Reasons Low-Income Parents Offer Snacks to Children: How Feeding Rationale Influences Snack Frequency and Adherence to Dietary Recommendations

Abstract
:1. Introduction
2. Methods
2.1. Participants and Study Designs
2.2. Measures
2.2.1. Reasons Parents Offer Children Snacks
2.2.2. Adherence to Childhood Dietary Recommendations
2.2.3. Parent, Child, and Family Characteristics
2.3. Data Analysis
3. Results
3.1. Participant Characteristics

{kind=link}
| Parent Characteristics | n | (%) |
|---|---|---|
| Relationship to child | ||
| Mother | 235 | 86.7 |
| Father | 25 | 9.2 |
| Grandparent | 8 | 3.0 |
| Legal guardian | 3 | 1.1 |
| Gender | ||
| Female | 245 | 90.4 |
| Male | 26 | 9.6 |
| Parent age in years (mean, range) | 32.1 | (19–62) |
| Parent education | ||
| Less than high school | 75 | 27.7 |
| High school graduate/GED | 102 | 37.6 |
| Some college or technical school | 80 | 29.5 |
| College graduate | 14 | 5.2 |
| Parent birthplace | ||
| United States | 151 | 55.7 |
| Outside United States | 120 | 44.3 |
| Parent language spoken | ||
| Only or mostly English | 124 | 45.8 |
| Equally English and another language | 96 | 35.4 |
| Only or mostly another language | 51 | 18.8 |
| Parent marital status | ||
| Single | 114 | 42.1 |
| Married or living with partner | 109 | 40.2 |
| Separated/living apart from spouse | 31 | 11.4 |
| Divorced/widowed | 17 | 6.3 |
| Parent body mass index | ||
| Normal | 71 | 26.2 |
| Overweight/obese | 172 | 63.4 |
| Missing | 27 | 10.0 |
| Family characteristics | n | (%) |
| Household income | ||
| ≤$10,000 | 85 | 31.3 |
| $10,001 to $15,000 | 48 | 17.7 |
| $15,001 to $20,000 | 54 | 19.9 |
| $20,001 to $35,000 | 47 | 17.4 |
| >$35,000 | 37 | 13.7 |
| Number in household (mean, range) | 4.0 | (2–13) |
| Family assistance received (select all that apply) | ||
| SNAP/EBT/food stamps | 192 | 70.9 |
| Free/reduced meals for child at school | 188 | 69.4 |
| WIC (Women Infants & Children) | 103 | 38.0 |
| Family food insecurity in the past 12 months | ||
| Yes | 146 | 53.9 |
