

Retrospective Analysis of the Impact of a Dietitian and the Canadian Nutrition Screening Tool in a Geriatric Oncology Clinic


Abstract
1. Background
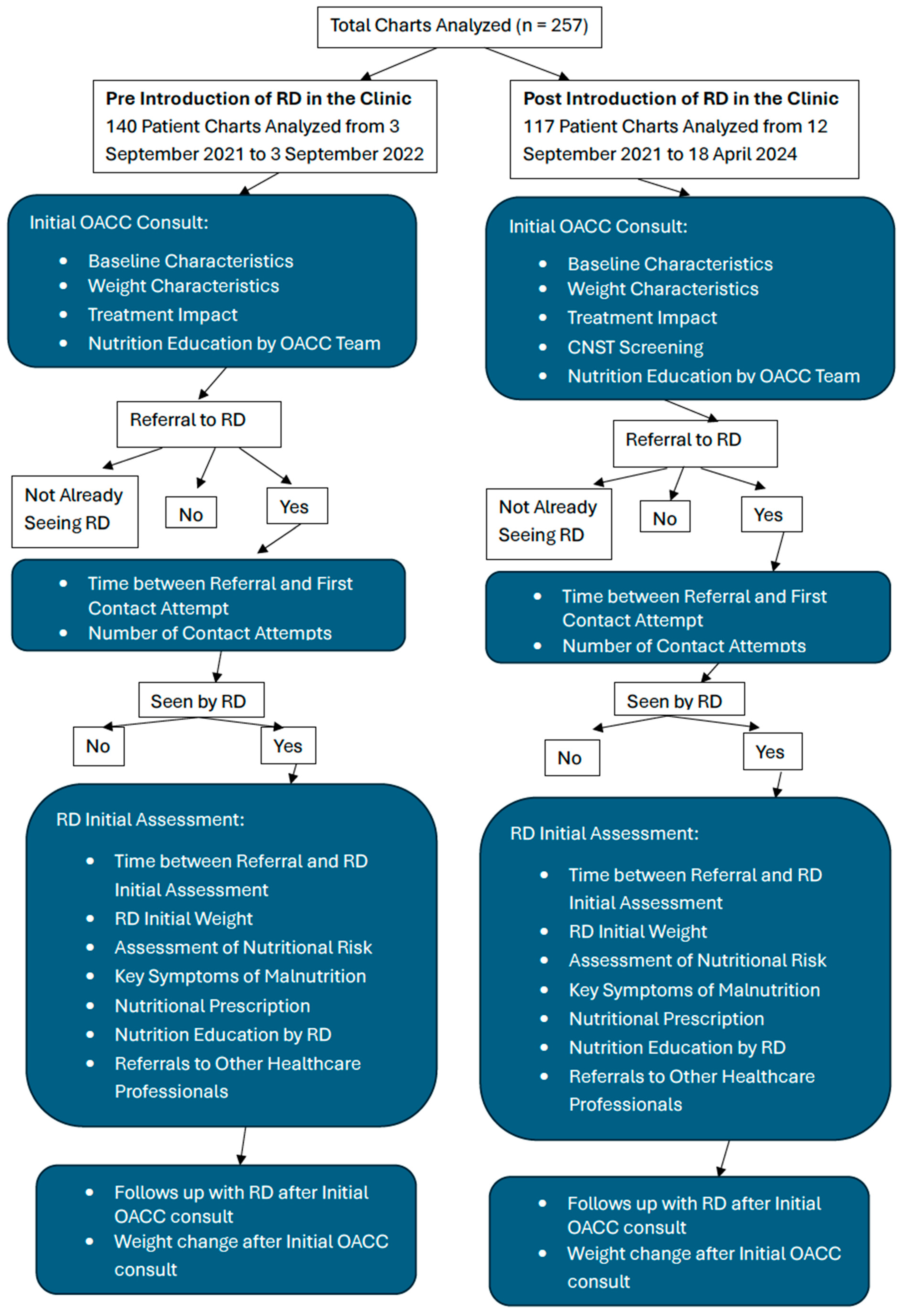
2. Materials and Methods
2.1. Outcome Measures
2.2. Data Extraction
2.3. Sample Size
2.4. Statistical Analyses
3. Results
3.1. Objective 1: Nutrition-Related Patient Outcomes
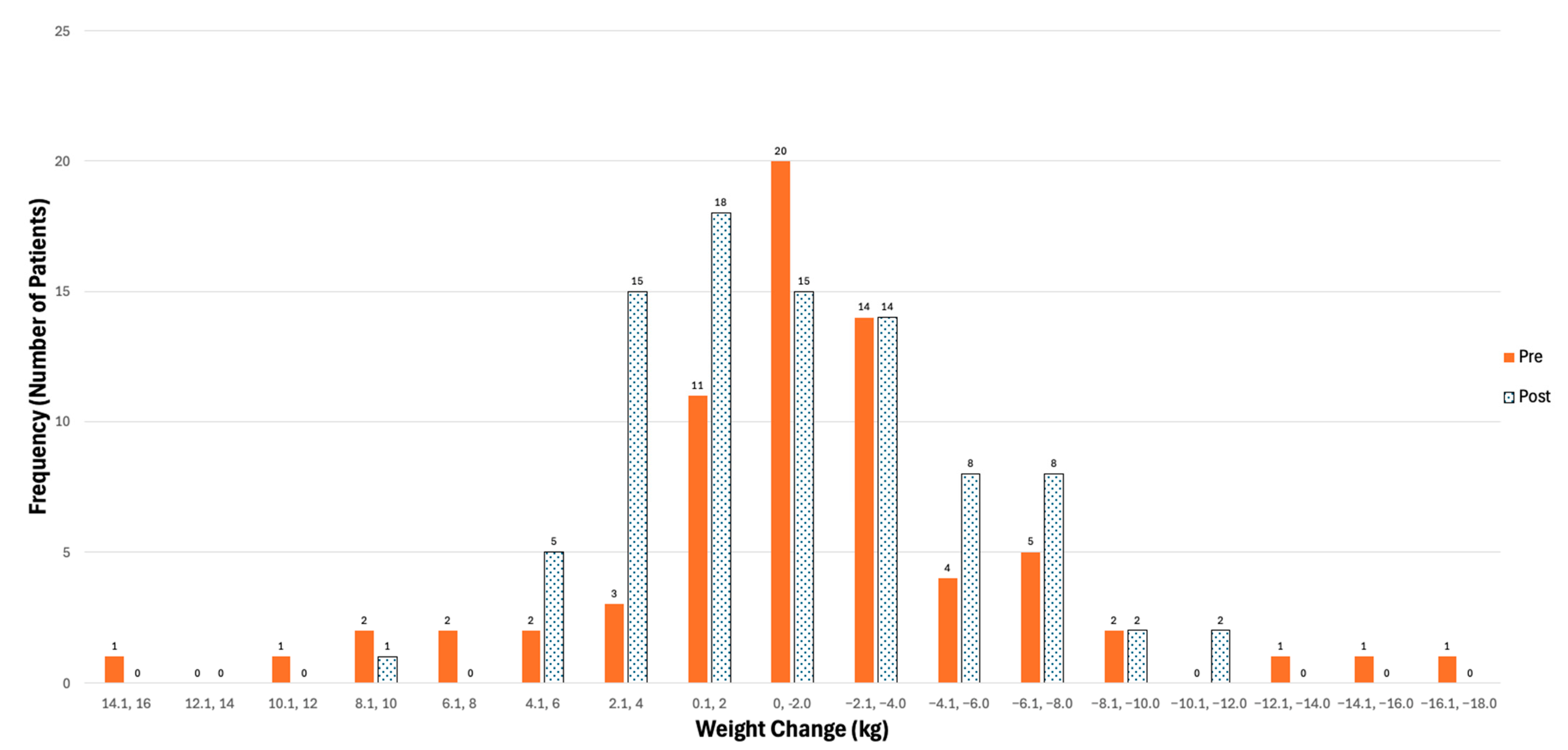
3.1.1. Weight Characteristics at Initial OACC Visit, Initial RD Assessment, % Weight Change at RD Assessment, Prior Weight Loss, Weight Change After OACC Visit
3.1.2. Treatment Impact
3.2. Objective 2: Malnutrition Screening/Identification
3.2.1. Timeliness of Assessment, Referral to First Contact Attempt, Number of Contact Attempts, Referral to Initial RD Assessment
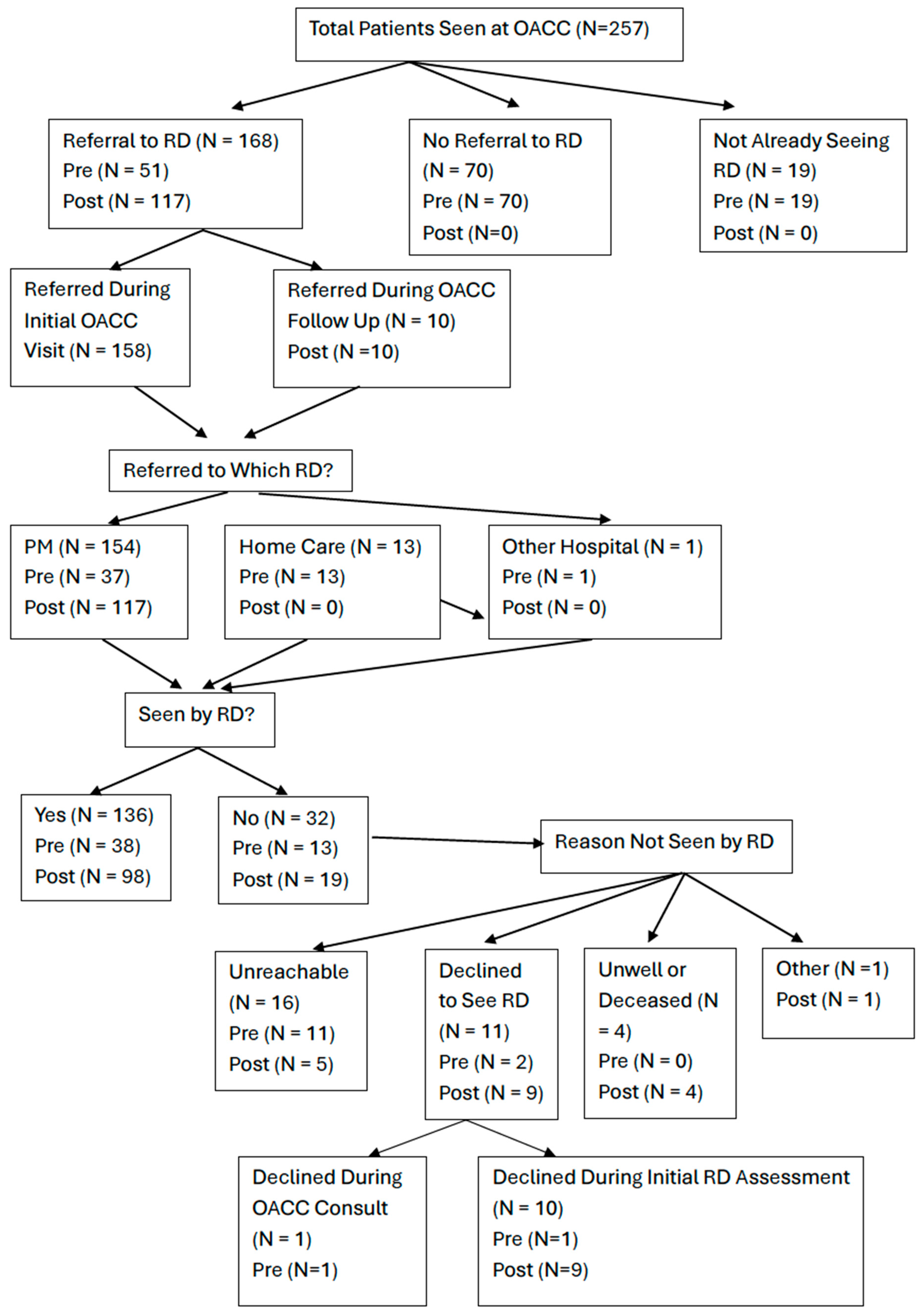
3.2.2. Referrals to Registered Dietitian
3.2.3. RD Nutritional Risk Judgement
3.3. Objective 2: Malnutrition Assessment and Management
3.3.1. Key Symptoms of Malnutrition, Nutritional Prescription with RD
3.3.2. Nutritional Education by RD vs. OACC MD/RN
3.3.3. Referrals to Other Healthcare Professionals by RD
3.3.4. Follow-Ups with RD
3.4. Objective 3: Usefulness of the CNST
Screening Implementation and Comparison of CNST, OACC MD, and RD Nutritional Risk Judgements
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Strohschein, F.J.; Newton, L.; Puts, M.; Jin, R.; Haase, K.; Plante, A.; Loucks, A.; Kenis, C.; Fitch, M. Optimizing the Care of Older Canadians with Cancer and their Families: A Statement Articulating the Position and Contribution of Canadian Oncology Nurses. Can. Oncol. Nurs. J. 2021, 31, 352–356. [Google Scholar] [PubMed] [PubMed Central]
