The Role for Dietary Omega-3 Fatty Acids Supplementation in Older Adults

Abstract
:1. Introduction
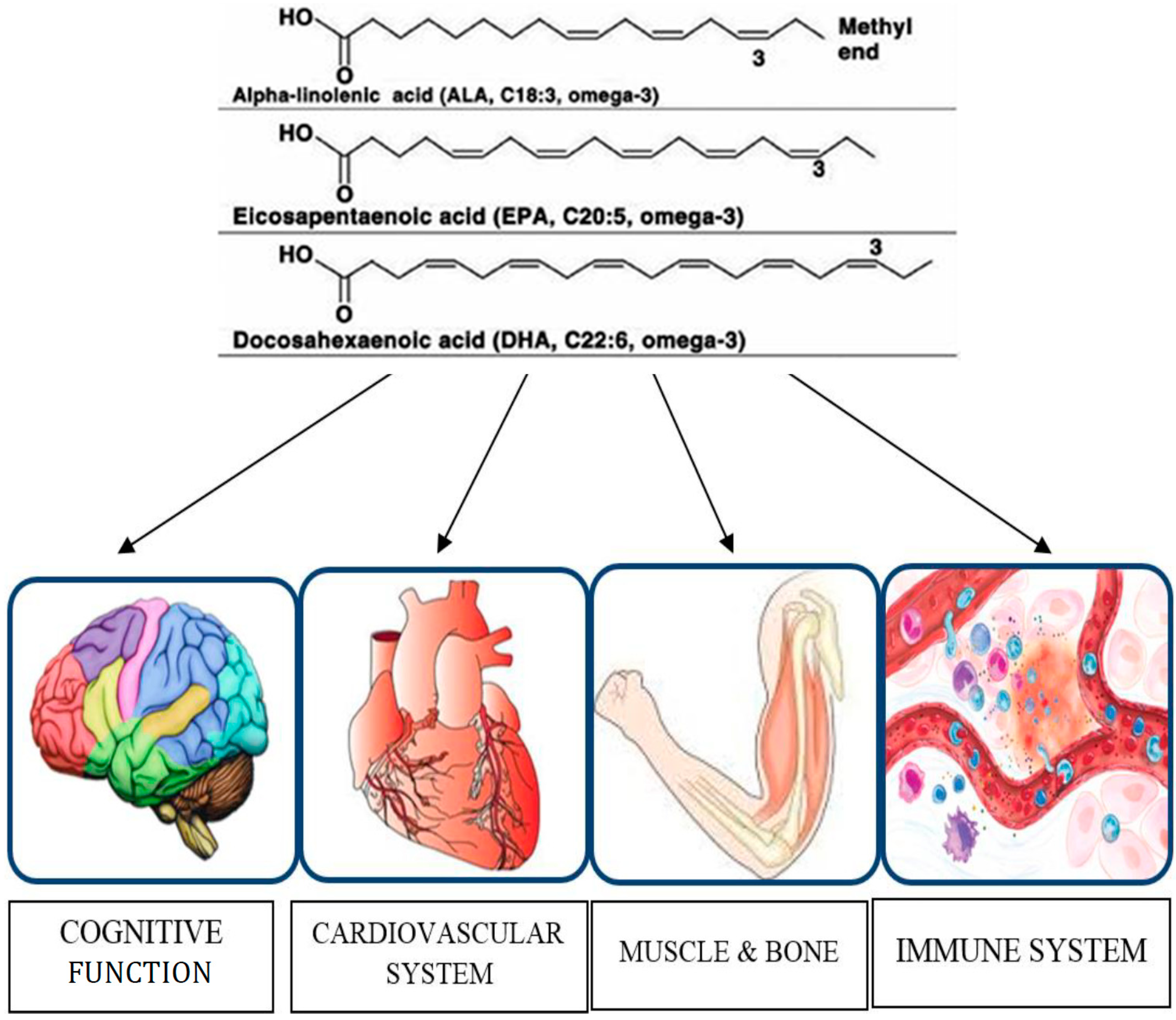
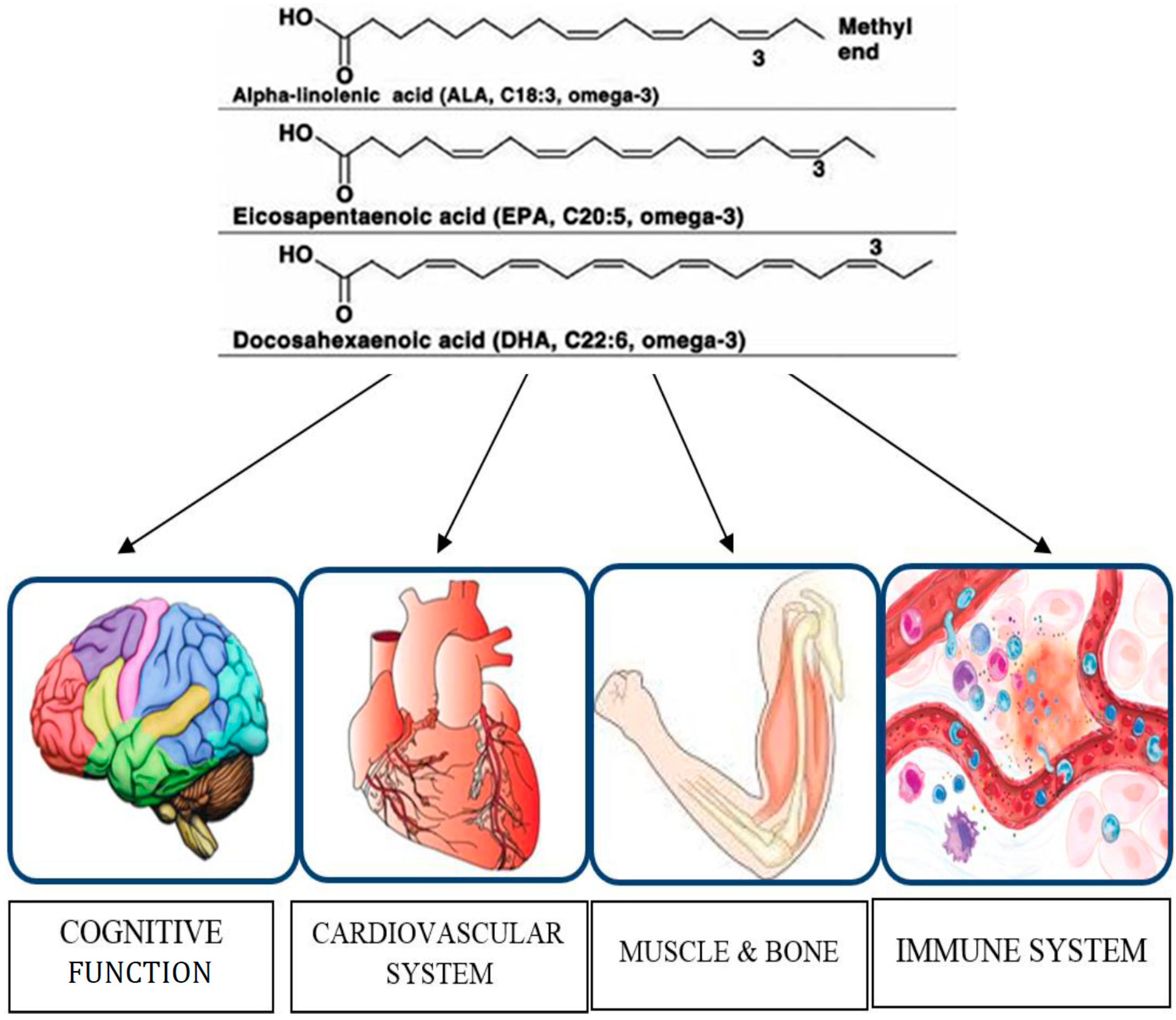
2. Effects of Omega-3 PUFAs on Brain Function
2.1. Dementia
2.2. Depression and Cognitive Function
3. Effects of Omega-3 PUFAs on Cardiovascular System
3.1. Atherosclerosis
3.2. Arrhythmias

{kind=link}
| Function | Summary of Positive Effects | Reference(s) |
|---|---|---|
| Cognitive (9 positive studies, 3 negative studies) | Incidence of dementia ↓ | [20] |
| Immediate and delayed verbal recognition memory scores ↑ | [21] | |
| PAL score ↑ | [21] | |
| Short-term and working memory ↑ | [22] | |
| Immediate verbal memory ↑ | [22] | |
| Delayed recall capability ↑ | [22] | |
| 12-month change in memory ↑ | [22] | |
| Verbal fluency scores ↑ | [23] | |
| Memory scores ↑ | [23] | |
| Rate of learning ↑ | [24] | |
| MMSE ↑ | [24] | |
| Olfactory sensitivity assessment ↑ | [24] | |
| Semantic verbal fluency ↑ | [24] | |
| MNA score ↑ | [25] | |
| GDS scores ↑ | [25] | |
| Mental health ↑ | [25] | |
| Verbal fluency ↑ | [25] | |
| Working memory test ↑ | [26] | |
| Immediate and delayed verbal recall ↑ | [27] | |
| Time to copy complex figure ↓ | [27] | |
| Learning abilities ↑ | [27] | |
| Depressive symptomatology ↓ | [32] | |
| Cardiovascular (9 positive studies, 3 negative studies) | Plasma tryacilglycerydes ↓ | [26] |
| Systolic blood pressure ↓ | [26] | |
| Coronary atherosclerosis plaque volume ↓ | [34] | |
| Risk of ICAS ↓ | [36] | |
| Isolated and paired premature ventricular contractions ↓ | [37] | |
| Unstable ventricular tachycardia paroxysms ↓ | [37] | |
| The effect of antiarrhythmic therapy ↑ | [37] | |
| Hearth rate variability ↑ | [37,40] | |
| Red blood cells omega-3 index ↑ | [37] | |
| Glutathione peroxidase activity in atrial tissue ↑ | [39] | |
| Incidence of postoperative atrial fibrillation ↓ | [39] | |
| Cardiac autonomic modulation ↑ | [41] | |
| HF-related total mortality ↓ | [41] | |
| Mean RR interval ↑ | [41] | |
| Standard deviation of all normal-to-normal RR intervals ↑ | [41] | |
| Turbulence slope ↑ | [41] | |
| Very low frequency power ↑ | [41] | |
| Incident CHF risk ↓ | [42] | |
| Percentage of successive normal RR intervals differing by more than 50 ms ↑ | [40] | |
| EPA and DHA in platelet and atrial tissue membranes ↑ | [43] | |
| Immune (7 positive studies, no negative studies) | Proliferative response of T lymphocytes ↑ | [44] |
| Serum IL-10 ↑ | [45] | |
| Serum Tumor necrosis factor-α ↓ | [45] | |
| Serum IL-8 ↓ | [45] | |
