Fructose Containing Sugars at Normal Levels of Consumption Do Not Effect Adversely Components of the Metabolic Syndrome and Risk Factors for Cardiovascular Disease

Abstract
:1. Introduction
2. Experimental Section
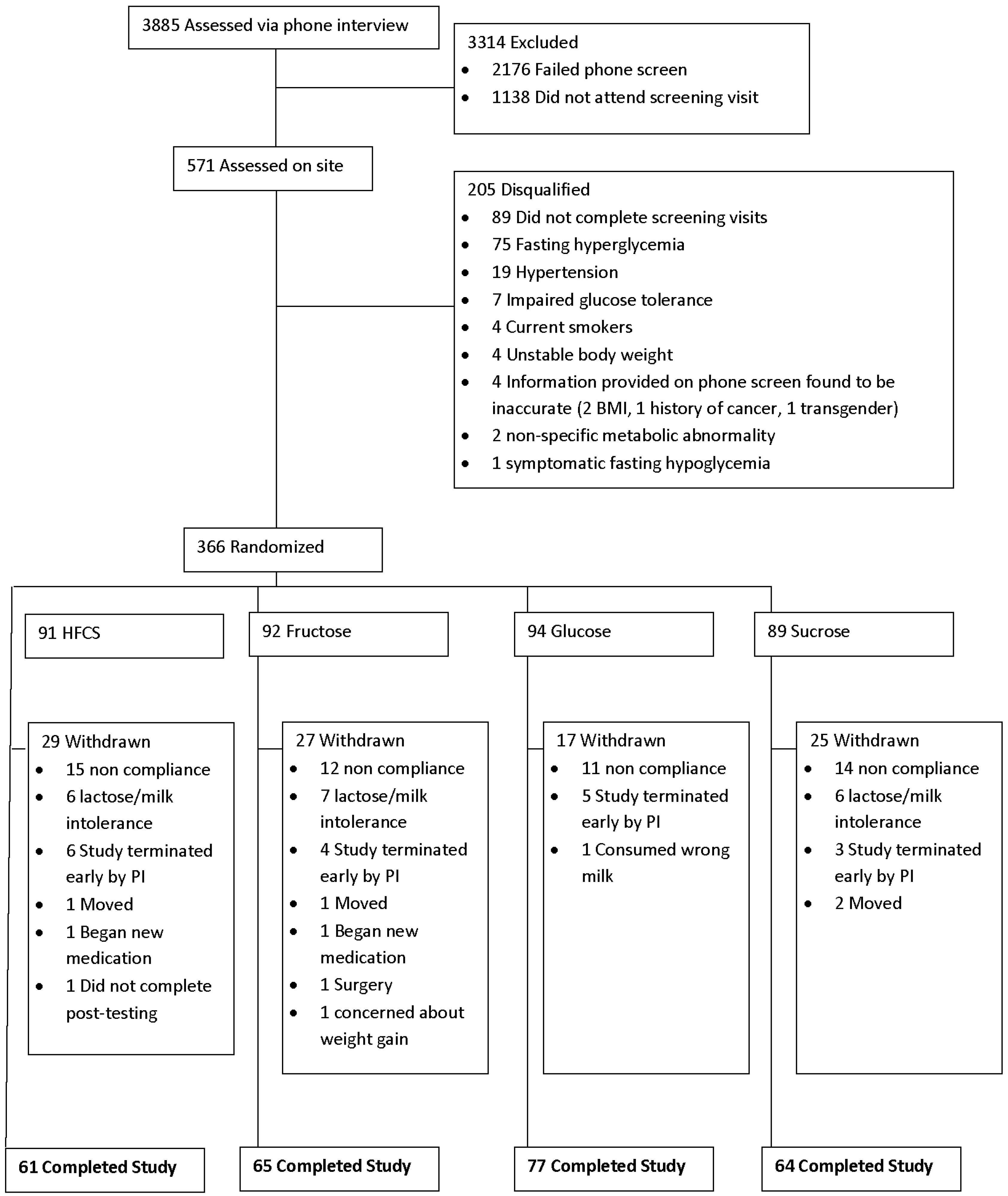
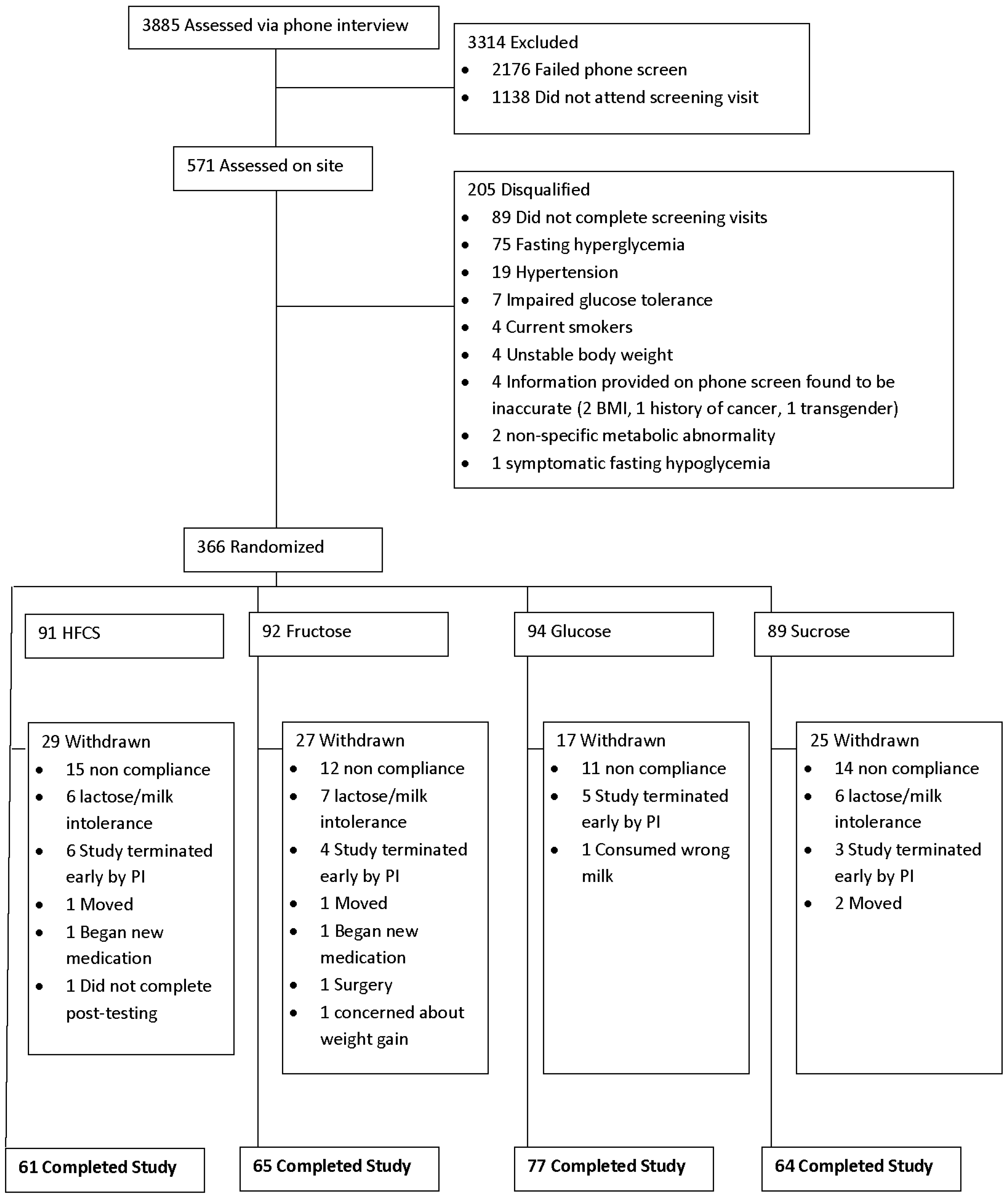
2.1. Study Design and Participants
2.2. Dietary Plans
2.3. Statistical Analysis
3. Results
3.1. Baseline Subject Characteristics
3.2. Dietary Intake
3.3. Components of the Metabolic Syndrome
3.4. Cardiovascular Disease Risk Factors
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. The Global Burden of Disease: 2004 Update; World Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart Disease and Stroke Statistics—2013 Update: A Report from the American Heart Association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [PubMed]
- Reaven, G.M. Banting Lecture. Role of insulin resistance in human disease. Diabetes 1988, 37, 1595–1607. [Google Scholar] [CrossRef] [PubMed]
- DeFronzo, R.A.; Ferrannini, E. Insulin resistance: A multifaceted syndrome responsible for NIDDM, obesity, hypertension, dyslipidemia, and atherosclerotic heart disease. Diabetes Care 1991, 14, 173–194. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, N.M. The deadly quartet. Upper-body obesity, glucose intolerance, hypertriglyceridemia, and hypertension. Arch. Intern. Med. 1989, 149, 1514–1520. [Google Scholar] [CrossRef] [PubMed]
- Whaley-Connell, A.; Johnson, M.; Sowers, J.R. Aldosterone: Role in the cardiometabolic syndrome and resistant hypertension. Prog. Cardiovasc. Dis. 2010, 52, 401–409. [Google Scholar] [CrossRef] [PubMed]
- Groop, L.; Ortho-Melander, M. The dysmetabolic syndrome. Intern. Med. 2001, 250, 105–120. [Google Scholar] [CrossRef]
