Zinc Intake and Its Dietary Sources: Results of the 2007 Australian National Children’s Nutrition and Physical Activity Survey


Abstract
:1. Introduction
2. Methods
2.1. 2007 Children’s Survey
2.2. 1995 National Nutrition Survey
2.3. Under- and Over-Reporters
2.4. Statistical Methods
3. Results
3.1. Zinc Intakes; 2007 Children’s Survey

{kind=link}
| Percentile | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| n | Supplements | Mean (SD) | 10 | 25 | 50 | 75 | 90 | ||
| Boys | |||||||||
| 2–3 years | 622 | Excluded | 8.6 (2.0) | 6.3 | 7.2 | 8.5 | 9.8 | 11.4 | |
| Included | 8.8 (2.2) | 6.4 | 7.3 | 8.6 | 10.0 | 11.7 | |||
| 4–8 years | 640 | Excluded | 9.9 (2.3) | 7.2 | 8.4 | 9.7 | 11.2 | 12.7 | |
| Included | 10.2 (2.6) | 7.3 | 8.5 | 9.9 | 11.4 | 13.2 | |||
| 9–13 years | 579 | Excluded | 11.2 (2.8) | 7.8 | 9.4 | 11.0 | 13.0 | 15.0 | |
| Included | 11.4 (3.0) | 7.9 | 9.5 | 11.1 | 13.2 | 15.2 | |||
| 14–16 years | 596 | Excluded | 13.3 (4.1) | 8.9 | 10.6 | 12.8 | 15.2 | 18.3 | |
| Included | 13.7 (4.3) | 9.0 | 10.9 | 13.1 | 15.6 | 18.8 | |||
| Girls | |||||||||
| 2–3 years | 569 | Excluded | 8.3 (2.1) | 5.8 | 6.9 | 8.1 | 9.4 | 10.9 | |
| Included | 8.6 (2.4) | 5.9 | 7.1 | 8.4 | 9.8 | 11.5 | |||
| 4–8 years | 623 | Excluded | 9.0 (2.1) | 6.7 | 7.5 | 8.8 | 10.1 | 11.9 | |
| Included | 9.2 (2.3) | 6.8 | 7.8 | 8.9 | 10.3 | 12.2 | |||
| 9–13 years | 640 | Excluded | 10.0 (2.8) | 6.9 | 8.2 | 9.6 | 11.4 | 13.7 | |
| Included | 10.2 (3.0) | 6.9 | 8.3 | 9.8 | 11.7 | 14.0 | |||
| 14–16 years | 565 | Excluded | 9.8 (2.7) | 6.4 | 7.9 | 9.7 | 11.3 | 13.1 | |
| Included | 10.3 (3.5) | 6.5 | 8.2 | 10.0 | 11.8 | 13.9 | |||
| Total | 4834 | Excluded | 10.2 (3.0) | 6.8 | 8.1 | 9.7 | 11.7 | 14.0 | |
| Included | 10.4 (3.3) | 6.9 | 8.3 | 9.9 | 12.0 | 14.4 | |||
| Supplements | EAR (mg) | % Meeting EAR | UL (mg) | % Exceeding UL | ||
|---|---|---|---|---|---|---|
| Boys | ||||||
| 2–3 years | Excluded | 2.5 | 100 | 7 | 79.1 | |
| Included | 100 | 81.0 | ||||
| 4–8 years | Excluded | 3.0 | 100 | 12 | 15.5 | |
| Included | 100 | 19.4 | ||||
| 9–13 years | Excluded | 5.0 | 99.2 | 25 | 0 | |
| Included | 99.2 | 0.1 | ||||
| 14–16 years | Excluded | 11.0 | 71.2 | 35 | 0 | |
| Included | 74.3 | 0 | ||||
| Girls | ||||||
| 2–3 years | Excluded | 2.5 | 100 | 7 | 74.1 | |
| Included | 100 | 75.8 | ||||
| 4–8 years | Excluded | 3.0 | 100 | 12 | 9.3 | |
