Substitution Models of Water for Other Beverages, and the Incidence of Obesity and Weight Gain in the SUN Cohort


 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Beverage Exposure Assessment
2.3. Outcome Assessment
2.4. Assessment of Other Variables
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Flegal, K.M.; Carroll, M.D.; Ogden, C.L.; Johnson, C.L. Prevalence and trends in obesity among us adults, 1999–2000. JAMA 2002, 288, 1723–1727. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The Challenge of Obesity in the WHO European Region and the Strategies for Response; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Stevens, G.A.; Singh, G.M.; Lu, Y.; Danaei, G.; Lin, J.K.; Finucane, M.M.; Bahalim, A.N.; McIntire, R.K.; Gutierrez, H.R.; Cowan, M.; et al. National, regional, and global trends in adult overweight and obesity prevalences. Popul. Health Metr. 2012, 10, 22. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.M.; Weedermann, M.; Fuemmeler, B.F.; Martin, C.K.; Dhurandhar, N.V.; Bredlau, C.; Heymsfield, S.B.; Ravussin, E.; Bouchard, C. Dynamic model predicting overweight, obesity, and extreme obesity prevalence trends. Obesity 2014, 22, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Swinburn, B.A.; Sacks, G.; Hall, K.D.; McPherson, K.; Finegood, D.T.; Moodie, M.L.; Gortmaker, S.L. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011, 378, 804–814. [Google Scholar] [CrossRef]
- Guh, D.P.; Zhang, W.; Bansback, N.; Amarsi, Z.; Birmingham, C.L.; Anis, A.H. The incidence of co-morbidities related to obesity and overweight: A systematic review and meta-analysis. BMC Public Health 2009, 9, 88. [Google Scholar] [CrossRef] [PubMed]
- Marti, A.; Moreno-Aliaga, M.J.; Hebebrand, J.; Martinez, J.A. Genes, lifestyles and obesity. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2004, 28 (Suppl. S3), S29–S36. [Google Scholar] [CrossRef] [PubMed]
- Gesta, S.; Bluher, M.; Yamamoto, Y.; Norris, A.W.; Berndt, J.; Kralisch, S.; Boucher, J.; Lewis, C.; Kahn, C.R. Evidence for a role of developmental genes in the origin of obesity and body fat distribution. Proc. Natl. Acad. Sci. USA 2006, 103, 6676–6681. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, C.; Smith, T.G.; Jewell, J.; Wardle, J.; Hammond, R.A.; Friel, S.; Thow, A.M.; Kain, J. Smart food policies for obesity prevention. Lancet 2015, 385, 2410–2421. [Google Scholar] [CrossRef]
- Popkin, B.M.; Armstrong, L.E.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A new proposed guidance system for beverage consumption in the united states. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar] [PubMed]
- Sociedad Española de Nutrición Comunitaria. Guía para una hidratación saludable. La Declaración de Zaragoza. SENC, 2008. Rev. Esp. Nutr. Comunitaria 2009, 15, 225–230. [Google Scholar]
- Wolf, A.; Bray, G.A.; Popkin, B.M. A short history of beverages and how our body treats them. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2008, 9, 151–164. [Google Scholar] [CrossRef] [PubMed]