- Blackberry, I.; Boak, J.; Rasekaba, T.; Steer, C. Real-world implementation of geriatric assessment in cancer care among older adults: The role of implementation science frameworks. Curr. Opin. Support. Palliat. Care 2025, 19, 12–18. [Google Scholar] [CrossRef]
- Dale, W.; Klepin, H.D.; Williams, G.R.; Alibhai, S.M.H.; Bergerot, C.; Brintzenhofeszoc, K.; Hopkins, J.O.; Jhawer, M.P.; Katheria, V.; Loh, K.P.; et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Systemic Cancer Therapy: ASCO Guideline Update. J. Clin. Oncol. 2023, 41, 4293–4312. [Google Scholar] [CrossRef]
- Wildiers, H.; Heeren, P.; Puts, M.; Topinkova, E.; Janssen-Heijnen, M.L.; Extermann, M.; Falandry, C.; Artz, A.; Brain, E.; Colloca, G.; et al. International Society of Geriatric Oncology consensus on geriatric assessment in older patients with cancer. J. Clin. Oncol. 2014, 32, 2595–2603. [Google Scholar] [CrossRef]
- Magnuson, A.; Loh, K.P.; Stauffer, F.; Dale, W.; Gilmore, N.; Kadambi, S.; Klepin, H.D.; Kyi, K.; Lowenstein, L.M.; Phillips, T.; et al. Geriatric assessment for the practicing clinician: The why, what, and how. CA Cancer J. Clin. 2024, 74, 496–518. [Google Scholar] [CrossRef]
- Mohile, S.G.; Dale, W.; Somerfield, M.R.; Schonberg, M.A.; Boyd, C.M.; Burhenn, P.S.; Canin, B.; Cohen, H.J.; Holmes, H.M.; Hopkins, J.O.; et al. Practical Assessment and Management of Vulnerabilities in Older Patients Receiving Chemotherapy: ASCO Guideline for Geriatric Oncology. J. Clin. Oncol. 2018, 36, 2326–2347. [Google Scholar] [CrossRef]
- Kleckner, A.S.; Magnuson, A. The nutritional needs of older cancer survivors. J. Geriatr. Oncol. 2022, 13, 738–741. [Google Scholar] [CrossRef] [PubMed]
- Siwakoti, K.; Nabell, L.; McDonald, A.M.; Williams, G.R. Association of malnutrition with geriatric assessment impairments and health-related quality of life among older adults with head and neck cancers. J. Geriatr. Oncol. 2024, 15, 101818. [Google Scholar] [CrossRef] [PubMed]
