An Exploratory Investigation of Endotoxin Levels in Novice Long Distance Triathletes, and the Effects of a Multi-Strain Probiotic/Prebiotic, Antioxidant Intervention

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design and Procedures
2.3. Biochemical Assays
2.4. Nutritional Interventions and Diaries
2.5. Training Monitoring, GI Questionnaires and Assessment of Race Times
2.6. Statistical Analyses
3. Results
3.1. Nutrition and Training Data
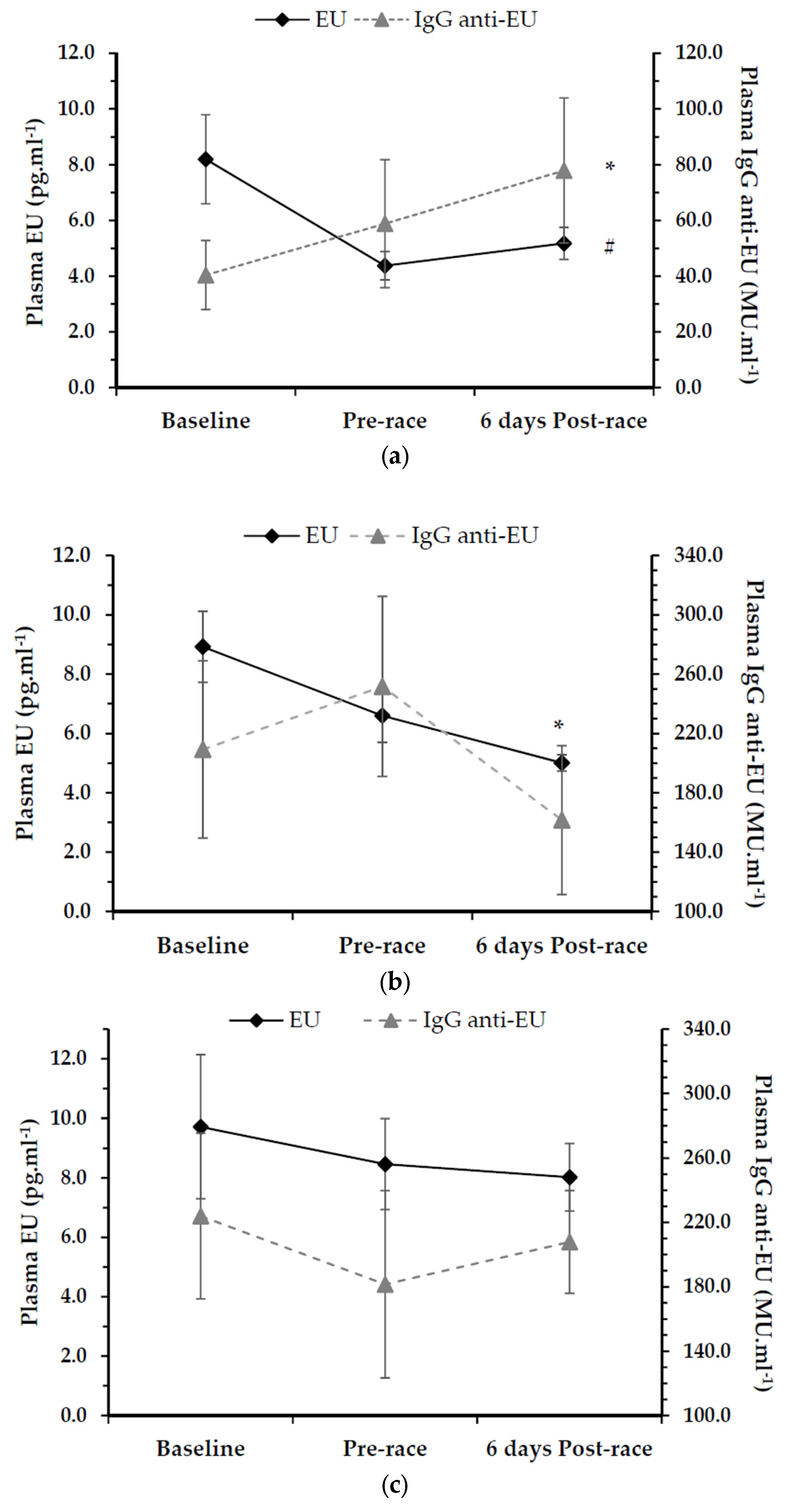
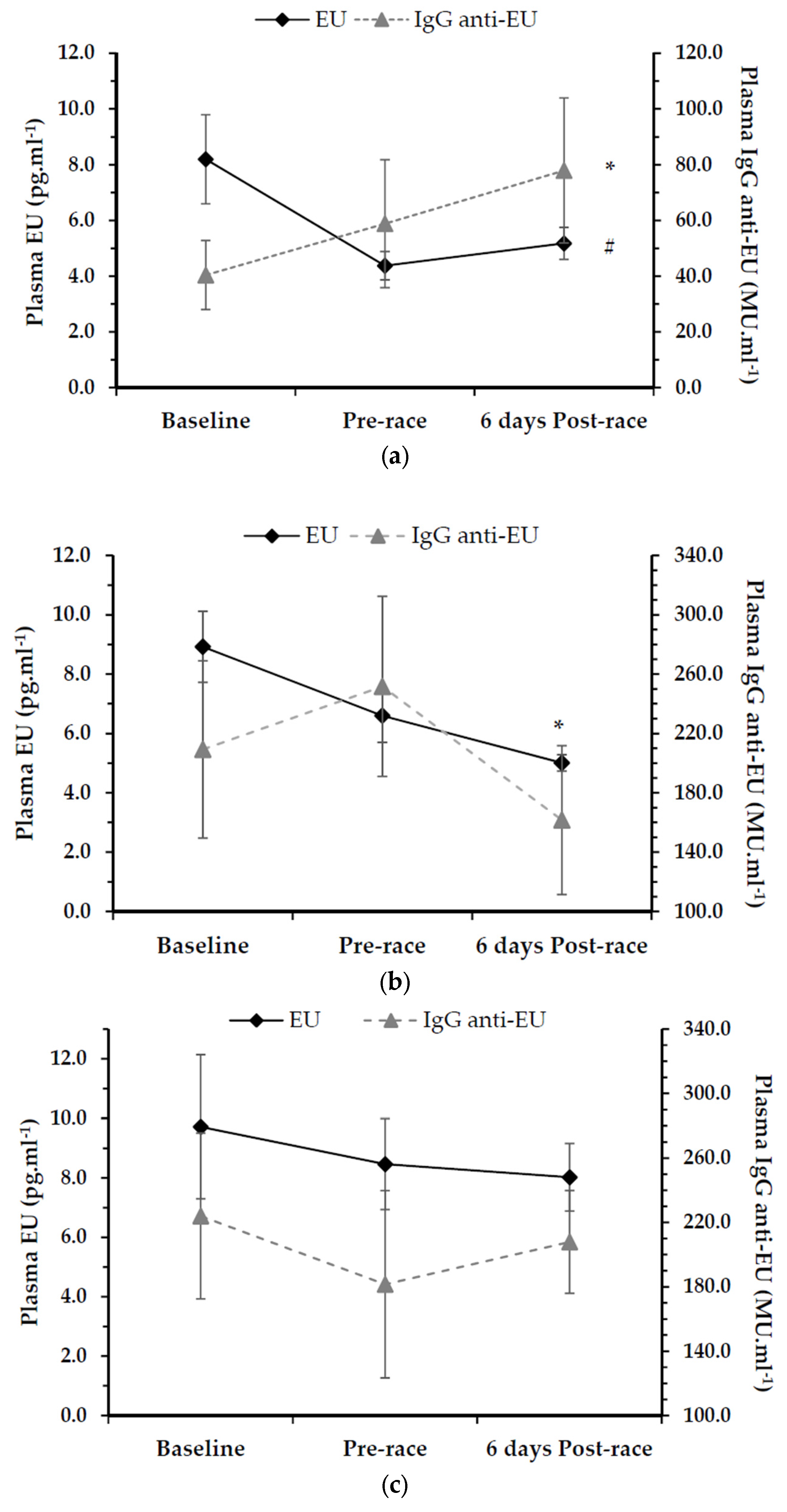
3.2. Endotoxin Unit (EU) Assessment
3.3. IgG Endotoxin-Core Antibody (Anti-EU) Assessment
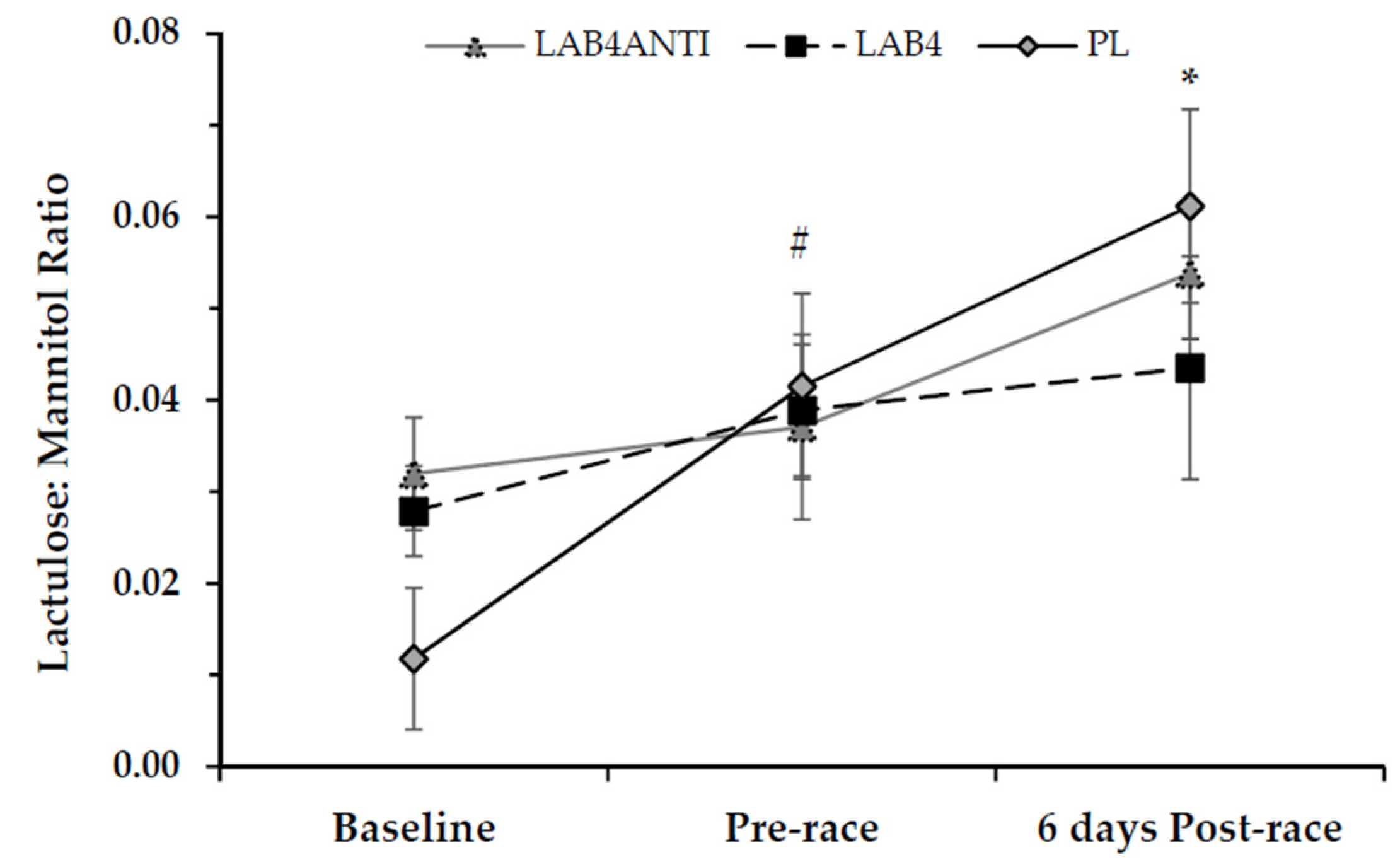
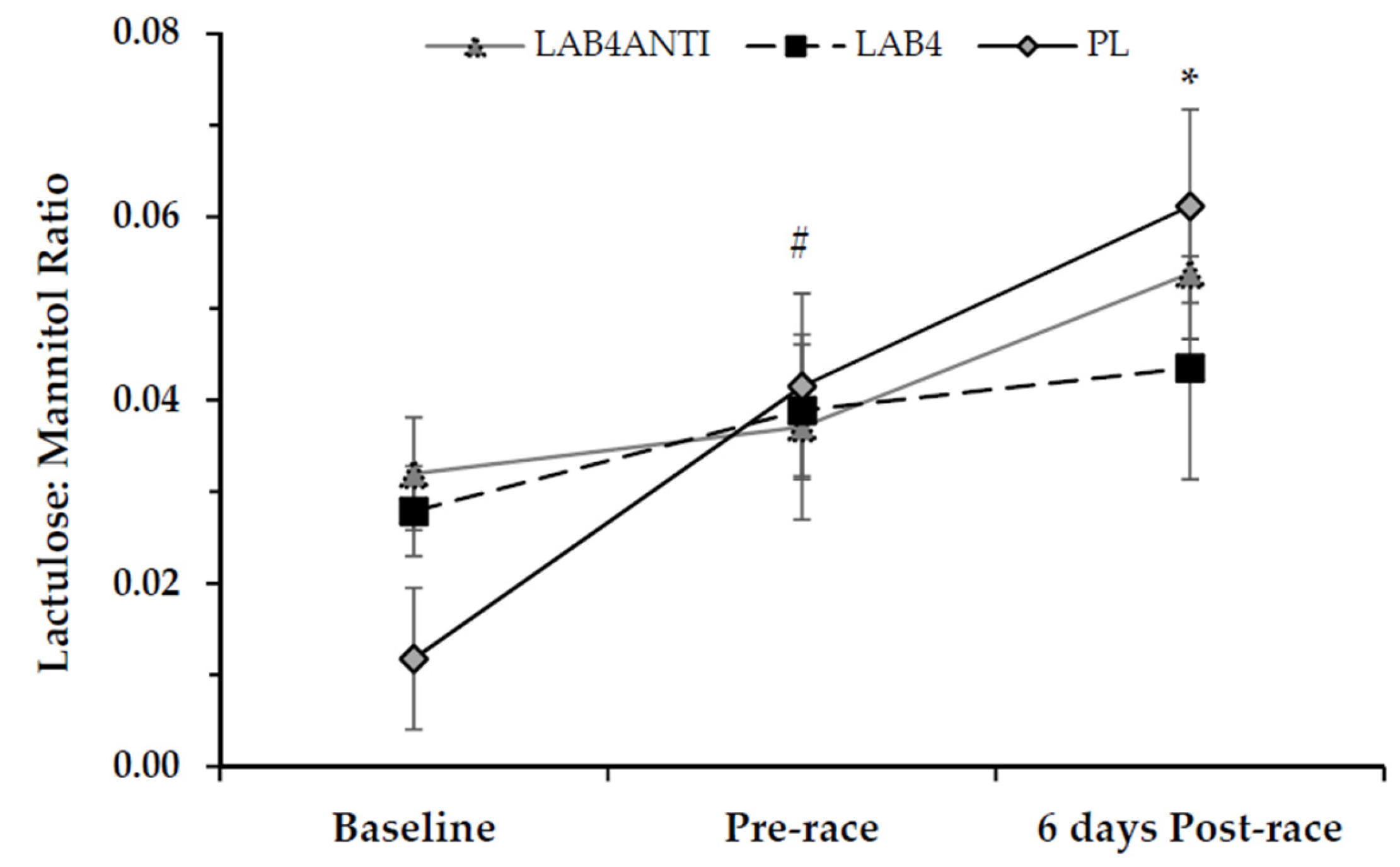
3.4. Intestinal Permeability
3.5. GI Questionnaire
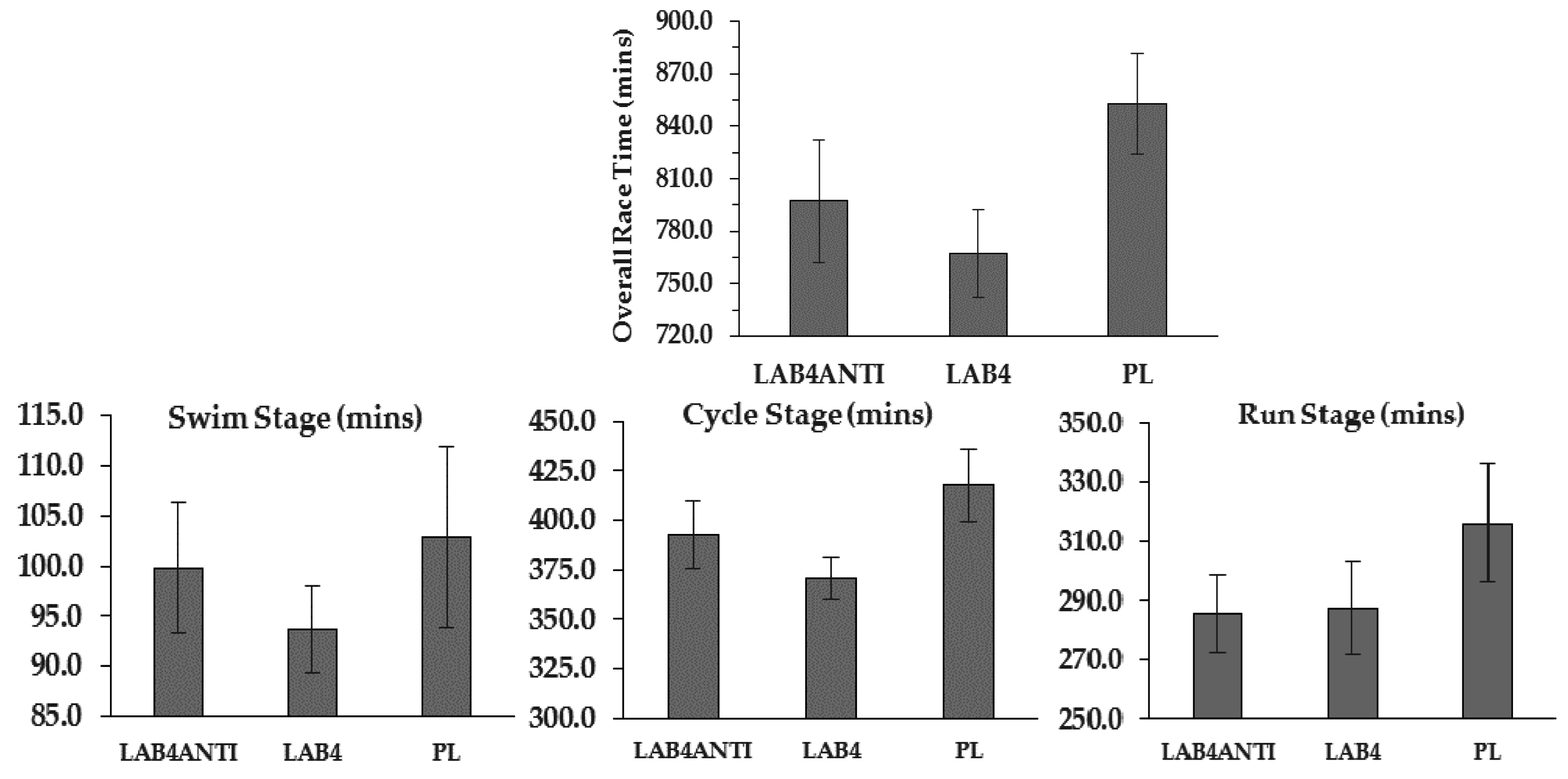
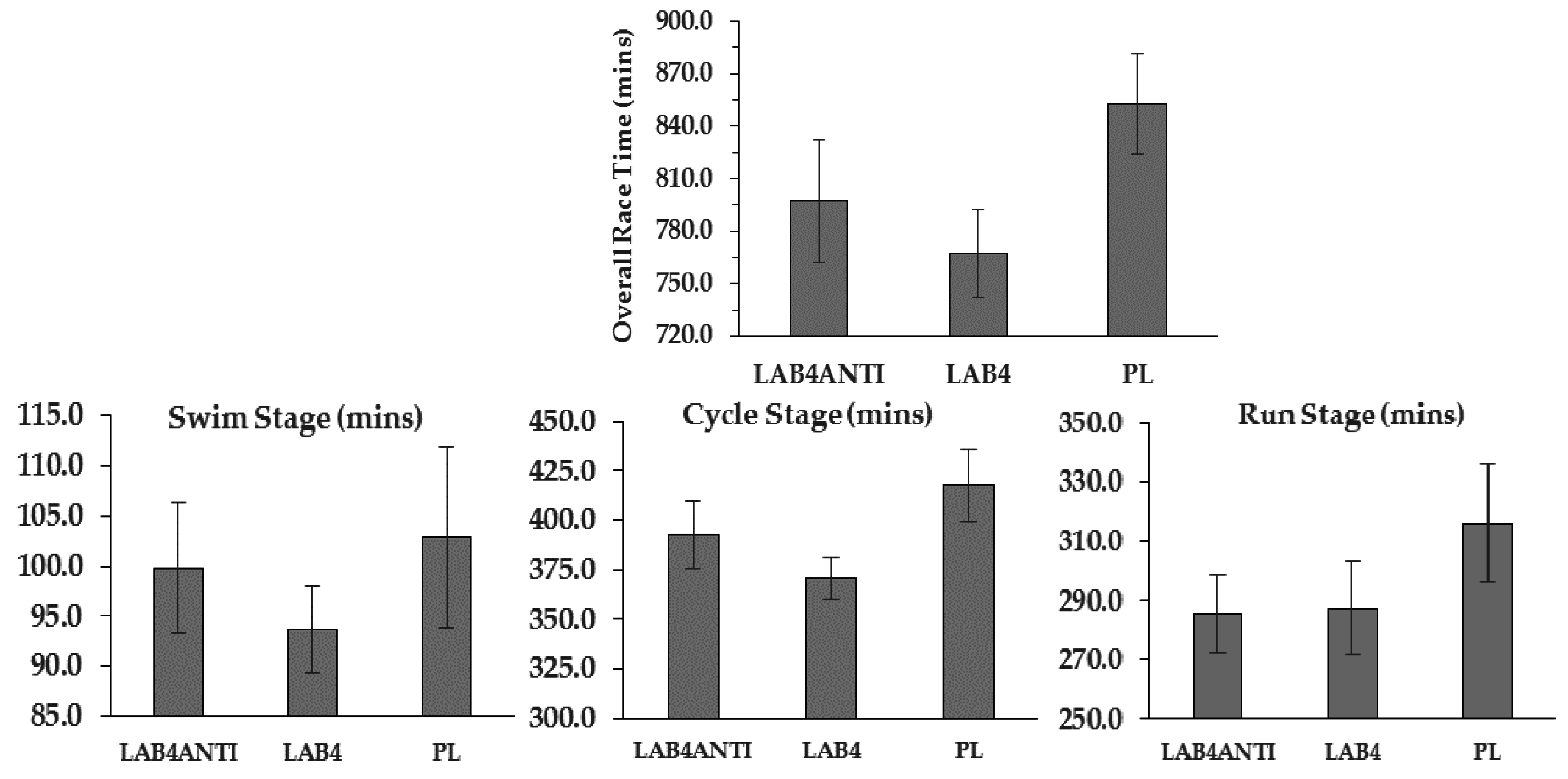
3.6. Race Times
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Da Fonseca-Engelhardt, K.; Knechtle, B.; Rüst, C.A.; Knechtle, P.; Lepers, R.; Rosemann, T. Participation and performance trends in ultra-endurance running races under extreme conditions-’Spartathlon’ versus ‘Badwater’. Extreme Physiol. Med. 2013, 2, 15. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.D. Performance trends in 161-km ultramarathons. Int. J. Sports Med. 2010, 31, 31–37. [Google Scholar] [CrossRef] [PubMed]
- De Oliveira, E.P.; Burini, R.C.; Jeukendrup, A. Gastrointestinal complaints during exercise: Prevalence, etiology, and nutritional recommendations. Sports Med. 2014, 44 (Suppl. 1), S79–S85. [Google Scholar] [CrossRef] [PubMed]
- Ten Haaf, D.S.M.; van der Worp, M.P.; Groenewould, H.M.M.; Leij-Halfwerk, S.; Nijhuis-van der Sanden, M.W.G.; Verbeek, A.L.M.; Staal, J.B. Nutritional indicators for gastrointestinal symptoms in female runners: The ‘Marikenloop study’. BMJ Open 2014, 4, e005780. [Google Scholar] [CrossRef] [PubMed]
- Stuempfle, K.; Hoffman, M.D. Gastrointestinal distress is common during a 161-km ultramarathon. J. Sports Sci. 2015, 33, 1814–1821. [Google Scholar] [CrossRef] [PubMed]
- Van Wick, K.; Lenaerts, K.; van Loon, L.J.C.; Peters, W.H.M.; Buurman, W.A.; Dejong, C.H.C. Exercise-induced splanchnic hypoperfusion results in gut dysfunction in healthy men. PLoS ONE 2011, 6, e22366. [Google Scholar] [CrossRef] [PubMed]
- Pals, K.L.; Ray-Tai, C.; Ryan, A.J.; Gisolfi, C.V. Effect of running intensity on intestinal permeability. J. Appl. Physiol. 1997, 82, 571–576. [Google Scholar] [PubMed]
- Zuhl, M.; Schneider, S.; Lanphere, K.; Conn, C.; Dokladny, K.; Mosely, P. Exercise regulation of intestinal tight junction proteins. Br. J. Sports Med. 2014, 48, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Jeukendrup, A.E.; Vet-Joop, K.; Sturk, A.; Stegen, J.H.J.C.; Senden, J.; Saris, W.H.M.; Wagenmakers, A.J.M. Relationship between gastro-intestinal complaints and endotoxemia, cytokine release and the acute-phase reaction during and after a long-distance triathlon in highly trained men. Clin. Sci. 2000, 98, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Brock-Utne, J.G.; Gaffin, S.L.; Wells, M.T.; Gathiram, P.; Sohar, E.; James, M.F.; Morrell, D.F.; Norman, R.J. Endotoxemia in exhausted runners after a long-distance race. S. Afr. Med. J. 1988, 73, 533–536. [Google Scholar] [PubMed]
