Acute Effects of Different Multivitamin Mineral Preparations with and without Guaraná on Mood, Cognitive Performance and Functional Brain Activation

 ,
,
Abstract
:1. Introduction
2. Method
2.1. Design
2.2. Participants
2.3. Treatments

{kind=link}
{kind=link}
{kind=link}
| Berocca Boost | Berocca Performance | |
|---|---|---|
| Vitamin B1 | 1.40 mg | 15 mg |
| Riboflavin (Vitamin B2) | 1.60 mg | 15 mg |
| Nicotinamide (B3/niacin) | 18 mg | 50 mg |
| Vitamin B5 | 6 mg | 23 mg |
| Vitamin B6 | 2 mg | 10 mg |
| Folic Acid (Vitamin B9) | 200 μg | 400 μg |
| Vitamin B12 | 1 μg | 10 μg |
| Biotin (Vitamin B7) | 150 μg | 150 μg |
| Vitamin C | 60 mg | 500 mg |
| Calcium | 100 mg | 100 mg |
| Magnesium | 100 mg | 100 mg |
| Zinc | 9.5 mg | 10 mg |
| Guaraná | 222.2 mg (40 mg of caffeine) |
2.4. Procedure
2.5. Cognitive and Mood Measures
2.5.1. Cognitive Demand Battery
2.5.2. State-Trait Anxiety Inventory [33]—State Portion (STAI-S)
2.5.3. Visual Analogue Mood Scales (VAMS)
2.6. Functional Magnetic Imaging (fMRI) Measures
2.6.1. fMRI Testing Procedure
2.6.2. Imaging Procedures
2.6.3. fMRI Preprocessing
2.6.4. fMRI Modelling: Participant Level Analysis
2.6.5. fMRI Modelling: Participant Level Analysis
3. Results
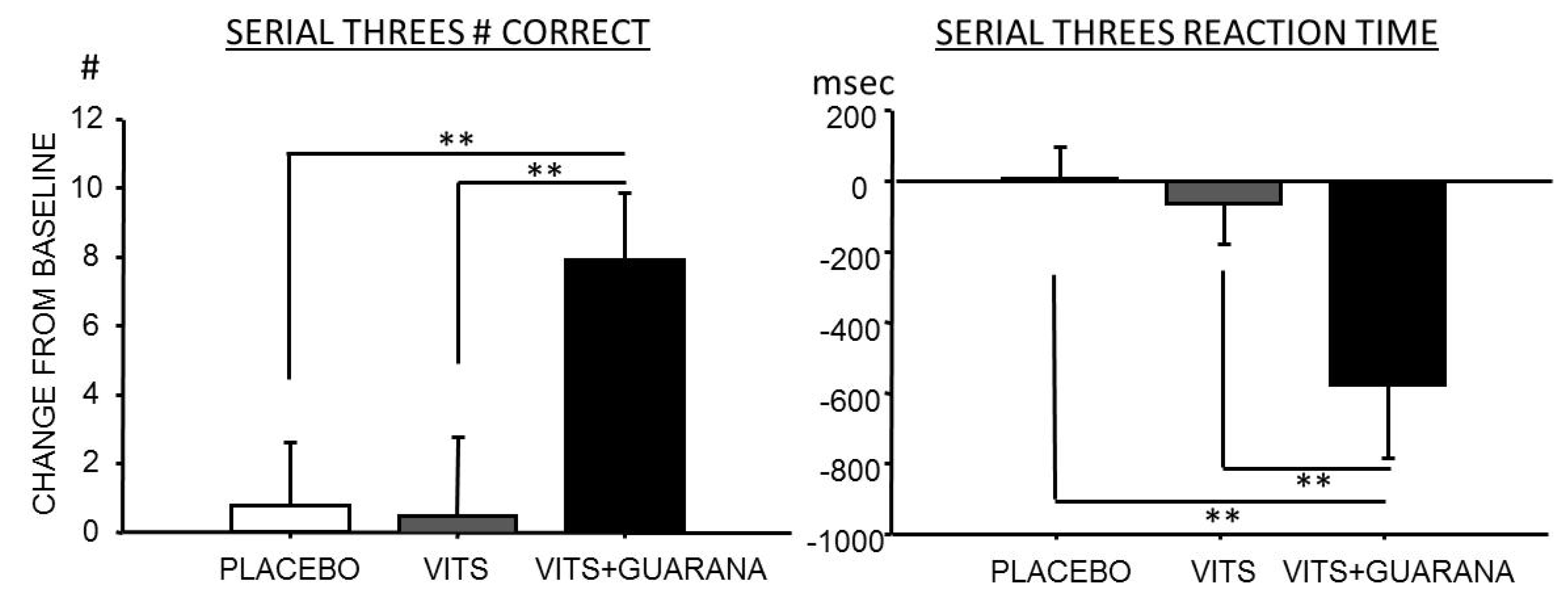
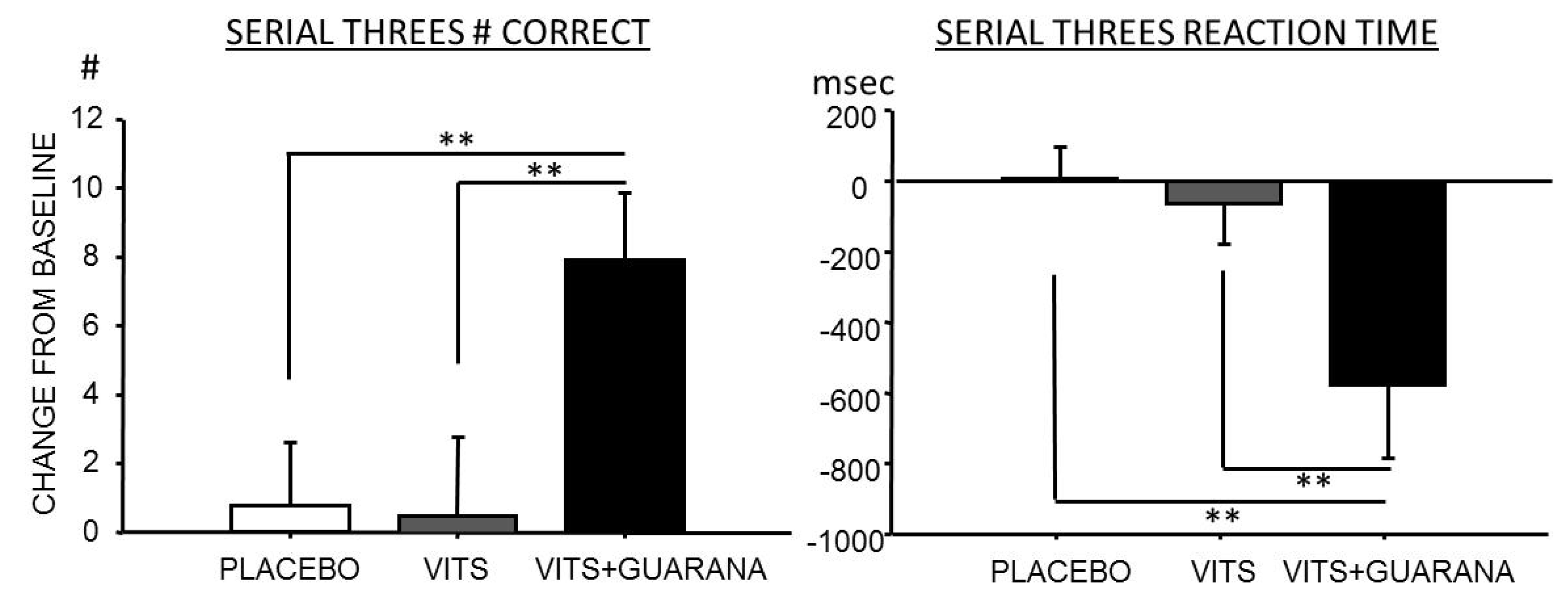
3.1. Mood and Cognitive Performance
| Baseline | Post-treatment | ||||
|---|---|---|---|---|---|
| Measure | Treatment | Pre | Post | Pre | Post |
| Bond-Lader Alert | Placebo | 66.96 (16.25) | 58.90 (18.03) | 67.00 (15.26) | 62.50 (18.06) |
| Berocca Performance | 66.77 (12.86) | 60.27 (15.46) | 66.43 (15.71) | 58.61 (16.56) | |