- National Cholesterol Education Program. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar]
- Lichtenstein, A.H.; Appel, L.J.; Brands, M.; Carnethon, M.; Daniels, S.; Franch, H.A.; Franklin, B.; Kris-Etherton, P.; Harris, W.S.; Howard, B.; et al. Diet and Lifestyle Recommendations Revision 2006: A Scientific Statement from the American Heart Association Nutrition Committee. Circulation 2006, 114, 82–96. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.K.; Appel, L.J.; Brands, M.; Howard, B.V.; Lefevre, M.; Lustig, R.H.; Sacks, F.; Steffen, L.M.; Wylie-Rosett, J. Dietary Sugars Intake and Cardiovascular Health: A Scientific Statement from the American Heart Association. Circulation 2009, 120, 1011–1020. [Google Scholar] [CrossRef] [PubMed]
- Bray, G.A. Fructose and risk of cardiometabolic disease. Curr. Atheroscler. Rep. 2012, 14, 570–578. [Google Scholar] [CrossRef] [PubMed]
- Johnson, R.J.; Segal, M.S.; Sautin, Y.; Nakagawa, T.; Feig, D.I.; Kang, D.; Gersch, M.S.; Benner, S.; Sanchez-Lozada, L.G. Potential role of sugar (fructose) in the epidemic of hypertension, obesity and the metabolic syndrome, diabetes, kidney disease, and cardiovascular disease. Am. J. Clin. Nutr. 2007, 86, 899–906. [Google Scholar] [PubMed]
- Bray, G.A. Fructose: Pure, White, and Deadly? Fructose, by any other name, is a health hazard. J. Diabetes Sci. Technol. 2010, 4, 1003–1007. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Hu, F.B. Sugars, Obesity and Chronic Diseases in Adults in Dietary Sugars and Health; Goran, M.I., Tappy, L., Lê, K.-A., Eds.; CRC Press: Boca Raton, FL, USA, 2014. [Google Scholar]