- Guo, Y.; Zhou, G.; He, C.; Yang, W.; He, Z.; Liu, Z. Serum levels of lipopolysaccharide and 1,3-β-d-Glucan refer to the severity in patients with Crohn’s disease. Mediat. Inflamm. 2015, 2015, 843089. [Google Scholar] [CrossRef] [PubMed]
- Opal, S.M.; Scannon, P.J.; Vincent, J.-E.; White, M.; Carroll, S.F.; Palardy, J.E.; Parejo, N.A.; Pribble, J.P.; Lemke, J.H. Relationship between plasma levels of lipopolysaccharide (LPS) and LPS-binding protein in patients with severe sepsis and septic shock. J. Infect. Dis. 1999, 180, 1584–1589. [Google Scholar] [CrossRef] [PubMed]
- Selkirk, G.A.; McLellan, T.M.; Wright, H.E.; Rhind, S.G. Mild endotoxemia, NF-κB translocation, and cytokine increase during exertional heat stress in trained and untrained individuals. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2008, 295, R611–R623. [Google Scholar] [CrossRef] [PubMed]
- Yeh, Y.J.; Law, L.Y.L.; Lim, C.L. Gastrointestinal response and endotoxemia during intense exercise in hot and cool environments. Eur. J. Appl. Physiol. 2013, 113, 1575–1583. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.K.; Teixeira, A.; Rama, L.; Rosado, F.; Hankey, J.; Scheer, V.; Hemmings, K.; Ansley-Robson, P.; Costa, R.J.S. Circulatory endotoxin concentration and cytokine profile in response to exertional-heat stress during a multi-stage ultra-marathon competition. Exerc. Immunol. Rev. 2015, 21, 114–128. [Google Scholar] [PubMed]
- Maitra, U.; Deng, H.; Glaros, T.; Baker, B.; Capelluto, D.G.S.; Li, Z.; Li, L. Molecular mechanisms responsible for the selective low-grade induction of pro-inflammatory mediators in murine macrophages by lipopolysaccharide. J. Immunol. 2012, 189, 1014–1023. [Google Scholar] [CrossRef] [PubMed]
- Tuohy, K.M.; Probert, H.M.; Smejkal, C.W.; Gibson, G.R. Using probiotics and prebiotics to improve gut health. Drug Discov. Today 2003, 8, 692–700. [Google Scholar] [CrossRef]
- Gareau, M.G.; Sherman, P.M.; Walker, W.A. Probiotics and the gut microbiota in intestinal health and disease. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 503–514. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.; Miquel, S.; Ulmer, J.; Kechaou, N.; Langella, P.; Bermudez-Humaran, L. Role of commensal and probiotic bacteria in human health: A focus on inflammatory bowel disease. Microb. Cell Fact. 2013, 12, 71. [Google Scholar] [CrossRef] [PubMed]