| Inflammation ↓ | [45] | |
| Perioperative systemic inflammation ↓ | [43] | |
| Postoperative IL-6 ↓ | [43] | |
| Lymphocyte proliferation ↓ | [46,47] | |
| Lymphocyte particulate phosphodiesterase activity↓ | [47] | |
| Glutathione peroxidase activity ↓ | [47] | |
| Natural killer cell activity ↓ | [48] | |
| Prostaglandin E2 production by mononuclear cells ↓ | [49] | |
| Neutrophil respiratory burst ↓ | [49] | |
| Bone & Muscle (6 positive studies, no negative studies) | Muscle protein synthesis ↑ | [50] |
| BMD ↑ | [51,52] | |
| Knee flexor muscle thickness ↑ | [53] | |
| IL-6 during resistance training ↓ | [53] | |
| Grip strength ↑ | [54] | |
| Lower extremity performance ↑ | [55] | |
| Physical performance ↑ | [55] | |
| Other (2 positive studies, 1 negative study) | Plasma glucose, lactate, blood carboxyhemoglobin after surgery ↓ | [43] |
| Serum adiponectin ↑ | [56] |
4. Effects of Omega-3 PUFAs on Immune Function
4.1. Immune Cell Proliferation
4.2. Pro-Inflammatory Cytokines
4.3. Other Cellular Effects
5. Effects of Omega-3 PUFAs on Muscle Mass and Function
6. Effects of Omega-3 PUFAs on Bone Health
7. Other Effects of Omega-3 PUFAs
8. Conclusions
Conflicts of Interest
References
- LaCroix, A.Z. Editorial: Introducing the 2013 volume of Epidemiologic Reviews on Ageing. Am. J. Epidemiol. 2013, 177, 377–379. [Google Scholar]
- Elia, M.; Jones, B.; Russell, C. Malnutrition in various care settings in the UK: The 2007 Nutrition Screening Week Survey. Clin. Med. 2008, 8, 364–365. [Google Scholar]
- Briefel, R.R.; McDowell, M.A.; Alaimo, K.; Caughman, C.R.; Bischof, A.L.; Carroll, M.D.; Johnson, C.L. Total energy intake of the US population: The third National Health and Nutrition Examination Survey, 1988–1991. Am. J. Clin. Nutr. 1995, 62, 1072S–1080S. [Google Scholar]
- Knoops, K.T.; de Groot, L.C.; Kromhout, D.; Perrin, A.E.; Moreiras-Varela, O.; Menotti, A.; van Staveren, W.A. Mediterranean diet, lifestyle factors, and 10-year mortality in elderly european men and women, the HALE project. JAMA 2004, 292, 1433–1439. [Google Scholar]
- Kozlowska, K.; Szczecinska, A.; Roszkowski, W.; Brzozowska, A.; Alfonso, C.; Fjellstrom, C.; Morais, C.; Nielsen, N.A.; Pfau, C.; Saba, A.; et al. Patterns of healthy lifestyle and positive health attitudes in older europeans. J. Nutr. Health Ageing 2008, 12, 728–733. [Google Scholar]
- Wakimoto, P.; Block, G. Dietary intake, dietary patterns, and changes with age: An epidemiological perspective. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, 65–80. [Google Scholar]