| Berocca Boost | 66.26 (15.09) | 58.94 (15.89) | 63.98 (13.35) | 60.76 (15.90) | |
| Bond-Lader Content | Placebo | 70.67 (11.87) | 64.93 (15.76) | 71.94 (10.98) | 68.70 (12.57) |
| Berocca Performance | 72.51 (9.23) | 69.15 (11.69) | 72.14 (10.77) | 67.28 (13.29) | |
| Berocca Boost | 72.54 (12.29) | 66.54 (11.50) | 69.46 (11.91) | 69.22 (12.32) | |
| Bond-Lader Calm | Placebo | 66.85 (14.24) | 65.50 (13.61) | 62.05 (14.23) | 65.50 (13.61) |
| Berocca Performance | 66.35 (14.40) | 64.70 (12.94) | 64.80 (15.60) | 63.45 (14.00) | |
| Berocca Boost | 65.95 (15.71) | 62.43 (10.10) | 62.48 (13.81) | 61.85 (13.26) | |
| VAS Stress | Placebo | 28.05 (19.85) | 32.70 (19.84) | 28.05 (19.85) | 32.70 (19.84) |
| Berocca Performance | 23.70 (15.38) | 32.35 (18.51) | 25.45 (16.47) | 30.90 (17.07) | |
| Berocca Boost | 27.20 (23.54) | 38.45 (21.25) | 28.15 (19.20) | 33.50 (19.91) | |
| VAS Fatigue | Placebo | 31.80 (18.95) | 37.35 (22.81) | 31.80 (18.95) | 32.70 (19.84) |
| Berocca Performance | 31.85 (16.85) | 42.00 (20.12) | 33.15 (16.62) | 43.40 (20.88) | |
| Berocca Boost | 37.15 (22.79) | 45.00 (21.03) | 36.15 (15.15) | 39.25 (20.93) | |
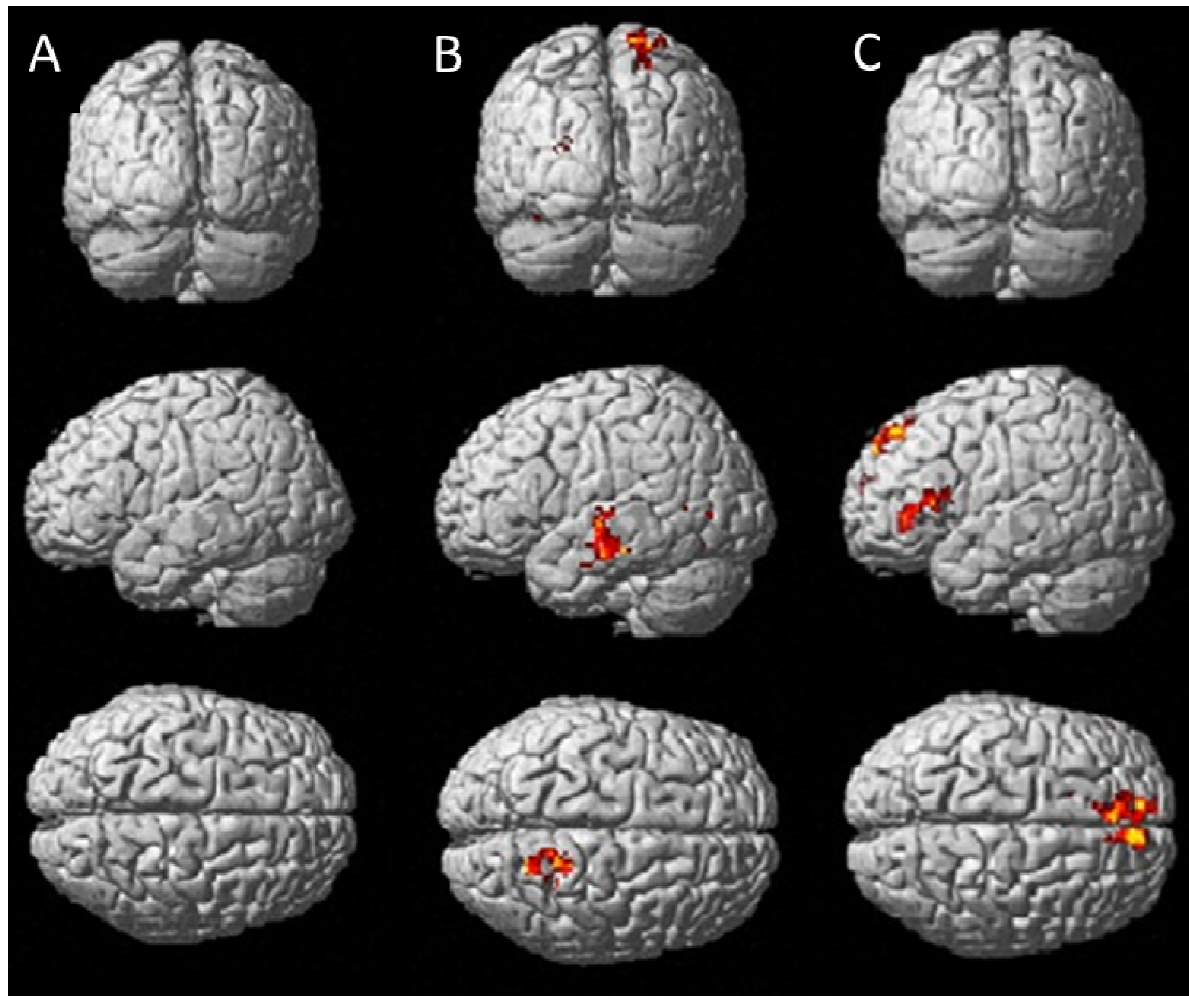
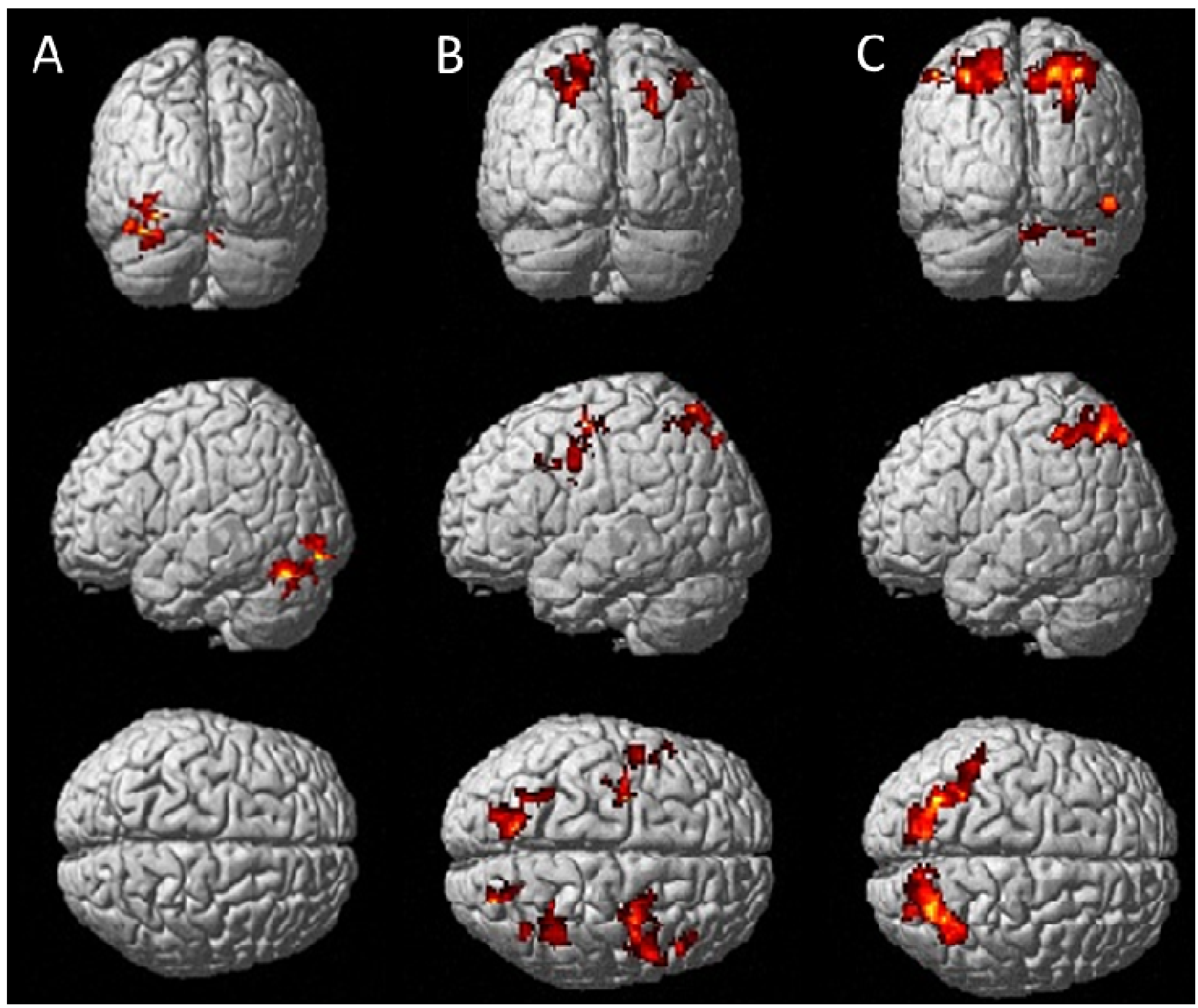
3.2. Brain Activation Associated with the fMRI Tasks
| Comparison | L/R | Region | Peak voxel T-value | Cluster | Coordinates (MNI) X, Y, Z |
|---|---|---|---|---|---|
| a) RVIP Task > control | L | Superior Parietal Lobule | 32.37 | 830 | −30, −66, 52 |
| L | Cerebellum | 20.59 | 847 | −28, −72, −26 | |
| R | Supplementary Motor Area | 22.40 | 196 | 4, 8, 54 | |