- Bray, G.A.; Popkin, B.M. Calorie-sweetened beverages and fructose: What have we learned 10 years later. Pediatr. Obes. 2013, 8, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Lê, K.A.; Tappy, L. Metabolic effects of fructose. Curr. Opin. Clin. Nutr. Metab. Care 2006, 9, 469–475. [Google Scholar] [CrossRef] [PubMed]
- Havel, P.J. Dietary fructose: Implications for dysregulation of energy homeostasis and lipid/carbohydrate metabolism. Nutr. Rev. 2005, 63, 133–157. [Google Scholar] [CrossRef] [PubMed]
- Gross, L.S.; Li, S.; Ford, E.S.; Liu, S. Increased consumption of refined carbohydrates and the epidemic of type 2 diabetes in the United States: An ecologic assessment. Am. J. Clin. Nutr. 2004, 79, 774–779. [Google Scholar] [PubMed]
- Elliott, S.S.; Keim, N.L.; Stern, J.S.; Teff, K.; Havel, P.J. Fructose, weight gain, and the insulin resistance syndrome. Am. J. Clin. Nutr. 2002, 76, 911–922. [Google Scholar] [PubMed]
- Dhingra, R.; Sullivan, L.; Jacques, P.F.; Wang, T.J.; Fox, C.S.; Meigs, J.B.; D’Agostino, R.B.; Gaziano, J.M.; Vasan, R.S. Soft drink consumption and risk of developing cardiometabolic risk factors and the metabolic syndrome in middle-aged adults in the community. Circulation 2007, 116, 480–488; correction e557. [Google Scholar] [CrossRef] [PubMed]
- Aeberli, I.; Hochuli, M.; Gerber, P.A.; Sze, L.; Murer, S.B.; Tappy, L.; Spinas, G.A.; Berneis, K. Moderate amounts of fructose consumption impair insulin sensitivity in healthy young men: A randomized controlled trial. Diabetes Care 2013, 36, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Wells, H.F.; Buzby, J.C. Dietary Assessment of Major Trends in US Food Consumption, 1970–2005; US Department of Agriculture, Economic Research Service: Washington, DC, USA, 2008.