- Dean, M.; Raats, M.M.; Grunert, K.G.; Lumbers, M.; Food in later life team. Factors influencing eating a varied diet in old age. Public Health Nutr. 2009, 12, 2421–2427. [Google Scholar]
- Patenaude, A.; Rodriguez-Leyva, D.; Edel, A.L.; Dibrov, E.; Dupasquier, C.M.; Austria, J.A.; Richard, M.N.; Chahine, M.N.; Malcolmson, L.J.; Pierce, G.N. Bioavailability of alpha-linolenic acid from flaxseed diets as a function of the age of the subject. Eur. J. Clin. Nutr. 2009, 63, 1123–1129. [Google Scholar]
- Swanson, D.; Block, R.; Mousa, S.A. Omega-3 fatty acids EPA and DHA: Health benefits throughout life. Adv. Nutr. 2012, 3, 1–7. [Google Scholar]
- Buhr, G.; Bales, C.W. Nutritional supplements for older adults: Review and recommendations—Part I. J. Nutr. Elder. 2009, 28, 5–29. [Google Scholar]
- Burdge, G.C. Metabolism of alpha-linolenic acid in humans. Prostaglandins Leukot. Essent. Fat. Acids 2006, 75, 161–168. [Google Scholar]
- Ubeda, N.; Achon, M.; Varela-Moreiras, G. Omega 3 fatty acids in the elderly. Br. J. Nutr. 2012, 107, S137–S151. [Google Scholar]
- Buhr, G.; Bales, C.W. Nutritional supplements for older adults: Review and recommendations—Part II. J. Nutr. Elder. 2010, 29, 42–71. [Google Scholar]
- Harris, W.S. The omega-3 index: Clinical utility for therapeutic intervention. Curr. Cardiol. Rep. 2010, 12, 503–508. [Google Scholar]
- Katan, M.B.; Deslypere, J.P.; van Birgelen, A.P.; Penders, M.; Zegwaard, M. Kinetics of the incorporation of dietary fatty acids into serum cholesteryl esters, erythrocyte membranes, and adipose tissue: An 18-month controlled study. J. Lipid Res. 1997, 38, 2012–2022. [Google Scholar]
- Harris, W.S.; von Schacky, C. The Omega-3 Index: A new risk factor for death from coronary heart disease? Prev. Med. 2004, 39, 212–220. [Google Scholar]
- Riediger, N.D.; Othman, R.A.; Suh, M.; Moghadasian, M.H. A systemic review of the roles of n-3 fatty acids in health and disease. J. Am. Diet. Assoc. 2009, 109, 668–679. [Google Scholar]
- Lin, P.Y.; Chiu, C.C.; Huang, S.Y.; Su, K.P. A meta-analytic review of polyunsaturated fatty acid compositions in dementia. J. Clin. Psychiatry 2012, 73, 1245–1254. [Google Scholar]
- Rapoport, S.I.; Ramadan, E.; Basselin, M. Docosahexaenoic acid (DHA) incorporation into the brain from plasma, as an in vivo biomarker of brain DHA metabolism and neurotransmission. Prostaglandins Other Lipid Mediat. 2011, 96, 109–113. [Google Scholar]
- Samieri, C.; Féart, C.; Letenneur, L.; Dartigues, J.F.; Pérès, K.; Auriacombe, S.; Peuchant, E.; Delcourt, C.; Barberger-Gateau, P. Low plasma eicosapentaenoic acid and depressive symptomatology are independent predictors of dementia risk. Am. J. Clin. Nutr. 2008, 88, 714–721. [Google Scholar]