| R | Superior Parietal Lobule | 17.89 | 1032 | 30, −60, 54 | |
| L | Inferior Occipital Gyrus | 15.64 | 204 | −28, −88, −10 | |
| L | Inferior frontal gyrus | 13.81 | 206 | −42, 6, 28 | |
| L | Hippocampus | 13.33 | 229 | −18, −36, 12 | |
| L | Precentral gyrus | 12.86 | 208 | −38, −10, 66 | |
| R | Middle frontal gyrus | 7.74 | 150 | 42, 40, 32 | |
| b) IT Correct > incorrect | R | Caudate nucleus | 20.90 | 4253 | 14, 12, 10 |
| R | Cerebellum | 9.32 | 225 | 38, −66, −34 | |
| R | Cerebellum | 9.11 | 605 | 8, −54, −42 | |
| L | Middle temporal gyrus | 9.27 | 258 | −60, −8, −6 |
3.3. Brain Activation Associated with Treatments
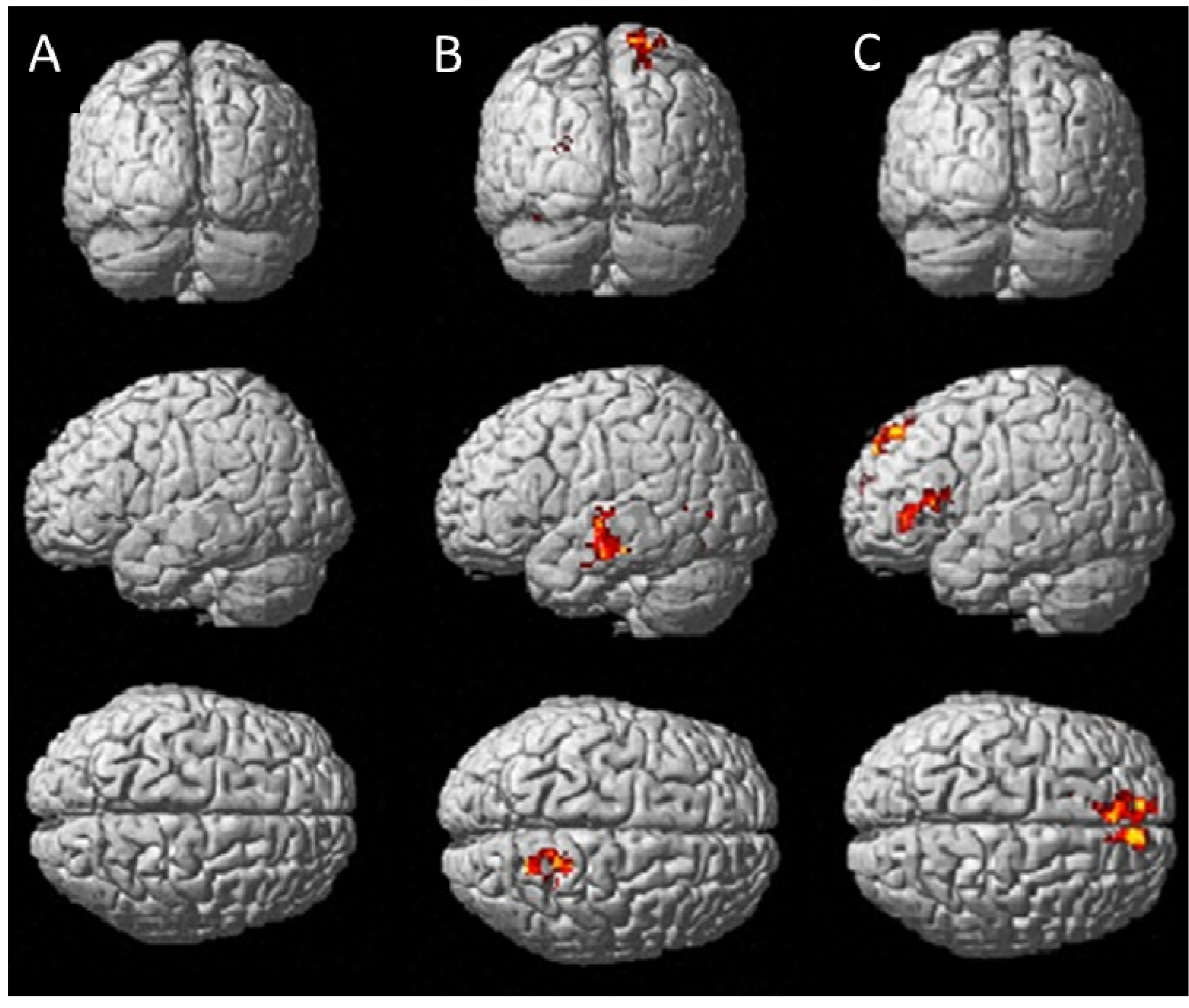
3.4. Brain Activation Associated with Treatments
4. Discussion
5. Conclusions
Acknowledgments
Conflicts of Interest
References
- Black, M.M. Micronutrient deficiencies and cognitive functioning. J. Nutr. 2003, 133, 3927S–3931S. [Google Scholar]
- Bryan, J.; Osendarp, S.; Hughes, D.; Calvaresi, E.; Baghurst, K.; van Klinken, J.W. Nutrients for cognitive development in school-aged children. Nutr. Rev. 2004, 62, 295–306. [Google Scholar] [CrossRef]
- Heseker, H.; Kubler, W.; Pudel, V.; Westenhofer, J. Interaction of vitamins with mental performance. Bibl. Nutr. Dieta 1995, 52, 43–55. [Google Scholar]
- Malouf, M.; Grimley, E.J.; Areosa, S.A. Folic acid with or without vitamin B12 for cognition and dementia. Cochrane Database Syst. Rev. 2003, 4, CD004514. [Google Scholar]
- Malouf, R.; Areosa Sastre, A. Vitamin B12 for cognition. Cochrane Database Syst. Rev. 2003, 3, CD004326. [Google Scholar]