- Garriguet, D. Beverage Consumption of Canadian Adults. Available online: http://www.statcan.gc.ca/pub/82-003-x/2008004/article/6500240-eng.htm (accessed on 30 June 2016).
- Almiron-Roig, E.; Palla, L.; Guest, K.; Ricchiuti, C.; Vint, N.; Jebb, S.A.; Drewnowski, A. Factors that determine energy compensation: A systematic review of preload studies. Nutr. Rev. 2013, 71, 458–473. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar] [PubMed]
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am. J. Public Health 2007, 97, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Sayon-Orea, C.; Martinez-Gonzalez, M.A.; Bes-Rastrollo, M. Alcohol consumption and body weight: A systematic review. Nutr. Rev. 2011, 69, 419–431. [Google Scholar] [CrossRef] [PubMed]
- Muckelbauer, R.; Sarganas, G.; Gruneis, A.; Muller-Nordhorn, J. Association between water consumption and body weight outcomes: A systematic review. Am. J. Clin. Nutr. 2013, 98, 282–299. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Malik, V.S.; Hao, T.; Willett, W.C.; Mozaffarian, D.; Hu, F.B. Changes in water and beverage intake and long-term weight changes: Results from three prospective cohort studies. Int. J. Obes. 2013, 37, 1378–1385. [Google Scholar] [CrossRef] [PubMed]
- Segui-Gomez, M.; de la Fuente, C.; Vazquez, Z.; de Irala, J.; Martinez-Gonzalez, M.A. Cohort profile: The ‘Seguimiento Universidad de Navarra’ (SUN) study. Int. J. Epidemiol. 2006, 35, 1417–1422. [Google Scholar] [CrossRef] [PubMed]
- Willett, W. Nutritional Epidemiology, 3rd ed.; Oxford University Press: New York, NY, USA, 2013. [Google Scholar]
- De la Fuente-Arrillaga, C.; Ruiz, Z.V.; Bes-Rastrollo, M.; Sampson, L.; Martinez-Gonzalez, M.A. Reproducibility of an ffq validated in spain. Public Health Nutr. 2010, 13, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-Ballart, J.D.; Pinol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martinez-Gonzalez, M.A.; Salas-Salvado, J.; Martin-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed]
- Sayon-Orea, C.; Bes-Rastrollo, M.; Nunez-Cordoba, J.M.; Basterra-Gortari, F.J.; Beunza, J.J.; Martinez-Gonzalez, M.A. Type of alcoholic beverage and incidence of overweight/obesity in a Mediterranean cohort: The SUN project. Nutrition 2011, 27, 802–808. [Google Scholar] [CrossRef] [PubMed]
- Bes-Rastrollo, M. Validation of self-reported weight and body mass index of the participants of a cohort of university graduates. Rev. Esp. Obes. 2005, 3, 352–358. [Google Scholar]
- Ainsworth, B.E.; Haskell, W.L.; Herrmann, S.D.; Meckes, N.; Bassett, D.R., Jr.; Tudor-Locke, C.; Greer, J.L.; Vezina, J.; Whitt-Glover, M.C.; Leon, A.S. 2011 compendium of physical activities: A second update of codes and MET values. Med. Sci. Sports Exerc. 2011, 43, 1575–1581. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Gonzalez, M.A.; Lopez-Fontana, C.; Varo, J.J.; Sanchez-Villegas, A.; Martinez, J.A. Validation of the Spanish version of the physical activity questionnaire used in the Nurses’ Health Study and the Health Professionals’ follow-up Study. Public Health Nutr. 2005, 8, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Stampfer, M.J.; Manson, J.E.; Rimm, E.; Colditz, G.A.; Rosner, B.A.; Hennekens, C.H.; Willett, W.C. Dietary fat intake and the risk of coronary heart disease in women. N. Engl. J. Med. 1997, 337, 1491–1499. [Google Scholar] [CrossRef] [PubMed]