| Included | 100 | 11.6 | ||||
| 9–13 years | Excluded | 5.0 | 98.8 | 25 | 0 | |
| Included | 98.9 | 0.2 | ||||
| 14–16 years | Excluded | 6.0 | 92.3 | 35 | 0 | |
| Included | 92.9 | 0 | ||||
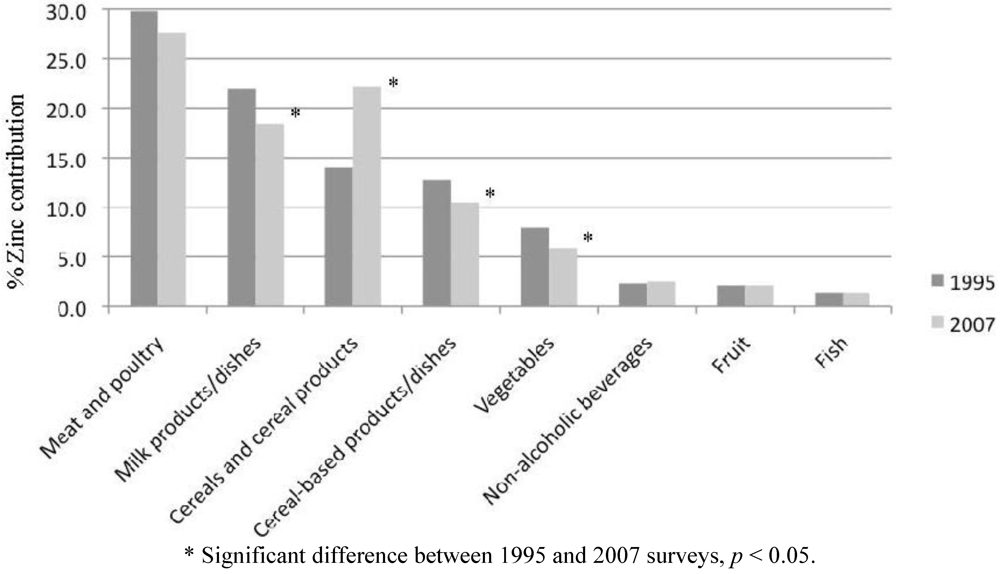
3.2. Contribution of Food Sources to Zinc Intake
| 2–3 years | 4–8 years | 9–13 years | 14–16 years Boys | 14–16 years Girls | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1995 | 2007 | 1995 | 2007 | 1995 | 2007 | 1995 | 2007 | 1995 | 2007 | ||
| n | 302 | 577 | 842 | 1506 | 832 | 1462 | 240 | 437 | 219 | 398 | |
| Meat, poultry and game products/dishes | 1.47 | 1.74 | 2.09 | 2.29 | 3.39 | 3.19 | 4.14 | 5.15 | 2.96 | 2.97 | |
| Beef, veal, lamb cuts | 0.26 | 0.86 | 0.44 | 1.08 | 1.05 | 1.47 | 1.56 | 2.50 | 0.94 | 1.43 | |
| Beef, veal, lamb mixed | 0.52 | 0.25 | 0.68 | 0.23 | 1.03 | 0.47 | 0.87 | 0.86 | 0.92 | 0.36 | |
| Pork cuts | 0.02 | 0.04 | 0.07 | 0.04 | 0.19 | 0.06 | 0.31 | 0.11 | 0.04 | 0.10 | |
| Pork mixed dishes | 0.00 | 0.01 | 0.04 | 0.01 | 0.02 | 0.01 | 0.08 | 0.01 | 0.06 | 0.03 | |
| Poultry cuts | 0.12 | 0.16 | 0.19 | 0.22 | 0.21 | 0.34 | 0.38 | 0.42 | 0.36 | 0.38 | |
| Poultry mixed dishes | 0.07 | 0.06 | 0.15 | 0.15 | 0.18 | 0.21 | 0.20 | 0.44 | 0.22 | 0.15 | |
| Sausages | 0.28 | 0.17 | 0.32 | 0.21 | 0.45 | 0.28 | 0.39 | 0.29 | 0.23 | 0.19 | |
| Ham, bacon | 0.09 | 0.14 | 0.12 | 0.23 | 0.14 | 0.23 | 0.26 | 0.35 | 0.10 | 0.23 | |
| Luncheon meat | 0.09 | 0.06 | 0.08 | 0.10 | 0.09 | 0.09 | 0.08 | 0.12 | 0.03 | 0.09 | |
| Offal | 0.00 | 0.00 | 0.00 | 0.00 | 0.01 | 0.02 | 0.00 | 0.00 | 0.06 | 0.00 | |
| Fish and seafood products/dishes | 0.06 | 0.08 | 0.15 | 0.18 | 0.13 | 0.14 | 0.13 | 0.13 | 0.15 | 0.12 | |
| Eggs products/dishes | 0.06 | 0.07 | 0.08 | 0.09 | 0.09 | 0.08 | 0.14 | 0.11 | 0.07 | 0.10 | |
| Seed and nut products/dishes | 0.06 | 0.05 | 0.09 | 0.05 | 0.07 | 0.12 | 0.06 | 0.09 | 0.07 | 0.10 | |
| Milk products/dishes | 2.26 | 2.06 | 1.86 | 1.78 | 2.03 | 1.88 | 2.46 | 2.41 | 1.73 | 1.77 | |
| Milk | 1.54 | 1.21 | 1.18 | 0.97 | 1.25 | 1.08 | 1.64 | 1.43 | 0.87 | 0.88 | |
| Cheese | 0.39 | 0.52 | 0.36 | 0.54 | 0.43 | 0.52 | 0.49 | 0.73 | 0.53 | 0.65 | |
| Yoghurt, custard | 0.21 | 0.29 | 0.16 | 0.20 | 0.11 | 0.14 | 0.08 | 0.16 | 0.15 | 0.16 | |
| Soy milk | 0.04 | 0.07 | 0.01 | 0.03 | 0.01 | 0.02 | 0.01 | 0.04 | 0.00 | 0.03 | |
| Cereals and cereal products | 0.93 | 1.81 | 1.13 | 2.10 | 1.43 | 2.49 | 1.73 | 3.39 | 1.26 | 1.92 | |