- Rosenberg, I.H.; Miller, J.W. Nutritional factors in physical and cognitive functions of elderly people. Am. J. Clin. Nutr. 1992, 55, 1237S–1243S. [Google Scholar]
- Zimmermann, M.B.; Connolly, K.; Bozo, M.; Bridson, J.; Rohner, F.; Grimci, L. Iodine supplementation improves cognition in iodine-deficient schoolchildren in Albania: A randomized, controlled, double-blind study. Am. J. Clin. Nutr. 2006, 83, 108–114. [Google Scholar]
- Rosenthal, M.J.; Goodwin, J.S. Cognitive effects of nutritional deficiency. Adv. Nutr. Res. 1985, 7, 71–100. [Google Scholar] [CrossRef]
- Bryan, J.; Calvaresi, E.; Hughes, D. Short-Term Folate, Vitamin B-12 or Vitamin B-6 supplementation slightly affects memory performance but not mood in women of various ages. J. Nutr. 2002, 132, 1345–1356. [Google Scholar]
- Institute of Medicine (IOM), Reference Intakes for Thiamin, Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pantothenic Acid, Biotin, and Choline; National Academy Press: Washington, DC, USA, 1998.
- Institute of Medicine (IOM), Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium and Carotenoid; National Academy Press: Washington, DC, USA, 2000.
- Grima, N.A.; Pase, M.P.; Macpherson, H.; Pipingas, A. The effects of multivitamins on cognitive performance: A systematic review and meta-analysis. J. Alzheimer’s Dis. 2012, 29, 561–569. [Google Scholar]
- Kennedy, D.O.; Haskell, C.F. Vitamins and cognition: What is the evidence? Drugs 2011, 71, 1957–1971. [Google Scholar] [CrossRef]
- Kennedy, D.O.; Veasey, R.; Watson, A.; Dodd, F.; Jones, E.; Maggini, S.; Haskell, C.F. Effects of high-dose B vitamin complex with vitamin C and minerals on subjective mood and performance in healthy males. Psychopharmacology 2010, 211, 55–68. [Google Scholar] [CrossRef]
