | 0.02, 0.15 | <0.001 | ||
| Methods | ||||||||||
| Objective | 10 | 0.09 | 0.07, 0.12 | <0.001 | 0.37 | |||||
| Psychophysical | 4 | 0.05 | −0.15, 0.24 | <0.001 | ||||||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ma, L.; Liu, R.; Du, J.H.; Liu, T.; Wu, S.S.; Liu, X.H. Lutein, Zeaxanthin and Meso-zeaxanthin Supplementation Associated with Macular Pigment Optical Density. Nutrients 2016, 8, 426. https://doi.org/10.3390/nu8070426
Ma L, Liu R, Du JH, Liu T, Wu SS, Liu XH. Lutein, Zeaxanthin and Meso-zeaxanthin Supplementation Associated with Macular Pigment Optical Density. Nutrients. 2016; 8(7):426. https://doi.org/10.3390/nu8070426
Chicago/Turabian StyleMa, Le, Rong Liu, Jun Hui Du, Tao Liu, Shan Shan Wu, and Xiao Hong Liu. 2016. "Lutein, Zeaxanthin and Meso-zeaxanthin Supplementation Associated with Macular Pigment Optical Density" Nutrients 8, no. 7: 426. https://doi.org/10.3390/nu8070426
APA StyleMa, L., Liu, R., Du, J. H., Liu, T., Wu, S. S., & Liu, X. H. (2016). Lutein, Zeaxanthin and Meso-zeaxanthin Supplementation Associated with Macular Pigment Optical Density. Nutrients, 8(7), 426. https://doi.org/10.3390/nu8070426