| Breads | 0.50 | 0.63 | 0.66 | 0.80 | 0.80 | 0.81 | 0.89 | 1.10 | 0.67 | 0.82 | |
| Breakfast cereals | 0.22 | 0.79 | 0.26 | 0.91 | 0.33 | 1.05 | 0.45 | 1.67 | 0.24 | 0.54 | |
| Pasta, noodle | 0.04 | 0.13 | 0.05 | 0.16 | 0.06 | 0.19 | 0.05 | 0.21 | 0.10 | 0.21 | |
| Rice | 0.08 | 0.09 | 0.12 | 0.10 | 0.16 | 0.17 | 0.25 | 0.22 | 0.20 | 0.17 | |
| Cereal-based products/dishes | 0.54 | 0.47 | 0.90 | 0.83 | 1.25 | 1.24 | 2.34 | 2.13 | 1.48 | 1.32 | |
| Meat pie, sausage rolls, etc. | 0.15 | 0.09 | 0.26 | 0.18 | 0.29 | 0.25 | 0.98 | 0.51 | 0.29 | 0.38 | |
| Takeaway burgers, pizza, pasta | 0.23 | 0.16 | 0.37 | 0.37 | 0.68 | 0.65 | 1.07 | 1.27 | 0.90 | 0.60 | |
| Fruit products/dishes | 0.22 | 0.26 | 0.23 | 0.23 | 0.20 | 0.20 | 0.15 | 0.18 | 0.16 | 0.18 | |
| Vegetable products/dishes | 0.42 | 0.40 | 0.54 | 0.47 | 0.88 | 0.68 | 1.11 | 0.94 | 0.88 | 0.83 | |
| Non-alcoholic beverages | 0.17 | 0.14 | 0.19 | 0.21 | 0.23 | 0.29 | 0.24 | 0.34 | 0.23 | 0.36 | |
| TOTAL | 6.56 | 7.71 | 7.71 | 8.98 | 10.24 | 11.16 | 13.38 | 15.87 | 9.51 | 10.61 | |

4. Discussion
5. Conclusions
Acknowledgements
References
- Gibson, R.; Heath, A.-L. Population groups at risk of zinc deficiency in Australia and New Zealand: A review. Nutr. Diet. 2011, 68, 97–108. [Google Scholar] [CrossRef]
- Prasad, A.S. Discovery and importance of zinc in human nutrition. Fed. Proc. 1984, 43, 2829–2834. [Google Scholar]
- Samman, S. Zinc. Nutr. Diet. 2007, 64, S131–S134. [Google Scholar] [CrossRef]
- King, J.C.; Cousins, R.J. Zinc. In Modern Nutrition in Health and Disease, 10th; Shils, M.E., Shike, M., Ross, A.C., Caballero, B., Cousins, R.J., Eds.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2006; pp. 271–285. [Google Scholar]
- Gibson, R.S.; Vanderkooy, P.D.; MacDonald, A.C.; Goldman, A.; Ryan, B.A.; Berry, M. A growth-limiting, mild zinc-deficiency syndrome in some southern Ontario boys with low height percentiles. Am. J. Clin. Nutr. 1989, 49, 1266–1273. [Google Scholar]
- McLennan, W.; Podger, A. National Nutrition Survey 1995: Nutrient Intakes and Physical Measurements; ABS Catalogue No. 4805.0; Australian Bureau of Statistics: Canberra, Australia, 1998. [Google Scholar]
- National Health and Medical Research Council, Nutrient Reference Values for Australia and New Zealand; Commonwealth of Australia: Canberra, Australia, 2006.