| No | 125 | 46.1 |
| Child characteristics | n | (%) |
| Child age | ||
| Preschool-aged (2–5 years) | 120 | 44.3 |
| Elementary (6–10 years) | 114 | 42.1 |
| Middle (11–12 years) | 37 | 13.6 |
| Child gender | ||
| Female | 120 | 44.3 |
| Male | 151 | 55.7 |
| Child race | ||
| Hispanic/Latino | 154 | 56.8 |
| White | 40 | 14.8 |
| Black/African American | 32 | 11.8 |
| Multiracial | 24 | 8.9 |
| Other | 21 | 7.7 |
| Child body mass index a | ||
| Normal | 152 | 56.1 |
| Overweight | 45 | 16.6 |
| Obese | 72 | 26.6 |
| Child adherence to dietary recommendations b | n | (%) |
| Soda (<1 time per week) | 189 | 70.0 |
| Sweetened juice drinks (<1 time per week) | 80 | 29.5 |
| 100% juice (≤1 serving per day) | 211 | 77.9 |
| Fast food (<1 time per week) | 173 | 63.8 |
| Fruit (≥2 servings per day) | 68 | 25.1 |
| Vegetables (≥2 servings per day) | 54 | 19.9 |
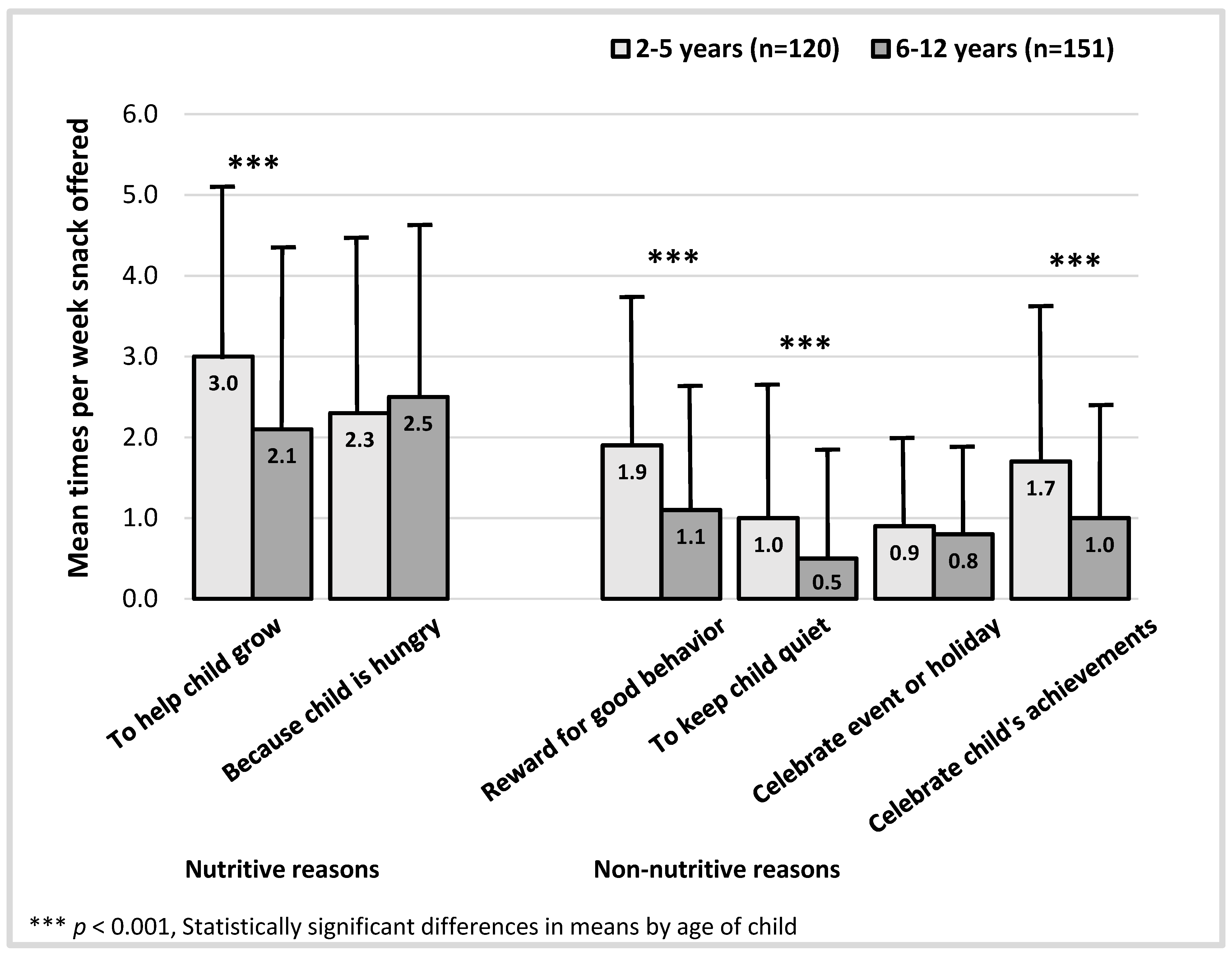
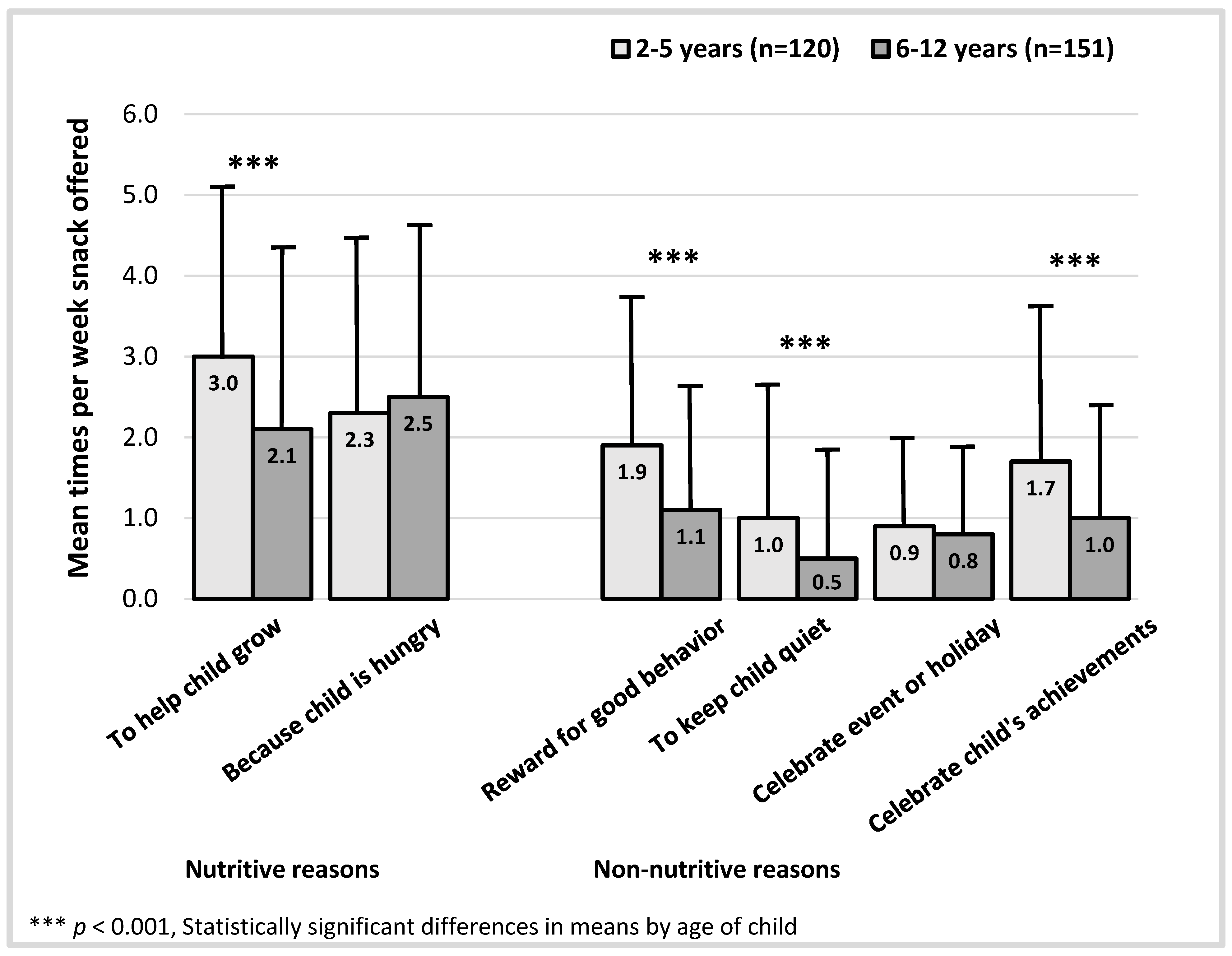
3.2. Frequency of Parents Offering Snacks
| Child BMI a | Child Sex | Child Race/Ethnicity | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Times Per Week Parent Offered Snacks | Total (n = 271) | Normal (n = 152) | Overweight or Obese (n = 117) | Male (n = 120) | Female (n = 151) | Hispanic/Latino (n = 154) | Black/AA (n = 32) | White (n = 40) | Mixed Race (n = 24) |
| Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Nutritive reasons | |||||||||
| To help child grow | 2.5 (2.2) | 2.7 (2.2) | 2.2 (2.2) | 2.8 (2.2) | 2.3 (2.2) | 2.4 (2.2) | 2.1 (2.2) b | 2.9 (2.3) | 3.3 (2.0) |
| Because child is hungry | 2.4 (2.1) | 2.5 (2.2) | 2.2 (2.1) | 2.5 (2.2) | 2.3 (2.1) | 2.3 (2.2)c | 1.5 (1.8) | 3.5 (1.9) d | 2.2 (2.0) |
| Non-nutritive reasons | |||||||||
| Reward for good behavior | 1.5 (1.8) | 1.5 (1.8) | 1.4 (1.8) | 1.6 (1.8) | 1.4 (1.8) | 1.5 (1.8) | 1.0 (1.6) | 1.3 (1.9) | 1.3 (1.7) |
| To keep child quiet | 0.7 (1.5) | 0.7 (1.4) | 0.8 (1.5) | 0.7 (1.5) | 0.8 (1.4) | 0.8 (1.5) | 0.5 (1.3) | 0.3 (1.4) | 0.6 (1.2) |