- Frankenfield, D.; Roth-Yousey, L.; Compher, C. Comparison of predictive equations for resting metabolic rate in healthy nonobese and obese adults: A systematic review. J. Am. Diet. Assoc. 2005, 105, 775–789. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Field, A.E.; Colditz, G.A.; Rimm, E.B. Alcohol intake and 8-year weight gain in women: A prospective study. Obes. Res. 2004, 12, 1386–1396. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Shaper, A.G. Alcohol, body weight, and weight gain in middle-aged men. Am. J. Clin. Nutr. 2003, 77, 1312–1317. [Google Scholar] [PubMed]
- Alcacera, M.A.; Marques-Lopes, I.; Fajo-Pascual, M.; Puzo, J.; Blas Perez, J.; Bes-Rastrollo, M.; Martinez-Gonzalez, M.A. Lifestyle factors associated with BMI in a Spanish graduate population: The SUN Study. Obes. Facts 2008, 1, 80–87. [Google Scholar] [PubMed]
- Wang, L.; Lee, I.M.; Manson, J.E.; Buring, J.E.; Sesso, H.D. Alcohol consumption, weight gain, and risk of becoming overweight in middle-aged and older women. Arch. Intern. Med. 2010, 170, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Vadstrup, E.S.; Petersen, L.; Sorensen, T.I.; Gronbaek, M. Waist circumference in relation to history of amount and type of alcohol: Results from the Copenhagen City Heart Study. Int. J. Obes. Relat. Metab. Disord. J. Int. Assoc. Study Obes. 2003, 27, 238–246. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Pavon, D.; Cervantes-Borunda, M.S.; Diaz, L.E.; Marcos, A.; Castillo, M.J. Effects of a moderate intake of beer on markers of hydration after exercise in the heat: A crossover study. J. Int. Soc. Sports Nutr. 2015, 12, 26. [Google Scholar] [CrossRef] [PubMed]
- Halkjaer, J.; Tjonneland, A.; Thomsen, B.L.; Overvad, K.; Sorensen, T.I. Intake of macronutrients as predictors of 5-y changes in waist circumference. Am. J. Clin. Nutr. 2006, 84, 789–797. [Google Scholar] [PubMed]
- Sanchez-Villegas, A.; Toledo, E.; Bes-Rastrollo, M.; Martin-Moreno, J.M.; Tortosa, A.; Martinez-Gonzalez, M.A. Association between dietary and beverage consumption patterns in the SUN (Seguimiento Universidad de Navarra) cohort study. Public Health Nutr. 2009, 12, 351–358. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, R.; Soares, R.; Guerreiro, S.; Pestana, D.; Calhau, C.; Azevedo, I. Red wine increases adipose tissue aromatase expression and regulates body weight and adipocyte size. Nutrition 2009, 25, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Fischer-Posovszky, P.; Kukulus, V.; Tews, D.; Unterkircher, T.; Debatin, K.M.; Fulda, S.; Wabitsch, M. Resveratrol regulates human adipocyte number and function in a Sirt1-dependent manner. Am. J. Clin. Nutr. 2010, 92, 5–15. [Google Scholar] [CrossRef] [PubMed]
