Antioxidant Activity and Nutritional Status in Anorexia Nervosa: Effects of Weight Recovery

Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Study Design and Procedure
2.3. Nutritional Intake
2.4. Anthropometric and Body Mass Index Measurements
2.5. Blood Collection and Processing for Biochemical and other Determinations
2.6. Biochemical Parameters Measurements
2.7. Total Antioxidant Capacity Measurements
2.8. Antioxidant Enzymes Activity Measurements
2.9. Data Analysis
3. Results
3.1. AN Patients’ Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time 0 | Time 1 | |
|---|---|---|
| Body Mass Index (kg/m2) | 16.80 ± 1.04 | 19.43 ± 0.70 * |
| Fat mass (%) | 10.24 ± 4.95 | 16.80± 3.78 ** |
| Lean mass (%) | 89.76 ± 4.95 | 83.19 ± 3.77 ** |
| Total body water (%) | 65.59 ± 3.83 | 60.83 ± 2.88 ** |
3.2. Hematological and Biochemical Parameters
| Time 0 | Time 1 | |
|---|---|---|
| Hematological Parameters | ||
| Erythrocytes (million/mm3) | 4.38 ± 0.50 | 4.51 ± 0.52* |
| Hemoglobin (g/100 mL) | 13.29 ± 1.32 | 13.53 ± 1.17 |
| Hematocrit (mL/100 mL) | 40.33 ± 4.17 | 41.32 ± 3.78* |
| Mean Corpuscular Volume (mm3) | 92.33 ± 3.48 | 92.02 ± 4.83 |
| Mean Corpuscular Hemoglobin (pg/cell) | 30.46 ± 1.73 | 30.18 ± 2.27 |
| Mean Corpuscular Hemoglobin Concentration (g/100 mL) | 32.99 ± 1.28 | 32.78 ± 1.36 |
| Leucocytes/mm3 | 6.14 ± 1.53 | 6.33 ± 1.57 |
| Lymphocytes (%) | 40.84 ± 8.21 | 35.25 ± 7.66 ** |
| Biochemical Parameters | ||