| Celebrate event or holiday | 0.8 (1.1) | 1.0 (1.3) | 0.7 (0.9) | 0.9 (1.2) | 0.8 (1.0) | 0.9 (1.2) e | 0.6 (0.9) | 0.5 (0.3) | 0.6 (0.4) |
| Celebrate child’s achievements | 1.3 (1.7) | 1.6 (1.8) | 1.0 (1.4) ** | 1.5 (1.8) | 1.2 (1.6) | 1.4 (1.7) e | 1.3 (1.5) | 0.8 (1.2) | 0.9 (1.4) |
| Parent Education | Parent BMI | Family Food Insecurity a | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 271) | High School Graduate or Less (n = 177) | College or Technical School (n = 94) | Normal (n = 71) | Overweight (n = 77) | Obese (n = 122) | Yes (n = 146) | No (n = 125) | ||
| Times per week parent offered snacks | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | Mean (SD) | |
| Nutritive reasons | |||||||||
| To help child grow | 2.5 (2.2) | 2.3 (2.2) | 2.8 (2.2) | 2.9 (2.2) b | 2.5 (2.1) | 2.2 (2.1) | 2.3 (2.2) | 2.7 (2.2) | |
| Because child is hungry | 2.4 (2.1) | 2.2 (2.1) | 2.7 (2.2) | 2.5 (2.1) | 2.4 (2.2) | 2.3 (2.1) | 2.4 (2.2) | 2.4 (2.1) | |
| Non-nutritive reasons | |||||||||
| Reward for good behavior | 1.5 (1.8) | 1.7 (1.9) | 1.0 (1.5) * | 1.7 (1.9) | 1.5 (1.8) | 1.3 (1.7) | 1.5 (1.8) | 1.4 (1.8) | |
| To keep child quiet | 0.7 (1.5) | 0.8 (1.5) | 0.6 (1.4) | 0.9 (1.7) | 0.7(1.4) | 0.7 (1.4) | 0.8 (1.6) | 0.7 (1.4) | |
| Celebrate event or holiday | 0.8 (1.1) | 0.9 (1.2) | 0.7 (1.0) | 0.9 (1.2) | 0.8 (1.0) | 0.8 (1.1) | 0.9 (1.2) | 0.8 (1.0) | |
| Celebrate child’s achievements | 1.3 (1.7) | 1.5 (1.7) | 1.1 (1.6) | 1.7 (1.9) b | 1.4 (1.8) | 1.1 (1.5) | 1.4 (1.7) | 1.3 (1.7) | |
3.3. Snack Offerings and Child Adherence to Dietary Recommendations
| Times Per Week Parent Offered Snack to Child b | Referent Group: Child Adhering to the Majority of Dietary Recommendations in the Previous Month (n = 81) a |
|---|---|
| OR (95% CI) c | |
| Nutritive reasons | |
| To help child grow | 1.05 (0.92, 1.19) |
| Because child is hungry | 0.88 (0.77, 1.01) |
| Non-nutritive reasons | |
| Reward for good behavior | 0.83 (0.70, 0.99) * |
| To keep child quiet | 0.89 (0.73, 1.08) |
| Celebrate event or holiday | 0.72 (0.52, 0.99) * |
| Celebrate child’s achievements | 0.82 (0.68, 0.98) * |