- West, N.P.; Pyne, D.B.; Cripps, A.W.; Hopkins, W.G.; Eskesen, D.C.; Jairath, A.; Christophersen, C.T.; Conlon, M.A.; Fricker, P.A. Lactobacillus fermentum (PCC®) supplementation and gastrointestinal and respiratory-tract illness symptoms: A randomised control trial in athlete. Nutr. J. 2011, 10, 30. [Google Scholar] [CrossRef] [PubMed]
- Gleeson, M.; Bishop, N.C.; Oliveira, M.; Tauler, P. Daily probiotic’s (Lactobacillus casei Shirota) reduction of infection incidence in athletes. Int. J. Sports Nutr. Exerc. Metabol. 2011, 21, 55–64. [Google Scholar] [CrossRef]
- Nageo, F.; Nakayama, M.; Muto, T.; Okumura, K. Effects of a fermented milk drink containing Lactobacillus casei strain Shirota on the immune system in healthy human subjects. Biosci. Biotechnol. Biochem. 2000, 64, 2706–2708. [Google Scholar] [CrossRef]
- Jager, R.; Purpura, M.; Stone, J.D.; Turner, S.M.; Anzalone, A.J.; Eimerbrink, M.J.; Pane, M.; Amoruso, A.; Rowlands, D.S.; Oliver, J.M. Probiotic Streptococcus thermophilus FP4 and Bifidobacterium breve BR03 supplementation attenuates performance and range-of-motion decrements following muscle damaging exercise. Nutrients 2016, 8, E642. [Google Scholar] [CrossRef] [PubMed]
- Williams, E.A.; Stimpson, J.; Wang, D.; Plummer, S.; Garaiova, I.; Barker, M.E.; Corfe, B.M. Clinical trial: A multistrain probiotic preparation significantly reduces symptoms of irritable bowel syndrome in a double-blind placebo-controlled study. Aliment. Pharmacol. Ther. 2008, 29, 97–103. [Google Scholar] [CrossRef] [PubMed]
- Plummer, S.F.; Garaiova, I.; Sarvotham, T.; Cottrell, S.L.; Le Scouiller, S.; Weaver, M.A.; Tang, J.; Dee, P.; Hunter, J. Effects of probiotics on the composition of the intestinal microbiota following antibiotic therapy. Int. J. Antimicrob. Agents 2005, 26, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Lamprecht, M.; Bogner, S.; Schippinger, G.; Steinbauer, K.; Fankhauser, F.; Hallstroem, S.; Schuetz, B.; Greilberger, J.F. Probiotic supplementation affects markers of intestinal barrier, oxidation, and inflammation in trained men; a randomized, double-blinded, placebo-controlled trial. J. Int. Soc. Sports Nutr. 2012, 9, 45. [Google Scholar] [CrossRef] [PubMed]
- Topping, D.L.; Clifton, P.M. Short-chain fatty acids and human colonic function: Roles of resistant starch and nonstarch polysaccharides. Physiol. Rev. 2001, 81, 1031–1064. [Google Scholar] [PubMed]
- Ashton, T.; Young, I.S.; Davison, G.W.; Rowlands, C.C.; McEneny, J.; Van Blerk, C.; Jones, E.; Peters, J.R.; Jackson, S.K. Exercise-induced endotoxemia: The effect of ascrobic acid supplementation. Free Radic. Biol. Med. 2003, 35, 284–291. [Google Scholar] [CrossRef]
- Suzuki, T.; Hara, H. Quercitin enhances intestinal barrier function through the assembly of zonnula occludens-2, occludin, and claudin-1 and the expression of claudin-4 in caco-2 cells. J. Nutr. 2009, 139, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Bereswill, S.; Munoz, M.; Fischer, A.; Plickert, R.; Haag, L.-M.; Otto, B.; Kuhl, A.A.; Loddenkemper, C.; Gobel, U.B.; Heimsaat, M.M. Anti-inflammatory effects of resveratrol, curcumin and simvastatin in acute small intestinal inflammation. PLoS ONE 2010, 5, e15099. [Google Scholar] [CrossRef] [PubMed]