- Yurko-Mauro, K.; McCarthy, D.; Rom, D.; Nelson, E.B.; Ryan, A.S.; Blackwell, A.; Salem, N., Jr.; Stedman, M.; MIDAS Investigators. Beneficial effects of docosahexaenoic acid on cognition in age-related cognitive decline. Alzheimers Dement. 2010, 6, 456–464. [Google Scholar]
- Lee, L.K.; Shahar, S.; Chin, A.V.; Yusoff, N.A. Docosahexaenoic acid-concentrated fish oil supplementation in subjects with mild cognitive impairment (MCI): A 12-month randomised, double-blind, placebo-controlled trial. Psychopharmacology 2013, 225, 605–612. [Google Scholar]
- Johnson, E.J.; McDonald, K.; Caldarella, S.M.; Chung, H.Y.; Troen, A.M.; Snodderly, D.M. Cognitive findings of an exploratory trial of docosahexaenoic acid and lutein supplementation in older women. Nutr. Neurosci. 2008, 11, 75–83. [Google Scholar]
- Rondanelli, M.; Opizzi, A.; Faliva, M.; Mozzoni, M.; Antoniello, N.; Cazzola, R.; Savarè, R.; Cerutti, R.; Grossi, E.; Cestaro, B. Effects of a diet integration with an oily emulsion of DHA-phospholipids containing melatonin and tryptophan in elderly patients suffering from mild cognitive impairment. Nutr. Neurosci. 2012, 15, 46–54. [Google Scholar]
- Sinn, N.; Milte, C.M.; Street, S.J.; Buckley, J.D.; Coates, A.M.; Petkov, J.; Howe, P.R. Effects of n-3 fatty acids, EPA v. DHA, on depressive symptoms, quality of life, memory and executive function in older adults with mild cognitive impairment: A 6-month randomised controlled trial. Br. J. Nutr. 2012, 107, 1682–1693. [Google Scholar]
- Nilsson, A.; Radeborg, K.; Salo, I.; Björck, I. Effects of supplementation with n-3 polyunsaturated fatty acids on cognitive performance and cardiometabolic risk markers in healthy 51 to 72 years old subjects: A randomized controlled cross-over study. Nutr. J. 2012, 11, 99. [Google Scholar]
- Vakhapova, V.; Cohen, T.; Richter, Y.; Herzog, Y.; Korczyn, A.D. Phosphatidylserine containing omega-3 fatty acids may improve memory abilities in non-demented elderly with memory complaints: A double-blind placebo-controlled trial. Dement. Geriatr. Cogn. Disord. 2010, 29, 467–474. [Google Scholar]
- Yasuno, F.; Tanimukai, S.; Sasaki, M.; Ikejima, C.; Yamashita, F.; Kodama, C.; Mizukami, K.; Asada, T. Combination of antioxidant supplements improved cognitive function in the elderly. J. Alzheimers Dis. 2012, 32, 895–903. [Google Scholar]
