1. Introduction
Female participation in sports dramatically increased following the passage of the Education Amendment of 1972, also known as “Title IX,” and its reinforcement in the 1988 Civil Rights Restoration Act [
1]. Since Title IX, the number of female athletes has risen from nearly 32,000 in 1971 to more than 150,000 in 2000 [
2]. This rise in female athletes has contributed to an extreme amount of support for volleyball, and it is evidenced by the 603 NCAA Division I, II, and III women’s volleyball teams in 1981 that nearly doubled to 1015 teams in 2008 [
1]. As a result of this increase in support, a considerable amount of research has been attributed to understanding the female physiology and major nutritional concerns of female athletes.
Currently, a vast amount of research is available on nutrient intake among female athletes [
3,
4,
5,
6,
7,
8,
9]. However, there is little research addressing sport-specific nutritional needs, especially those of volleyball players. Volleyball is a high intensity game requiring speed and large muscle groups for actions such as jumping, spiking, blocking, and retrieving the ball. Moreover, if a player were to spend an equal amount of time between the front and back courts, these high intensity actions can occur in shorts bouts every 30 s of play over a total period of 30 min to 180 min [
10]. Consequently, during the off season female volleyball players have been reported to have total energy expenditures as high as 2815 ± 306 [
11]. It is essential for an athlete expending energy at these high levels to consume adequate calories, yet a number of studies indicate that female athletes fail to meet these energy demands while training and competing [
5,
7,
8,
11,
12,
13]. According to the American College of Sports Medicine, adequate calorie intake is needed to maintain lean tissue mass, immune and reproductive function, and optimal athletic performance [
3]. When calorie intake is inadequate, the body will use fat and lean tissue mass as fuel, and as a result, muscle mass will be lost and strength and endurance will be compromised [
3].
Achieving energy balance is a critical component to meeting adequate energy requirements. Energy balance occurs when energy intake equals energy expended. Energy expenditure is influenced by a number of factors including the type of exercise, duration and intensity of exercise, age, gender, body size, fat-free mass (FFM), and nutritional status prior to exercise [
14]. The Recommended Dietary Allowance (RDA) for normally active people states that individuals should consume energy at a rate of 37 to 41 kcal/kg of body weight [
3]. For female athletes who engage primarily in resistance training, the energy requirements may be as high as 39 to 44 kcal/kg of body weight to support high levels of fat free mass and thus to maintain body weight [
15].
In addition to meeting energy requirements, macronutrients must be consumed in adequate amounts to sufficiently replenish glycogen stores. An important factor impacting muscle glycogen storage is carbohydrate consumption [
16]. Many female athletes restrict their carbohydrate intake and, as a result, do not meet the RDA to maintain muscle glycogen stores [
6,
17]. Athletes are generally recommended to consume 60% of energy from carbohydrates assuming that energy intake is adequate to meet needs. Moreover, a range of 6 to 10 g of carbohydrates per kilogram of body weight per day is recommended to meet optimal muscle glycogen storage [
14].
All of the foregoing research explains why adequate energy intake is necessary to achieve optimal performance. However, despite this readily available research, it is a well known fact that low energy availability is a prevailing issue among female athletes across many sports. In addition, female athletes have demonstrated a limited working knowledge of sports nutrition [
18,
19]. Many researchers have suggested that athletes as well as coaches will benefit from nutrition education and counseling regarding performance and prevention of health concerns [
4,
6,
8,
18,
19,
20]. Therefore, to gain a better understanding of the foregoing issues, a preliminary investigation of a 2009 NCAA Division I women’s volleyball team was conducted. The study was performed during the 2009 off-season, and throughout the study, no nutritional intervention was employed. This investigation revealed participants’ diets were inadequate to meet their daily caloric needs [
21]. Thus, the purpose of this paper is to conduct an evaluation of dietary intake, nutrition knowledge, and whether education improves dietary intake of collegiate female volleyball players.