- Hussein, S.A.; El-Senosy, Y.A.; Hassan, M.F. Gastro protective, antiapoptotic and anti-inflammatory effect of alpha-lipoic acid on ethanol induced gastric mucosal lesions in rats. Am. J. Biochem. Mol. Biol. 2014, 4, 48–63. [Google Scholar] [CrossRef]
- Sung, M.J.; Kim, W.; Ahn, S.Y.; Cho, C.-H.; Koh, G.Y.; Moon, S.-O.; Kim, D.H.; Lee, S.; Kang, K.P.; Jang, K.Y.; et al. Protective effect of α-lipoic acid in lipopolysaccharide-induced endothelial fractalkine expression. Circ. Res. 2005, 97, 880–890. [Google Scholar] [CrossRef] [PubMed]
- Zembron-Lacny, A.; Slowinska-Lisowska, M.; Szygula, Z.; Witkowski, K.; Stefaniak, T.; Dziubek, W. Assessment of the antioxidant effectiveness of α-lipoic acid in healthy men exposed to muscle-damaging exercise. J. Physiol. Pharmacol. 2009, 60, 139–143. [Google Scholar] [PubMed]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.D.; Smye, M.; Watson, R.G.P.; McMillan, S.A.; Trimble, E.R.; Love, A.H.G. Lactulose-mannitol intestinal permeability test: A useful screening test for adult coeliac disease. Ann. Clin. Biochem. 2000, 37, 512–519. [Google Scholar] [PubMed]
- Foster, C.; Florhaug, J.A.; Franklin, J.; Gottschall, L.; Hrovatin, L.A.; Parker, S.; Doleshal, P.; Dodge, C. A new approach to monitoring exercise training. J. Strength Cond. Res. 2001, 15, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Comyns, T.; Flanagan, E.P. Applications of the session rating of perceived exertion system in professional rugby union. Strength Cond. J. 2013, 35, 78–85. [Google Scholar] [CrossRef]
- Jentjens, R.L.P.G.; Wagenmakers, A.J.M.; Jeukendrup, A.E. Heat stress increases muscle glycogen use but reduces the oxidation of ingested carbohydrates during exercise. J. Appl. Physiol. 2002, 92, 1562–1572. [Google Scholar] [CrossRef] [PubMed]
- Nadhazi, Z.; Takats, A.; Offenmuller, K.; Bertok, L. Plasma endotoxin level of healthy donors. Acta Microbiol. Immunol. Hung. 2002, 49, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Hurley, J.C. Endotoxemia: Methods of detection and clinical correlates. Clin. Microbiol. Rev. 1995, 8, 268–292. [Google Scholar] [PubMed]
- Flynn, M.G.; McFarlin, B.K. Toll-like receptor 4: Link to the anti-inflammatory effects of exercise? Exerc. Sport Sci. Rev. 2006, 34, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Stuempfle, K.J.; Valentino, T.; Hew-Butler, T.; Hecht, F.M.; Hoffman, M.D. Nausea is associated with endotoxemia during a 161-km ultramarathon. J. Sports Sci. 2016, 34, 1662–1668. [Google Scholar] [CrossRef] [PubMed]
- Sharma, B.; Srivastava, S.; Singh, N.; Sachdev, V.; Kapur, S.; Saraya, A. Role of probiotics on gut permeability and endotoxemia in patients with acute pancreatitis: A double-blind randomised controlled trial. J. Clin. Gastroenterol. 2011, 45, 442–448. [Google Scholar] [CrossRef] [PubMed]