- Kennedy, D.O.; Veasey, R.C.; Watson, A.W.; Dodd, F.L.; Jones, E.K.; Tiplady, B.; Haskell, C.F. Vitamins and psychological functioning: A mobile phone assessment of the effects of a B vitamin complex, vitamin C and minerals on cognitive performance and subjective mood and energy. Hum. Psychopharmacol. Clin. Exp. 2011, 26, 538–547. [Google Scholar]
- Harris, E.; Kirk, J.; Rowsell, R.; Vitetta, L.; Sali, A.; Scholey, A.B.; Pipingas, A. The effect of multivitamin supplementation on mood and stress in healthy older men. Hum. Psychopharmacol. Clin. Exp. 2011, 26, 560–567. [Google Scholar] [CrossRef]
- Stough, C.; Scholey, A.; Lloyd, J.; Spong, J.; Myers, S.; Downey, L.A. The effect of 90 day administration of a high dose vitamin B—Complex on work stress. Hum. Psychopharmacol. Clin. Exp. 2011, 26, 470–476. [Google Scholar] [CrossRef]
- Haskell, C.F.; Robertson, B.; Jones, E.; Forster, J.; Jones, R.; Wilde, A.; Maggini, S.; Kennedy, D.O. Effects of a multi—Vitamin/mineral supplement on cognitive function and fatigue during extended multi—Tasking. Hum. Psychopharmacol. Clin. 2010, 25, 448–461. [Google Scholar] [CrossRef]
- Haskell, C.F.; Scholey, A.B.; Jackson, P.A.; Elliott, J.M.; Defeyter, M.A.; Greer, J.; Robertson, B.C.; Buchanan, T.; Tiplady, B.; Kennedy, D.O. Cognitive and mood effects in healthy children during 12 weeks’ supplementation with multi-vitamin/minerals. Br. J. Nutr. 2010, 100, 1086–1096. [Google Scholar]