3. Results
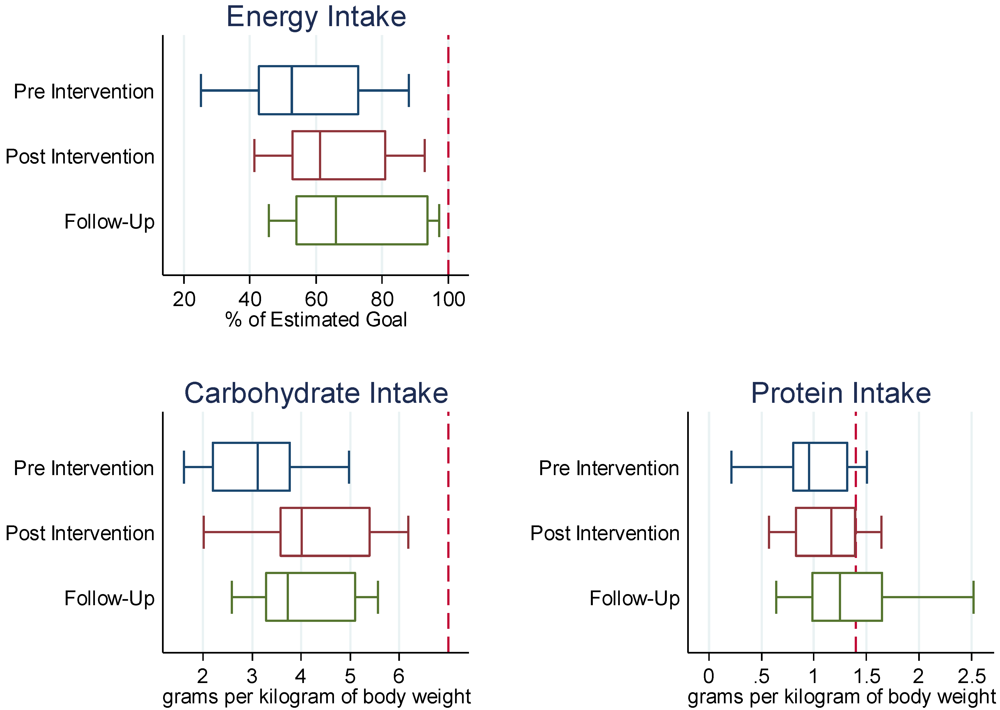
Dietary collection from the non-intervention season and the intervention season revealed that participants did not meet the recommended energy requirement of 37–41 kcal/kg of body weight. For the intervention season, the average percent of energy intake for the team at the beginning of the season was 56% of estimated needs with a range of 25% to 88%. The average percent of energy intake for the team at the end of the intervention season was 70% of estimated needs with a range of 44% to 95%, representing a significant improvement (
p = 0.002) (
Table 2).
Table 2.
Female volleyball players (n=11) intervention season beginning and end mean intakes of total energy and macronutrients.
Table 2.
Female volleyball players (n=11) intervention season beginning and end mean intakes of total energy and macronutrients.
| | Intervention | Recommendation | p value |
|---|
| Beginning | End |
|---|
| Energy Expenditure (kcal) | 3162 ± 421.3 | 3162 ± 421.3 | | |
| | | | | |
| Energy Intake (kcal) | 1756.0 ± 557.5 | 2178.4 ± 491.8 * | | |
| kcal/kg | 24.0 ± 8.6 | 29.4 ± 7.5 | (37–41 kcal/kg) | 0.002 |
| % total kcal needs | 56.3 ± 18.5 | 70.0 ± 17.7 | | |
| | | | | |
| Carbohydrate Total (g) | 224.3 ± 64.4 | 304.0 ± 79.9 * | | |
| | g/kg | 3.08 ± 1.1 | 4.15 ± 1.3 | (6–10 g/kg) | 0.01 |
| | % total kcal | 52.3 ± 8.9 | 56.0 ± 9.2 | | |
| | % total kcal needs | 48.2 ± 16.2 | 66.0 ± 21.7 | (474.4 ± 63.2 g/day) | |
| | | | | |
| Protein Total (g) | 69.3 ± 26.8 | 84.0 ± 20.5 * | | |
| | g/kg | 0.9 ± 0.3 | 1.14 ± 0.3 | (1.2–1.7 g/kg) | 0.01 |
| | % total kcal | 15.5 ± 3.4 | 15.6 ± 2.9 | | |
| | % total kcal needs | 59.0 ± 22.2 | 72 ± 19.8 | (118.5 ± 15.8 g/day) | |
| | | | | |
| Fat Total (g) | 67.4 ± 27.8 | 69.0 ± 24.8 | | |
| | % total kcal | 33.7 ± 6.4 | 27.9 ± 5.2 | | |
| | % total kcal needs | 77.0 ± 30.5 | 79.0 ± 26.6 | (87.7 ± 11.7 g/day) | 0.63 |
Based on the dietary collection for the non-intervention and intervention seasons, the team’s average percent of carbohydrate intake did not meet the recommended intake of 6 to 10 g of carbohydrate per kilogram of body weight [
14]. It is generally recommended to eat a diet high in carbohydrates at 60% of total energy intake; however, adequate energy intake must be consumed for this recommendation to be appropriate. At the beginning of the intervention season, the team’s average percent of carbohydrate intake was 48% of estimated needs with a range of 29% to 76%. At the end of the intervention season, the team’s average percent of carbohydrate intake was 66% of estimated needs with a range of 33% to 101% representing a statistically significant increase (
p = 0.01).