- Greco, L.; D’Adamo, G.; Truscelli, A.; Parrilli, G.; Mayar, M.; Budillon, G. Intestinal permeability after single dose gluten challenge in coeliac disease. Arch. Dis. Child. 1991, 66, 870–872. [Google Scholar] [CrossRef] [PubMed]
- Van Elburg, R.M.; Uil, J.J.; Kokke, F.T.M.; Mulder, A.M.; van de Broek, W.G.M.; Mulder, C.J.J.; Heymans, H.S.A. Repeatibility of the sugar-absorption test, using lactulose and mannitol, for measuring intestinal permeability for sugars. J. Pediatr. Gastroenterol. Nutr. 1995, 20, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Rosenfeldt, V.; Benfeldt, E.; Valerius, N.H.; Paerregaard, A.; Michaelsen, K.F. Effect of probiotics on gastrointestinal symptoms and small intestinal permeability in children with atopic dermatitis. J. Pediatr. 2004, 145, 612–616. [Google Scholar] [CrossRef] [PubMed]
- Cox, A.J.; Pyne, D.B.; Saunders, P.U.; Fricker, P.A. Oral administration of the probiotic Lactobacillus fermentum VRI-003 and mucosal immunity in endurance athletes. Br. J. Sports Med. 2010, 44, 222–226. [Google Scholar] [CrossRef] [PubMed]
- Ulluwishewa, D.; Anderson, R.C.; McNabb, W.C.; Moughan, P.J.; Wells, J.M.; Roy, N.C. Regulation of tight junction permeability by intestinal bacteria and dietary components. J. Nutr. 2011, 141, 769–776. [Google Scholar] [CrossRef] [PubMed]
- Gill, S.K.; Allerton, D.M.; Ansley-Robson, P.; Hemmings, K.; Cox, M.; Costa, R.J.S. Does short-term high dose probiotic supplementation containing Lactobacillus casei attenuate exertional-heat stress induced endotoxemia and cytokinaemia? Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 268–275. [Google Scholar] [CrossRef] [PubMed]
- Munford, R.S. Sensing gram-negative bacterial lipopolysaccharides: A human disease determinant? Infect. Immun. 2008, 76, 454–465. [Google Scholar] [CrossRef] [PubMed]
- Mach, N.; Botella-Fuster, D. Endurance exercise and gut microbiota: A review. J. Sports Health Sci. 2016, in press. [Google Scholar] [CrossRef]
- Nakamura, Y.K.; Omaye, S.T. Metabolic disease and pro- and prebiotics: Mechanistic insights. Nutr. Metab. 2012, 9, 60. [Google Scholar] [CrossRef] [PubMed]
- Lescheid, D.W. Probiotics as regulators of inflammation: A review. Funct. Foods Health Dis. 2014, 4, 299–311. [Google Scholar]
- Pagnini, C.; Saeed, R.; Bamias, G.; Arseneau, K.O.; Pizarro, T.T.; Cominelli, F. Probiotics promote gut health through stimulation of epithelial innate immunity. Proc. Natl. Acad. Sci. USA 2010, 107, 454–459. [Google Scholar] [CrossRef] [PubMed]
- Madden, J.A.J.; Plummer, S.F.; Tang, J.; Garaiova, I.; Plummer, N.T.; Herbison, M.; Hunter, J.O.; Shimada, T.; Cheng, L.; Shirakawa, T. Effects of probiotics on preventing disruption of the intestinal microflora following antibiotic therapy: A double-blind, placebo-controlled pilot study. Int. Immunopharmacol. 2005, 5, 1091–1097. [Google Scholar] [CrossRef] [PubMed]