| Glucose (mg/dL) | 81.20 ± 8.63 | 84.08 ± 11.42 |
| Urea (mg/dL) | 32.61 ± 8.20 | 32.91 ± 7.74 |
| Creatinine (mg/dL) | 0.71 ± 0.07 | 0.66 ± 0.07 * |
| Albumin (g/dL) | 4.59 ± 0.22 | 4.65 ± 0.25 |
| Prealbumin (mg/dL) | 30.08 ± 2.90 | 30.21 ±3.38 |
| Total proteins (g/100 dL) | 7.10 ± 0.57 | 7.01 ± 0.60 |
| Cholesterol (mg/dL) | 184.20 ± 33.83 | 179.88 ± 39.52 |
| HDL-Cholesterol (mg/dL) | 60.08 ± 18.00 | 68.08 ± 18.31 * |
| LDL-Cholesterol (mg/dL) | 112.04 ± 36.46 | 98.98 ± 31.12 * |
| Triglycerides (mg/dL) | 77.80 ± 39.47 | 66.04 ± 17.89 * |
3.3. Dietary Characteristics
| Time 0 | Time 1 | |
|---|---|---|
| Energy (Kcal/day) | 1341.64 ± 621.36 | 1880.60 ± 454.62 ** |
| Macronutrients (day) | ||
| Proteins (g) | 52.57 ± 21.63 | 104.10 ± 18.95 ** |
| Carbohydrates (g) | 135.25 ± 69.00 | 291.68 ± 57.15 ** |
| Total fat (g) | 62.41 ± 30.19 | 137.80 ± 22.81 ** |
| Micronutrients (day) | ||
| Vitamin B1 (mg) | 0.93 ± 0.47 | 1.83 ± 0.38 ** |
| Vitamin B2 (mg) | 1.31 ± 0.58 | 2.29 ± 0.36 ** |
| Vitamin B3-Niacin (mg) | 22.32 ± 9.61 | 45.43 ± 8.62 ** |
| Vitamin B9-Folic acid (μg) | 196.09 ± 101.76 | 397.92 ± 71.69 ** |
| Vitamin C (mg) | 111.37 ± 62.30 | 194.48 ± 49.51 ** |
| Vitamin A (μg retinol equivalents) | 601.08 ± 307.55 | 1268.20 ± 246.22 ** |
| Retinol (μg) | 260.69 ± 146.38 | 564.00 ± 123.38 ** |
| Beta-carotene (μg) | 1746 ± 960.12 | 3840 ± 1211.38 ** |
| Vitamin E (μg alpha-tocopherol equivalents) | 6.27 ± 3.42 | 11.82 ± 2.90 ** |
| Iron (mg) | 8.89 ± 4.44 | 18.08 ±3.26 ** |