- Magarey, A.; Bannerman, E. Evaluation of micronutrient intakes of children and adolescents: National Nutrition Survey 1995 and comparison with 1985 data. Nutr. Diet. 2003, 60, 16–22. [Google Scholar]
- Department of Health and Ageing. 2007 Australian National Children’s Nutrition and Physical Activity Survey—Main Findings; Commonwealth of Australia: Canberra, Australia, 2008. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/phd-nutrition-childrens-survey (accessed on 14 April 2012).
- Australian Social Science Data Archive. The 2007 National Children’s Nutrition and Physical Activity Survey; The Australian National University: Canberra, Australia, 2009. Available online: http://www.assda.edu.au/ (accessed on 12 August 2009).
- Department of Health and Ageing. 2007 Australian National Children’s Nutrition and Physical Activity Survey—User Guide; Commonwealth of Australia: Canberra, Australia, 2007. Available online: http://www.health.gov.au/internet/main/publishing.nsf/Content/phd-nutrition-childrens-survey-userguide (accessed on 12 April 2012).
- Food Standards Australia New Zealand. AUSNUT 2007; FSANZ: Canberra, Australia, 2007. Available online: http://www.foodstandards.gov.au/monitoringandsurveillance/foodcompositionprogram/ausnut2007/ (accessed on 12 April 2012).
- McLennan, W.; Podger, A. National Nutrition Survey User’s Guide 1995; AGPS: Canberra, Australia, 1998. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:Basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef]
- Harttig, U.; Haubrock, J.; Knuppel, S.; Boeing, H. EFCOVAL Consortium. The MSM program: Web-Based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur. J. Clin. Nutr. 2011, 65, S87–S91. [Google Scholar] [CrossRef]
- Souverein, O.W.; Dekkers, A.L.; Geelen, A.; Haubrock, J.; de Vries, J.H.; Ocké, M.C.; Harttig, U.; Boeing, H.; van’t Veer, P. EFCOVAL Consortium. Comparing four methods to estimate usual intake distributions. Eur. J. Clin. Nutr. 2011, 65, S92–S101. [Google Scholar] [CrossRef]
- Food and Nutrition Board, Institute of Medicine. Dietary Reference Intakes; National Academy Press: Washington, DC, USA, 2001.
- De Benoist, B.; Darnton-Hill, I.; Davidsson, L.; Fontaine, O.; Hotz, C. Conclusions of the joint WHO/UNICEF/IAEA/IZiNCG Interagency meeting on zinc status indicators. Food Nutr. Bull. 2007, 28, 5480–5484. [Google Scholar]
- Health Canada. Do Canadian Adolescents Meet Their Nutrient Requirements through Food Intake Alone? Available online: http://www.hc-sc.gc.ca/fn-an/surveill/nutrition/commun/art-nutr-adol-eng.php#a331 (accessed on 29 April 2012).