- Plummer, S.; Weaver, M.A.; Harris, J.C.; Dee, P.; Hunter, J. Clostridium difficile pilot study: Effects of probiotic supplementation on the incidence of C. difficile diarrhea. Int. Microbiol. 2004, 7, 59–62. [Google Scholar] [PubMed]
- Dehghan, P.; Gargari, B.P.; Jafar-abadi, A.M. Oligofructose-enriched inulin improves some inflammatory markers and metabolic endotoxemia in women with type 2 diabetes mellitus: A randomized controlled clinical trial. Nutrition 2014, 30, 418–423. [Google Scholar] [CrossRef] [PubMed]
- Rastall, R.A.; Gibson, G.R. Recent developments in prebiotics to selectively impact beneficial microbes and promote intestinal health. Curr. Opin. Biotechnol. 2015, 32, 42–46. [Google Scholar] [CrossRef] [PubMed]
- Delzenne, N.M.; Neyrinck, A.M.; Cani, P.D. Gut microbiota and metabolic disorders: How prebiotic can work? Br. J. Nutr. 2013, 109 (Suppl 2), S81–S85. [Google Scholar] [CrossRef] [PubMed]
- Dewulf, E.M.; Cani, P.D.; Claus, S.P.; Fuentes, S.; Puylaert, P.G.B.; Neyrinck, A.M.; Bindels, L.B.; de Vos, W.M.; Gibson, G.R.; Thissen, J.-P.; et al. Insight into the prebiotic concept: Lessons from an exploratory, double-blind intervention study with inulin-type fructans in obese women. Gut 2013, 62, 1112–1121. [Google Scholar] [CrossRef] [PubMed]
- Rajkumar, H.; Kumar, M.; Das, N.; Kumar, S.N.; Challa, H.R.; Nagpal, R. Effect of probiotic Lactobacillus salivarius UBL S22 and prebiotic fructo-oligosaccharide on serum lipids, inflammatory markers, insulin sensitivity, and gut bacteria in healthy young volunteers: A randomized controlled single-blind pilot study. J. Cardiovasc. Pharmacol. Ther. 2015, 20, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Lindsay, J.O.; Whelan, K.; Stagg, A.J.; Gobin, P.; Al-Hassi, H.O.; Rayment, N.; Kamm, M.A.; Knight, S.C.; Forbes, A. Clinical, microbiological, and immunological effects of fructo-oligosaccharide in patients with Crohn’s disease. Gut 2006, 55, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Nova, E.; Viadel, B.; Warnberg, J.; Carreres, J.E.; Marcos, A. Beneficial effects of a synbiotic supplement on self-perceived gastrointestinal well-being and immunoinflammatory status of healthy adults. J. Med. Food 2011, 14, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Khanna, S.; Atalay, M.; Lakksonen, D.E.; Gul, M.; Roy, S.; Sen, C.L. α-lipoic acid supplementation: Tissue glutathione homeostasis at rest and after exercise. J. Appl. Physiol. 1999, 86, 1191–1196. [Google Scholar] [PubMed]
- Shay, K.P.; Moreau, R.F.; Smith, E.J.; Smith, A.R.; Hagen, T.M. Alpha-lipoic acid as a dietary supplement: Molecular mechanisms and therapeutic potential. Biochem. Biophys. Acta 2009, 1790, 1149–1160. [Google Scholar] [CrossRef] [PubMed]