| Magnesium (mg) | 180.02 ± 80.73 | 369.20 ± 61.74 ** |
| Zinc (mg) | 5.77 ± 2.42 | 10.80 ± 1.96 ** |
| Selenium (μg) | 67.67 ± 28.95 | 211.40 ± 29.05 ** |
| Copper (mg) | 0.79 ± 0.37 | 1.71 ± 0.29 ** |
| Manganese (mg) | 1.72 ± 1.30 | 3.34 ± 0.58 ** |
| Beta-sisosterol (mg) | 16.98 ± 13.07 | 37.39 ± 11.85 ** |
| Campesterol (mg) | 1.52 ± 1.34 | 4.05 ± 1.46 ** |
| Stigmasterol (mg) 3.23 ± 2.55 | 7.94 ± 3.29 ** |
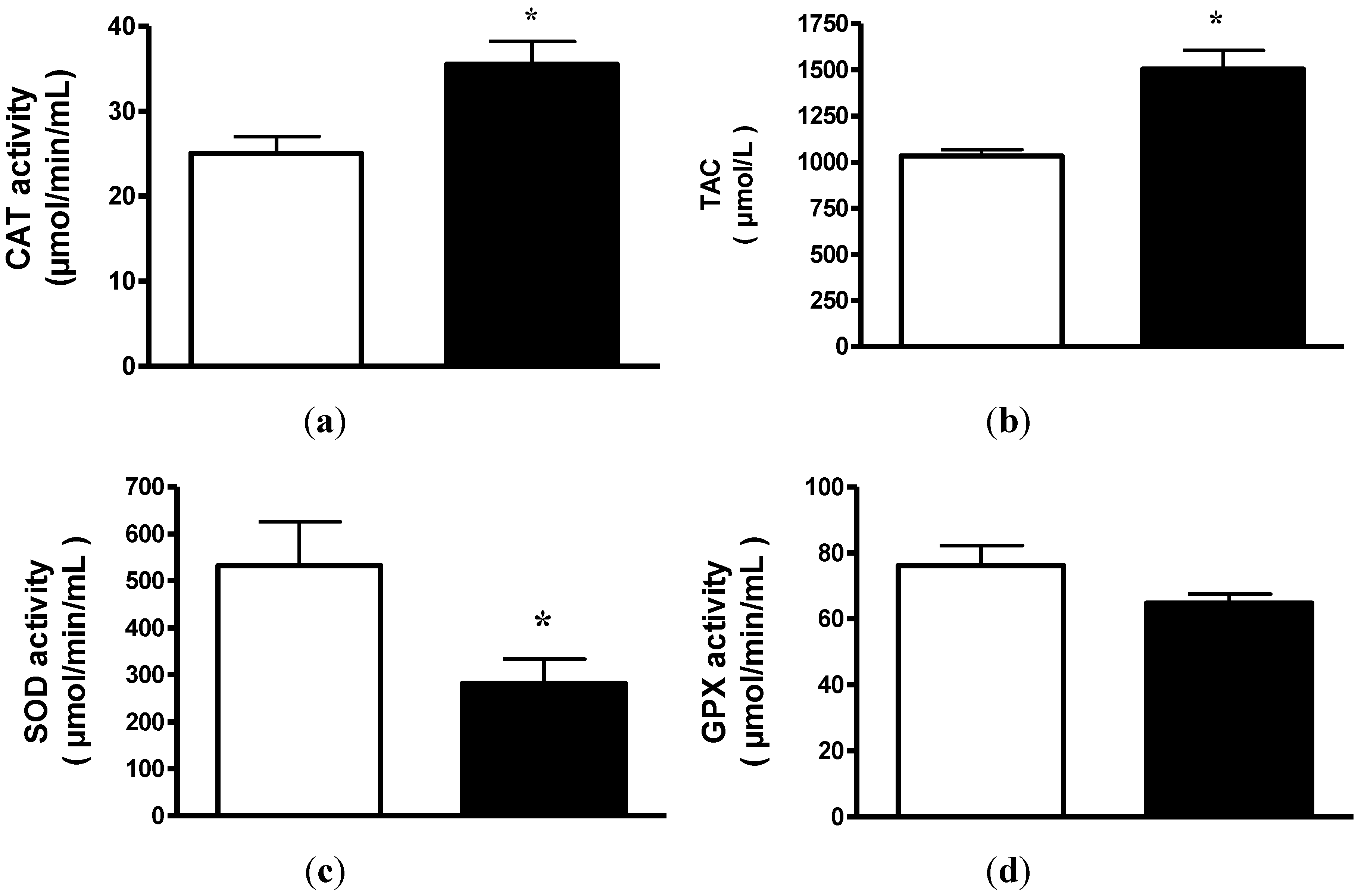
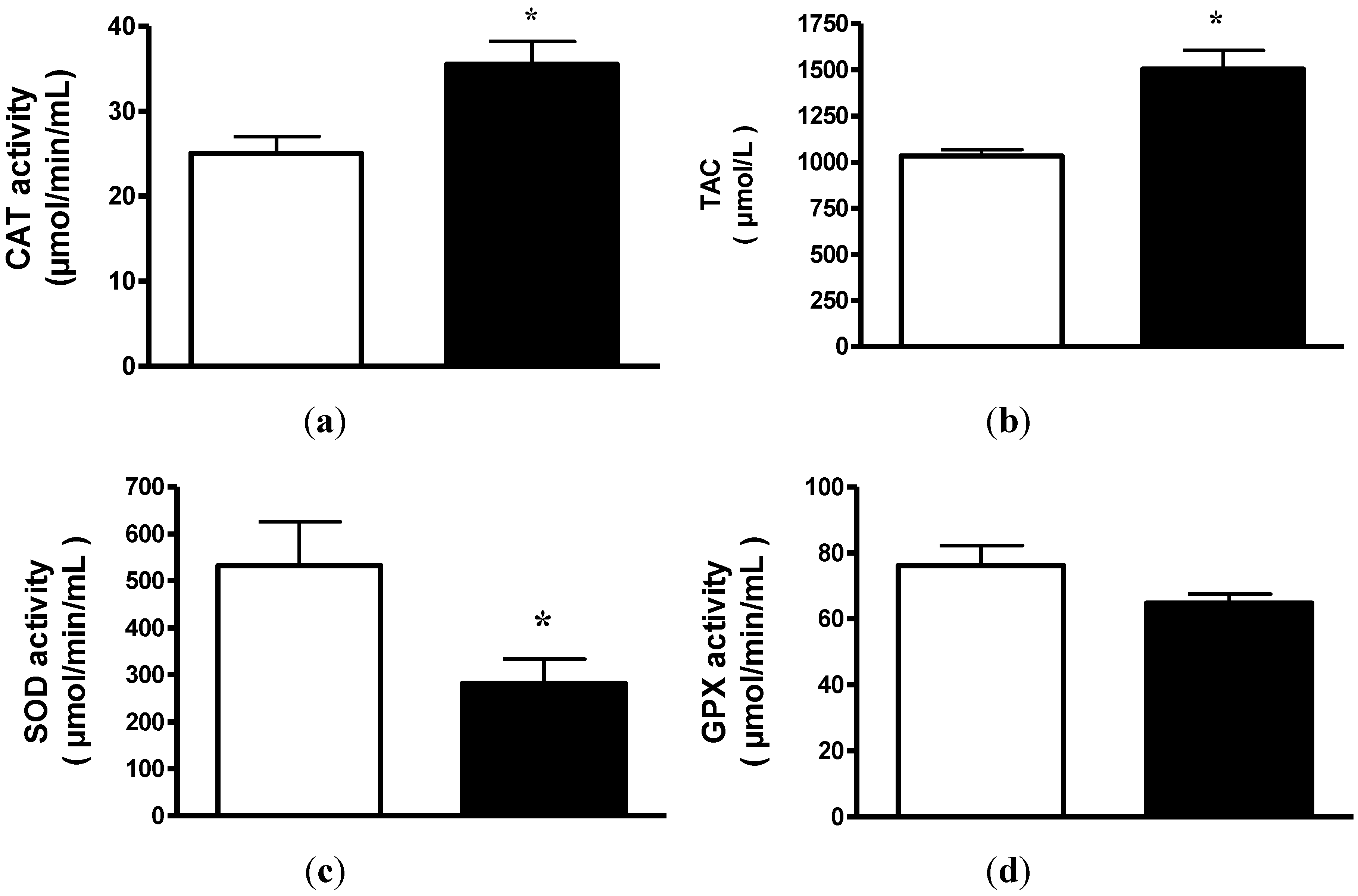
3.4. Plasma Antioxidant Enzymes Activity
3.5. Total Antioxidant Capacity
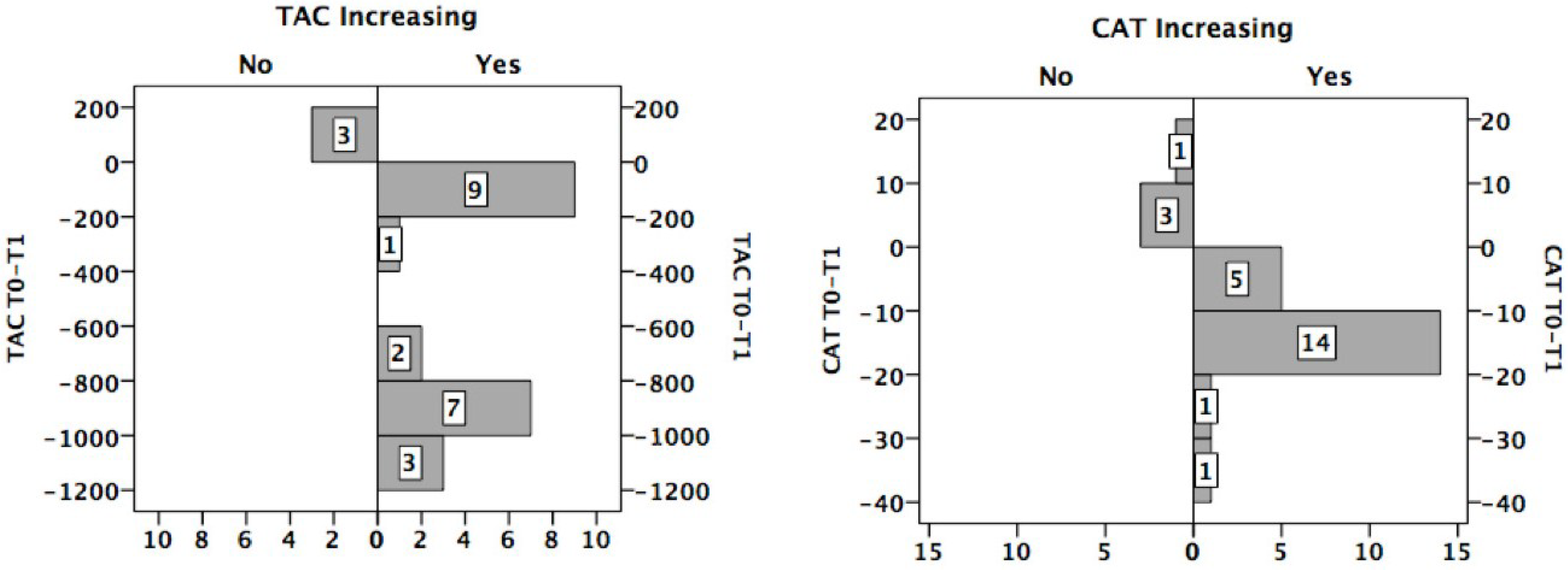
3.6. Distribution of the Sample with Respect to the Change in TAC/CAT
3.7. TAC/CAT Activity and Mineral Ingestion
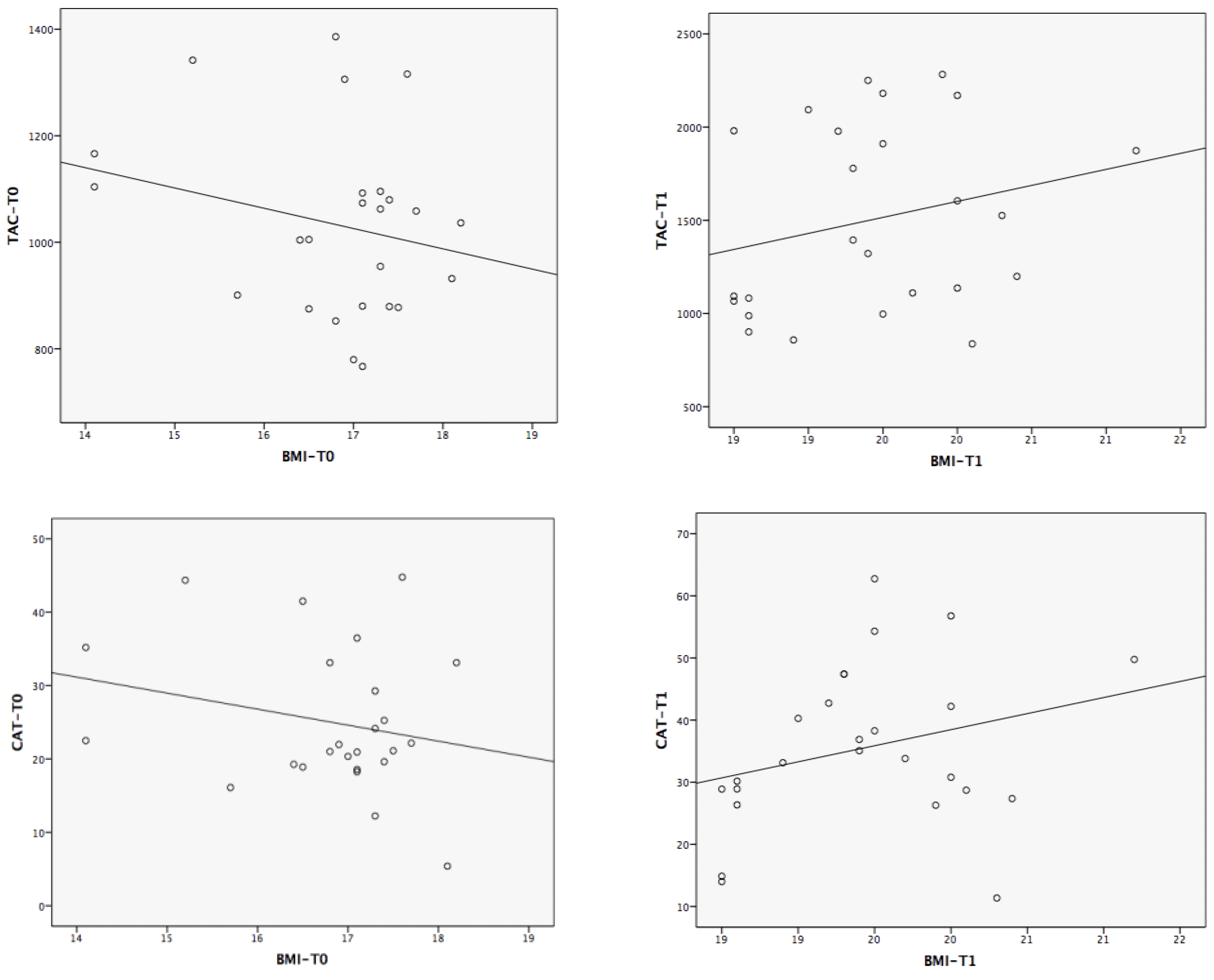
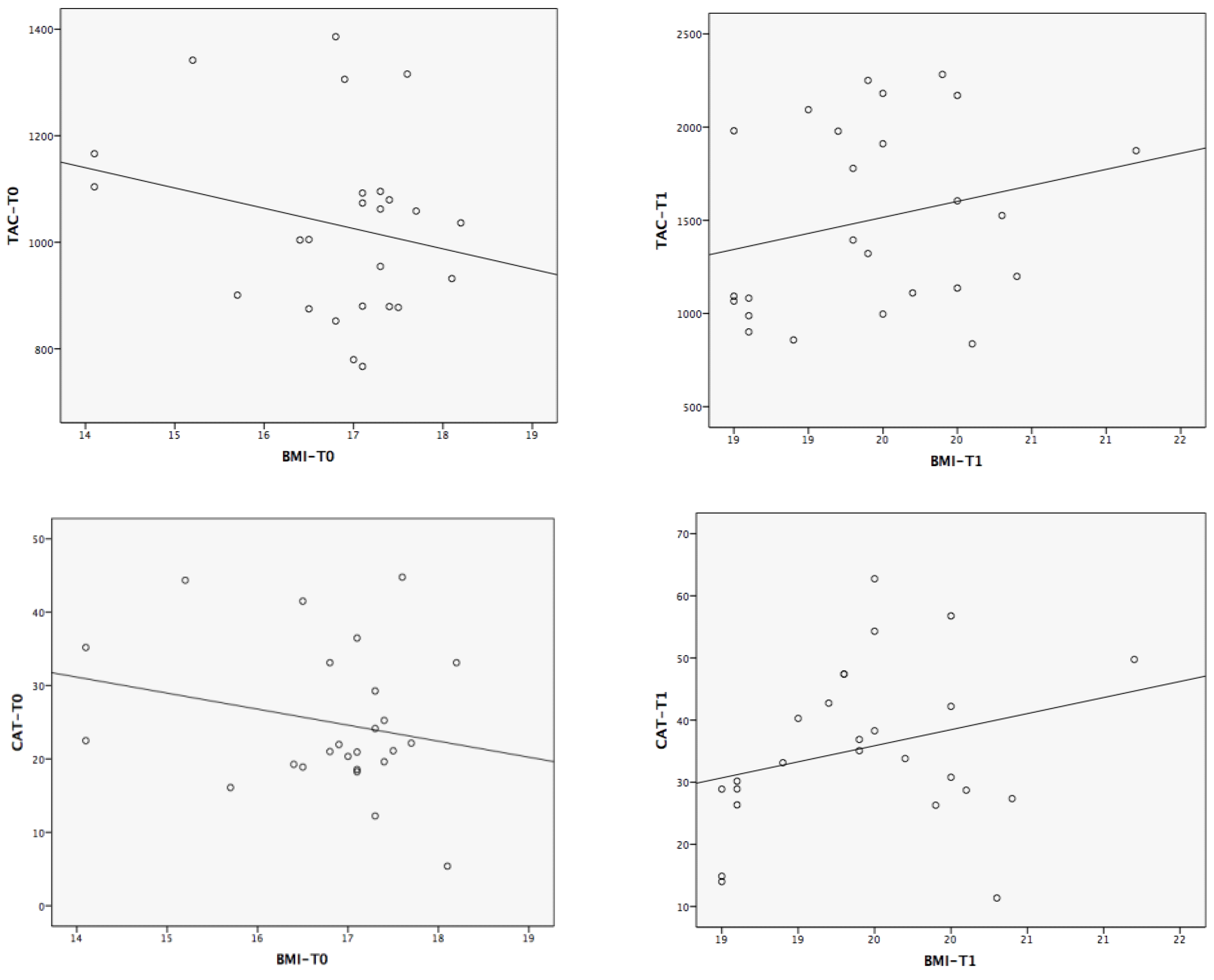
3.8. Correlations between the Magnitude of Change in TAC/CAT and the Experimental Variables
| CAT-Difference (T0 − T1) | TAC-Difference (T0 − T1) | |
|---|---|---|
| Body Mass Index | −0.48 * | −0.25 |
| Nutrients Intake | ||
| Energy | −0.72 ** | −0.15 |
| Proteins | −0.60 ** | −0.21 |
| Vitamin B1 | −0.41 | −0.04 |
| Vitamin B2 | −0.35 | −0.04 |
| Vitamin B3 | −0.51 * | −0.28 |
| Vitamin B9 | −0.45 * | −0.11 |
| Vitamin C | −0.12 | −0.10 |
| Vitamin A | −0.40 | −0.36 |
| Retinol | −0.35 | −0.05 |
| Beta-Carotene | −0.31 | −0.39 |
| Vitamin E | −0.29 | −0.41 |
| Iron | −0.53 * | −0.21 |
| Magnesium | −0.60 ** | −0.25 |
| Zinc | −0.54 * | −0.24 |