- Phillips, M.A.; Childs, C.E.; Calder, P.C.; Rogers, P.J. Lower omega-3 fatty acid intake and status are associated with poorer cognitive function in older age: A comparison of individuals with and without cognitive impairment and Alzheimer’s disease. Nutr. Neurosci. 2012. [Google Scholar] [CrossRef]
- Dangour, A.D.; Allen, E.; Elbourne, D.; Fasey, N.; Fletcher, A.E.; Hardy, P.; Holder, G.E.; Knight, R.; Letley, L.; Richards, M.; et al. Effect of 2-y n-3 long-chain polyunsaturated fatty acid supplementation on cognitive function in older people: A randomized, double-blind, controlled trial. Am. J. Clin. Nutr. 2010, 91, 1725–1732. [Google Scholar]
- Van de Rest, O.; Geleijnse, J.M.; Kok, F.J.; van Staveren, W.A.; Dullemeijer, C.; Olderikkert, M.G.; Beekman, A.T.; de Groot, C.P. Effect of fish oil on cognitive performance in older subjects: A randomized, controlled trial. Neurology 2008, 71, 430–438. [Google Scholar]
- Féart, C.; Peuchant, E.; Letenneur, L.; Samieri, C.; Montagnier, D.; Fourrier-Reglat, A.; Barberger-Gateau, P. Plasma eicosapentaenoic acid is inversely associated with severity of depressive symptomatology in the elderly: Data from the Bordeaux sample of the Three-City Study. Am. J. Clin. Nutr. 2008, 87, 1156–1162. [Google Scholar]
- Van de Rest, O.; Geleijnse, J.M.; Kok, F.J.; van Staveren, W.A.; Hoefnagels, W.H.; Beekman, A.T.; de Groot, L.C. Effect of fish-oil supplementation on mental well-being in older subjects: A randomized, double-blind, placebo-controlled trial. Am. J. Clin. Nutr. 2008, 88, 706–713. [Google Scholar]
- Nozue, T.; Yamamoto, S.; Tohyama, S.; Fukui, K.; Umezawa, S.; Onishi, Y.; Kunishima, T.; Sato, A.; Nozato, T.; Miyake, S.; et al. Comparison of effects of serum n-3 to n-6 polyunsaturated fatty acid ratios on coronary atherosclerosis in patients treated with pitavastatin or pravastatin undergoing percutaneous coronary intervention. Am. J. Cardiol. 2013, 111, 1570–1575. [Google Scholar]
- Mackay, I.; Ford, I.; Thies, F.; Fielding, S.; Bachoo, P.; Brittenden, J. Effect of Omega-3 fatty acid supplementation on markers of platelet and endothelial function in patients with peripheral arterial disease. Atherosclerosis 2012, 221, 514–520. [Google Scholar]
- Kim, Y.J.; Kim, O.Y.; Cho, Y.; Chung, J.H.; Jung, Y.S.; Hwang, G.S.; Shin, M.J. Plasma phospholipid fatty acid composition in ischemic stroke: Importance of docosahexaenoic acid in the risk for intracranial atherosclerotic stenosis. Atherosclerosis 2012, 225, 418–424. [Google Scholar]
- Gavva, E.M.; Tsaregorodtsev, D.A.; Mamedov, I.S.; Sulimov, V.A. Effect of ω-3 polyunsaturated fatty acids on predictors of sudden cardiac death in patients with ischemic heart disease and ventricular rhythm disturbances. Kardiologiia 2012, 52, 14–21. [Google Scholar]