4. Discussion
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Duffey, K.J.; Popkin, B.M. Causes of increased energy intake among children in the U.S., 1977–2010. Am. J. Prev. Med. 2013, 44. [Google Scholar] [CrossRef]
- Bleich, S.N.; Wolfson, J.A. US adults and child snacking patterns among sugar sweetened beverage drinkers and non-drinkers. Prev. Med. 2015, 72, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Piernas, C.; Popkin, B.M. Trends in snacking among U.S. children. Health Aff. (Millwood) 2010, 29, 398–404. [Google Scholar] [CrossRef] [PubMed]
- Ford, C.N.; Slining, M.M.; Popkin, B.M. Trends in dietary intake among US 2- to 6-year-old children, 1989–2008. J. Acad. Nutr. Diet. 2013, 113, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Kuhl, E.S.; Clifford, L.M.; Stark, L.J. Obesity in Preschoolers: Behavioral Correlates and Directions for Treatment. Obesity 2012, 20, 3–29. [Google Scholar] [CrossRef] [PubMed]
- Barlow, S.E. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics 2007, 120 (Suppl. S4), S164–S192. [Google Scholar] [CrossRef] [PubMed]
- Davis, M.M.; Gance-Cleveland, B.; Hassink, S.; Johnson, R.; Paradis, G.; Resnicow, K. Recommendations for prevention of childhood obesity. Pediatrics 2007, 120 (Suppl. S4), S229–S253. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.; Story, M. A review of snacking patterns among children and adolescents: What are the implications of snacking for weight status? Child. Obes. 2013, 9, 104–115. [Google Scholar] [PubMed]
- Wen, X.; Gillman, M.W.; Rifas-Shiman, S.L.; Sherry, B.; Kleinman, K.; Taveras, E.M. Decreasing prevalence of obesity among young children in Massachusetts from 2004 to 2008. Pediatrics 2012, 129, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Ogden, C.L.; Carroll, M.D.; Kit, B.K.; Flegal, K.M. Prevalence of childhood and adult obesity in the United States, 2011–2012. JAMA 2014, 311, 806–814. [Google Scholar] [CrossRef] [PubMed]