| Selenium | −0.35 | −0.39 |
| Copper | −0.76 ** | −0.33 |
| Manganese | −0.59 ** | −0.13 |
| Sisosterol | −0.38 | −0.33 |
| Campesterol | −0.45 * | −0.14 |
| Stigmasterol | −0.33 | −0.13 |
4. Discussion
5. Conclusions
Acknowledgements
Author Contributions
Conflicts of interest
References
- Muñoz, M.Y.; Argente, J. Anorexia nervosa in femaleadolescents: Endocrine and bone mineral densitydisturbances. Eur. J. Endocr. 2002, 147, 275–286. [Google Scholar] [CrossRef]
- Feillet, F.; Feillet-Coudray, C.; Bard, J.M.; Parra, H.J.; Favre, E.; Kabuth, B.; Fruchart, J.C.; Vidailhet, M. Plasma cholesterol and endogenous cholesterol synthesis during refeeding in anorexia nervosa. Clin. Chim. Acta 2000, 294, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Jáuregui-Garrido, B.; Bolaños-Ríos, P.; Santiago-Fernández, M.J.; Jaúregui-Lobera, I. Lipid profile and cardiovascular risk in anorexia nervosa; the effect of nutritional treatment. Nutr. Hosp. 2012, 27, 908–913. [Google Scholar] [PubMed]
- Misra, M.; Tsai, P.; Anderson, E.J.; Hubbard, J.L.; Gallagher, K.; Soyka, L.A.; Miller, K.K.; Herzog, D.B.; Klibanski, A. Nutrient intake in community-dwelling adolescent girls with anorexia nervosa and in healthy adolescents. Am. J. Clin. Nutr. 2006, 84, 698–706. [Google Scholar] [PubMed]
- Hadigan, C.; Anderson, E.; Miller, K.; Hubbard, J.; Herzog, D.; Klibanski, A.; Grinspoon, S.K. Assessment of macronutrient and micronutrient intake in women with anorexia nervosa. Int. J. Eat. Disord. 2000, 28, 284–292. [Google Scholar] [CrossRef] [PubMed]