- Williams, G.R.; Al-Obaidi, M.; Dai, C.; Mir, N.; Challa, S.A.; Daniel, M.; Patel, H.; Barlow, B.; Young-Smith, C.; Gbolahan, O.; et al. Association of malnutrition with geriatric assessment impairments and health-related quality of life among older adults with gastrointestinal malignancies. Cancer 2020, 126, 5147–5155. [Google Scholar] [CrossRef]
- Vitaloni, M.; Caccialanza, R.; Ravasco, P.; Carrato, A.; Kapala, A.; de van der Schueren, M.; Constantinides, D.; Backman, E.; Chuter, D.; Santangelo, C.; et al. The impact of nutrition on the lives of patients with digestive cancers: A position paper. Support. Care Cancer 2022, 30, 7991–7996. [Google Scholar] [CrossRef]
- Isenring, E.A.; Capra, S.; Bauer, J.D. Nutrition intervention is beneficial in oncology outpatients receiving radiotherapy to the gastrointestinal or head and neck area. Br. J. Cancer 2004, 91, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Dai, W.; Wang, S.A.; Wang, K.; Chen, C.; Wang, J.; Chen, X.; Yan, J. Impact of Nutrition Counseling in Head and Neck Cancer Sufferers Undergoing Antineoplastic Therapy: A Randomized Controlled Pilot Study. Curr. Oncol. 2022, 29, 6947–6955. [Google Scholar] [CrossRef] [PubMed]
- Ravasco, P.; Monteiro-Grillo, I.; Camilo, M. Individualized nutrition intervention is of major benefit to colorectal cancer patients: Long-term follow-up of a randomized controlled trial of nutritional therapy. Am. J. Clin. Nutr. 2012, 96, 1346–1353. [Google Scholar] [CrossRef]
- Sullivan, E.S.; Rice, N.; Kingston, E.; Kelly, A.; Reynolds, J.V.; Feighan, J.; Power, D.G.; Ryan, A.M. A national survey of oncology survivors examining nutrition attitudes, problems and behaviours, and access to dietetic care throughout the cancer journey. Clin. Nutr. ESPEN 2021, 41, 331–339. [Google Scholar] [CrossRef] [PubMed]