- Magarey, A.; Boulton, J. The Adelaide Nutrition Study. 2. Macronutrient and micronutrient intakes at ages 11, 13 and 15 years: Age and sex differences. Aust. J. Nutr. Diet. 1994, 51, 111–119. [Google Scholar]
- Landers, M.C.G.; Warden, R.A.; Hunt, K.A.; Boulton, T.J.C. Nutrition in long day child care centres: Are the guidelines realistic? Aust. J. Nutr. Diet. 1994, 51, 186–190. [Google Scholar]
- Karr, M.; Mira, M.; Causer, J.; Earl, J.; Alperstein, G.; Wood, F.; Fett, M.J.; Coakley, J. Plasma and serum micronutrient concentrations in preschool children. Acta Paediatr. 1997, 86, 677–682. [Google Scholar] [CrossRef]
- Gibson, R.S.; Bailey, K.B.; Parnell, W.R.; Wilson, N.; Ferguson, E.L. Higher risk of zinc deficiency in New Zealand Pacific school children compared with their MÄori and European counterparts: A New Zealand national survey. Br. J. Nutr. 2011, 105, 436–446. [Google Scholar] [CrossRef]
- Briefel, R.R.; Bialostosky, K.; Kennedy-Stephenson, J.; McDowell, M.A.; Ervin, R.B.; Wright, J.D. Zinc intake of the U.S. population: Findings from the third National Health and Nutrition Examination Survey, 1988-1994. J. Nutr. 2000, 130, S1367–S1373. [Google Scholar]
- Samman, S.; Roberts, D.C. The effect of zinc supplements on plasma zinc and copper levels and the reported symptoms in healthy volunteers. Med. J. Aust. 1987, 146, 246–249. [Google Scholar]
- Foster, M.; Petocz, P.; Samman, S. Effects of zinc on plasma lipoprotein cholesterol concentrations in humans: A meta-analysis of randomised controlled trials. Atherosclerosis 2010, 210, 344–352. [Google Scholar] [CrossRef]
- Abdallah, S.M.; Samman, S. The effect of increasing dietary zinc on the activity of superoxide dismutase and zinc concentration in erythrocytes of healthy female subjects. Eur. J. Clin. Nutr. 1993, 47, 327–332. [Google Scholar]
- Walravens, P.A.; Hambidge, K.M. Growth of infants fed a zinc supplemented formula. Am. J. Clin. Nutr. 1976, 29, 1114–1121. [Google Scholar]
- Arsenault, J.E.; Brown, K.H. Zinc intake of US preschool children exceeds new dietary reference intakes. Am. J. Clin. Nutr. 2003, 78, 1011–1017. [Google Scholar]
- Ruz, M.; Castillo-Duran, C.; Lara, X.; Codoceo, J.; Rebolledo, A.; Atalah, E. A 14-mo zinc-supplementation trial in apparently healthy Chilean preschool children. Am. J. Clin. Nutr. 1997, 66, 1406–1413. [Google Scholar]
- Hotz, C.; Wuehler, S. Review of New Information on the Safe Upper Level for Zinc; International Zinc Nutrition Consultative Group. Available online: http://www.izincg.org/Hotz_IIWCPHN.pdf (accessed on 29 April 2012).
- Sandström, B. Bioavailability of zinc. Eur. J. Clin. Nutr. 1997, 51, S17–S19. [Google Scholar]
- World Health Organization, Trace Elements in Human Nutrition and Health; World Health Organization: Geneva, Switzerland, 1996.
- Foster, M.; Karra, M.; Picone, T.; Chu, A.; Hancock, D.; Petocz, P.; Samman, S. Dietary fibre intake increases the risk of zinc deficiency in healthy and diabetic women. Biol. Trace Elem. Res. 2012. [Google Scholar] [CrossRef]
- Sandström, B.; Sandberg, A.-S. Inhibitory effects of isolated inositol phosphates on zinc absorption in humans. J. Trace Elem. Electrol. Health Dis. 1992, 6, 99–103. [Google Scholar]
- Dwyer, J.; Picciano, M.F.; Raiten, D.J. Members of the Steering Committee. Collection of food and dietary supplement intake data: What We Eat in America—NHANES. J. Nutr. 2003, 133, S590–S600. [Google Scholar]
- Rutishauser, I.H.E. Getting it Right: How to Use the Data from the 1995 National Nutrition Survey; Commonwealth Department of Health and Aged Care: Canberra, Australia, 2000. [Google Scholar]
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Rangan, A.M.; Samman, S. Zinc Intake and Its Dietary Sources: Results of the 2007 Australian National Children’s Nutrition and Physical Activity Survey. Nutrients 2012, 4, 611-624. https://doi.org/10.3390/nu4070611
Rangan AM, Samman S. Zinc Intake and Its Dietary Sources: Results of the 2007 Australian National Children’s Nutrition and Physical Activity Survey. Nutrients. 2012; 4(7):611-624. https://doi.org/10.3390/nu4070611
Chicago/Turabian StyleRangan, Anna M., and Samir Samman. 2012. "Zinc Intake and Its Dietary Sources: Results of the 2007 Australian National Children’s Nutrition and Physical Activity Survey" Nutrients 4, no. 7: 611-624. https://doi.org/10.3390/nu4070611
APA StyleRangan, A. M., & Samman, S. (2012). Zinc Intake and Its Dietary Sources: Results of the 2007 Australian National Children’s Nutrition and Physical Activity Survey. Nutrients, 4(7), 611-624. https://doi.org/10.3390/nu4070611