- Kennedy, D.O.; Haskell, C.F.; Robertson, B.; Reay, J.; Brewster-Maund, C.; Luedemann, J.; Maggini, S.; Ruf, M.; Zangara, A.; Scholey, A.B. Improved cognitive performance and mental fatigue following a multi-vitamin and mineral supplement with added guarana (Paullinia cupana). Appetite 2008, 50, 506–513. [Google Scholar] [CrossRef]
- Scholey, A.; Haskell, C. Neurocognitive effects of guarana plant extract. Drugs Future 2010, 33, 869. [Google Scholar] [CrossRef]
- Haskell, C.F.; Kennedy, D.O.; Wesnes, K.A.; Milne, A.L.; Scholey, A.B. A double-blind, placebo-controlled, multi-dose evaluation of the acute behavioural effects of guarana in humans. J. Psychopharmacol. 2007, 21, 65–70. [Google Scholar]
- Huskisson, E.; Maggini, S.; Ruf, M. The influence of micronutrients on cognitive function and performance. J. Int. Med. Res. 2007, 35, 1–19. [Google Scholar] [CrossRef]
- Mattson, M.P.; Shea, T.B. Folate and homocysteine metabolism in neural plasticity and neurodegenerative disorders. Trends Neurosci. 2003, 26, 137–146. [Google Scholar] [CrossRef]
- Logothetis, N.K. What we can do and what we cannot do with fMRI. Nature 2008, 453, 869–878. [Google Scholar] [CrossRef]
- Deary, I.J.; Simonotto, E.; Meyer, M.; Marshall, A.; Marshall, I.; Goddard, N.; Wardlaw, J.M. The functional anatomy of inspection time: An event-related fMRI study. NeuroImage 2004, 22, 1466–1479. [Google Scholar] [CrossRef]
- Lawrence, N.S.; Ross, T.J.; Hoffmann, R.; Garavan, H.; Stein, E.A. Multiple neuronal networks mediate sustained attention. J. Cogn. Neurosci. 2003, 15, 1028–1038. [Google Scholar] [CrossRef]
- Scholey, A.B.; Harper, S.; Kennedy, D.O. Cognitive demand and blood glucose. Physiol. Behav. 2001, 73, 585–592. [Google Scholar] [CrossRef]