- Beaumont, P.; Chambers, T.; Rouse, L.; Abraham, S. The diet composition and nutritional knowledge of patients with anorexia nervosa. J. Hum. Nutr. 1981, 35, 265–273. [Google Scholar] [PubMed]
- Schebendach, J.E.; Mayer, L.E.; Devlin, M.J.; Attia, E.; Contento, I.R.; Wolf, R.L.; Walsh, B.T. Dietary energy density and diet variety as predictors of outcome in anorexia nervosa. Am. J. Clin. Nutr. 2008, 87, 810–816. [Google Scholar] [PubMed]
- Nova, E.; Varela, P.; López-Vidriero, I.; Toro, O.; Ceñal, M.J.; Casas, J.; Marcos, A. A one-year follow-up study in anorexia nervosa. Dietary pattern and anthropometrical evolution. Eur. J. Clin. Nutr. 2001, 55, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Affenito, S.G.; Dohm, F.A.; Crawford, P.B.; Daniels, S.R.; Striegel-Moore, R.H. Macronutrient intake in anorexia nervosa: The National Heart, Lung, and Blood Institute Growth and Health Study. J. Pediatr. 2002, 141, 701–705. [Google Scholar] [CrossRef] [PubMed]
- Winston, A.P. The clinical biochemistry of anorexia nervosa. Ann. Clin. Biochem. 2012, 49, 132–143. [Google Scholar] [CrossRef] [PubMed]
- Moyano, D.; Sierra, C.; Brandi, N.; Artuch, R.; Mira, A.; García-Tornel, S.; Vilaseca, M.A. Antioxidant status in anorexia nervosa. Int. J. Eat. Disord. 1999, 25, 99–103. [Google Scholar] [CrossRef] [PubMed]