- Welsh, J.A.; Sharma, A.J.; Grellinger, L.; Vos, M.B. Consumption of added sugars is decreasing in the United States. Am. J. Clin. Nutr. 2011, 94, 726–734. [Google Scholar] [CrossRef] [PubMed]
- Stanhope, K.L.; Bremer, A.A.; Medici, V.; Nakajima, K.; Ito, Y.; Nakana, T.; Chen, G.; Fong, T.H.; Lee, V.; Menorca, R.I.; et al. Consumption of fructose and high fructose corn syrup increase postprandial triglycerides, LDL-cholesterol, and apolipoprotein-B in young men and women. J. Clin. Endocrinol. Metab. 2011, 96, E1596–E1605. [Google Scholar] [CrossRef] [PubMed]
- Marckmann, P. Dietary treatment of thrombogenic disorders related to the metabolic syndrome. Br. J. Nutr. 2000, 83 (Suppl. S1), S121–S126. [Google Scholar] [CrossRef] [PubMed]
- Maersk, M.; Belza, A.; Stodkilde-Jorgensen, H.; Ringgaard, S.; Chabanova, E.; Thomsen, H.; Pedersen, S.B.; Astrup, A.; Richelsen, B. Sucrose-sweetened beverages increase fat storage in the liver, muscle, and visceral fat depot: A 6-mo randomized intervention study. Am. J. Clin. Nutr. 2012, 95, 283–289. [Google Scholar] [CrossRef] [PubMed]
- Stanhope, K.L.; Havel, P.J. Fructose consumption: Potential mechanisms for its effects to increase visceral adiposity and induce dyslipidemia and insulin resistance. Curr. Opin. Lipidol. 2008, 19, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Feig, D.I.; Soletsky, B.; Johnson, R.J. Effect of allopurinol on blood pressure of adolescents with newly diagnosed essential hypertension: A randomized trial. JAMA 2008, 300, 924–932. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.; Choi, H.K.; Lustig, R.H.; Hsu, C.Y. Sugar-sweetened beverages, serum uric acid, and blood pressure in adolescents. J. Pediatr. 2009, 154, 807–813. [Google Scholar] [CrossRef] [PubMed]
- Bremer, A.A.; Auinger, P.; Byrd, R.S. Relationship between insulin resistance-associated metabolic parameters and anthropometric measurements with sugar-sweetened beverage intake and physical activity levels in US adolescents: Findings from the 1999–2004 National Health and Nutrition Examination Survey. Arch. Pediatr. Adolesc. Med. 2009, 163, 328–335. [Google Scholar] [PubMed]
- Liu, S.; Manson, J.E.; Buring, J.E.; Stampfer, M.J.; Willett, W.C.; Ridker, P.M. Relation between a diet with a high glycemic load and plasma concentrations of high-sensitivity C-reactive protein in middle-aged women. Am. J. Clin. Nutr. 2002, 75, 492–498. [Google Scholar] [PubMed]
- Price, K.D.; Price, C.S.; Reynolds, R.D. Hyperglycemia-induced ascorbic acid deficiency promotes endothelial dysfunction and the development of atherosclerosis. Atherosclerosis 2001, 158, 1–12. [Google Scholar] [CrossRef]
- Ceriello, A.; Bortolotti, N.; Crescentini, A.; Motz, E.; Lizzio, S.; Russo, A.; Ezsol, Z.; Tonutti, L.; Taboga, C. Antioxidant defenses are reduced during the oral glucose tolerance test in normal and non-insulin-dependent diabetic subjects. Eur. J. Clin. Investig. 1998, 28, 329–333. [Google Scholar] [CrossRef]