- Taveras, E.M.; Gillman, M.W.; Kleinman, K.; Rich-Edwards, J.W.; Rifas-Shiman, S.L. Racial/ethnic differences in early-life risk factors for childhood obesity. Pediatrics 2010, 125, 686–695. [Google Scholar] [CrossRef] [PubMed]
- Flores, G.; Lin, H. Factors predicting severe childhood obesity in kindergarteners. Int. J. Obes. (Lond.) 2013, 37, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Wroten, K.C.; O’Neil, C.E.; Stuff, J.E.; Liu, Y.; Nicklas, T.A. Resemblance of Dietary Intakes of Snacks, Sweets, Fruit, and Vegetables among Mother-Child Dyads from Low Income Families. Appetite 2012, 59, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Kral, T.V.; Rauh, E.M. Eating behaviors of children in the context of their family environment. Physiol. Behav. 2010, 100, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Hurley, K.M.; Cross, M.B.; Hughes, S.O. A systematic review of responsive feeding and child obesity in high-income countries. J. Nutr. 2011, 141, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Taveras, E.M.; Rifas-Shiman, S.L.; Belfort, M.B.; Kleinman, K.P.; Oken, E.; Gillman, M.W. Weight status in the first 6 months of life and obesity at 3 years of age. Pediatrics 2009, 123, 1177–1183. [Google Scholar] [CrossRef] [PubMed]
- Kiefner-Burmeister, A.E.; Hoffmann, D.A.; Meers, M.R.; Koball, A.M.; Musher-Eizenman, D.R. Food consumption by young children: A function of parental feeding goals and practices. Appetite 2014, 74, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Rhee, K. Childhood Overweight and the Relationship between Parent Behaviors, Parenting Style, and Family Functioning. Ann. Am. Acad. Pol. Soc. Sci. 2008, 615, 11–37. [Google Scholar] [CrossRef]
- Dovey, T.M.; Staples, P.A.; Gibson, E.L.; Halford, J.C. Food neophobia and “picky/fussy” eating in children: A review. Appetite 2008, 50, 181–193. [Google Scholar] [CrossRef] [PubMed]
- Taveras, E.M.; Blaine, R.E.; Davison, K.K.; Gortmaker, S.; Anand, S.; Falbe, J.; Kwass, J.-A.; Perkins, M.; Giles, C.; Criss, S. Design of the Massachusetts Childhood Obesity Research Demonstration (MA-CORD) Study. Child. Obes. 2015, 11, 11–22. [Google Scholar] [PubMed]