- Heer, M.; Repond, F.; Hany, A.; Sulser, H.; Kehl, O.; Jager, K. Actue ischaemic colitis in a female long distance runner. Gut 1987, 28, 896–899. [Google Scholar] [CrossRef] [PubMed]
- Buffinton, G.D.; Doe, W.F. Depleted mucosal antioxidant defences in inflammatory bowel disease. Free Radic. Biol. Med. 1995, 19, 911–918. [Google Scholar] [CrossRef]
- Goraca, A.; Peichota, A.; Huk-Kolega, H. Effect of alpha-lipoic acid on LPS-induced oxidative stress in the heart. J. Physiol. Pharmacol. 2009, 60, 61–68. [Google Scholar] [PubMed]
- Heibashy, M.I.A.; Mazen, G.M.A.; Shahin, M.I. The curative effects of some antioxidants on endotoxin induced with lipopolysaccharides in the liver of rats. J. Am. Sci. 2013, 9, 529–538. [Google Scholar]
- Zhang, W.-J.; Wel, H.; Hagen, T.; Frel, B. α-lipoic acid attenuates LPS-induced inflammatory responses by activating the phosphoinositide 3-kinase/Akt signaling pathway. Proc. Natl. Acad. Sci. USA 2007, 104, 4077–4082. [Google Scholar] [CrossRef] [PubMed]
- Kuennen, M.; Gillum, T.; Doklandy, K.; Bedrick, E.; Schneider, S.; Moseley, P. Thermotolerance and heat acclimcation may share a common mechanism in humans. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2011, 301, R524–R533. [Google Scholar] [CrossRef] [PubMed]
- Prado de Oliveira, E.; Jeukendrup, A. Nutritional recommendations to avoid gastrointestinal complaints during exercise. Sports Sci. Exch. 2013, 26, 1–4. [Google Scholar]
- Pyne, D.B.; West, N.P.; Cox, A.J.; Cripps, A.W. Probitoics supplementation for athletes—Clinical and physiological effects. Eur. J. Sport Sci. 2015, 15, 63–72. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Variable | LAB4ANTI | LAB4 | PL | |||
|---|---|---|---|---|---|---|
| Distribution | (n = 10; 7 male, 3 female) | (n = 10; 9 male, 1 female) | (n = 10; 9 male, 1 female) | |||
| Age (years) | 33 ± 2 | 35 ± 2 | 35 ± 3 | |||
| Height (m) | 1.74 ± 0.34 | 1.79 ± 0.27 | 1.76 ± 0.16 | |||
| Pre-screening | Baseline | Pre-screening | Baseline | Pre-screening | Baseline | |
| Weight (kg) | 75.21 ± 4.12 | 73.61 ± 3.96 * | 83.77 ± 4.71 | 81.94 ± 4.44 * | 77.42 ± 3.03 | 74.56 ± 2.76 |
| Body fat (%) | 22.56 ± 1.67 | 19.36 ± 2.23 * | 21.88 ± 1.68 | 20.93 ± 1.52 | 21.28 ± 2.38 | 18.64 ± 1.93 * |
| VO2max (L·min−1) | 3.26 ± 0.20 | 3.57 ± 0.19 * | 3.78 ± 0.28 | 3.94 ± 0.27 | 3.30 ± 0.14 | 3.70 ± 0.10 * |
| VO2max (mL·kg−1·min−1) | 42.90 ± 1.59 | 48.60 ± 1.80 * | 43.89 ± 1.75 | 47.56 ± 1.69 * | 43.40 ± 2.53 | 50.50 ± 1.71 * |
| Variable | LAB4ANTI | LAB4 | PL |
|---|---|---|---|
| Energy intake (kcal·kg−1·day−1) | |||
| T1 | 35.96 ± 2.16 | 33.13 ± 1.16 | 35.57 ± 2.88 |
| T2 | 33.88 ± 2.06 | 33.03 ± 4.66 | 34.57 ± 2.98 |
| T3 | 35.42 ± 2.57 | 35.76 ± 2.43 | 36.60 ± 2.85 |
| Fat (g·kg−1·day−1) | |||
| T1 | 1.45 ± 0.13 | 1.28 ± 0.10 | 1.24 ± 0.14 |
| T2 | 1.37 ± 0.12 | 1.27 ± 0.21 | 1.19 ± 0.08 |
| T3 | 1.52 ± 0.18 | 1.26 ± 0.12 | 1.47 ± 0.11 |
| Carbohydrate (g·kg−1·day−1) | |||