- Ma, S.W.; Tomlinson, B.; Benzie, I.F. A study of the effect of oral glucose loading on plasma oxidant: Antioxidant balance in normal subjects. Eur. J. Nutr. 2005, 44, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Stanhope, K.L.; Schwarz, J.M.; Keim, N.L.; Griffen, S.C.; Bremer, A.A.; Graham, J.L.; Hatcher, B.; Cox, C.L.; Dyachenko, A.; Zhang, W.; et al. Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans. J. Clin. Investig. 2009, 119, 1322–1334. [Google Scholar] [CrossRef] [PubMed]
- Teff, K.; Grudziak, J.; Townsend, R.; Dunn, T.N.; Grant, R.W.; Adams, S.H.; Keim, N.L.; Cummings, B.P.; Stanhope, K.L.; Havel, P.J. Endocrine and metabolic effects of consuming fructose- and glucose-sweetened beverages with meals in obese men and women: Influence of insulin resistance on plasma triglyceride responses. J. Clin. Endocrinol. Metab. 2009, 94, 1562–1569. [Google Scholar] [CrossRef] [PubMed]
- Marriott, B.P.; Olsho, L.; Hadden, L.; Connor, P. Intake of Added Sugars and Selected Nutrients in the United States, National Health and Nutrition Examination Survey (NHANES) 2003–2006. Crit. Rev. Food Sci. Nutr. 2010, 50, 228–258. [Google Scholar] [CrossRef] [PubMed]
- Chiavaroli, L.; Mirrahimi, A.; De Souza, R.J.; Cozma, A.I.; Ha, V.; Wang, D.D.; Yu, M.E. Does fructose consumption elicit a dose-response effect on fasting triglycerides? A systematic review and meta-regression of controlled feeding trials. Can. J. Diabetes 2012, 36, S37. [Google Scholar] [CrossRef]
- Wang, D.D.; Sievenpiper, J.L.; de Souza, R.J.; Cozma, A.I.; Chiavaroli, L.; Ha, V.; Mirrahimi, A.; Carleton, A.J.; Di Buono, M.; Jenkins, A.L.; et al. Effect of fructose on postprandial triglycerides: A systematic review and meta-analysis of controlled feeding trials. Atherosclerosis 2014, 232, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Lowndes, J.; Sinnett, S.; Pardo, S.; Nguyen, V.; Melanson, K.; Yu, Z.; Lowther, B.; Rippe, J. The effect of normally consumed amounts of sucrose or high fructose corn syrup on lipid profiles, body composition and related parameters in overweight/obese subjects. Nutrients 2014, 6, 1128–1144. [Google Scholar] [CrossRef] [PubMed]
- Lowndes, J.; Sinnett, S.; Yu, Z.; Rippe, J. The effects of fructose-containing sugars on weight, body composition and cardiometabolic risk factors when consumed at up to the 90th percentile population consumption level for fructose. Nutrients 2014, 6, 3153–3168. [Google Scholar] [CrossRef] [PubMed]
- Angelopoulos, T.J.; Lowndes, J.; Sinnett, S.; Rippe, J.M. Fructose containing sugars do not raise blood pressure or uric acid at normal levels of human consumption. J. Clin. Hypertens. 2014, 17, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Wienen, W.J.; Shallenberger, R.S. Influence of acid and temperature on the rate of inversion of sucrose. Food Chem. 1988, 29, 51–55. [Google Scholar] [CrossRef]
- Hellerstein, M.K. Carbohydrate-induced hypertriglyceridemia: Modifying factors and implications for cardiovascular risk. Curr. Opin. Lipidol. 2002, 3, 33–40. [Google Scholar] [CrossRef]
- Mensink, R.P.; Zock, P.L.; Kester, A.D.; Katan, M.B. Effects of dietary fatty acids and carbohydrates on the ratio of serum total to HDL cholesterol and on serum lipids and apolipoproteins: A meta-analysis of 60 controlled trials. Am. J. Clin. Nutr. 2003, 77, 1146–1155. [Google Scholar] [PubMed]