- Trujillo, E.B.; Claghorn, K.; Dixon, S.W.; Hill, E.B.; Braun, A.; Lipinski, E.; Platek, M.E.; Vergo, M.T.; Spees, C. Inadequate Nutrition Coverage in Outpatient Cancer Centers: Results of a National Survey. J. Oncol. 2019, 2019, 7462940. [Google Scholar] [CrossRef]
- Roeland, E.J.; Dunne, R.F. The Impact of Early Referrals to Dietitians for Patients With Esophagogastric Cancer. J. Natl. Compr. Cancer Netw. 2021, 19, 235–238. [Google Scholar] [CrossRef]
- Abu Helal, A.; Chon, J.; Timilshina, N.; Berger, A.; Romanovsky, L.; Jin, R.; Monginot, S.; Alibhai, S.M.H. Quality of care of consultations from the geriatric oncology clinic: “Are we addressing the needs of patients?”. J. Geriatr. Oncol. 2022, 13, 440–446. [Google Scholar] [CrossRef]
- Laporte, M.; Keller, H.H.; Payette, H.; Allard, J.P.; Duerksen, D.R.; Bernier, P.; Jeejeebhoy, K.; Gramlich, L.; Davidson, B.; Vesnaver, E.; et al. Validity and reliability of the new Canadian Nutrition Screening Tool in the ‘real-world’ hospital setting. Eur. J. Clin. Nutr. 2015, 69, 558–564. [Google Scholar] [CrossRef]
- Mislang, A.R.; Di Donato, S.; Hubbard, J.; Krishna, L.; Mottino, G.; Bozzetti, F.; Biganzoli, L. Nutritional management of older adults with gastrointestinal cancers: An International Society of Geriatric Oncology (SIOG) review paper. J. Geriatr. Oncol. 2018, 9, 382–392. [Google Scholar] [CrossRef]
- Canadian Malnutrition Task Force. Research–Nutrition Care in Canada [Internet]; Canadian Malnutrition Task Force: Toronto, ON, Canada, 2025; Available online: https://nutritioncareincanada.ca/research (accessed on 25 April 2025).