- Cordain, L.; Bryan, E.D.; Melby, C.L.; Smith, M.J. Influence of moderate daily wine consumption on body weight regulation and metabolism in healthy free-living males. J. Am. Coll. Nutr. 1997, 16, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Olsen, N.J.; Heitmann, B.L. Intake of calorically sweetened beverages and obesity. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2009, 10, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Daniels, M.C.; Popkin, B.M. Impact of water intake on energy intake and weight status: A systematic review. Nutr. Rev. 2010, 68, 505–521. [Google Scholar] [CrossRef] [PubMed]
- Stookey, J.D.; Constant, F.; Gardner, C.D.; Popkin, B.M. Replacing sweetened caloric beverages with drinking water is associated with lower energy intake. Obesity 2007, 15, 3013–3022. [Google Scholar] [CrossRef] [PubMed]
- Stookey, J.D.; Constant, F.; Popkin, B.M.; Gardner, C.D. Drinking water is associated with weight loss in overweight dieting women independent of diet and activity. Obesity 2008, 16, 2481–2488. [Google Scholar] [CrossRef] [PubMed]
- Boschmann, M.; Steiniger, J.; Franke, G.; Birkenfeld, A.L.; Luft, F.C.; Jordan, J. Water drinking induces thermogenesis through osmosensitive mechanisms. J. Clin. Endocrinol. Metab. 2007, 92, 3334–3337. [Google Scholar] [CrossRef] [PubMed]
- Pan, A.; Malik, V.S.; Schulze, M.B.; Manson, J.E.; Willett, W.C.; Hu, F.B. Plain-water intake and risk of type 2 diabetes in young and middle-aged women. Am. J. Clin. Nutr. 2012, 95, 1454–1460. [Google Scholar] [CrossRef] [PubMed]
- Ebbeling, C.B.; Feldman, H.A.; Osganian, S.K.; Chomitz, V.R.; Ellenbogen, S.J.; Ludwig, D.S. Effects of decreasing sugar-sweetened beverage consumption on body weight in adolescents: A randomized, controlled pilot study. Pediatrics 2006, 117, 673–680. [Google Scholar] [CrossRef] [PubMed]
- Tate, D.F.; Turner-McGrievy, G.; Lyons, E.; Stevens, J.; Erickson, K.; Polzien, K.; Diamond, M.; Wang, X.; Popkin, B. Replacing caloric beverages with water or diet beverages for weight loss in adults: Main results of the Choose Healthy Options Consciously Everyday (CHOICE) randomized clinical trial. Am. J. Clin. Nutr. 2012, 95, 555–563. [Google Scholar] [CrossRef] [PubMed]
- Piernas, C.; Tate, D.F.; Wang, X.; Popkin, B.M. Does diet-beverage intake affect dietary consumption patterns? Results from the Choose Healthy Options Consciously Everyday (CHOICE) randomized clinical trial. Am. J. Clin. Nutr. 2013, 97, 604–611. [Google Scholar] [CrossRef] [PubMed]
- de Ruyter, J.C.; Olthof, M.R.; Seidell, J.C.; Katan, M.B. A trial of sugar-free or sugar-sweetened beverages and body weight in children. N. Engl. J. Med. 2012, 367, 1397–1406. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.C.; Wyatt, H.R.; Foster, G.D.; Pan, Z.; Wojtanowski, A.C.; Vander Veur, S.S.; Herring, S.J.; Brill, C.; Hill, J.O. The effects of water and non-nutritive sweetened beverages on weight loss during a 12-week weight loss treatment program. Obesity 2014, 22, 1415–1421. [Google Scholar] [CrossRef] [PubMed]
- Bes-Rastrollo, M.; Sanchez-Villegas, A.; Gomez-Gracia, E.; Martinez, J.A.; Pajares, R.M.; Martinez-Gonzalez, M.A. Predictors of weight gain in a Mediterranean cohort: The Seguimiento Universidad de Navarra Study 1. Am. J. Clin. Nutr. 2006, 83, 362–370. [Google Scholar] [PubMed]