- Appel, L.J.; Sacks, F.M.; Carey, V.J.; Obarzanek, E.; Swain, J.F.; Miller, E.R., III; Conlin, P.R.; Erlinger, T.P.; Rosner, B.A.; Laranjo, N.M.; et al. Effects of protein, monounsaturated fat, and carbohydrate intake on blood pressure and serum lipids: Results of the OmniHeart randomized trial. JAMA 2005, 294, 2455–2464. [Google Scholar] [CrossRef] [PubMed]
- Chong, M.F.; Fielding, B.A.; Frayn, K.N. Mechanisms for the acute effect of fructose of postprandial lipemia. Am. J. Clin. Nutr. 2007, 85, 11511–11520. [Google Scholar]
- Fried, S.K.; Rao, S.P. Sugars, hypertriglyceridemia, and cardiovascular disease. Am. J. Clin. Nutr. 2003, 78, 873S–880S. [Google Scholar] [PubMed]
- Bantle, J.P.; Raatz, S.K.; Thomas, W.; Georgopoulos, A. Effects of dietary fructose of plasma lipids in healthy subjects. Am. J. Clin. Nutr. 2000, 72, 1128–1134. [Google Scholar] [PubMed]
- Parks, E.J.; Skokan, L.E.; Timlin, M.T.; Dingfelder, C.S. Dietary sugars stimulate fatty acid synthesis in adults. J. Nutr. 2008, 138, 1039–1046. [Google Scholar] [PubMed]
- Sievenpiper, J.L.; de Souza, R.J.; Cozma, A.I.; Chiavaroli, L.; Ha, V.; Mirrahimi, A. Fructose vs. glucose and metabolism: Do the metabolic differences matter? Curr. Opin. Lipidol. 2014, 25, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Van Buul, V.J.; Tappy, L.; Brouns, F.J.P.H. Misconceptions about fructose-containing sugars and their role in the obesity epidemic. Nutr. Res. Rev. 2014. [Google Scholar] [CrossRef] [PubMed]
- Sievenpiper, J.L.; Tappy, L.; Brouns, F. Fructose as a Driver of Diabetes: An Incomplete View of the Evidence. Mayo Clin. Proc. 2015, 90, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Sievenpiper, J.L.; de Souza, R.J.; Mirrahimi, A.; Yu, M.E.; Carleton, A.J.; Beyene, J.; Chiavaroli, L.; Di Buono, M.; Jenkins, A.L.; Leiter, L.A.; et al. Effect of fructose on body weight in controlled feeding trials: A systematic review and meta-analysis. Ann. Intern. Med. 2012, 156, 291–304. [Google Scholar] [CrossRef] [PubMed]
- Livesey, G.; Taylor, R. Fructose consumption and consequences for glycation, plasma triacylglycerol, and body weight: Meta-analyses and meta-regression models of intervention studies. Am. J. Clin. Nutr. 2008, 88, 1419–1437. [Google Scholar] [PubMed]
- Cozma, A.I.; Sievenpiper, J.L.; de Souza, R.J.; Chiavaroli, L.; Ha, V.; Wang, D.D.; Mirrahimi, A.; Yu, M.E.; Carleton, A.J.; Di Buono, M.; et al. Effect of fructose on glycemic control in diabetes: A systematic review and meta-analysis of controlled feeding trials. Diabetes Care 2012, 35, 1611–1620. [Google Scholar] [CrossRef] [PubMed]
- Ha, V.; Sievenpiper, J.L.; de Souza, R.J.; Chiavaroli, L.; Wang, D.D.; Cozma, A.I.; Mirrahimi, A.; Yu, M.E.; Carleton, A.J.; Dibuono, M.; et al. Effect of fructose on blood pressure: A systematic review and meta-analysis of controlled feeding trials. Hypertension 2012, 59, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Van der Schaaf, M.R.; Koomans, H.A.; Joles, J.A. Dietary sucrose does not increase twenty-four-hour ambulatory blood pressure in patients with either essential hypertension or polycystic kidney disease. J. Hypertens. 1999, 17, 453–454. [Google Scholar] [CrossRef] [PubMed]