- Taylor, L.M.; Eslamparast, T.; Farhat, K.; Kroeker, K.; Halloran, B.; Shommu, N.; Kumar, A.; Fitzgerald, Q.; Gramlich, L.; Abraldes, J.G.; et al. Using Patient Completed Screening Tools to Predict Risk of Malnutrition in Patients With Inflammatory Bowel Disease. Crohns Colitis 360 2021, 3, otab043. [Google Scholar] [CrossRef]
- Canadian Taskforce on Anthropometric Measures (CTAN). Nourish: Nourishing Canada’s Aging Population [Internet]; Nourish: Toronto, ON, Canada, 2025; Available online: https://www.nourishonline.ca/ctan/ (accessed on 25 April 2025).
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef] [PubMed]
- Almugbel, F.A.; Timilshina, N.; AlQurini, N.; Loucks, A.; Jin, R.; Berger, A.; Romanovsky, L.; Puts, M.; Alibhai, S.M.H. Role of the vulnerable elders survey-13 screening tool in predicting treatment plan modification for older adults with cancer. J. Geriatr. Oncol. 2021, 12, 786–792. [Google Scholar] [CrossRef] [PubMed]
- Alibhai, S.M.H.; Jin, R.; Loucks, A.; Yokom, D.W.; Watt, S.; Puts, M.; Timilshina, N.; Berger, A. Beyond the black box of geriatric assessment: Understanding enhancements to care by the geriatric oncology clinic. J. Geriatr. Oncol. 2018, 9, 679–682. [Google Scholar] [CrossRef]
- University Health Network. Standards of Care: Clinical Nutrition Prioritization Matrix; University Health Network: Toronto, ON, Canada, 2019; p. 38. [Google Scholar]
- Richards, J.; Arensberg, M.B.; Thomas, S.; Kerr, K.W.; Hegazi, R.; Bastasch, M. Impact of Early Incorporation of Nutrition Interventions as a Component of Cancer Therapy in Adults: A Review. Nutrients 2020, 12, 3403. [Google Scholar] [CrossRef] [PubMed]
- Cancer Care Ontario. Appendix 1-45: CCO DBK, version 2; Cancer Care Ontario: Toronto, ON, Canada, 2024; p. 5. Available online: https://quorum.hqontario.ca/Portals/0/Users/125/53/22653/CCO_DBK_Appendix_1-45_APR_21(2).pdf (accessed on 25 April 2025).
- Soares, C.H.; Beuren, A.G.; Friedrich, H.J.; Gabrielli, C.P.; Stefani, G.P.; Steemburgo, T. The Importance of Nutrition in Cancer Care: A Narrative Review. Curr. Nutr. Rep. 2024, 13, 950–965. [Google Scholar] [CrossRef]
- Gray, A.; Dang, B.N.; Moore, T.B.; Clemens, R.; Pressman, P. A review of nutrition and dietary interventions in oncology. SAGE Open Med. 2020, 8, 2050312120926877. [Google Scholar] [CrossRef]
- Princess Margaret Cancer Campus. Malnutrition in Cancer Care [Internet]; University Health Network: Toronto, ON, Canada, 2025; Available online: https://pmcancercampus.ca/local/courseinfo/courseInfoPage.php?id=280 (accessed on 25 April 2025).

{kind=link}
{kind=link}
{kind=link}
| Objective | Outcome Measure | Outcome Measure Definition Pre OACC RD | Outcome Measure Definition Post OACC RD | Source of Outcome Measure |
|---|---|---|---|---|
| (1) To assess nutrition-related patient outcomes prior to and after the introduction of a dietitian in the OACC | Weight Characteristics | Body Mass Index measured by OACC MD/RN | Body Mass Index measured by OACC MD/RN | OACC consult note in Epic (electronic health record) |
| Initial RD Assessment Weight | Initial RD Assessment Weight | Extracted from RD’s notes on Epic or RD’s notes | ||
| Prior weight loss at OACC consult | Prior weight loss at OACC consult | Self-reported by patient and taken from initial OACC consult note in Epic | ||
| Clinically significant weight loss based on the UHN Clinical Nutrition Prioritization matrix defined as unintentional weight loss meeting any of the following criteria: greater than 2% within 1 week, 5% within 1 month, 7.5% within 3 months, or 10% within 6 months [26] | Clinically significant weight loss based on the UHN Clinical Nutrition Prioritization matrix defined as unintentional weight loss meeting any of the following criteria: greater than 2% within 1 week, 5% within 1 month, 7.5% within 3 months, or 10% within 6 months [26] | Calculate weight % change from self-reported weight loss by patient and baseline weight in initial OACC consult note. Determine if weight % change in patient reported time frame meets UHN Clinical Prioritization Matrix | ||