- Jáuregui-Lobera, I.; Ezquerra-Cabrera, M.; Carbonero-Carreño, R.; Ruiz-Prieto, I. Weight misperception, self-reported physical fitness, dieting and some psychological variables as risk factors for eating disorders. Nutrients 2013, 5, 4486–4502. [Google Scholar] [CrossRef] [PubMed]
- Nova, E.; Samartin, S.; Gomez, S.; Morande, G.; Marcos, A. The adaptive response of the immune system to the particular malnutrition of eating disorders. Eur. J. Clin. Nutr. 2002, 56, S34–S37. [Google Scholar] [CrossRef] [PubMed]
- Celik, M.; Sermatov, K.; Abuhandan, M.; Zeyrek, D.; Kocyigit, A.; Iscan, A. Oxidative status and DNA damage in children with marasmic malnutrition. J. Clin. Lab. Anal. 2012, 26, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Ece, A.; Gürkan, F.; Celik, F.; Boşnak, M.; Yel, S.; Balik, H.; Erel, O. Paraoxonase, total antioxidant activity and peroxide levels in marasmic children: Relationships with leptin. Clin. Biochem. 2007, 40, 634–639. [Google Scholar] [CrossRef] [PubMed]
- Catal, F.; Avci, A.; Karadag, A.; Alioglu, B.; Avci, Z. Oxidant and antioxidant status of Turkish marasmic children: A single center study. J. Trace Elem. Med. Biol. 2007, 21, 108–112. [Google Scholar] [CrossRef] [PubMed]
- Shaaban, S.Y.; Nassar, M.F.; Ibrahim, S.A.; Mahmoud, S.E. Impact of nutritional rehabilitation on enzymatic antioxidant levels in protein energy malnutrition. East Mediterr. Health J. 2002, 8, 290–297. [Google Scholar] [PubMed]
- Diagnostic and Statistical Manual of Mental Disorders: DSM IV-RT; American Psychiatric Association: Washington, DC, USA, 2000.