- Araujo, I.C.; Andrade, R.P.; Santos, F.; Soares, E.S.; Yokota, R.; Mostarda, C.; Fiorino, P.; de Angelis, K.; Irigoyen, M.C. Early developmental exposure to high fructose intake in rats with NaCl stimulation causes cardiac damage. Eur. J. Nutr. 2016, 55, 83–91. [Google Scholar] [CrossRef] [PubMed]
- De Angelis, K.; Senador, D.D.; Mostarda, C.; Irigoyen, M.C.; Morris, M. Sympathetic overactivity precedes metabolic dysfunction in a fructose model of glucose intolerance in mice. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2012, 302, R950–R957. [Google Scholar] [CrossRef] [PubMed]
- Jadali, A.; Ghazizadeh, S. Protein kinase D is implicated in the reversible commitment to differentiation in primary cultures of mouse keratinocytes. J. Biol. Chem. 2010, 285, 23387–23397. [Google Scholar] [CrossRef] [PubMed]
- Stanhope, K.L.; Griffen, S.C.; Bair, B.R.; Swarbrick, M.M.; Keim, N.L.; Havel, P.J. Twenty-four-hour endocrine and metabolic profiles following consumption of high-fructose corn syrup-, sucrose-, fructose-, and glucose-sweetened beverages with meals. Am. J. Clin. Nutr. 2008, 87, 1194–1203. [Google Scholar] [PubMed]
- Sievenpiper, J.L.; de Souza, R.J.; Kendall, C.W.; Jenkins, D.J. Is fructose a story of mice but not men? J. Am. Diet. Assoc. 2011, 111, 219–220; author reply 220–212. [Google Scholar] [CrossRef] [PubMed]
- Dugan, C.E.; Barona, J.; Fernandez, M.L. Increased Dairy Consumption Differentially Improves Metabolic Syndrome Markers in Male and Female Adults. Metab. Syndr. Relat. Disord. 2013, 12, 62–69. [Google Scholar] [CrossRef] [PubMed]
- Laughlin, M.R.; Bantle, J.P.; Havel, P.J.; Parks, E.; Klurfeld, D.M.; Teff, K.; Maruvada, P. Clinical research strategies for fructose metabolism. Adv. Nutr. 2014, 5, 248–259. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| HFCS | Fructose | Glucose | Sucrose | All | ||
|---|---|---|---|---|---|---|
| Age (Years) | Baseline | 36.32 ± 10.72 | 38.65 ± 12.19 | 36.10 ± 12.06 | 39.83 ± 13.19 | 37.66 ± 12.11 |
| Weight (Lbs) | Baseline | 162.09 ± 26.12 | 166.61 ± 30.90 | 159.13 ± 24.88 | 161.66 ± 27.26 | 162.28 ± 27.28 |
| Week 10 | 164.05 ± 27.28 | 168.15 ± 32.52 | 160.44 ± 24.81 | 164.66 ± 27.99 | 164.15 ± 28.14 ** | |
| Energy Intake (Kcal) | Baseline | 1929.4 ±733.7 | 2065.8 ± 722.9 | 1978.6 ± 644.3 | 2069.5 ± 711.6 | 2011.8 ± 708.2 |
| Week 10 | 2390.1 ± 700.7 | 2195.4 ± 581.7 | 2182.2 ± 636.6 | 2277.5 ± 668.8 | 2254.6 ± 647.6 ** | |
| Calories from Fat (%) | Baseline | 32.6 ± 7.5 | 33.4 ± 12.4 | 33.7 ± 7.4 | 33.7 ± 6.5 | 33.7 ± 8.7 |
| Week 10 | 26.0 ± 5.5 | 28.1 ± 5.8 | 28.6 ± 6.0 | 25.2 ± 5.3 | 27.1 ± 5.8 ** | |
| Calories from Carbohydrate (%) | Baseline | 47.8 ± 9.7 | 51.0 ± 13.5 | 47.8 ± 10.0 | 48.2 ± 7.9 | 48.7 ± 10.5 |
| Week 10 | 55.3 ± 6.6 | 52.3 ± 7.2 †,¥ | 51.7 ± 7.9 † | 57.1 ± 5.7 | 54.0 ± 7.3 ** | |
| Calories from Protein (%) | Baseline | 18.6 ± 6.8 | 18.3 ± 5.5 | 17.4 ± 5.1 | 17.0 ± 4.8 | 17.8 ± 5.5 |
| Week 10 | 18.3 ± 4.0 | 18.9 ± 3.4 | 19.3 ± 4.5 | 16.9 ± 2.7 | 18.4 ± 3.8 |
| HFCS | Fructose | Glucose | Sucrose | All | ||
|---|---|---|---|---|---|---|
| Waist circumference (cm) | Baseline | 80.51 ± 9.29 | 82.06 ± 10.43 | 79.72 ± 8.47 | 81.45 ± 9.73 | 80.88 ± 9.45 |
| Week 10 | 81.31 ± 8.89 | 82.61 ± 10.97 | 79.84 ± 8.47 | 82.38 ± 9.43 | 81.45 ± 9.46 ** | |