| Weight change between initial OACC consult and 3 ± 1 months after initial OACC consult | Weight change between initial OACC consult and 3 ± 1 months after initial OACC consult | Initial weight and follow up weight taken from Epic or RD excel spreadsheet notes. | ||
| Positive CNST | OACC initial consult note in Epic | |||
| Treatment Impact | Was nutrition explicitly mentioned in the treatment recommendation from OACC? Yes/No | Was nutrition explicitly mentioned in the treatment recommendation from OACC? Yes/No | Found in OACC consult note under cancer treatment decision making recommendation | |
| Was nutrition explicitly mentioned in final treatment plan from oncology? Yes/No | Was nutrition explicitly mentioned in final treatment plan from oncology? Yes/No | Found in Epic notes from oncologist | ||
| (2) To assess whether malnutrition was adequately assessed and managed when identified | Malnutrition Screening/Identification | Time between referral request and first contact attempt from RD | Time between referral request and first contact attempt from RD | Found in RD’s notes by comparing date of referral to first contact attempt |
| Number of contact attempts by RD | Number of contact attempts by RD | Found in RD’s notes | ||
| Time between referral request and initial assessment from RD | Time between referral request and initial assessment from RD | Found in Epic by comparing date of referral request and date of initial assessment by the RD | ||
| Referral to RD: Yes/No If yes, which dietitian, PM or Home Care or Other Hospital | Referral to RD: Yes/No If yes, which dietitian, PM or Home Care or Other Hospital | Found in initial OACC consult and first follow up notes and referral request in Epic | ||
| Referral to RD During Follow up OACC Visit Yes/No | Referral to RD During Follow up OACC Visit Yes/No | Found in follow up OACC note and referral request in Epic | ||
| Seen by RD: Yes/No | Seen by RD: Yes/No | Found in RD’s initial assessment notes in Epic | ||
| Reason not seen by RD: patient declined to see RD/Unreachable (RD contact attempt but no answer)/Unwell or Deceased/Other | Reason not seen by RD: patient declined to see RD//Unreachable (RD contact attempt but no answer)/Unwell or Deceased/Other | Found in Epic or RD’s notes | ||
| Standard of Care Clinical Nutrition Prioritization Matrix –Assessment of Nutritional Risk: High/Moderate/Low (Supplementary Figure S1) | Standard of Care Clinical Nutrition Prioritization Matrix—Assessment of Nutritional Risk: High/Moderate/Low (Supplementary Figure S1) | Determined by the RD initial assessment and follow ups in Epic or RD Notes | ||
| Malnutrition Assessment and Management | Key symptoms of malnutrition: appetite, constipation, muscle weakness Yes/No | Key symptoms of malnutrition: appetite, constipation, muscle weakness Yes/No | Under nutrition focused findings in initial assessment by the RD in Epic | |
| Nutritional prescription: Were recommendations made by RD: dietary (energy/protein/fluids requirements), medications (e.g., modifying bowel routine, correcting electrolyte imbalances), investigations (blood work, x-rays)? Yes/No | Nutritional prescription: Were recommendations made by RD: dietary (energy/protein/fluids requirements), medications (e.g., modifying bowel routine, correcting electrolyte imbalances), investigations (blood work, x-rays)? Yes/No | Found in RD’s notes or in Epic, specifically under nutritional interventions and recommendation | ||
| Nutrition education: Was education on nutrition provided by RD? Yes/No | Nutrition education: Was education on nutrition provided by RD? Yes/No | Found in RD’s notes under nutritional interventions and recommendation | ||
| Nutrition education: Was education on nutrition provided by OACC MD/RN? Yes/No | Nutrition education: Was education on nutrition provided by OACC MD/RN? Yes/No | Found in OACC consult note | ||