- Rajpathak, S.N.; Rimm, E.B.; Rosner, B.; Willett, W.C.; Hu, F.B. Calcium and dairy intakes in relation to long-term weight gain in US men. Am. J. Clin. Nutr. 2006, 83, 559–566. [Google Scholar] [PubMed]
- Louie, J.C.; Flood, V.M.; Hector, D.J.; Rangan, A.M.; Gill, T.P. Dairy consumption and overweight and obesity: A systematic review of prospective cohort studies. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2011, 12, e582–e592. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Pan, A.; Malik, V.S.; Hu, F.B. Effects of dairy intake on body weight and fat: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 96, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Bernstein, A.M.; de Koning, L.; Flint, A.J.; Rexrode, K.M.; Willett, W.C. Soda consumption and the risk of stroke in men and women. Am. J. Clin. Nutr. 2012, 95, 1190–1199. [Google Scholar] [CrossRef] [PubMed]
- Guasch-Ferre, M.; Babio, N.; Martinez-Gonzalez, M.A.; Corella, D.; Ros, E.; Martin-Pelaez, S.; Estruch, R.; Aros, F.; Gomez-Gracia, E.; Fiol, M.; et al. Dietary fat intake and risk of cardiovascular disease and all-cause mortality in a population at high risk of cardiovascular disease. Am. J. Clin. Nutr. 2015, 102, 1563–1573. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Quintiles of Water Consumption | ||||||
|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | p-Value * | |
| N | 5227 | 1457 | 3250 | 4000 | 2131 | |
| Water intake 1 (mL) | 357 (0, 500) | 529 (513, 700) | 1000 (1000, 1000) | 1400 (1013, 1400) | 1500 (1413, 2800) | <0.001 |
| Sex (men %) | 44.4 | 44.0 | 39.0 | 37.2 | 34.6 | <0.001 |
| Age (years) | 40.8 (12.0) | 38.3 (11.4) | 38.2 (11.8) | 35.8 (11.1) | 34.1 (10.3) | <0.001 |
| Baseline body mass index (kg/m2) | 23.7 (3.42) | 23.4 (3.33) | 23.4 (3.50) | 23.4 (3.49) | 23.3 (3.53) | 0.052 |
| Current smoker (%) | 21.8 | 20.9 | 20.4 | 21.8 | 22.9 | <0.001 |
| Former smoker (%) | 31.1 | 26.1 | 29.4 | 26.6 | 25.2 | <0.001 |
| Personal history of obesity (%) | 7.21 | 6.18 | 7.51 | 7.23 | 8.40 | 0.149 |
| Family history of obesity (%) | 21.6 | 22.9 | 23.0 | 24.3 | 23.0 | 0.047 |
| Weight loss in the previous 5 years (%) | 20.4 | 20.5 | 22.6 | 26.2 | 28.3 | <0.001 |
| Weight gain in the previous 5 years (%) | 52.2 | 54.4 | 50.2 | 48.9 | 48.4 | <0.001 |
| Physical activity (MET-h/week) | 19.1 (21.2) | 20.6 (20.9) | 21.1 (19.9) | 23.8 (24.1) | 25.8 (27.0) | <0.001 |
| Total energy intake (kcal/day) | 2233 (620) | 2397 (602) | 2369 (600) | 2394 (596) | 2430 (620) | 0.047 |
| Snacking between meals (%) | 31.6 | 34.0 | 33.1 | 32.7 | 35.5 | 0.023 |
| Following special diet (%) | 6.62 | 5.97 | 7.23 | 8.18 | 10.09 | <0.001 |
| Adherence to Mediterranean diet (0–9) | 3.98 (1.74) | 4.10 (1.79) | 4.14 (1.77) | 4.30 (1.76) | 4.40 (1.78) | 0.690 |
| Fat intake (g/day) | 90.9 (30.7) | 98.8 (30.9) | 97.6 (30.4) | 98.0 (30.5) | 99.5 (31.5) | 0.397 |
| Saturated fatty acids intake (g/day) | 31.5 (12.3) | 33.9 (12.0) | 33.1 (11.7) | 33.0 (12.1) | 33.6 (12.4) | 0.025 |