- Scalfi, L.; Potito, A.; Bianchi, L.; Marra, M.; Caldara, A.; Nicolai, E.; Contaldo, F. Body composition changes in patients with anorexia nervosa after complete weight recovery. Eur. J. Clin. Nutr. 2002, 56, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Meguerditchian, C.; Samuelian-Massat, C.; Valéro, R.; Begu-Le Corroller, A.; Fromont, I.; Mancini, J.; Sparrow, J.D.; Poinso, F.; Vialettes, B. The impact of weight normalization on quality of recovery in anorexia nervosa. J. Am. Coll. Nutr. 2009, 28, 397–404. [Google Scholar] [CrossRef] [PubMed]
- Jáuregui-Lobera, I.; Bolaños, P. Revisión del tratamientodietético-nutricional de la anorexia nerviosa. Rev. Med. Chile 2012, 140, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Schebendach, J.E.; Mayer, L.E.; Devlin, M.J.; Attia, E.; Contento, I.R.; Wolf, R.L.; Walsh, T. Food choice and diet variety in weight-restored patients with anorexia nervosa. J. Am. Diet. Assoc. 2011, 111, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Schebendach, J.; Mayer, L.E.; Devlin, M.J.; Attia, E.; Walsh, B.T. Dietary energy density and diet variety as risk factors for relapse in anorexia nervosa: A replication. Int. J. Eat. Disord. 2012, 45, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Birmingham, C.L.; Hlynsky, J.; Whiteside, L.; Geller, J. Caloric requirement for refeedinginpatients with anorexia nervosa: The contribution of anxiety exercise, and cigarette smoking. J. Eat. Disord. 2005, 10, e6–e9. [Google Scholar]
- World Health Organisation (WHO). Obesity: Preventing and Managing the Global Epidemic; WHO Technical Report Series 894; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Programa para la evaluación de dietas y gestión de datos de alimentación; ALCE Ingeniería: Madrid, Spain, 2008.
- Kyle, U.G.; Bosaeus, I.; de Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; et al. Composition of the ESPEN Working Group. Bioelectrical impedance analysis—Part I: Review of principles and methods. Clin.Nutr. 2004, 23, 1226–1243. [Google Scholar] [CrossRef] [PubMed]
- Kyle, U.G.; Bosaeus, I.; de Lorenzo, A.D.; Deurenberg, P.; Elia, M.; Gómez, J.M.; Heitmann, B.L.; Kent-Smith, L.; Melchior, J.C.; Pirlich, M.; Scharfetter, H.; et al. Bioelectrical impedance analysis—Part II: Utilization in clinical practice. Clin. Nutr. 2004, 23, 1430–1453. [Google Scholar] [CrossRef] [PubMed]
- Golden, N.H.; Meyer, W. Nutritional rehabilitation of anorexia nervosa. Goals and dangers. Int. J. Adolesc. Med. Health 2004, 16, 131–144. [Google Scholar] [CrossRef] [PubMed]
- El Ghoch, M.; Calugi, S.; Lamburghini, S.; Dalle Grave, R. Anorexia nervosa and body fat distribution: A systematic review. Nutrients 2014, 6, 3895–3912. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Serra, E.; Andrés-Perpiña, S.; Lázaro-García, L.; Castro-Fornieles, J. Adolescent anorexia nervosa: Cognitive performance after weight recovery. J. Psychosom. Res. 2014, 76, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Cumurcu, B.E.; Ozyurt, H.; Etikan, I.; Demir, S.; Karlidag, R. Total antioxidant capacity and total oxidant status in patients with major depression: Impact of antidepressant treatment. Psychiatry Clin. Neurosci. 2009, 63, 639–645. [Google Scholar] [CrossRef] [PubMed]
- Kolling, J.; Scherer, E.B.; da Cunha, A.A.; da Cunha, M.J.; Wyse, A.T. Homocysteine induces oxidative-nitrative stress in heart of rats: Prevention by folic acid. Cardiovasc. Toxicol. 2011, 11, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Dandana, A.; Ferchichi, S.; Addad, F.; Jaidane, Z.; Chahed, H.; Gammoudi, I.; Chalghoum, A.; Bricca, G.; Miled, A. Evaluation of oxidative stress among coronary diabetics patients. Acta Biomed. 2011, 82, 187–196. [Google Scholar] [PubMed]
- Kim, Y.J.; Ahn, Y.H.; Lim, Y.; Kim, J.Y.; Kim, J.; Kwon, O. Daily nutritional dose supplementation with antioxidant nutrients and phytochemicals improves DNA and LDLstability: A double-blind, randomized, and placebo-controlled trial. Nutrients 2013, 5, 5218–5232. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Yang, M.; Lee, S.G.; Davis, C.G.; Koo, S.I.; Chun, O.K. Dietary total antioxidant capacity is associated with diet and plasma antioxidant status in healthy young adults. J. Acad. Nutr. Diet. 2012, 112, 1626–1635. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Chung, S.J.; Floegel, A.; Song, W.O.; Koo, S.I.; Chun, O.K. Dietary antioxidant capacity is associated with improved serum antioxidant status and decreased serum C-reactive protein and plasma homocysteine concentrations. Eur. J. Nutr. 2013, 52, 1901–1911. [Google Scholar] [CrossRef] [PubMed]