The team’s average percent of protein intake at the beginning of the intervention season was 59% of estimated needs with a range of 16% to 88%. At the end of the intervention season, the average percent of protein intake increased significantly (
p = 0.01) to 72% of estimated needs with a range of 37% to 102%. At the beginning of the intervention season, the teams’ average percent of fat intake was at 77% of estimated needs with a range of 23% to 124%. At the end of the intervention season, the team’s average percent of fat intake increased slightly to 79% of estimated needs with a range of 52% to 118% (
p = 0.63) (
Figure 1).
A significant improvement (p = 0.001) was seen in the team’s nutrition knowledge after the intervention. Every participant answered more questions accurately after the intervention than prior to the intervention on the sports nutrition knowledge survey. The mean pre-test and post-test scores for all female volleyball players were 24.7 (±5.9) and 31.5 (±6.1), respectively, out of a possible 55 points. Scores ranged from 16 to 37 on the pre-test and 22 to 43 on the post-test.
Figure 1.
Nutritional intakes at Pre, Post Intervention and at Follow-Up (N = 11). Notes: Box plots represent medians, the 25th percentile, and the 75th percentile. Whisker plots represent lower and upper adjacent values. The dashed line represents the (estimated) nutritional goal.
Figure 1.
Nutritional intakes at Pre, Post Intervention and at Follow-Up (N = 11). Notes: Box plots represent medians, the 25th percentile, and the 75th percentile. Whisker plots represent lower and upper adjacent values. The dashed line represents the (estimated) nutritional goal.
4. Discussion
The present study revealed that many participants failed to meet current energy, carbohydrate, protein, and fat recommendations for physically active females during two off-seasons. However, from the non-intervention season to the intervention season, there were significant differences seen in energy, carbohydrate, and protein intake (
Table 3). The mean energy intake for the team at the beginning of the intervention season was 1756 kcal/day (about 24 kcal/kg of body weight) with 0% of participants in energy balance. At the end of the intervention season, the team’s mean energy intake increased to 2178 kcal/day (about 29 kcal/kg of body weight) with 18% of participants on energy balance (meeting 93%–95% of estimated needs). While this change in mean energy intake is a significant improvement, it is still less than the recommended 37 to 41 kcal/kg of body weight. Similar findings were reported in a study of female volleyball players in Greece, with participants baseline mean energy intake during the off-season was estimated at 1541 kcal/day (about 23.8 kcal/kg of body weight per day) [
7]. Moreover, these findings are also supported by other studies showing female athletes with low energy intake compared to energy expenditure [
5,
7,
8,
11,
12].
Table 3.
Percentage of participants either increasing or decreasing dietary intake according to variable upon completion of the study.
Table 3.
Percentage of participants either increasing or decreasing dietary intake according to variable upon completion of the study.
| Variable | Intervention End Increase | Intervention End Decrease |
|---|
| Energy | 73% | 27% |
| Carbohydrate | 82% | 18% |
| Protein | 73% | 27% |
| Fat | 36% | 64% |
| Total | 66% | 34% |
These findings of low energy availability are a major nutritional concern, especially considering the high energy demands of off-season training which was evidenced by participants mean predicted energy expenditure at 3162 kcal/day. According to the Academy of Nutrition and Dietetics, female athletes with persistent low energy intake below 2000 kcal/day can lead to weight loss and disruption of endocrine function [
14]. Moreover, it has been reported that female athletes with low energy intake also have poor micronutrient intakes [
23] and are at risk for a diet deficient in the micronutrients calcium, iron, magnesium, zinc, and B-complex vitamins [
24].
In addition to low energy intake, the team’s mean energy intake from carbohydrates was inadequate for sufficient glycogen repletion both prior to dietary intervention and after dietary intervention. The team’s carbohydrate intake at the beginning of the intervention season averaged at 224 g/day (3.08 g/kg) with 0% of participants meeting estimated needs. At the end of the intervention season, mean carbohydrate intake increased to 304 g/day (4.15 g/kg), with 9% (n = 1) of participants meeting estimated carbohydrate needs.