- Reay, J.L.; Kennedy, D.O.; Scholey, A.B. Effects of Panax ginseng, consumed with and without glucose, on blood glucose levels and cognitive performance during sustained ‘mentally demanding’ tasks. J. Psychopharmacol. 2006, 20, 771–781. [Google Scholar] [CrossRef]
- Kennedy, D.O.; Scholey, A.B. A glucose-caffeine ‘energy drink’ ameliorates subjective and performance deficits during prolonged cognitive demand. Appetite 2004, 42, 331–333. [Google Scholar] [CrossRef]
- Reay, J.L.; Kennedy, D.O.; Scholey, A.B. Single doses of Panax ginseng (G115) reduce blood glucose levels and improve cognitive performance during sustained mental activity. J. Psychopharmacol. 2005, 19, 357–365. [Google Scholar] [CrossRef]
- Scholey, A.B.; French, S.J.; Morris, P.J.; Kennedy, D.O.; Milne, A.L.; Haskell, C.F. Consumption of cocoa flavanols results in acute improvements in mood and cognitive performance during sustained mental effort. J. Psychopharmacol. 2010, 24, 1505–1514. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gorsuch, R.L.; Lushene, R.; Vagg, P.R.; Jacobs, G.A. Manual for the State-Trait Anxiety Inventory; Consulting Psychologists Press: Palo Alto, CA, USA, 1983. [Google Scholar]
- Bond, A.; Lader, M. The use of analogue scales in rating subjective feelings. Br. J. Med. Psychol. 1974, 47, 211–218. [Google Scholar] [CrossRef]
- Mazaika, P.; Whitfield-Gabrieli, S.; Reiss, A.; Glover, G. Artifact Repair for fMRI Data from High Motion Clinical Subjects. In Proceeding of the 13th Annual Meeting of the Organization for Human Brain Mapping, Chicago, IL, USA, June 2007.