- Wesson, R.N.; Sparaco, A.; Smith, M.D. Chronic pancreatitis in a patient with malnutrition due to anorexia nervosa. JOP 2008, 9, 327–331. [Google Scholar] [PubMed]
- Theys, N.; Clippe, A.; Bouckenooghe, T.; Reusens, B.; Remacle, C. Early low protein diet aggravates unbalance between antioxidant enzymes leading to islet dysfunction. PLoS ONE 2009, 4, e6110. [Google Scholar] [CrossRef] [PubMed]
- Casado, A.; de la Torre, R.; López-Fernández, E.; Carrascosa, D.; Venarucci, D. Superoxidedismutase and catalaselevels in diseases of theaged. Gac. Med. Mex. 1998, 134, 539–544. [Google Scholar] [PubMed]
- Flores-Mateo, G.; Carrillo-Santisteve, P.; Elosua, R.; Guallar, E.; Marrugat, J.; Bleys, J.; Covas, M.I. Antioxidant enzyme activity and coronary heart disease: Meta-analyses of observational studies. Am. J. Epidemiol. 2009, 170, 135–147. [Google Scholar] [CrossRef] [PubMed]
- Jiao, Y.; Zhang, J.; Yan, J.; Stuart, J.; Gibson, G.; Lu, L.; Williams, R.; Wang, Y.J.; Gu, W. Differential gene expression between wild-type and Gulo-deficient mice supplied with vitamin C. Genet. Mol. Biol. 2011, 34, 386–395. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.H.; Liu, P.J.; Hsia, S.; Chuang, C.J.; Chen, P.C. Role of certain trace minerals in oxidative stress, inflammation, CD4/CD8 lymphocyte ratios and lung function in asthmatic patients. Ann. Clin. Biochem. 2011, 48, 344–351. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Castro, J.; López-Frías, M.R.; Campos, M.S.; López-Frías, M.; Alférez, M.J.; Nestares, T.; Ojeda, M.L.; López-Aliaga, I. Severe nutricional iron-deficiency anaemia has a negative effect on some bone turnover biomarkers in rats. Eur. J. Nutr. 2012, 51, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Sofic, E.; Rustembegovic, A.; Kroyer, G.; Cao, G. Serum antioxidant capacity in neurological, psychiatric, renal diseases and cardiomyopathy. J. Neural. Transm. 2002, 109, 711–719. [Google Scholar] [CrossRef] [PubMed]
- Ashour, M.N.; Salem, S.I.; el-Gadban, H.M.; Elwan, N.M.; Basu, T.K. Antioxidant status in children with protein-energy malnutrition (PEM) living in Cairo, Egypt. Eur. J. Clin. Nutr. 1999, 53, 669–673. [Google Scholar] [CrossRef] [PubMed]
- Noor, R.; Mittal, S.; Iqbal, J. Superoxide dismutase-applications and relevance to human diseases. Med. Sci. Moni. 2002, 8, 210–215. [Google Scholar]
- Atli, T.; Keven, K.; Avci, A.; Kutlay, S.; Turkcapar, N.; Varli, M.; Aras, S.; Ertug, E.; Canbolat, O. Oxidative stress and antioxidant status in elderly diabetes mellitus and glucose intolerance patients. Arch. Gerontol. Geriatr. 2004, 39, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Badid, N.; Ahmed, F.; Merzouk, H.; Belbraouet, S.; Mokhtari, N.; Merzouk, S.; Benhabib, R.; Hamzaoui, D.; Narce, M. Oxidant/antioxidant status, lipids and hormonal profile in overweight women with breast cancer. Pathol. Oncol. Res. 2010, 16, 159–167. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliveras-López, M.-J.; Ruiz-Prieto, I.; Bolaños-Ríos, P.; De la Cerda, F.; Martín, F.; Jáuregui-Lobera, I. Antioxidant Activity and Nutritional Status in Anorexia Nervosa: Effects of Weight Recovery. Nutrients 2015, 7, 2193-2208. https://doi.org/10.3390/nu7042193
Oliveras-López M-J, Ruiz-Prieto I, Bolaños-Ríos P, De la Cerda F, Martín F, Jáuregui-Lobera I. Antioxidant Activity and Nutritional Status in Anorexia Nervosa: Effects of Weight Recovery. Nutrients. 2015; 7(4):2193-2208. https://doi.org/10.3390/nu7042193
Chicago/Turabian StyleOliveras-López, María-Jesús, Inmaculada Ruiz-Prieto, Patricia Bolaños-Ríos, Francisco De la Cerda, Franz Martín, and Ignacio Jáuregui-Lobera. 2015. "Antioxidant Activity and Nutritional Status in Anorexia Nervosa: Effects of Weight Recovery" Nutrients 7, no. 4: 2193-2208. https://doi.org/10.3390/nu7042193
APA StyleOliveras-López, M.-J., Ruiz-Prieto, I., Bolaños-Ríos, P., De la Cerda, F., Martín, F., & Jáuregui-Lobera, I. (2015). Antioxidant Activity and Nutritional Status in Anorexia Nervosa: Effects of Weight Recovery. Nutrients, 7(4), 2193-2208. https://doi.org/10.3390/nu7042193