- Fretts, A.M.; Mozaffarian, D.; Siscovick, D.S.; Heckbert, S.R.; McKnight, B.; King, I.B.; Rimm, E.B.; Psaty, B.M.; Sacks, F.M.; Song, X; et al. Associations of plasma phospholipid and dietary alpha linolenic acid with incident atrial fibrillation in older adults: The Cardiovascular Health Study. J. Am. Heart Assoc. 2013, 2, e003814. [Google Scholar]
- Rodrigo, R.; Gutiérrez, R.; Fernández, R.; Guzmán, P. Ageing improves the antioxidant response against postoperative atrial fibrillation: A randomized controlled trial. Interact. Cardiovasc. Thorac. Surg. 2012, 15, 209–214. [Google Scholar]
- Romieu, I.; Téllez-Rojo, M.M.; Lazo, M.; Manzano-Patiño, A.; Cortez-Lugo, M.; Julien, P.; Bélanger, M.C.; Hernandez-Avila, M.; Holguin, F. Omega-3 fatty acid prevents heart rate variability reductions associated with particulate matter. Am. J. Respir. Crit. Care Med. 2005, 172, 1534–1540. [Google Scholar]
- La Rovere, M.T.; Staszewsky, L.; Barlera, S.; Maestri, R.; Mezzani, A.; Midi, P.; Marchioli, R.; Maggioni, A.P.; Tognoni, G.; Tavazzi, L.; et al. n-3PUFA and Holter-derived autonomic variables in patients with heart failure: Data from the Gruppo Italiano per lo Studio della Sopravvivenza nell’Insufficienza Cardiaca (GISSI-HF) Holter substudy. Heart Rhythm. 2013, 10, 226–232. [Google Scholar]
- Mozaffarian, D.; Lemaitre, R.N.; King, I.B.; Song, X.; Spiegelman, D.; Sacks, F.M.; Rimm, E.B.; Siscovick, D.S. Circulating long-chain ω-3 fatty acids and incidence of congestive heart failure in older adults: The cardiovascular health study: A cohort study. Ann. Intern. Med. 2011, 155, 160–170. [Google Scholar]
- Berger, M.M.; Delodder, F.; Liaudet, L.; Tozzi, P.; Schlaepfer, J.; Chiolero, R.L.; Tappy, L. Three short perioperative infusions of n-3 PUFAs reduce systemic inflammation induced by cardiopulmonary bypass surgery: A randomized controlled trial. Am. J. Clin. Nutr. 2013, 97, 246–254. [Google Scholar]
- Han, S.N.; Lichtenstein, A.H.; Ausman, L.M.; Meydani, S.N. Novel soybean oils differing in fatty acid composition alter immune functions of moderately hypercholesterolemic older adults. J. Nutr. 2012, 142, 2182–2187. [Google Scholar]
- Barros, K.V.; Cassulino, A.P.; Schalch, L.; Munhoz, E.D.; Manetta, J.A.; Calder, P.C.; Silveira, V.L. Pharmaconutrition: Acute fatty acid modulation of circulating cytokines in elderly patients in the ICU. JPEN J. Parenter. Enteral Nutr. 2014, 38, 467–474. [Google Scholar]