| Monounsaturated fatty acids intake (g/day) | 38.7 (14.2) | 42.3 (14.4) | 42.0 (14.3) | 42.2 (14.3) | 42.8 (14.8) | 0.383 |
| Polyunsaturated fatty acids intake (g/day) | 13.1 (5.72) | 14.3 (5.94) | 13.9 (5.91) | 13.9 (5.80) | 14.0 (5.69) | 0.115 |
| Carbohydrates intake (g/day) | 244 (83.9) | 262 (81.8) | 259 (82.5) | 263 (83.7) | 265 (85.3) | 0.362 |
| Protein intake (g/day) | 101 (28.0) | 106 (26.4) | 105 (26.5) | 107 (27.3) | 110 (28.9) | <0.001 |
| Alcohol intake (g/day) | 4.84 (9.03) | 4.99 (7.59) | 4.59 (7.80) | 4.43 (7.62) | 4.64 (6.94) | 0.0734 |
| Dietary fibre intake (g/day) | 26.4 (12.2) | 27.1 (11.2) | 27.9 (11.8) | 28.9 (12.5) | 29.3 (12.4) | <0.001 |
| Sleeping hours (h/day) | 7.24 (0.91) | 7.32 (0.78) | 7.31 (0.80) | 7.32 (0.84) | 7.31 (0.82) | <0.001 |
| Sleeping siesta (h/day) | 0.34 (0.86) | 0.29 (0.76) | 0.28 (0.73) | 0.30 (0.74) | 0.27 (0.71) | <0.001 |
| Groups of beverages (servings/week) | ||||||
| 1. Water # | 11.0 (6.69) | 20.2 (2.72) | 35.0 (0.00) | 43.9 (6.03) | 58.3 (13.86) | <0.001 |
| 2. Low/non-caloric beverages | 7.01 (10.3) | 7.49 (10.0) | 7.21 (9.9) | 7.39 (10.2) | 7.77 (10.3) | 0.105 |
| Diet soda beverages # | 0.81 (3.22) | 0.78 (2.79) | 0.70 (2.58) | 0.85 (2.70) | 1.11 (3.54) | <0.001 |
| Coffee without sugar † | 6.20 (9.52) | 6.71 (9.47) | 6.52 (9.34) | 6.54 (9.63) | 6.66 (9.50) | 0.474 |
| 3. Milk, juice and sugared coffee | 15.8 (11.4) | 16.8 (10.9) | 16.8 (10.6) | 16.7 (11.4) | 16.8 (11.7) | <0.001 |
| Dairyproducts # | 9.33 (8.09) | 9.79 (7.63) | 9.58 (7.14) | 9.72 (7.67) | 9.71 (7.77) | <0.001 |
| Juices # | 2.91 (4.29) | 3.24 (4.13) | 3.01 (3.86) | 3.34 (4.83) | 3.33 (4.60) | <0.001 |
| Coffee with sugar † | 3.57 (6.37) | 3.79 (6.44) | 4.17 (6.66) | 3.62 (6.42) | 3.81 (7.06) | <0.001 |
| 4. Occasional consumption | 2.04 (3.85) | 2.09 (3.09) | 1.83 (3.00) | 1.83 (2.78) | 2.02 (3.25) | <0.001 |
| SSSBs # | 1.55 (3.41) | 1.55 (2.65) | 1.30 (2.29) | 1.26 (2.11) | 1.42 (2.87) | <0.001 |
| Spirits † | 0.49 (1.35) | 0.54 (1.21) | 0.53 (1.34) | 0.57 (1.46) | 0.60 (1.17) | <0.001 |
| 5.Wine ‡ | 3.64 (6.45) | 3.30 (5.75) | 2.74 (5.31) | 2.30 (5.01) | 2.11 (4.55) | <0.001 |
| 6. Beer • | 1.34 (2.92) | 1.37 (2.50) | 1.25 (2.42) | 1.14 (2.02) | 1.23 (2.41) | <0.001 |
| Substitution | Crude Model | Age- & Sex-Adjusted Model | Multiple-Adjusted Model 1 |
|---|---|---|---|
| Water for beer | 0.63 (0.55 to 0.71) | 0.78 (0.67 to 0.91) | 0.81 (0.69 to 0.94) |
| Water for SSSBs 2 | 0.80 (0.71 to 0.90) | 0.82 (0.73 to 0.91) | 0.85 (0.75 to 0.97) |
| Water for bottled juice | 0.96 (0.78 to 1.19) | 0.94 (0.79 to 1.13) | 0.86 (0.73 to 1.02) |
| Water for diet soda beverages | 0.77 (0.71 to 0.85) | 0.75 (0.69 to 0.82) | 0.91 (0.80 to 1.04) |
| Water for red wine | 0.78 (0.72 to 0.84) | 0.95 (0.87 to 1.04) | 0.92 (0.84 to 1.00) |
| Water for other wines (non-red) | 0.75 (0.64 to 0.87) | 0.91 (0.76 to 1.10) | 0.93 (0.76 to 1.13) |
| Water for skim milk | 0.93 (0.86 to 1.00) | 0.92 (0.86 to 0.99) | 0.94 (0.87 to 1.03) |
| Water for whole milk | 1.07 (0.97 to 1.18) | 1.12 (1.00 to 1.24) | 0.96 (0.87 to 1.06) |
| Water for regular coffee | 0.89 (0.85 to 0.94) | 0.94 (0.89 to 0.99) | 0.97 (0.91 to 1.02) |