| Referral to other healthcare professionals: speech language pathologist, social worker, dentistry, OACC MD physician, other (physician specialties) Yes/No | Referral to other healthcare professionals: speech language pathologist, social worker, dentistry, OACC MD physician, other (physician specialties) Yes/No | Found in RD’s spreadsheet notes or in the OACC initial consult or first initial assessment by RD in Epic | ||
| Number of follow up with RD within 3 ± 1 months after initial OACC consult | Number of follow up with RD within 3 ± 1 months after initial OACC consult | Extracted from RD’s notes in Epic | ||
| (3) To examine the usefulness of the CNST in identifying malnutrition risk | Nutritional Risk Determined by RD vs. CNST vs. OACC MD | Comparison of high/moderate/low nutritional risk determined by RD based on standard of care criteria, compared to CNST positive/negative, and OACC MD normal/at risk/malnourished nutritional risk diagnosis (clinical judgement). Additional comparison of CNST negative patients with clinically significant weight loss and their corresponding RD nutrition risk. | Data found in Epic and in RD’s notes |
| Characteristic | Total Mean (SD) or N (%) | Pre Mean (SD) or N (%) | Post Mean (SD) or N (%) |
|---|---|---|---|
| Age, y | 80.7 (6.4) | 80.2 (6.4) | 81.4 (6.5) |
| Female Sex | 138 (53.7%) | 68 (48.6%) | 70 (59.8%) |
| VES-13 Score ≥ 3 (Vulnerable) | 203 (79.0%) | 109 (77.9%) | 94 (80.3%) |
| Disease Site | Head and Neck 61 (23.7%) GI 53 (20.6%) Gyne 41 (16.0%) Lymphoma 27 (10.5%) GU 20 (7.8%) Thoracic 20 (7.8%) | Head and Neck 41 (29.3%) GI 34 (24.3%) Gyne 19 (13.6%) Lymphoma 14 (10.0%) GU 11 (7.9%) Thoracic 8 (5.7%) | Gyne 22 (18.8%) Head and Neck 20 (17.1%) GI 19 (16.2%) Lymphoma 13 (11.1%) Thoracic 12 (10.3%) Breast 10 (8.5%) |
| Treatment Intent | |||
| Palliative | 99 (38.5%) | 55 (39.3%) | 44 (37.6%) |
| Curative | 127 (49.4%) | 74 (52.9%) | 53 (45.3%) |
| Unknown | 31 (12.1%) | 11 (7.9%) | 11 (9.4%) |
| Reason for Referral | |||
| Pre Treatment | 198 (77.0%) | 112 (80.0%) | 86 (73.5%) |
| Active Treatment a | 39 (15.2%) | 15 (10.7%) | 24 (20.5%) |
| Other | 20 (7.8%) | 13 (9.3%) | 7 (6.0%%) |
| Current Treatment a | |||
| Yes | 108 (42.0%) | 51 (36.4%) | 57 (48.7%) |
| Current Treatment Modality | |||
| Chemotherapy | 30 | 13 | 17 |
| Multimodal | 16 | 8 | 8 |
| Surveillance | 16 | 8 | 8 |
| Surgery | 15 | 9 | 6 |
| Radiation | 15 | 5 | 10 |
| Hormone Therapy | 9 | 4 | 5 |
| Immunotherapy | 5 | 1 | 4 |
| Other | 5 | 2 | 3 |
| Targeted Therapy | 3 | 2 | 1 |
| Proposed Treatment Modality | |||
| Surgery | 75 | 47 | 28 |
| Chemotherapy | 52 | 30 | 22 |
| Multimodal b | 46 | 23 | 23 |
| Radiation | 19 | 10 | 9 |
| Immunotherapy | 6 | 4 | 2 |
| Hormone Therapy | 4 | 2 | 2 |
| Other | 4 | 1 | 3 |
| Targeted | 3 | 1 | 2 |
| Surveillance/Supportive Care | 0 | 0 | 0 |
| GERIATRIC DOMAINS c | |||
| Comorbidity | |||
| High | 39 (15.2) | 20 (14.3) | 19 (16.2) |
| Moderate | 82 (31.9) | 42 (30.0) | 40 (34.2) |
| Low | 136 (52.9) | 78 (55.7) | 58 (49.6) |
| Functional Status -IADLs | |||
| Independent | 94 (36.6) | 54 (38.6) | 40 (34.2) |
| Dependent in 1 + IADLs | 163 (63.4) | 86 (61.4) | 77 (65.8) |
| Functional Status—Physical Performance | |||
| Normal | 59 (23.0) | 32 (22.9) | 27 (23.1) |
| Decreased | 195 (75.9) | 105 (75.0) | 90 (76.9) |
| Deferred | 3 (1.2) | 3 (2.1) | 0 (0.0) |
| Falls Risk | |||
| Increased | 168 (65.4) | 91 (65.0) | 77 (65.8) |
| Not Increased | 87 (33.9) | 47 (33.6) | 40 (34.2) |
| Deferred | 2 (0.8) | 2 (1.4) | 0 (0.0) |
| Medication Optimization | |||
| Potential for Optimization | 176 (68.5) | 87 (62.1) | 89 (76.1) |
| No Issues | 81 (31.5) | 53 (37.9) | 28 (23.9) |
| Social Support | |||
| Good | 171 (66.5) | 98 (70.0) | 73 (62.4) |
| Vulnerable | 84 (32.7) | 41 (29.3) | 43 (36.8) |
| None | 2 (0.8) | 1 (0.7) | 1 (0.9) |
| Mood | |||
| Normal | 183 (71.2) | 106 (75.7) | 77 (65.8) |
| Depressed | 60 (23.3) | 26 (18.6) | 34 (29.1) |
| Unable to Assess Fully | 14 (5.4) | 8 (5.7) | 6 (5.1) |
| Cognition | |||
| Normal | 127 (49.4) | 68 (48.6) | 59 (50.4) |
| Abnormal | 68 (26.5) | 40 (28.6) | 28 (23.9) |
| Borderline/Req Further Testing | 62 (24.1) | 32 (22.9) | 30 (25.6) |
| Nutrition | |||
| Malnourished | 62 (24.1) | 21 (15.0) | 41 (35.0) |