- Thies, F.; Nebe-von-Caron, G.; Powell, J.R.; Yaqoob, P.; Newsholme, E.A.; Calder, P.C. Dietary supplementation with gamma-linolenic acid or fish oil decreases T lymphocyte proliferation in healthy older humans. J. Nutr. 2001, 131, 1918–1927. [Google Scholar]
- Bechoua, S.; Dubois, M.; Véricel, E.; Chapuy, P.; Lagarde, M.; Prigent, A.F. Influence of very low dietary intake of marine oil on some functional aspects of immune cells in healthy elderly people. Br. J. Nutr. 2003, 89, 523–531. [Google Scholar]
- Thies, F.; Nebe-von-Caron, G.; Powell, J.R.; Yaqoob, P.; Newsholme, E.A.; Calder, P.C. Dietary supplementation with eicosapentaenoic acid, but not with other long-chain n-3 or n-6 polyunsaturated fatty acids, decreases natural killer cell activity in healthy subjects aged >55 years. Am. J. Clin. Nutr. 2001, 73, 539–548. [Google Scholar]
- Rees, D.; Miles, E.A.; Banerjee, T.; Wells, S.J.; Roynette, C.E.; Wahle, K.W.; Calder, P.C. Dose-related effects of eicosapentaenoic acid on innate immune function in healthy humans: A comparison of young and older men. Am. J. Clin. Nutr. 2006, 83, 331–342. [Google Scholar]
- Smith, G.I.; Atherton, P.; Reeds, D.N.; Mohammed, B.S.; Rankin, D.; Rennie, M.J.; Mittendorfer, B. Dietary omega-3 fatty acid supplementation increases the rate of muscle protein synthesis in older adults: A randomized controlled trial. Am. J. Clin. Nutr. 2011, 93, 402–412. [Google Scholar]
- Rousseau, J.H.; Kleppinger, A.; Kenny, A.M. Self-reported dietary intake of omega-3 fatty acids and association with bone and lower extremity function. J. Am. Geriatr. Soc. 2009, 57, 1781–1788. [Google Scholar]
- Weiss, L.A.; Barrett-Connor, E.; von Mühlen, D. Ratio of n-6 to n-3 fatty acids and bone mineral density in older adults: The Rancho Bernardo Study. Am. J. Clin. Nutr. 2005, 81, 934–938. [Google Scholar]
- Cornish, S.M.; Chilibeck, P.D. Alpha-linolenic acid supplementation and resistance training in older adults. Appl. Physiol. Nutr. Metab. 2009, 34, 49–59. [Google Scholar]
- Robinson, S.M.; Jameson, K.A.; Batelaan, S.F.; Martin, H.J.; Syddall, H.E.; Dennison, E.M.; Cooper, C.; Sayer, A.A.; Hertfordshire Cohort Study Group. Diet and its relationship with grip strength in community-dwelling older men and women: The Hertfordshire cohort study. J. Am. Geriatr. Soc. 2008, 56, 84–90. [Google Scholar]
- Abbatecola, A.M.; Cherubini, A.; Guralnik, J.M.; Andres Lacueva, C.; Ruggiero, C.; Maggio, M.; Bandinelli, S.; Paolisso, G.; Ferrucci, L. Plasma polyunsaturated fatty acids and age-related physical performance decline. Rejuvenation Res. 2009, 12, 25–32. [Google Scholar]