| Water for spirits | 0.69 (0.55 to 0.85) | 0.84 (0.67 to 1.04) | 1.02 (0.77 to 1.34) |
| Water for decaffeinated coffee | 0.87 (0.79 to 0.97) | 0.93 (0.84 to 1.03) | 1.05 (0.94 to 1.18) |
| Water for reduced-fat milk | 1.10 (1.01 to 1.21) | 1.08 (0.99 to 1.19) | 1.06 (0.96 to 1.16) |
| Water for fresh non-orange fruit juice | 1.09 (0.75 to 1.58) | 1.13 (0.80 to 1.59) | 1.06 (0.73 to 1.52) |
| Water for fresh orange juice | 1.10 (0.93 to 1.31) | 1.14 (0.97 to 1.33) | 1.06 (0.90 to 1.24) |
| Water for milk shake | 1.94 (0.89 to 4.25) | 1.56 (0.83 to 2.97) | 1.32 (0.79 to 2.22) |
| Substitution | Crude Model | Age- & Sex-Adjusted Model | Multiple-Adjusted Model 1 |
|---|---|---|---|
| Water for milk shake | −554 (−1205 to 98) | −482 (−1134 to 171) | −399 (−1049 to 250) |
| Water for fresh non-orange fruit juice | −303 (−724 to 118) | −336 (−757 to 85) | −342 (−760 to 76) |
| Water for beer | −226 (−458 to 6) | −272 (−511 to −34) | −328 (−566 to −89) |
| Water for spirits | −265 (−695 to 166) | −274 (−713 to 165) | −226 (−667 to 216) |
| Water for SSSBs 2 | −291 (−508 to −75) | −215 (−435 to 5) | −205 (−425 to 16) |
| Water for bottled juice | −203 (−469 to 63) | −172 (−437 to 94) | −137 (−400 to 127) |
| Water for diet soda beverages | −152 (−367 to 62) | −122 (−336 to 93) | −86 (−300 to 129) |
| Water for other wines (non-red) | 86 (−270 to 441) | −24 (−382 to 335) | −41 (−397 to 315) |
| Water for red wine | 60 (−75 to 195) | −24 (−167 to 119) | −38 (−181 to 104) |
| Water for regular coffee | −49 (−126 to 28) | −56 (−135 to 22) | −21 (−101 to 58) |
| Water for decaffeinated coffee | 48 (−104 to 199) | −14 (−168 to 139) | 5 (−148 to 157) |
| Water for reduced-fat milk | 31 (−76 to 138) | 31 (−76 to 138) | 6 (−100 to 113) |
| Water for fresh orange juice | 81 (−115 to 276) | 43 (−153 to 239) | 7 (−189 to 202) |
| Water for skim milk | 52 (−57 to 160) | 23 (−86 to 133) | 28 (−82 to 137) |
| Water for whole milk | 4 (−107 to 115) | 20 (−92 to 132) | 61 (−55 to 177) |
| Beverage | Cumulative R2 | % of Total Liquid Intake |
|---|---|---|
| Water | 0.715 | 56.28 |
| Reduced-fat milk | 0.740 | 6.90 |
| Whole milk | 0.765 | 6.78 |
| Regular coffee | 0.786 | 4.56 |
| Skim milk | 0.847 | 5.77 |
| Bottled juice | 0.861 | 1.71 |
| Fresh orange juice | 0.891 | 3.93 |
| Diet soda beverage | 0.914 | 1.57 |
| SSSBs 1 | 0.933 | 3.07 |
| Beer | 0.978 | 4.26 |
| Decaffeinated coffee | 0.981 | 0.96 |
| Red wine | 0.992 | 2.10 |
| Milk shake | 0.994 | 0.54 |
| Fresh non-orange fruit juice | 0.998 | 0.84 |
| Another type of wine (non-red) | 0.999 | 0.43 |
| Spirits | 1.000 | 0.30 |
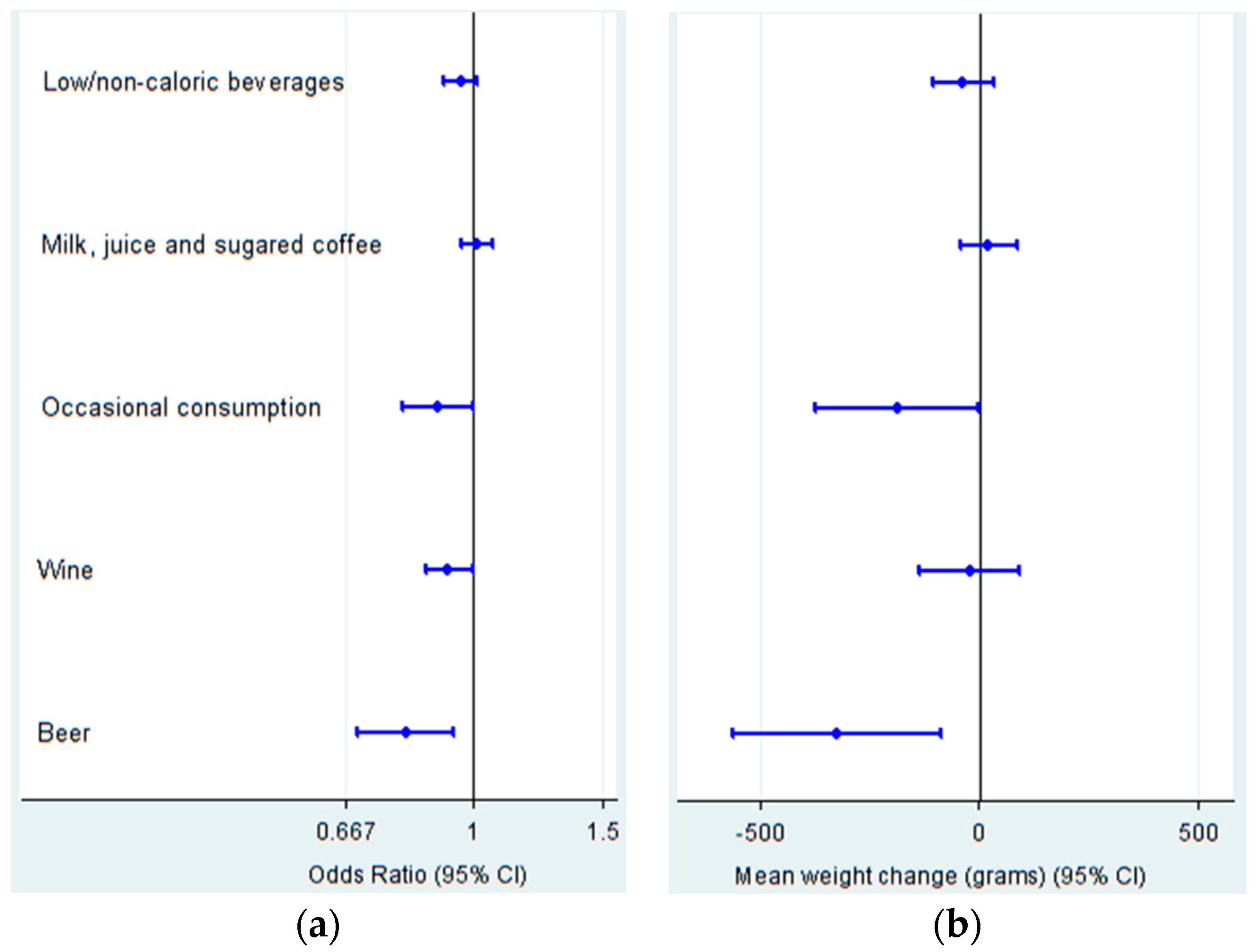
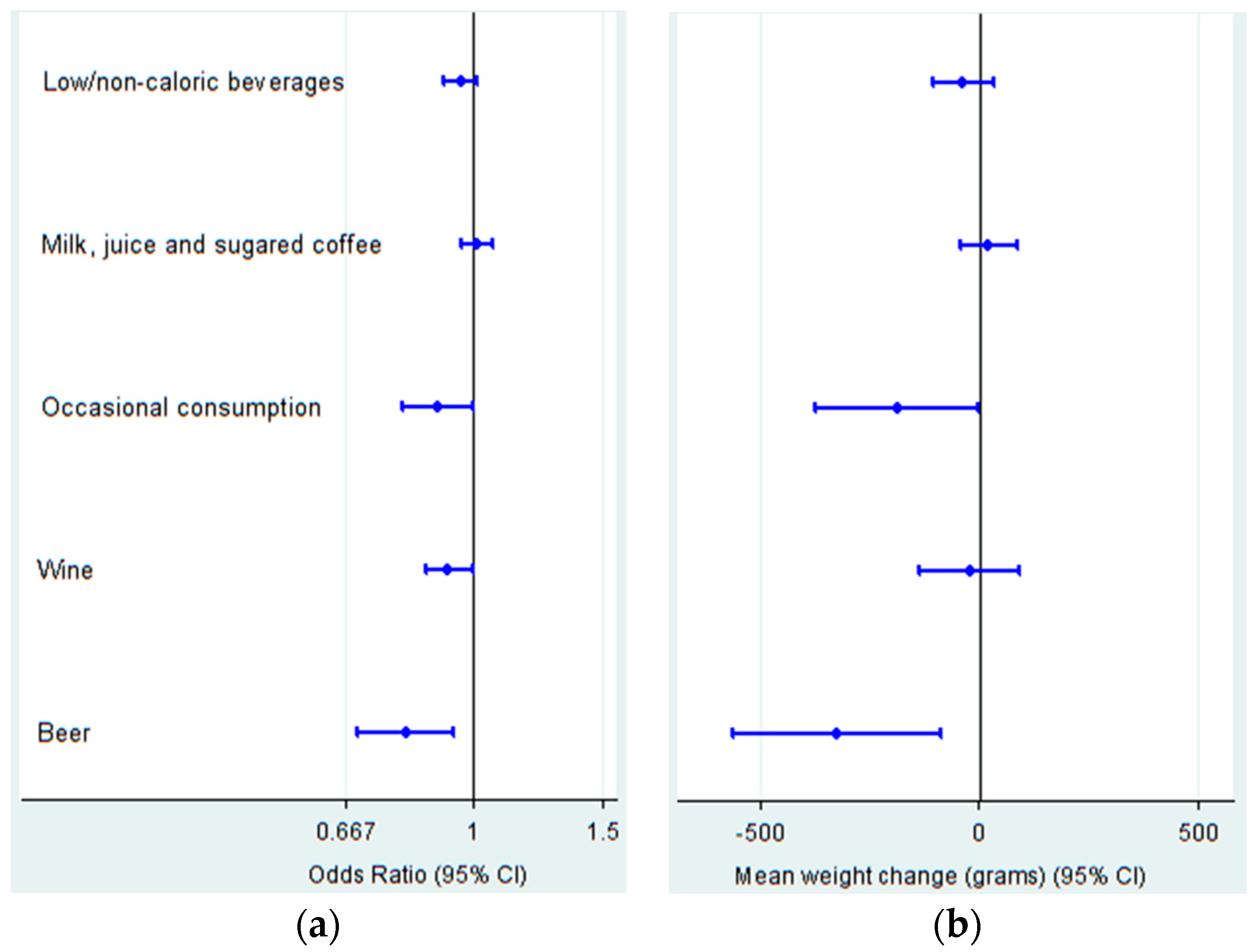
| Cases | Low/Non-Caloric Beverages 1 | Milk, Juice and Sugared Coffee 2 | Occasional Consumption 3 | Wine | Beer | |
|---|---|---|---|---|---|---|
| Overall | 873 | 0.96 (0.91 to 1.01) | 1.01 (0.96 to 1.06) | 0.89 (0.80 to 0.99) | 0.92 (0.86 to 0.99) | 0.81 (0.69 to 0.94) |