| At Risk | 182 (70.8) | 119 (85.0) | 63 (53.8) |
| Normal | 13 (5.1) | 0 (0.0) | 13 (11.1) |
| Characteristic | Total Mean (SD) or N (%) | Pre Mean (SD) or N (%) | Post Mean (SD) or N (%) | Between Groups, p Value |
|---|---|---|---|---|
| Body Mass Index (kg/m2) | 24.8 (5.7) | 25.1 (6.0) | 24.5 (5.3) | 0.39 |
| Initial Weight at RD Assessment (kg) | 62.2 (14.7) | 67.6 (14.3) | 62.1 (14.7) | 0.10 |
| Prior Weight Loss | ||||
| Yes | 217 (84.4) | 114 (81.4) | 103 (88.0) | |
| Yes, quantifiable | 191 (88.0) | 102 (89.5) | 89 (86.4) | |
| Weight Loss (kg) a | 6.8 (4.5–10.0) | 6.8 (4.5–9.8) | 6.0 (3.2–9.8) | 0.19 |
| Time of Weight Loss (months) | 6.3 (2.9) | 6.5 (3.2) | 6.0 (2.5) | |
| Clinically Significant Weight Loss b | 80 (41.9) | 40 (40.2) | 39 (43.8) | 0.61 |
| Weight Change (kg) | −1.2 (4.6) | −1.4 (5.3) | −1.2 (4.0) | 0.77 |
| Time period of Weight Change (days) c | 90.8 (14.9) | 90.6 (15.8) | 90.9 (14.4) | 0.90 |
| Reported Weight Change | 158 (61.5) | 70 (50.0) | 88 (75.2) | |
| Weight Loss of ≥ 5 kg | 26 (16.5) | 13 (18.6) | 13 (14.8) | 0.52 |
| Missing Weight | 99 (38.5) | 70 (50.0) | 29 (24.8) | <0.001 |
| Reason for Missing Weight | ||||
| Not Seen at Hospital | 45 (45.5) | 31 (44.3) | 14 (48.3) | |
| Seen but Not Recorded | 46 (46.5) | 38 (54.3) | 8 (27.6) | |
| No Initial Weight | 8 (8.1) | 1 (1.4) | 7 (24.1) |
| Characteristic | Total | Pre | Post | High Risk Pre | High Risk Post | Between Groups, p Value a |
|---|---|---|---|---|---|---|
| Referral to First Contact Attempt (Days) | ||||||
| Mean (SD) | 16.9 (12.6) | 19.9 (18.7) | 16.2 (10.7) | 18.6 (17.7) | 14.3 (10.4) | 0.20 |
| Median (IQR) | 14 (9–23) | 14 (7–26.25) | 14 (10–22) | 14 (8–27.8) | 13 (7–19.5) | 0.97 |
| Range | 0–73 | 0–67 | 2–73 | 0–62 | 2–73 | |
| Number of Contact Attempts Mean (SD) | 1.16 (0.46) | 1 (0) | 1.20 (0.51) | 1 (0) | 1.12 (0.50) | 0.06 |
| Referral to Initial Assessment (Days) | ||||||
| Mean (SD) | 25.5 (22.7) | 20.4 (18.4) | 26.7 (23.6) | 19.6 (17.1) | 21.8 (24.1) | 0.23 |
| Median (IQR) | 20 (10–32) | 14 (8.5–26.3) | 21 (10–34) | 14 (9–27.7) | 14 (7–23.5) | 0.18 |
| Range | 2–138 | 2–67 | 2–138 | 2–63 | 2–138 |
| Characteristic | CNST Positive N (%) | CNST Negative N (%) | Between Groups, p Value |
|---|---|---|---|
| Total | N = 71 | N = 42 | |
| OACC MD Nutritional Clinical Judgement | |||
| Malnourished | 34 (47.9) | 7 (16.7) | <0.001 |
| At Risk | 37 (52.1) | 24 (57.1) | |
| Normal | 0 (0.0) | 11 (26.2) * | |
| Seen by RD | |||
| Yes | 58 (81.7) | 36 (85.7) | |
| No | 13 (18.3) | 6 (14.3) | |
| Reason Not Seen | |||
| Unreachable | 6 (46.2) | 0 (0.0) | |
| Unwell/Deceased | 2 (15.4) | 2 (33.3) | |
| RD Nutritional Risk Judgement a | |||
| High | 39 (67.2) | 16 (44.4) | 0.03 |
| Moderate | 18 (31.0) | 16 (44.4) | 0.006 b |
| Low | 1 (1.7) | 4 (11.1) | |
| RD Nutritional Risk Judgement with Patients Who Had Clinically Significant Weight Loss but were CNST negative (n = 8) | |||
| High | 4 (50.0) | ||
| Moderate | 3 (37.5) | ||
| Low | 1 (12.5) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, H.; Cerullo, L.; Jin, R.; Monginot, S.; Alibhai, S.M.H. Retrospective Analysis of the Impact of a Dietitian and the Canadian Nutrition Screening Tool in a Geriatric Oncology Clinic. Nutrients 2025, 17, 1591. https://doi.org/10.3390/nu17091591
Ho H, Cerullo L, Jin R, Monginot S, Alibhai SMH. Retrospective Analysis of the Impact of a Dietitian and the Canadian Nutrition Screening Tool in a Geriatric Oncology Clinic. Nutrients. 2025; 17(9):1591. https://doi.org/10.3390/nu17091591
Chicago/Turabian StyleHo, Harriet, Linda Cerullo, Rana Jin, Susie Monginot, and Shabbir M. H. Alibhai. 2025. "Retrospective Analysis of the Impact of a Dietitian and the Canadian Nutrition Screening Tool in a Geriatric Oncology Clinic" Nutrients 17, no. 9: 1591. https://doi.org/10.3390/nu17091591
APA StyleHo, H., Cerullo, L., Jin, R., Monginot, S., & Alibhai, S. M. H. (2025). Retrospective Analysis of the Impact of a Dietitian and the Canadian Nutrition Screening Tool in a Geriatric Oncology Clinic. Nutrients, 17(9), 1591. https://doi.org/10.3390/nu17091591