| T1 | 4.29 ± 0.33 | 3.80 ± 0.30 | 4.46 ± 0.47 |
| T2 | 3.95 ± 0.43 | 3.90 ± 0.59 | 4.32 ± 0.58 |
| T3 | 3.93 ± 0.39 | 4.36 ± 0.36 | 4.34 ± 0.57 |
| Protein (g·kg−1·day−1) | |||
| T1 | 1.51 ± 0.12 | 1.43 ± 0.14 | 1.81 ± 0.18 |
| T2 | 1.56 ± 0.07 | 1.39 ± 0.17 | 1.70 ± 0.14 |
| T3 | 1.57 ± 0.15 | 1.68 ± 0.28 | 1.67 ± 0.19 |
| Variable | Target Range | LAB4ANTI | LAB4 | PL |
|---|---|---|---|---|
| Weekly training load (AU) | ||||
| T1 | 2173–2716 | 2410 ± 242 | 2851 ± 279 | 2807 ± 368 |
| T2 | 2622–3278 | 3885 ± 558 # | 4311 ± 348 *# | 3915 ± 516 # |
| T3 | 2231–2789 | 2232 ± 148 | 2768 ± 498 | 2263 ± 180 |
| Training monotony (AU) | ||||
| T1 | 1.07–1.33 | 0.94 ± 0.11 | 0.98 ± 0.08 | 1.11 ± 0.08 |
| T2 | 0.97–1.21 | 0.88 ± 0.07 | 0.96 ± 0.08 | 0.88 ± 0.08 |
| T3 | 1.27–1.58 | 0.90 ± 0.12 | 0.87 ± 0.09 | 0.72 ± 0.05 |
| Training strain (AU) | ||||
| T1 | 2951–3688 | 2755 ± 562 | 2945 ± 450 | 3224 ± 566 |
| T2 | 3350–4187 | 3430 ± 620 | 4065 ± 381 *# | 3293 ± 552 |
| T3 | 3352–4440 | 2281 ± 370 | 2681 ± 650 | 1946 ± 186 |
| Variable | LAB4ANTI | LAB4 | PL |
|---|---|---|---|
| % recovery of lactulose | |||
| Baseline | 0.71 ± 0.13 | 0.52 ± 0.07 | 0.35 ± 0.18 |
| Pre-race | 0.55 ± 0.14 | 0.74 ± 0.10 | 0.72 ± 0.17 |
| 6 days Post-race | 0.83 ± 0.11 | 0.90 ± 0.24 | 0.94 ± 0.12 * |
| % recovery of mannitol | |||
| Baseline | 29.99 ± 2.87 | 25.57 ± 2.22 | 30.61 ± 3.96 |
| Pre-race | 23.31 ± 3.60 | 27.42 ± 3.33 | 23.51 ± 2.18 |
| 6 days Post-race | 22.42 ± 3.27 | 25.01 ± 1.89 | 23.48 ± 2.64 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roberts, J.D.; Suckling, C.A.; Peedle, G.Y.; Murphy, J.A.; Dawkins, T.G.; Roberts, M.G. An Exploratory Investigation of Endotoxin Levels in Novice Long Distance Triathletes, and the Effects of a Multi-Strain Probiotic/Prebiotic, Antioxidant Intervention. Nutrients 2016, 8, 733. https://doi.org/10.3390/nu8110733
Roberts JD, Suckling CA, Peedle GY, Murphy JA, Dawkins TG, Roberts MG. An Exploratory Investigation of Endotoxin Levels in Novice Long Distance Triathletes, and the Effects of a Multi-Strain Probiotic/Prebiotic, Antioxidant Intervention. Nutrients. 2016; 8(11):733. https://doi.org/10.3390/nu8110733
Chicago/Turabian StyleRoberts, Justin D., Craig A. Suckling, Georgia Y. Peedle, Joseph A. Murphy, Tony G. Dawkins, and Michael G. Roberts. 2016. "An Exploratory Investigation of Endotoxin Levels in Novice Long Distance Triathletes, and the Effects of a Multi-Strain Probiotic/Prebiotic, Antioxidant Intervention" Nutrients 8, no. 11: 733. https://doi.org/10.3390/nu8110733
APA StyleRoberts, J. D., Suckling, C. A., Peedle, G. Y., Murphy, J. A., Dawkins, T. G., & Roberts, M. G. (2016). An Exploratory Investigation of Endotoxin Levels in Novice Long Distance Triathletes, and the Effects of a Multi-Strain Probiotic/Prebiotic, Antioxidant Intervention. Nutrients, 8(11), 733. https://doi.org/10.3390/nu8110733