- Alsaleh, A.; Crepostnaia, D.; Maniou, Z.; Lewis, F.J.; Hall, W.L.; Sanders, T.A.; O’Dell, S.D.; MARINA study team. Adiponectin gene variant interacts with fish oil supplementation to influence serum adiponectin in older individuals. J. Nutr. 2013, 143, 1021–1027. [Google Scholar]
- Giltay, E.J.; Geleijnse, J.M.; Heijboer, A.C.; de Goede, J.; Oude Griep, L.M.; Blankenstein, M.A.; Kromhout, D. No effects of n-3 fatty acid supplementation on serum total testosterone levels in older men: The Alpha Omega Trial. Int. J. Androl. 2012, 35, 680–687. [Google Scholar]
- Rennie, M.J. Anabolic resistance in critically ill patients. Crit. Care Med. 2009, 37, S398–S399. [Google Scholar]
- Muscaritoli, M.; Lucia, S.; Molfino, A.; Cederholm, T.; Rossi Fanelli, F. Muscle atrophy in ageing and chronic diseases: Is it sarcopenia or cachexia? Intern. Emerg. Med. 2013, 8, 553–560. [Google Scholar]
- Parekh, N.; Voland, R.P.; Moeller, S.M.; Blodi, B.A.; Ritenbaugh, C.; Chappell, R.J.; Wallace, R.B.; Mares, J.A.; CAREDS Research Study Group. Association between dietary fat intake and age-related macular degeneration in the Carotenoids in Age-Related Eye Disease Study (CAREDS): An ancillary study of the Women’s Health Initiative. Arch. Ophthalmol. 2009, 127, 1483–1493. [Google Scholar]
- Parletta, N.; Milte, C.M.; Meyer, B.J. Nutritional modulation of cognitive function and mental health. J. Nutr. Biochem. 2013, 24, 725–743. [Google Scholar]
- Van de Rest, O.; Geleijnse, J.M.; Kok, F.J.; van Staveren, W.A.; Olderikkert, M.G.; Beekman, A.T.; de Groot, L.C. Effect of fish oil supplementation on quality of life in a general population of older Dutch subjects: A randomized, double-blind, placebo-controlled trial. J. Am. Geriatr. Soc. 2009, 57, 1481–1486. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molfino, A.; Gioia, G.; Fanelli, F.R.; Muscaritoli, M. The Role for Dietary Omega-3 Fatty Acids Supplementation in Older Adults. Nutrients 2014, 6, 4058-4072. https://doi.org/10.3390/nu6104058
Molfino A, Gioia G, Fanelli FR, Muscaritoli M. The Role for Dietary Omega-3 Fatty Acids Supplementation in Older Adults. Nutrients. 2014; 6(10):4058-4072. https://doi.org/10.3390/nu6104058
Chicago/Turabian StyleMolfino, Alessio, Gianfranco Gioia, Filippo Rossi Fanelli, and Maurizio Muscaritoli. 2014. "The Role for Dietary Omega-3 Fatty Acids Supplementation in Older Adults" Nutrients 6, no. 10: 4058-4072. https://doi.org/10.3390/nu6104058
APA StyleMolfino, A., Gioia, G., Fanelli, F. R., & Muscaritoli, M. (2014). The Role for Dietary Omega-3 Fatty Acids Supplementation in Older Adults. Nutrients, 6(10), 4058-4072. https://doi.org/10.3390/nu6104058