In addition to an increase in the team’s mean energy and carbohydrate intake, fat intake increased as well although not statistically significant. At the beginning of the intervention, the team’s average fat intake was at 77% of estimated needs (67 g/day) while at the end of the intervention, fat intake increased to 79% of estimated needs (69 g/day);27% of the team’s fat intake exceeded estimated needs by greater than 105% with a range of 108% to 181%. Moreover, most of these players failed to meet adequate carbohydrate intake, which indicates the consumption of high fat foods in place of carbohydrate rich foods. This finding is consistent with other female volleyball players [
25] and female soccer, track and swimming athletes [
6,
7,
8]. Generally, fat intake should range from 20% to 35% of total energy intake [
14]. Although fat is a valuable source of energy, high fat diets have not been shown to be beneficial for athletic performance especially in the presence of inadequate carbohydrate ingestion [
26]. Participants need to reduce their fat intake and increase their carbohydrate intake to meet the foregoing recommendation of 6 to 10 g of carbohydrates per kilogram of body weight.
The team’s average protein intake prior to intervention was at 69 g/day (0.9 g/kg of body weight) while protein intake post intervention was at 84 g/day (1.14 g/kg of body weight). Although these values meet the current DRI for all healthy individuals at 0.8 g/kg, some experts advocate that female athletes should consume protein in levels as high as 1.2–1.7 g/kg for optimal performance [
6,
15]. Furthermore, none of the participants met their estimated protein needs at the beginning of the study. However, 18% (
n = 2) of participants were within estimated protein needs (meeting 94%–102% of estimated needs) at the end of the study.
The sports nutrition knowledge survey revealed participants were least knowledgeable in the areas of weight control, dietary supplements, and general nutrition with greater than 50% of participants answering questions incorrectly most often from these sections. Some of the common questions missed by athletes in this study included those on caffeine and sports performance, functions of vitamins, fat burning foods and supplements as well as supplement regulation and safety which are consistent with the findings of Reilly and Maughan [
2].
The majority of participants (72.7%) had a positive response towards the importance of good nutrition and sports performance. Moreover, 54.5% of participants described their eating habits as fair with nearly 50% reporting a diet based on a wide variety of different foods. The pre-test survey revealed the Media/Internet/Coach/Trainer (83%) as the number one source of nutrition information, whereas the post-test survey revealed a sports dietitian/nutritionist (62.5%) as the number one source of nutrition information.
According to both the pre-test and post-test survey, 50% of participants reported trying to lose weight. In the pre-test survey, a majority of the participants (63.6%) accurately reported that when long term weight loss is desired, athletes should lose at most one to two pounds of body fat per week. However, 50% of participants were unsure of the daily amount of calories that should be reduced to lead to a weekly weight loss of just one pound. In addition, 72.7% of participants report skipping either breakfast (54.5%) or lunch (18.2%) with only 27.3% of participants report not skipping meals or snacks at all. These responses were also evident in the food diaries with the majority of participants not consuming any food or beverage until early afternoon however, reported waking from sleep between 7:00 and 9:00 a.m.
Generally, large discrepancies of energy intake seen in dietary records of female athletes of a stable weight have mostly been attributed to under-reporting [
27]. However, responses generated from the sports nutrition questionnaire might explain some of the inadequacies seen in the food records of this study. For example, the high amount of participants (50%) trying to lose weight, in addition to the high amount (50%) unsure about the appropriate amount of calories to restrict for weight loss, might explain the low calorie intake demonstrated in this study. While this is only an assumption, other reasons female athletes restrict their energy intake have been identified and include disordered eating behaviors, body image issues, and social influences to stay lean [
15,
20,
28]. According to Hinton
et al. [
17], 62% of female collegiate athletes report a desire to lose weight and will resort to decreasing energy and macronutrient intake. Moreover, Rosen, McKeag, Hugh and Curley [
29], found that 32% of female collegiate athletes reported using pathogenic weight control behaviors through laxatives, vomiting, and diet pills, and many of these same women felt these risky behaviors were harmless. This study did not assess weight control behaviors; however, it did indicate that no participants reported using “fat burners” such as Trim Spa, Lipodreme, and Ephedrine.
As previously mentioned, meal skipping evidently played a role in the inadequacies seen in the food records. According to the questionnaire, the most common reason for skipping meals was lack of time (54.5%). Many athletes face barriers that preclude them from maintaining a steady diet schedule. These barriers include class schedules, work, practice, studying, and making time for family and friends. Future studies should address these barriers and propose solutions to accommodate athletes and their busy schedules.
In conclusion, the three day food records used in this study appeared to accurately represent intake among this population. Moreover, the individualized nutrition counseling used in the study proved to be beneficial in producing positive changes in dietary intake and nutrition knowledge. While these changes did not result in the athletes reaching their individual goals, the results demonstrated a positive trend toward achieving these goals. The small sample size and omission of male athletes limits the findings; however, these results do provide a pilot investigation to utilize on a larger, more diverse population. More studies should explore whether an individualized or a group approach is more beneficial in producing positive dietary results when providing nutrition education among athletic teams.


{kind=link}