| Excluding participants who answered ≤10% beverage items | 862 | 0.95 (0.91 to 1.00) | 1.00 (0.95 to 1.05) | 0.89 (0.80 to 1.00) | 0.92 (0.85 to 0.99) | 0.80 (0.69 to 0.94) |
| Excluding participants with weight change in the previous 5 years due to pregnancy | 854 | 0.96 (0.91 to 1.02) | 1.01 (0.96 to 1.06) | 0.90 (0.80 to 1.01) | 0.92 (0.86 to 1.00) | 0.80 (0.68 to 0.95) |
| Excluding participants with personal history of obesity | 623 | 0.93 (0.87 to 0.98) | 1.03 (0.97 to 1.09) | 0.91 (0.81 to 1.02) | 0.92 (0.84 to 1.01) | 0.76 (0.64 to 0.89) |
| Excluding participants with family history of obesity | 587 | 0.96 (0.90 to 1.01) | 1.03 (0.97 to 1.10) | 0.96 (0.84 to 1.09) | 0.93 (0.85 to 1.01) | 0.81 (0.67 to 0.97) |
| Excluding participants with BMI ≥ 27.5 | 369 | 0.94 (0.87 to 1.01) | 1.04 (0.96 to 1.12) | 0.89 (0.77 to 1.03) | 0.90 (0.80 to 1.02) | 0.77 (0.61 to 0.96) |
| Energy limits: under or over limits of daily calories needs, according to BMR ‡ | 441 | 0.98 (0.91 to 1.05) | 0.92 (0.86 to 0.98) | 0.79 (0.69 to 0.90) | 0.87 (0.78 to 0.97) | 0.81 (0.67 to 0.98) |
| Assessing only women | 358 | 0.97 (0.89 to 1.05) | 1.01 (0.93 to 1.09) | 0.78 (0.63 to 0.96) † | 1.23 (0.95 to 1.59) ¥ | 0.71 (0.42 to 1.20) |
| Assessing only men | 515 | 0.96 (0.90 to 1.03) | 1.00 (0.94 to 1.07) | 0.96 (0.84 to 1.10) † | 0.92 (0.85 to 1.00) ¥ | 0.79 (0.68 to 0.91) |
| Assessing only people under 35 years old | 281 | 0.92 (0.85 to 1.00) | 1.06 (0.98 to 1.16) | 0.90 (0.75 to 1.08) | 0.83 (0.67 to 1.01) | 0.72 (0.56 to 0.94) |
| Assessing only people 35 year olds or older | 592 | 0.98 (0.92 to 1.05) | 0.99 (0.93 to 1.05) | 0.90 (0.78 to 1.03) | 0.92 (0.85 to 1.01) | 0.84 (0.70 to 1.02) |
| Assessing only less active people (under the median) | 500 | 0.95 (0.89 to 1.01) | 1.03 (0.97 to 1.10) | 0.83 (0.73 to 0.95) * | 0.93 (0.84 to 1.04) | 0.82 (0.67 to 1.02) |
| Assessing only more active people (in and over the median) | 373 | 0.97 (0.90 to 1.06) | 0.98 (0.91 to 1.05) | 1.02 (0.82 to 1.26) * | 0.89 (0.80 to 0.99) | 0.79 (0.63 to 0.99) |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fresán, U.; Gea, A.; Bes-Rastrollo, M.; Ruiz-Canela, M.; Martínez-Gonzalez, M.A. Substitution Models of Water for Other Beverages, and the Incidence of Obesity and Weight Gain in the SUN Cohort. Nutrients 2016, 8, 688. https://doi.org/10.3390/nu8110688
Fresán U, Gea A, Bes-Rastrollo M, Ruiz-Canela M, Martínez-Gonzalez MA. Substitution Models of Water for Other Beverages, and the Incidence of Obesity and Weight Gain in the SUN Cohort. Nutrients. 2016; 8(11):688. https://doi.org/10.3390/nu8110688
Chicago/Turabian StyleFresán, Ujué, Alfredo Gea, Maira Bes-Rastrollo, Miguel Ruiz-Canela, and Miguel A. Martínez-Gonzalez. 2016. "Substitution Models of Water for Other Beverages, and the Incidence of Obesity and Weight Gain in the SUN Cohort" Nutrients 8, no. 11: 688. https://doi.org/10.3390/nu8110688
APA StyleFresán, U., Gea, A., Bes-Rastrollo, M., Ruiz-Canela, M., & Martínez-Gonzalez, M. A. (2016). Substitution Models of Water for Other Beverages, and the Incidence of Obesity and Weight Gain in the SUN Cohort. Nutrients, 8(11), 688. https://doi.org/10.3390/nu8110688