- Davison, K.K.; Falbe, J.; Taveras, E.M.; Gortmaker, S.; Kulldorff, M.; Perkins, M.; Blaine, R.E.; Franckle, R.L.; Ganter, C.; Woo Baidal, J. Evaluation Overview for the Massachusetts Childhood Obesity Research Demonstration (MA-CORD) Project. Child. Obes. 2015, 11, 23–26. [Google Scholar] [PubMed]
- Vaughn, A.E.; Tabak, R.G.; Bryant, M.J.; Ward, D.S. Measuring parent food practices: A systematic review of existing measures and examination of instruments. Int. J. Behav. Nutr. Phys. Act. 2013, 10, 61. [Google Scholar] [CrossRef] [PubMed]
- Blum, R.E.; Wei, E.K.; Rockett, H.R.; Langeliers, J.D.; Leppert, J.; Gardner, J.D.; Colditz, G.A. Validation of a food frequency questionnaire in Native American and Caucasian children 1 to 5 years of age. Mater. Child Health J. 1999, 3, 167–172. [Google Scholar] [CrossRef]
- Miller, S.A.; Taveras, E.M.; Rifas-Shiman, S.L.; Gillman, M.W. Association between television viewing and poor diet quality in young children. Int. J. Pediatr. Obes. 2008, 3, 168–176. [Google Scholar] [CrossRef] [PubMed]
- McGuire, S. Institute of Medicine. 2012. Accelerating progress in obesity prevention: Solving the weight of the nation. Adv. Nutr. 2012, 3, 708–709. [Google Scholar] [CrossRef] [PubMed]
- Ludwig, D.S.; Peterson, K.E.; Gortmaker, S.L. Relation between consumption of sugar-sweetened drinks and childhood obesity: A prospective, observational analysis. Lancet 2001, 357, 505–508. [Google Scholar] [CrossRef]
- Wojcicki, J.M.; Heyman, M.B. Reducing childhood obesity by eliminating 100% fruit juice. Am. J. Public Health 2012, 102, 1630–1633. [Google Scholar] [CrossRef] [PubMed]
- Blumberg, S.J.; Bialostosky, K.; Hamilton, W.L.; Briefel, R.R. The effectiveness of a short form of the Household Food Security Scale. Am. J. Public Health 1999, 89, 1231–1234. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau: Poverty Thresholds. Available online: http://www.census.gov/hhes/www/poverty/data/threshld/index.html (accessed on 23 March 2015).