| SBP (mmHg) | Baseline | 108.61 ± 9.70 | 107.71 ± 10.51 | 109.17 ± 10.09 | 111.14 ± 10.28 | 109.16 ± 10.17 |
| Week 10 | 107.57 ± 11.29 | 105.49 ± 9.97 | 104.60 ± 9.78 | 107.25 ± 10.55 | 106.13 ± 10.39 ** | |
| DBP (mmHg) | Baseline | 69.48 ± 9.71 | 69.68 ± 8.83 | 68.96 ± 8.33 | 71.14 ± 8.02 | 69.78 ± 8.71 |
| Week 10 | 68.90 ± 10.78 | 67.82 ± 8.91 | 66.12 ± 9.35 | 69.81 ± 9.48 | 68.05 ± 9.68 * | |
| Triglycerides (mg/dL) | Baseline | 98.20 ± 52.46 | 104.29 ± 68.24 | 100.28 ± 56.19 | 103.54 ± 47.56 | 101.56 ± 56.47 |
| Week 10 | 129.03 ± 120.49 † | 106.86 ± 66.13 | 99.86 ± 57.21 | 114.21 ± 60.43 | 111.70 ± 79.14 * | |
| HDL (mg/dL) | Baseline | 53.52 ± 13.07 | 51.45 ± 12.97 | 52.92 ± 13.06 | 52.11 ± 12.11 | 52.51 ± 12.77 |
| Week 10 | 53.08 ± 12.91 | 51.42 ± 12.75 | 52.33 ± 12.91 | 52.67 ± 12.40 | 52.36 ± 12.93 | |
| Glucose (mg/dL) | Baseline | 89.43 ± 6.54 | 90.48 ± 7.07 | 90.66 ± 6.18 | 89.27 ± 6.27 | 90.00 ± 6.50 |
| Week 10 | 88.41 ± 8.24 | 91.65 ± 9.25 | 91.03 ± 6.69 | 91.38 ± 7.09 | 90.66 ± 7.89 |
| HFCS | Fructose | Glucose | Sucrose | All | ||
|---|---|---|---|---|---|---|
| BMI (kg/M2) | Baseline | 26.26 ± 3.16 | 26.52 ± 3.33 | 25.66 ± 3.14 | 26.75 ± 3.51 | 26.27 ± 3.29 |
| Week 10 | 26.58 ± 3.32 | 26.75 ±3.52 | 25.88 ± 3.17 | 27.24 ± 3.62 | 26.58 ± 3.42 ** | |
| Total Cholesterol (mg/dL) | Baseline | 175.33 ± 41.67 | 181.26 ± 40.84 | 176.28 ± 39.35 | 176.75 ± 36.43 | 177.39 ± 39.44 |
| Week 10 | 179.98 ± 41.96 | 180.72 ± 35.53 | 176.16 ± 42.30 | 184.33 ± 39.96 | 180.10 ± 39.98 * | |
| LDL (mg/dL) | Baseline | 100.52 ± 35.18 | 109.20 ± 34.74 | 103.37 ± 34.31 | 103.92 ± 32.80 | 104.27 ± 34.20 |
| Week 10 | 101.13 ± 33.37 | 107.97 ± 30.86 | 103.84 ± 36.68 | 108.78 ± 36.85 | 105.41 ± 34.58 | |
| CRP (mg/L) | Baseline | 1.92 ± 2.10 | 1.74 ± 1.74 | 1.21 ± 1.43 | 1.74 ± 1.78 | 1.63 ± 1.77 |
| Week 10 | 1.86 ± 2.13 | 2.16 ± 2.09 | 1.38 ± 1.70 | 1.71 ± 1.80 | 1.76 ± 1.94 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Angelopoulos, T.J.; Lowndes, J.; Sinnett, S.; Rippe, J.M. Fructose Containing Sugars at Normal Levels of Consumption Do Not Effect Adversely Components of the Metabolic Syndrome and Risk Factors for Cardiovascular Disease. Nutrients 2016, 8, 179. https://doi.org/10.3390/nu8040179
Angelopoulos TJ, Lowndes J, Sinnett S, Rippe JM. Fructose Containing Sugars at Normal Levels of Consumption Do Not Effect Adversely Components of the Metabolic Syndrome and Risk Factors for Cardiovascular Disease. Nutrients. 2016; 8(4):179. https://doi.org/10.3390/nu8040179
Chicago/Turabian StyleAngelopoulos, Theodore J., Joshua Lowndes, Stephanie Sinnett, and James M. Rippe. 2016. "Fructose Containing Sugars at Normal Levels of Consumption Do Not Effect Adversely Components of the Metabolic Syndrome and Risk Factors for Cardiovascular Disease" Nutrients 8, no. 4: 179. https://doi.org/10.3390/nu8040179
APA StyleAngelopoulos, T. J., Lowndes, J., Sinnett, S., & Rippe, J. M. (2016). Fructose Containing Sugars at Normal Levels of Consumption Do Not Effect Adversely Components of the Metabolic Syndrome and Risk Factors for Cardiovascular Disease. Nutrients, 8(4), 179. https://doi.org/10.3390/nu8040179