- Brett, M.; Anton, J.-L.; Valabregue, R.; Poline, J.-B. Region of interest analysis using the MarsBar toolbox for SPM 99. Neuroimage 2002, 16, S497. [Google Scholar]
- Scholey, A.B.; Kennedy, D.O. Cognitive and physiological effects of an “energy drink”: An evaluation of the whole drink and of glucose, caffeine and herbal flavouring fractions. Psychopharmacology 2004, 176, 320–330. [Google Scholar] [CrossRef]
- Garavan, H.; Ross, T.; Murphy, K.; Roche, R.; Stein, E. Dissociable executive functions in the dynamic control of behavior: Inhibition, error detection, and correction. Neuroimage 2002, 17, 1820–1829. [Google Scholar] [CrossRef]
- Strick, P.L.; Dum, R.P.; Fiez, J.A. Cerebellum and nonmotor function. Ann. Rev. Neurosci. 2009, 32, 413–434. [Google Scholar] [CrossRef]
- Stoodley, C.J.; Schmahmann, J.D. Functional topography in the human cerebellum: A meta-analysis of neuroimaging studies. Neuroimage 2009, 44, 489–501. [Google Scholar] [CrossRef]
- Koelsch, S.; Schulze, K.; Sammler, D.; Fritz, T.; Müller, K.; Gruber, O. Functional architecture of verbal and tonal working memory: An FMRI study. Hum. Brain Mapp. 2009, 30, 859–873. [Google Scholar] [CrossRef]
- Todd, J.J.; Han, S.W.; Harrison, S.; Marois, R. The neural correlates of visual working memory encoding: A time-resolved fMRI study. Neuropsychologia 2011, 49, 1527–1536. [Google Scholar] [CrossRef]
- Kanai, R.; Rees, G. The structural basis of inter-individual differences in human behaviour and cognition. Nat. Rev. Neurosci. 2011, 12, 231–242. [Google Scholar] [CrossRef]
- Hampshire, A.; Chamberlain, S.R.; Monti, M.M.; Duncan, J.; Owen, A.M. The role of the right inferior frontal gyrus: Inhibition and attentional control. Neuroimage 2010, 50, 1313–1319. [Google Scholar] [CrossRef]
- Yee, L.T.; Roe, K.; Courtney, S.M. Selective involvement of superior frontal cortex during working memory for shapes. J. Neurophysiol. 2010, 103, 557–563. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Scholey, A.; Bauer, I.; Neale, C.; Savage, K.; Camfield, D.; White, D.; Maggini, S.; Pipingas, A.; Stough, C.; Hughes, M. Acute Effects of Different Multivitamin Mineral Preparations with and without Guaraná on Mood, Cognitive Performance and Functional Brain Activation. Nutrients 2013, 5, 3589-3604. https://doi.org/10.3390/nu5093589
Scholey A, Bauer I, Neale C, Savage K, Camfield D, White D, Maggini S, Pipingas A, Stough C, Hughes M. Acute Effects of Different Multivitamin Mineral Preparations with and without Guaraná on Mood, Cognitive Performance and Functional Brain Activation. Nutrients. 2013; 5(9):3589-3604. https://doi.org/10.3390/nu5093589
Chicago/Turabian StyleScholey, Andrew, Isabelle Bauer, Chris Neale, Karen Savage, David Camfield, David White, Silvia Maggini, Andrew Pipingas, Con Stough, and Matthew Hughes. 2013. "Acute Effects of Different Multivitamin Mineral Preparations with and without Guaraná on Mood, Cognitive Performance and Functional Brain Activation" Nutrients 5, no. 9: 3589-3604. https://doi.org/10.3390/nu5093589
APA StyleScholey, A., Bauer, I., Neale, C., Savage, K., Camfield, D., White, D., Maggini, S., Pipingas, A., Stough, C., & Hughes, M. (2013). Acute Effects of Different Multivitamin Mineral Preparations with and without Guaraná on Mood, Cognitive Performance and Functional Brain Activation. Nutrients, 5(9), 3589-3604. https://doi.org/10.3390/nu5093589