- Blake, C.E.; Fisher, J.O.; Ganter, C.; Younginer, N.; Orloski, A.; Blaine, R.E.; Bruton, Y.; Davison, K.K. A qualitative study of parents’ perceptions and use of portion size strategies for preschool children’s snacks. Appetite 2015, 88, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Anzman, S.L.; Rollins, B.Y.; Birch, L.L. Parental influence on children’s early eating environments and obesity risk: Implications for prevention. Int. J. Obes. (Lond.) 2010, 34, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Vereecken, C.A.; Keukelier, E.; Maes, L. Influence of mother’s educational level on food parenting practices and food habits of young children. Appetite 2004, 43, 93–103. [Google Scholar] [CrossRef] [PubMed]
- Fisher, J.; Wright, G.; Herman, A.; Malhotra, K.; Serrano, E.; Foster, G.; Whitaker, R. “Snacks are not food”. Low-income, urban mothers’ perceptions of feeding snacks to their preschool-aged children. Appetite 2015, 84, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Sussner, K.M.; Lindsay, A.C.; Greaney, M.L.; Peterson, K.E. The influence of immigrant status and acculturation on the development of overweight in Latino families: A qualitative study. J. Immigr. Minor. Health/Center for Minor. Public Health 2008, 10, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Younginer, N.; Blake, C.; Orlet Fisher, J.; Blaine, R.E.; Ganter, C.; Oroloski, A.; Davison, K. “When I Say the Word “Snack” What Do You Think Of?” Towards a Cohesive Definition of Snacks among Low-Income Caregivers of Preschool-age Children. 2015; in press. [Google Scholar]
- Agostoni, C.; Braegger, C.; Decsi, T.; Kolacek, S.; Koletzko, B.; Mihatsch, W.; Moreno, L.A.; Puntis, J.; Shamir, R.; Szajewska, H. Role of dietary factors and food habits in the development of childhood obesity: A commentary by the ESPGHAN Committee on Nutrition. J. Pediatr. Gastroenterol. Nutr. 2011, 52, 662–669. [Google Scholar] [CrossRef] [PubMed]
- Alvina, M.; Araya, H. Rapid carbohydrate digestion rate produced lesser short-term satiety in obese preschool children. Eur. J. Clin. Nutr. 2004, 58, 637–642. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.; Brand, M.J.; Petocz, P. Interrelationships among postprandial satiety, glucose and insulin responses and changes in subsequent food intake. Eur. J. Clin. Nutr. 1996, 50, 788–797. [Google Scholar] [PubMed]
- Wansink, B.; Shimizu, M.; Brumberg, A. Association of nutrient-dense snack combinations with calories and vegetable intake. Pediatrics 2013, 131, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Sharkey, J.R.; Nalty, C.; Johnson, C.M.; Dean, W.R. Children’s very low food security is associated with increased dietary intakes in energy, fat, and added sugar among Mexican-origin children (6–11 year) in Texas border Colonias. BMC Pediatr. 2012, 12, 16. [Google Scholar] [CrossRef] [PubMed]
- Holben, D. Position of the American Dietetic Association: Food Insecurity in the United States. J. Am. Diet. Assoc. 2010, 110, 1368–1377. [Google Scholar] [CrossRef] [PubMed]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Hwang, L.-D.; Barton, S.; McLaury, K.C.; Dennett, C.C.; Ahern, K.C. Socioeconomic trends in household food expenditures: Comparing objective food shopping receipts vs. self-reports. Statistics 2014, 2010, 1997–1999. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blaine, R.E.; Fisher, J.O.; Taveras, E.M.; Geller, A.C.; Rimm, E.B.; Land, T.; Perkins, M.; Davison, K.K. Reasons Low-Income Parents Offer Snacks to Children: How Feeding Rationale Influences Snack Frequency and Adherence to Dietary Recommendations. Nutrients 2015, 7, 5982-5999. https://doi.org/10.3390/nu7075265
Blaine RE, Fisher JO, Taveras EM, Geller AC, Rimm EB, Land T, Perkins M, Davison KK. Reasons Low-Income Parents Offer Snacks to Children: How Feeding Rationale Influences Snack Frequency and Adherence to Dietary Recommendations. Nutrients. 2015; 7(7):5982-5999. https://doi.org/10.3390/nu7075265
Chicago/Turabian StyleBlaine, Rachel E., Jennifer Orlet Fisher, Elsie M. Taveras, Alan C. Geller, Eric B. Rimm, Thomas Land, Meghan Perkins, and Kirsten K. Davison. 2015. "Reasons Low-Income Parents Offer Snacks to Children: How Feeding Rationale Influences Snack Frequency and Adherence to Dietary Recommendations" Nutrients 7, no. 7: 5982-5999. https://doi.org/10.3390/nu7075265
APA StyleBlaine, R. E., Fisher, J. O., Taveras, E. M., Geller, A. C., Rimm, E. B., Land, T., Perkins, M., & Davison, K. K. (2015). Reasons Low-Income Parents Offer Snacks to Children: How Feeding Rationale Influences Snack Frequency and Adherence to Dietary Recommendations. Nutrients, 7(7), 5982-5999. https://doi.org/10.3390/nu7075265